
Glatiramer Acetate Treatment in Multiple Sclerosis-Associated Fatigue—Beneficial Effects on Self-Assessment Scales But Not on Molecular Markers

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Is fatigue one of your three most disabling symptoms?
- Does fatigue occur daily or on most days?
- Does fatigue affect your activities at home or at work?
2.2. Clinical Parameters
2.3. Immunological Parameters
- Cytokines: interleukin (IL)-4, IL-6, IL-12, IL-17, IFN gamma, tumor necrosis factor (TNF) alpha;
- Chemokines: CCL7, CXCL9, CXCL12;
- Neurotrophic factors: leukemia inhibitory factor (LIF), ciliary neurotrophic factor (CNTF), brain derived neurotrophic factor (BDNF), insulin-like growth factor 1 (IGF1), metallothionin-3 (MT3).
2.4. Neuropsychological Parameters
2.5. Statistical Analysis
3. Results
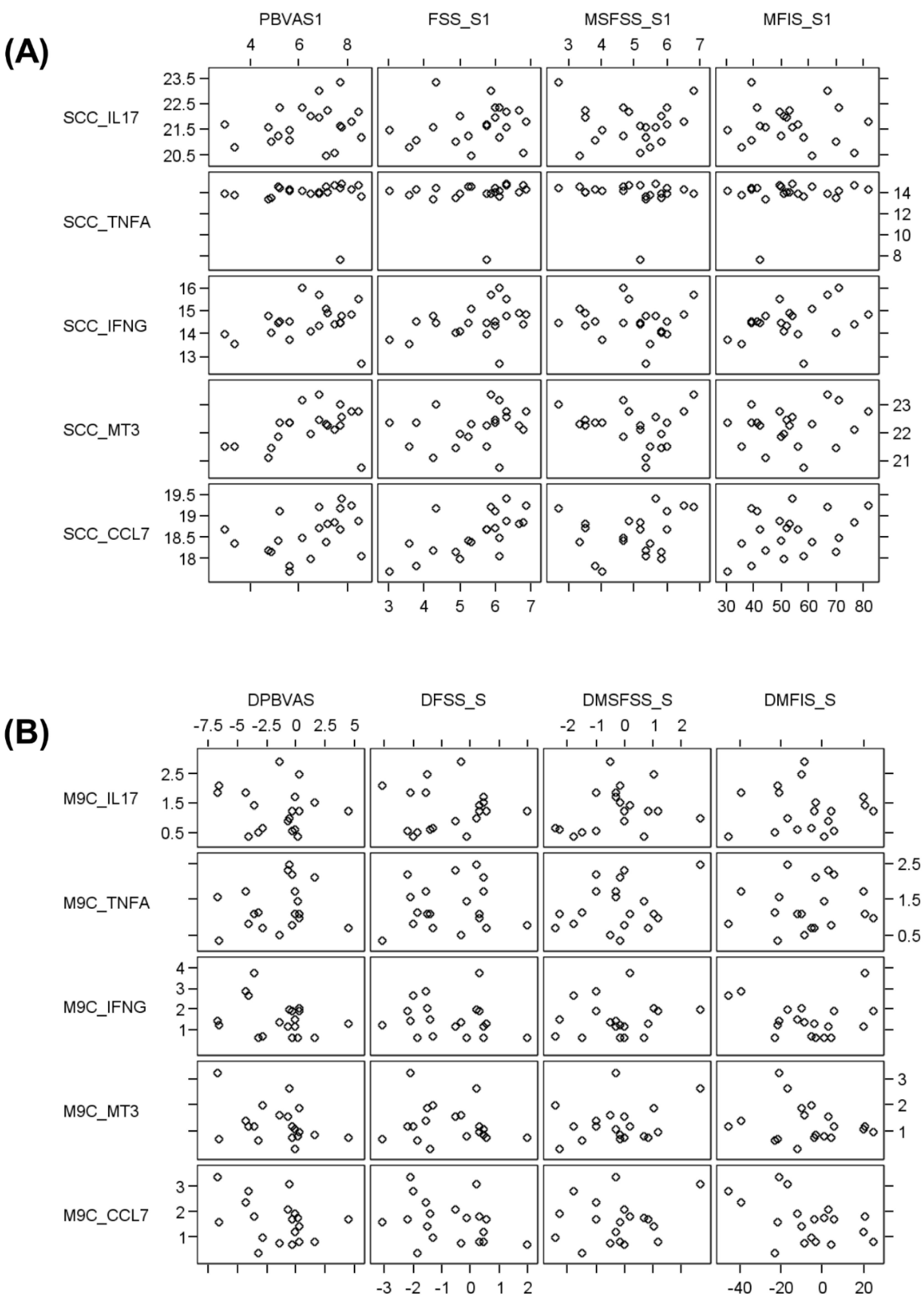
3.1. GA Did Not Exhibit Significant Effects on the mRNA Level
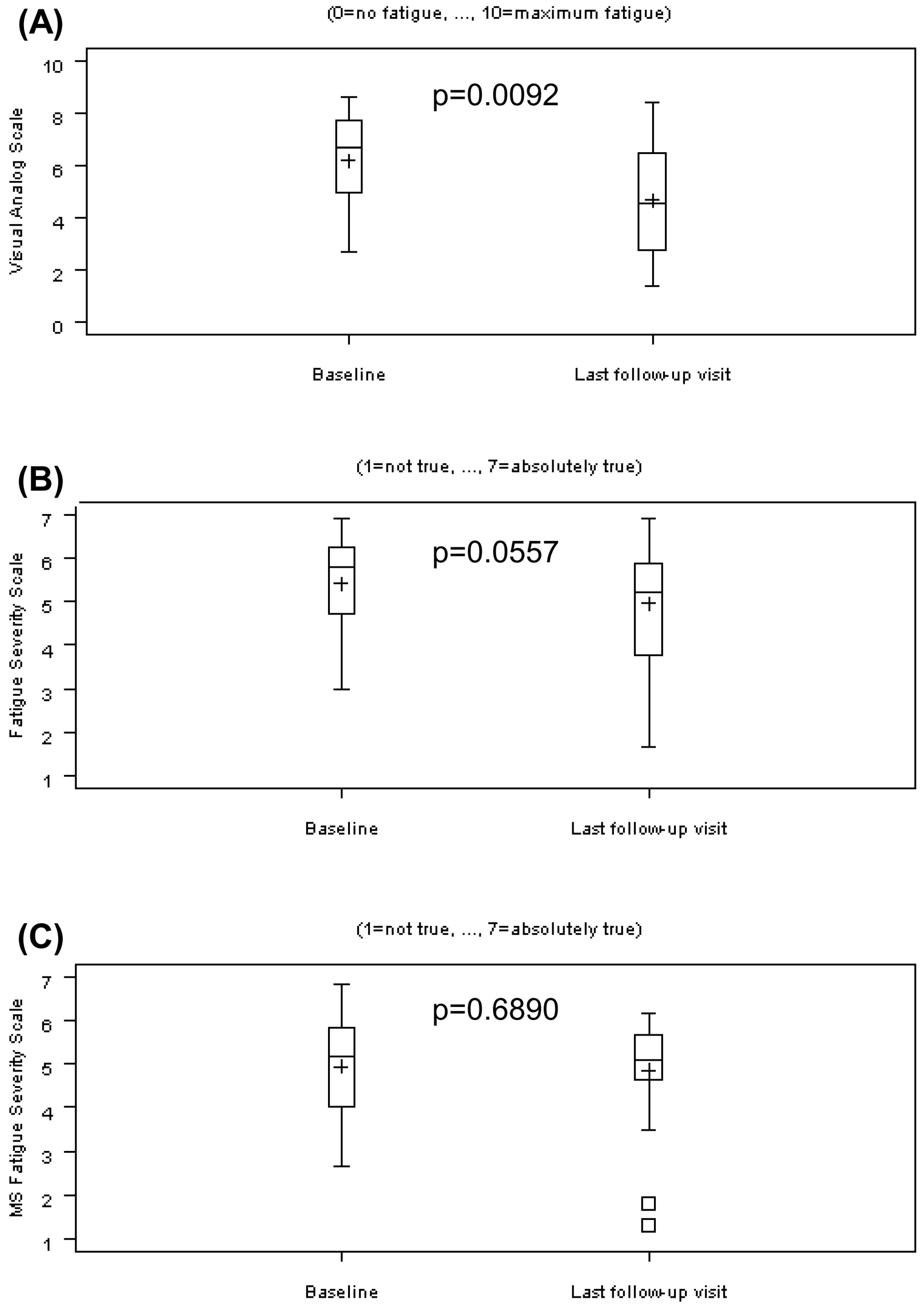
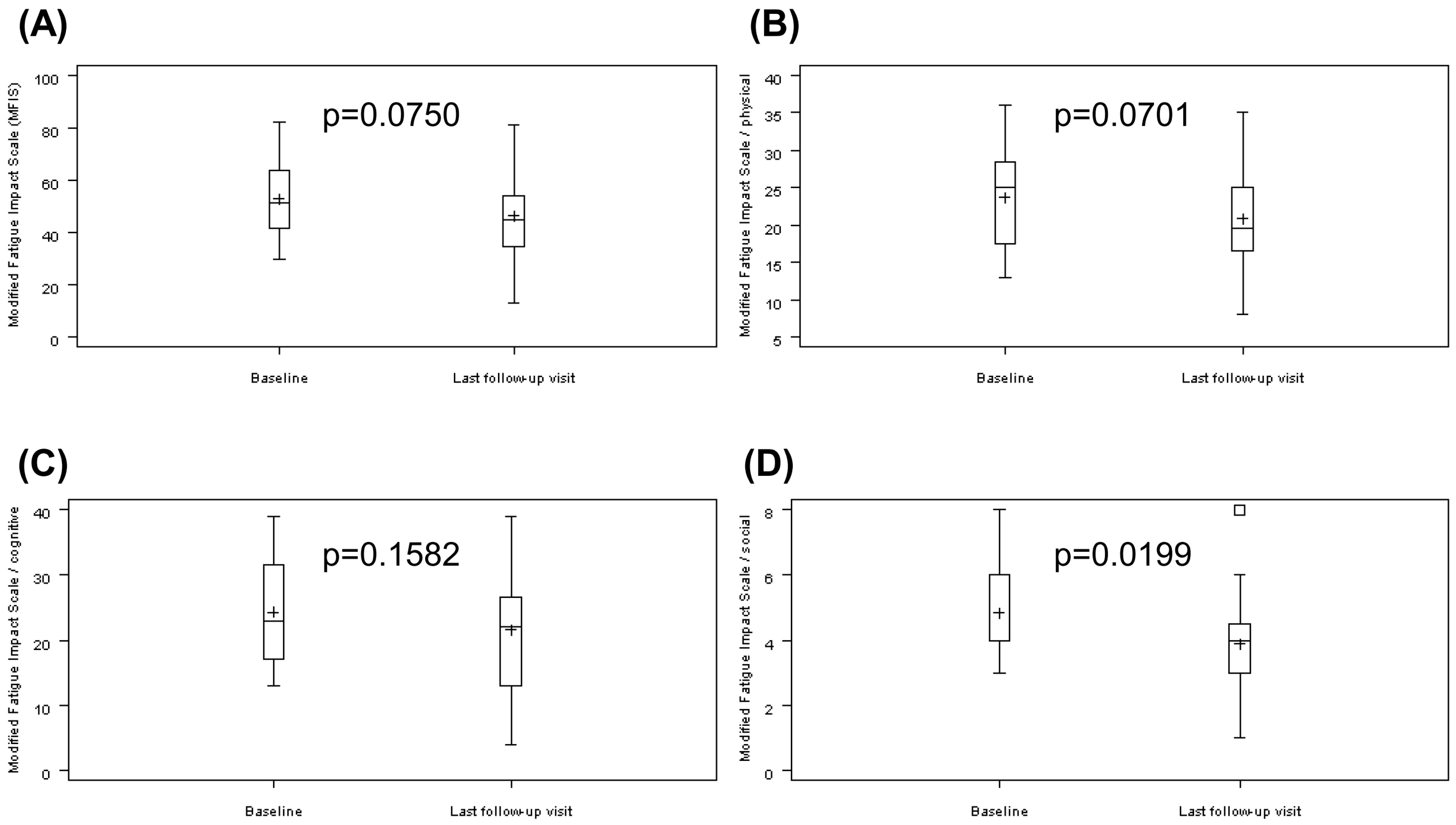
3.2. GA Partially Improved Fatigue Self-Assessments
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Pajtedl, R.; Penner, I.K.; Noack, T.K.; Zettl, U.K. Multiple sclerosis and fatigue: A review on the contribution of inflammation and immune-mediated neurodegeneration. Autoimmun. Rev. 2016, 15, 210–220. [Google Scholar]
- Rommer, P.S.; Eichstädt, K.; Ellenberger, D.; Flachenecker, P.; Friede, T.; Haas, J.; Kleinschnitz, C.; Pöhlau, D.; Rienhoff, O.; Stahmann, A.; et al. Symptomatology and symptomatic treatment in multiple sclerosis: Results from a nationwide MS registry. Mult. Scler. 2019, 25, 1641–1652. [Google Scholar] [CrossRef] [PubMed]
