
Forced Sedentariness and Sports Activity as Factors Differentiating Anthropometric Characteristics, Indices, and Body Composition in People with Disabilities


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Anthropometric Characteristics
2.4. Indices
2.5. Body Composition
2.6. Statistical Analysis
3. Results
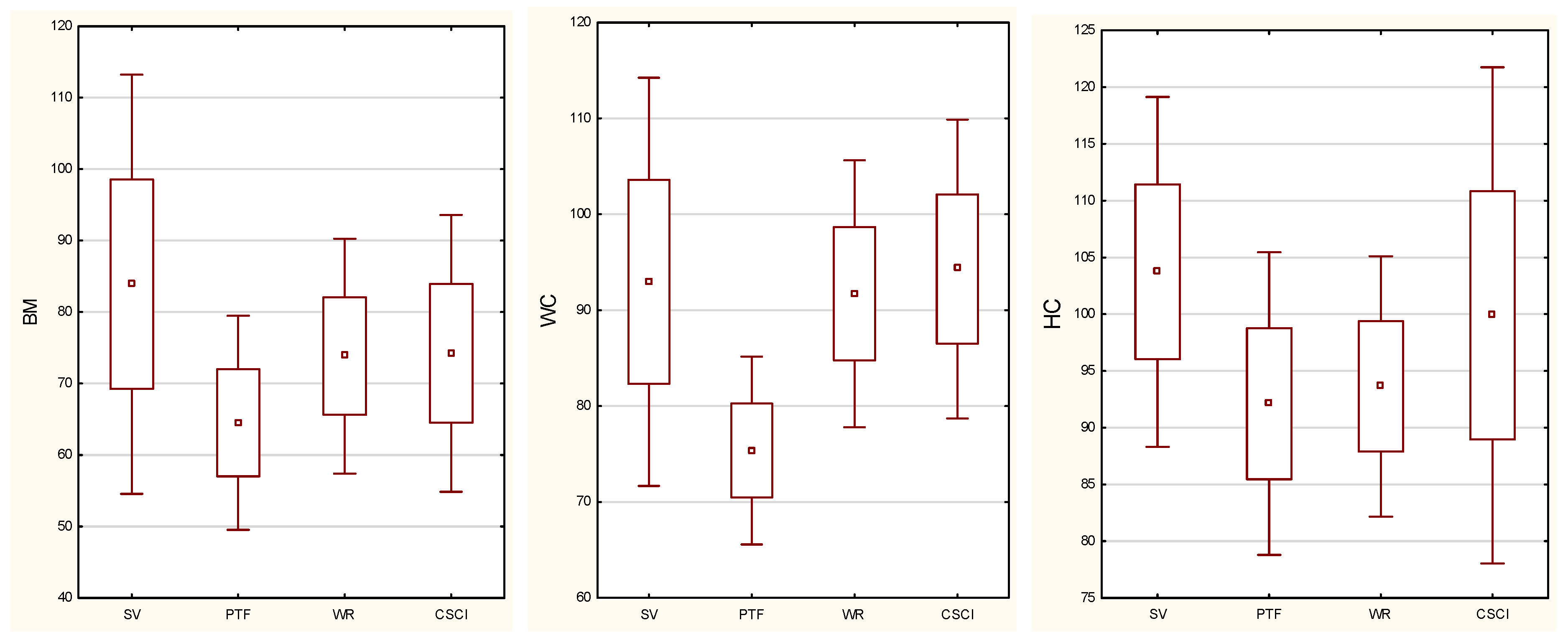
3.1. Anthropometric Characteristics
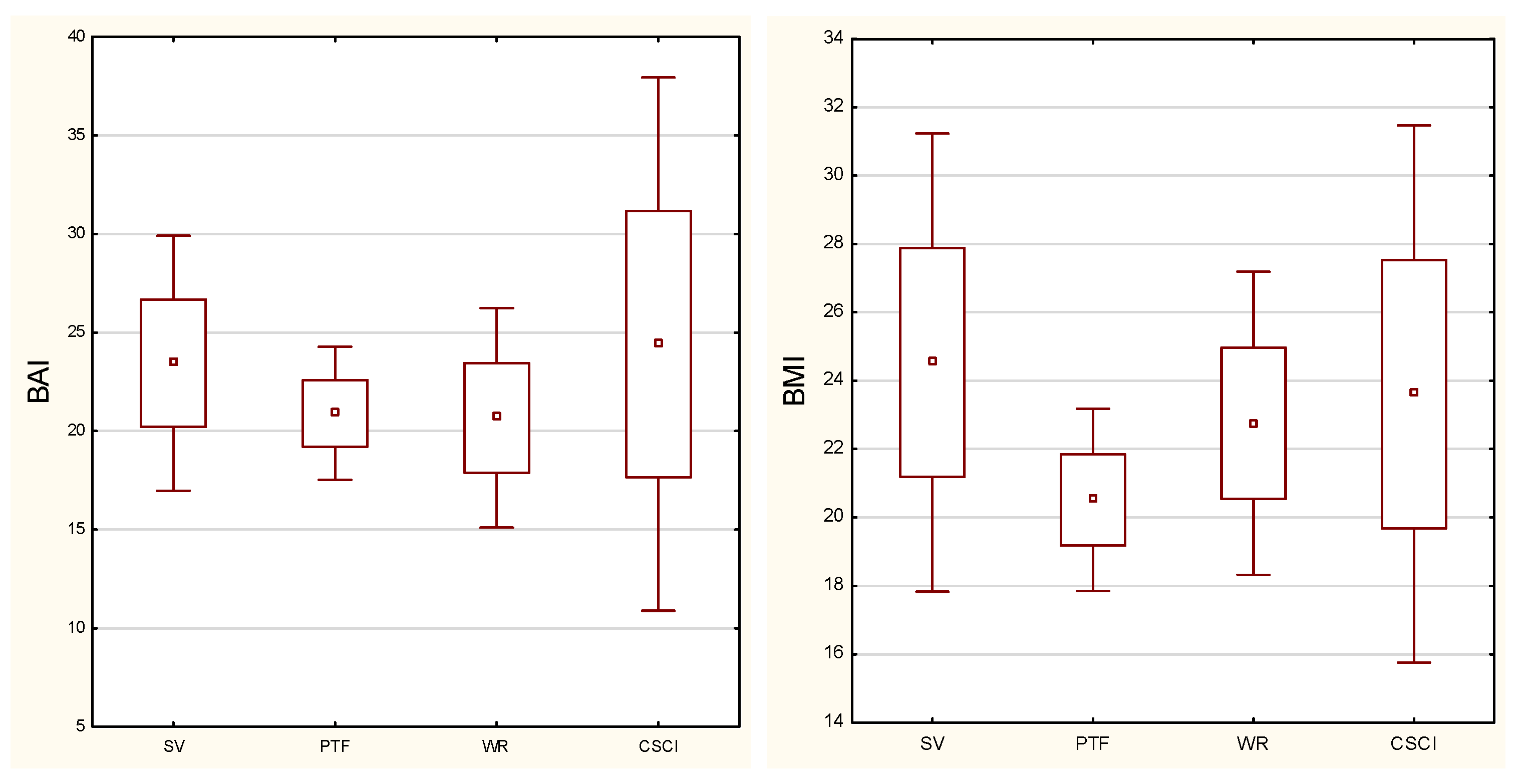
3.2. Indices (BMI, BAI)
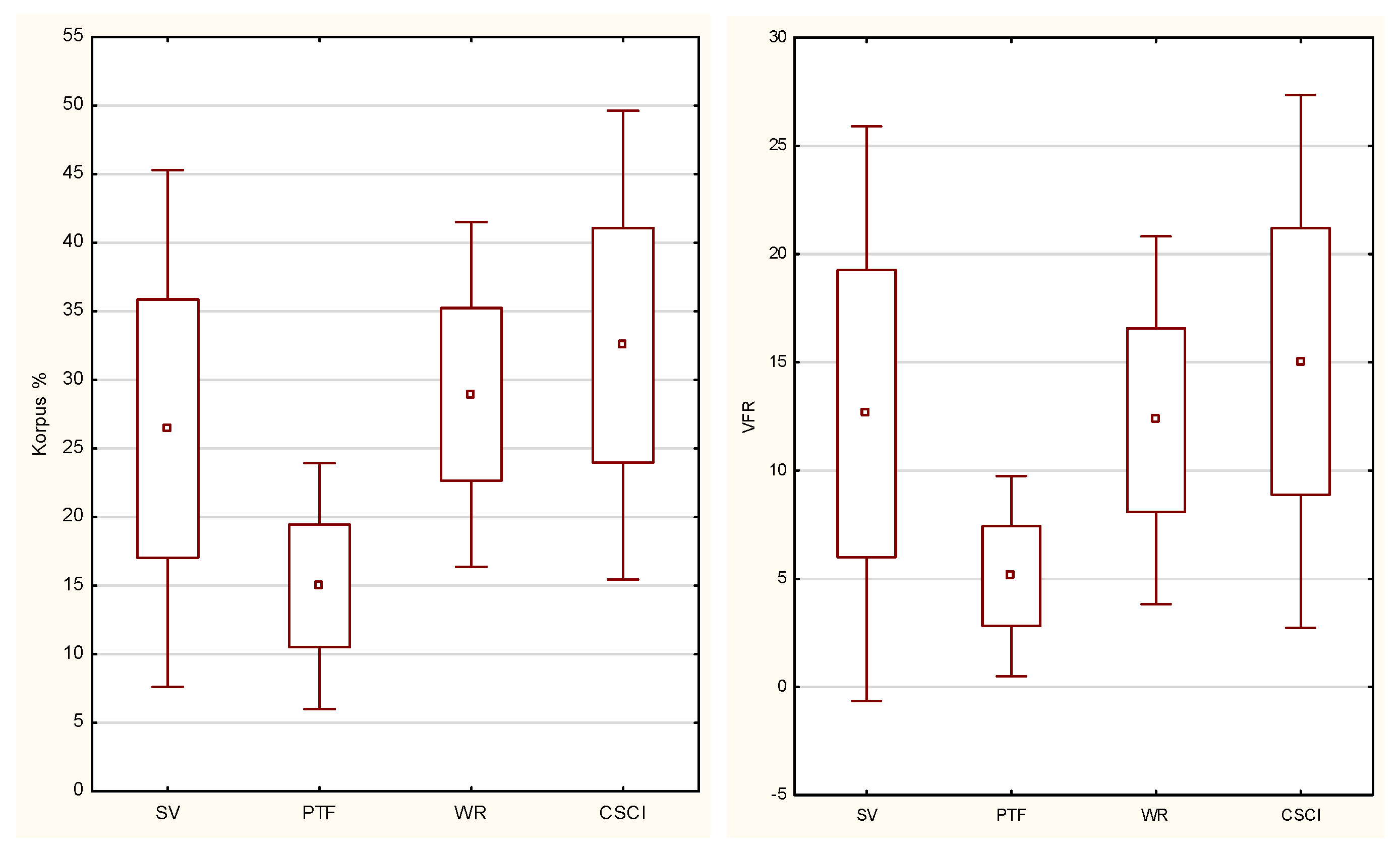
3.3. Body Composition
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liou, T.H.; Pi-Sunyer, F.X.; Laferrère, B. Physical disability and obesity. Nutr. Rev. 2005, 63, 321–331. [Google Scholar] [CrossRef] [PubMed]
- Zwierzchowska, A.; Głowacz, M.; Batko-Szwaczka, A.; Dudzińska-Griszek, J.; Mostowik, A.; Drozd, M.; Szewieczek, J. The Body Mass Index and Waist Circumference as Predictors of Body Composition in Post CSCI Wheelchair Rugby Players (Preliminary Investigations). J. Hum. Kinet. 2014, 12, 191–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorgey, A.S.; Wells, K.M.; Austin, T.L. Adiposity and spinal cord injury. World J. Orthop. 2015, 6, 567–576. [Google Scholar] [CrossRef]
- Spungen, A.M.; Adkins, R.H.; Stewart, C.A.; Wang, J.; Pierson, R.N., Jr.; Waters, R.L.; Bauman, W.A. Factors influencing body composition in persons with spinal cord injury: A cross-sectional study. J. Appl. Physiol. 2003, 95, 2398–2407. [Google Scholar] [CrossRef] [PubMed]
- Gaweł, E.; Zwierzchowska, A. Effect of Compensatory Mechanisms on Postural Disturbances and Musculoskeletal Pain in Elite Sitting Volleyball Players: Preparation of a Compensatory Intervention. Int. J. Environ. Res. Public Health 2021, 18, 10105. [Google Scholar] [CrossRef]
- Gorla, J.I.; Costa e Silva, A.; Borges, M.; Tanhoffer, R.A.; Godoy, P.S.; Calegari, D.R.; Santos, A.; Ramos, C.D.; Nadruz Junior, W.; Cliquet Junior, A. Impact of Wheelchair Rugby on Body Composition of Subjects With Tetraplegia: A Pilot Study. Arch. Phys. Med. Rehabil. 2016, 97, 92–96. [Google Scholar] [CrossRef]