- Mortezanejad, M.; Ehsani, F.; Masoudian, N.; Zoghi, M.; Jaberzadeh, S. Comparing the effects of multi-session anodal trans-cranial direct current stimulation of primary motor and dorsolateral prefrontal cortices on fatigue and quality of life in patients with multiple sclerosis: A double-blind, randomized, sham-controlled trial. Clin. Rehabil. 2020. [Google Scholar] [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reich, D.S.; Lucchinetti, C.F.; Calabresi, P.A. Multiple sclerosis. N. Engl. J. Med. 2018, 378, 169–180. [Google Scholar] [CrossRef]
- Tartaglia, M.C.; Narayanan, S.; Francis, S.J.; Santos, A.C.; De Stefano, N.; Lapierre, Y.; Arnold, D.L. The relationship between diffuse axonal damage and fatigue in multiple sclerosis. Arch. Neurol. 2004, 61, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rottoli, M.; La Gioia, S.; Frigeni, B.; Barcella, V. Pathophysiology, assessment and management of multiple sclerosis fatigue: An update. Exp. Rev. Neurother. 2017, 17, 373–379. [Google Scholar] [CrossRef]
- Huth, T.K.; Eaton-Fitch, N.; Staines, D.; Marshall-Gradisnik, S. A systematic review of metabolomic dysregulation in chronic fatigue syndrome/myalgic encephalomyelitis/systemic exertion intolerance disease (CFS/ME/SEID). J. Transl. Med. 2020. [Google Scholar] [CrossRef]
- Specogna, I.; Casagrande, F.; Lorusso, A.; Catalan, M.; Gorian, A.; Zugna, L.; Longo, R.; Zorzon, M.; Naccarato, M.; Pizzolato, G.; et al. Functional MRI during the execution of a motor task in patients with multiple sclerosis and fatigue. Radiol. Med. 2012, 117, 1398–1407. [Google Scholar] [CrossRef]
- Maksoud, R.; Du Preez, S.; Eaton-Fitch, N.; Thapaliya, K.; Barnden, L.; Cabanas, H.; Staines, D.; Marshall-Gradisnik, S. A systematic review of neurological impairments in myalgic encephalomyelitis/chronic fatigue syndrome using neuroimaging techniques. PLoS ONE 2020, 15, e0232475. [Google Scholar] [CrossRef]