- Sarabia, J.M.; Doménech, C.; Roche, E.; Vicente-Salar, N.; Reina, R. Anthropometrical Features of Para-Footballers According to Their Cerebral Palsy Profiles and Compared to Controls. Int. J. Environ. Res. Public Health 2020, 17, 9071. [Google Scholar] [CrossRef]
- Sadowska-Krępa, E.; Zwierzchowska, A.; Głowacz, M.; Borowiec-Rybak, K.; Kłapcińska, B. Blood metabolic response to a long-term wheelchair rugby training. Spinal. Cord. 2016, 54, 371–375. [Google Scholar] [CrossRef]
- Lemos, V.D.A.; Alves, E.D.S.; Schwingel, P.A.; Rosa, J.P.P.; Da Silva, A.; Winckler, C.; Vital, R.; De Almeida, A.A.; Tufik, S.; De Mello, M.T. Analysis of the body composition of Paralympic athletes: Comparison of two methods. Eur. J. Sport Sci. 2016, 16, 955–964. [Google Scholar] [CrossRef]
- Medeiros, R.M.V.; Alves, E.S.; Lemos, V.A.; Schwingel, P.A.; da Silva, A.; Vital, R.; Vieira, A.S.; Barreto, M.M.; Rocha, E.A.; Tufik, S.; et al. Assessment of body composition and sport performance of brazilian paralympic swim team athletes. J. Sport Rehabil. 2016, 25, 364–370. [Google Scholar] [CrossRef]
- Flueck, J.L. Body composition in Swiss elite wheelchair athletes. Front. Nutr. 2020, 7, 111. [Google Scholar] [CrossRef]
- Laughton, G.E.; Buchholz, A.C.; Martin Ginis, K.A.; Goy, R.E.; SHAPE SCI Research Group. Lowering body mass index cutoffs better identifies obese persons with spinal cord injury. Spinal. Cord. 2009, 47, 757–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durkin, J.L.; Dowling, J.J. Analysis of body segment parameter differences between four human populations and the estimation errors of four popular mathematical models. J. Biomech. Eng. 2003, 125, 515–522. [Google Scholar] [CrossRef] [PubMed]
- Bober, T.; Zawadzki, J. The Biomechanics of Human Musculoskeletal System, 2nd ed.; University School of Physical Education in Wroclaw: Wroclaw, Poland, 2003. [Google Scholar]
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.I.; Vale, B.S.; Lemos, C.C.; Torres, M.R.; Bregman, R. Body adiposity index assess body fat with high accuracy in nondialyzed chronic kidney disease patients. Obesity 2013, 21, 546–552. [Google Scholar] [CrossRef]
- Carpio-Rivera, E.; Hernández-Elizondo, J.; Salicetti-Fonseca, A.; Solera-Herrera, A.; Moncada-Jiménez, J. Predictive validity of the body adiposity index in costa rican students. Am. J. Hum. Biol. 2016, 28, 394–397. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, M.S.; Santos, C.A.D.; Silva, D.A.S.; Amorim, P.R.D.S.; Marins, J.C.B.; Franceschini, S.D.C.C. Validity of the Body Adiposity Index in Predicting Body Fat in Adults: A Systematic Review. Adv. Nutr. 2018, 9, 617–624. [Google Scholar] [CrossRef]
- Zwierzchowska, A.; Głowacz, M.; Maszczyk, A.; Zając, A. Body adiposity index a better marker of body fat than body mass index in wheelchair rugby players after cervical spinal cord injury (CSCI)—Preliminary investigations. Integr. Obesity Diabetes 2015, 1, 112–116. [Google Scholar] [CrossRef] [Green Version]
- Dingley, A.A.; Pyne, D.B.; Burkett, B. Relationships between propulsion and anthropometry in paralympic swimmers. Int. J. Sports Physiol. Perform. 2015, 10, 978–985. [Google Scholar] [CrossRef]
- Juzwiak, C.R.; Winckler, C.; Joaquim, D.P.; Silva, A.; De Mello, M.T. Comparison of measured and predictive values of basal metabolic rate in brazilian paralympic track and field athletes. Int. J. Sport Nutr. Exerc. Metab. 2016, 26, 330–337. [Google Scholar] [CrossRef]
- Willems, A.; Thomas, T.A.; Keil, M.; Brooke-Wavell, K.; Goosey-Tolfrey, V.L. Dual-energy X-ray absorptiometry, skinfold thickness, and waist circumference for assessing body composition in ambulant and non-ambulant wheelchair games players. Front. Physiol. 2015, 6, 356. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keil, M.; de Totosy Zepetnek, J.O.; Brooke-Wavell, K.; Goosey-Tolfrey, V.L. Measurement precision of body composition variables in elite wheelchair athletes, using dual-energy X-ray absorptiometry. Eur. J. Sport Sci. 2016, 16, 65–71. [Google Scholar] [CrossRef] [PubMed]