- Flachenecker, P.; Bihler, I.; Weber, F.; Gottschalk, M.; Toyka, K.V.; Rieckmann, P. Cytokine mRNA expression in patients with multiple sclerosis and fatigue. Mult. Scler. 2004, 10, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Stoppe, M.; Meyer, K.; Schlingmann, M.; Olbrich, S.; Then Bergh, F. Hyperstable arousal regulation in multiple sclerosis. Psychoneuroendocrinology 2019, 110. [Google Scholar] [CrossRef] [PubMed]
- Gottschalk, M.; Kümpfel, T.; Flachenecker, P.; Uhr, M.; Trenkwalder, C.; Holsboer, F.; Weber, F. Fatigue and regulation of the hypothalamo-pituitary-adrenal axis in multiple sclerosis. Arch. Neurol. 2005, 62, 277–280. [Google Scholar] [CrossRef]
- Schmidt, E.; Schinke, C.; Rullmann, M.; Luthardt, J.; Becker, G.-A.; Haars, S.; Stoppe, M.; Lobsien, D.; Hoffmann, K.-T.; Sabri, O.; et al. Changes of central noradrenaline transporter availability in immunotherapy-naïve multiple sclerosis patients. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Rammohan, K.W.; Rosenberg, J.H.; Lynn, D.J.; Blumenfeld, A.M.; Pollak, C.P.; Nagaraja, H.N. Efficacy and safety of modafinil (Provigil) for the treatment of fatigue in multiple sclerosis: A to centre phase 2 study. J. Neurol. Neurosurg. Psychiatry 2002, 72, 179–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupp, L.; LaRocca, N.; Muir-Nash, J.; Steinberg, A. The fatigue severity scale: Applications to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Krupp, L.B.; Coyle, P.K.; Doscher, C.; Miller, A.; Cross, A.H.; Jandorf, L.; Halper, J.; Johnson, B.; Morgante, L.; Grimson, R. Fatigue therapy in multiple sclerosis: Results of a double-blind, randomized, parallel trial of amantadine, pemoline, and placebo. Neurology 1995, 45, 1956–1961. [Google Scholar] [CrossRef] [PubMed]