- WHO. Waist Circumference and Waist-Hip Ratio; Report of a WHO Expert Consultation Geneva; WHO: Geneva, Switzeland, 2008. [Google Scholar]
- WHO. The Challenge of Obesity in the WHO European Region and the Strategies for Response; WHO: Geneva, Switzeland, 2007. [Google Scholar]
- Rajan, S.; McNeely, M.J.; Warms, C.; Goldstein, B. Clinical assessment and management of obesity in individuals with spinal cord injury: A review. J. Spinal. Cord. Med. 2008, 31, 361–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagai, M.; Komiya, H.; Mori, Y.; Ohta, T.; Kasahara, Y.; Ikeda, Y. Development of a new method for estimating visceral fat area with multi-frequency bioelectrical impedance. Tohoku J. Exp. Med. 2008, 214, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shoji, K.; Maeda, K.; Nakamura, T.; Funahashi, T.; Matsuzawa, Y.; Shimomura, I. Measurement of visceral fat by abdominal bioelectrical impedance analysis is beneficial in medical checkup. Obes. Res. Clin. Pract. 2008, 2, 269–275. [Google Scholar] [CrossRef]
- Beltrán-Carrillo, V.J.; Megías, Á.; González-Cutre, D.; Jiménez-Loaisa, A. Elements behind sedentary lifestyles and unhealthy eating habits in individuals with severe obesity. Int. J. Qual. Stud. Health Well-Being 2022, 17, 2056967. [Google Scholar] [CrossRef]
- Cavedon, V.; Zancanaro, C.; Milanese, C. Body composition assessment in athletes with physical impairment who have been practicing a wheelchair sport regularly and for a prolonged period. Disabil. Health J. 2020, 13, 100933. [Google Scholar] [CrossRef]
- Romanov, R.; Medovic, B.; Stupar, D.; Jezdimirovic, T.; Garunovic, B. The Connection between Certain Morphological Parameters and Results in Goalball Players. Int. J. Morphol. 2017, 35, 1396–1402. [Google Scholar] [CrossRef] [Green Version]
- Sutton, L.; Wallace, J.; Goosey-Tolfrey, V.; Scott, M.; Reilly, T. Body composition of female wheelchair athletes. Int. J. Sports Med. 2009, 30, 259–265. [Google Scholar] [CrossRef]
- Granados, C.; Yanci, J.; Badiola, A.; Iturricastillo, A.; Otero, M.; Olasagasti, J.; Bidaurrazaga-Letona, I.; Gil, S.M. Anthropometry and Performance in Wheelchair Basketball. J. Strength Cond. Res. 2015, 29, 1812–1820. [Google Scholar] [CrossRef]
- Cavedon, V.; Zancanaro, C.; Milanese, C. Anthropometry, Body Composition, and Performance in Sport-Specific Field Test in Female Wheelchair Basketball Players. Front. Physiol. 2018, 9, 568. [Google Scholar] [CrossRef] [PubMed]
- Goosey-Tolfrey, V.; Keil, M.; Brooke-Wavell, K.; de Groot, S. A Comparison of Methods for the Estimation of Body Composition in Highly Trained Wheelchair Games Players. Int. J. Sports Med. 2016, 37, 799–806. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Group | Mean Age (sd) [Year] | Mean Time from Injury (sd) [Year] |
|---|---|---|
| CSCI (n = 10) | 32.8 (4.5) | 11 (5.5) |
| PTF (n = 8) | 36.6 (10.6) | 15.3 (14.5) |
| SV (n = 15) | 32.8 (8.4) | 19.2 (12.1) |
| WR (n = 25) | 32.3 (5.2) | 12.3 (5.1) |
| CSCI | Sitting Volleyball Players | Para Track and Field Athletes | Rugby Players | |
|---|---|---|---|---|
| BM | ||||
| CSCI | - | 0.37 | 0.32 | 1.0 |
| Sitting volleyball players | 0.37 | - | 0.0008 | 0.17 |
| Para track and field athletes | 0.32 | 0.0008 | - | 0.15 |
| Rugby players | 1.0 | 0.17 | 0.15 | - |
| BH | ||||
| CSCI | - | 0.32 | 1.0 | 1.0 |
| Sitting volleyball players | 0.32 | - | 0.34 | 0.38 |
| Para track and field athletes | 1.0 | 0.34 | - | 1.0 |
| Rugby players | 1.0 | 0.38 | 1.0 | - |
| WC | ||||
| CSCI | - | 1.0 | 0.001 | 1.0 |
| Sitting volleyball players | 1.0 | - | 0.0007 | 1.0 |
| Para track and field athletes | 0.001 | 0.0007 | - | 0.001 |
| Rugby players | 1.0 | 1.0 | 0.001 | - |
| HC | ||||
| CSCI | - | 0.7 | 0.9 | 0.8 |
| Sitting volleyball players | 0.7 | - | 0.001 | |
| Para track and field athletes | 0.9 | 0.02 | - | 1.0 |
| Rugby players | 0.8 | 0.001 | 1.0 | - |
| CSCI | Sitting Volleyball Players | Para Track and Field Athletes | Rugby Players | |
|---|---|---|---|---|
| BMI | ||||
| CSCI | - | 1.0 | 0.2 | 1.0 |