- Fisk, J.D.; Ritvo, P.G.; Ross, L.; Haase, D.A.; Marrie, T.J.; Schlech, W.F. Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clin. Infect. Dis. 1994, 18 (Suppl. 1), S79–S83. [Google Scholar] [CrossRef] [PubMed]
- Zifko, U.A. Management of fatigue in patients with multiple sclerosis. Drugs 2004, 64, 1295–1304. [Google Scholar] [CrossRef] [PubMed]
- Wendebourg, M.J.; Heesen, C.; Finlayson, M.; Meyer, B.; Pöttgen, J.; Köpke, S. Patient education for people with multiple sclerosis-associated fatigue: A systematic review. PLoS ONE 2017. [Google Scholar] [CrossRef] [PubMed]
- Kotterba, S.; Neusser, T.; Norenberg, C.; Bussfeld, P.; Glaser, T.; Dörner, M.; Schürks, M. Sleep quality, daytime sleepiness, fatigue, and quality of life in patients with multiple sclerosis treated with interferon beta-1b: Results from a prospective observational cohort study. BMC Neurol. 2018, 18. [Google Scholar] [CrossRef] [PubMed]
- Sater, R.A.; Gudesblatt, M.; Kresa-Reahl, K.; Brandes, D.W.; Sater, P. NAPS-MS: Natalizumab effects on parameters of sleep in patients with multiple sclerosis. Int. J. MS Care 2016, 18, 177–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ozel, O.; Vaughn, C.B.; Eckert, S.; Jakimovski, D.; Lizarraga, A.A.; Weinstock-Guttman, B. Dimethyl fumarate in the treatment of relapsing-remitting multiple sclerosis: Patient reported outcomes and perspectives. Patient Relat. Outcome Meas. 2019, 10, 373–384. [Google Scholar] [CrossRef] [Green Version]
- Kunkel, A.; Fischer, M.; Faiss, J.; Dähne, D.; Köhler, W.; Faiss, J.H. Impact of natalizumab treatment on fatigue, mood, and aspects of cognition in relapsing-remitting multiple sclerosis. Front. Neurol. 2015, 11. [Google Scholar] [CrossRef] [Green Version]