| Sitting volleyball players | 1.0 | - | 0.004 | 0.4 |
| Para track and field athletes | 0.2 | 0.004 | - | 0.15 |
| Rugby players | 1.0 | 0.4 | 0.15 | - |
| BMIcor | ||||
| CSCI | - | 0.1 | 0.3 | 1.0 |
| Sitting volleyball players | 0.1 | - | 0.00008 | 0.005 |
| Para track and field athletes | 0.3 | 0.00008 | - | 0.3 |
| Rugby players | 1.0 | 0.005 | 0.3 | - |
| BAI | ||||
| CSCI | - | 1.0 | 1.0 | 0.9 |
| Sitting volleyball players | 1.0 | - | 0.5 | 0.08 |
| Para track and field athletes | 1.0 | 0.5 | - | 1.0 |
| Rugby players | 0.9 | 0.08 | 1.0 | - |
| CSCI | Sitting Volleyball Players | Para Track and Field Athletes | Rugby Players | |
|---|---|---|---|---|
| %FT | ||||
| CSCI | - | 0.37 | 0.32 | 1.0 |
| Sitting volleyball players | 0.37 | - | 0.0008 | 0.17 |
| Para track and field athletes | 0.32 | 0.0008 | - | 0.15 |
| Rugby players | 1.0 | 0.17 | 0.15 | - |
| VFR | ||||
| CSCI | - | 0.32 | 1.0 | 1.0 |
| Sitting volleyball players | 0.32 | - | 0.34 | 0.38 |
| Para track and field athletes | 1.0 | 0.34 | - | 1.0 |
| Rugby players | 1.0 | 0.38 | 1.0 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zwierzchowska, A.; Rosołek, B.; Sikora, M.; Celebańska, D. Forced Sedentariness and Sports Activity as Factors Differentiating Anthropometric Characteristics, Indices, and Body Composition in People with Disabilities. Biology 2022, 11, 906. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060906
Zwierzchowska A, Rosołek B, Sikora M, Celebańska D. Forced Sedentariness and Sports Activity as Factors Differentiating Anthropometric Characteristics, Indices, and Body Composition in People with Disabilities. Biology. 2022; 11(6):906. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060906
Chicago/Turabian StyleZwierzchowska, Anna, Barbara Rosołek, Marcin Sikora, and Diana Celebańska. 2022. "Forced Sedentariness and Sports Activity as Factors Differentiating Anthropometric Characteristics, Indices, and Body Composition in People with Disabilities" Biology 11, no. 6: 906. https://0-doi-org.brum.beds.ac.uk/10.3390/biology11060906