- Johnson, K.P.; Brooks, B.R.; Cohen, J.A.; Ford, C.C.; Goldstein, J.; Lisak, R.P.; Myers, L.W.; Panitch, H.S.; Rose, J.W.; Schiffer, R.B.; et al. Copolymer 1 reduces relapse rate and improves disability in relapsing-remitting multiple sclerosis: Results of a phase III multicenter, double-blind placebo-controlled trial. The Copolymer 1 Multiple Sclerosis Study Group. Neurology 1995, 45, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Moiola, L.; Rommer, P.S.; Zettl, U.K. Prevention and management of adverse effects of disease modifying treatments in multiple sclerosis. Curr. Opin. Neurol. 2020, 33, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Teitelbaum, D.; Arnon, R.; Sela, M. Copolymer 1: From basic research to clinical application. Cell. Mol. Life Sci. 1997, 53, 24–28. [Google Scholar] [CrossRef]
- Neuhaus, O.; Farina, C.; Yassouridis, A.; Wiendl, H.; Then Bergh, F.; Dose, T.; Wekerle, H.; Hohlfeld, R. Multiple sclerosis: Comparison of copolymer-1-reactive T cell lines from treated and untreated subjects reveals cytokine shift from T helper 1 to T helper 2 cells. Proc. Natl. Acad. Sci. USA 2000, 97, 7452–7457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ziemssen, T.; Kümpfel, T.; Klinkert, W.E.; Neuhaus, O.; Hohlfeld, R. Glatiramer acetate-specific T-helper 1- and 2-type cell lines produce BDNF: Implications for multiple sclerosis therapy. Brain 2002, 125, 2381–2391. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metz, L.M.; Patten, S.B.; Archibald, C.J.; Bakker, J.I.; Harris, C.J.; Patry, D.G.; Bell, R.B.; Yeung, M.; Murphy, W.F.; Stoian, C.A.; et al. The effect of immunomodulatory treatment on multiple sclerosis fatigue. J. Neurol. Neurosurg. Psychiatry 2004, 75, 1045–1047. [Google Scholar] [CrossRef] [Green Version]
- Flachenecker, P.; Kümpfel, T.; Kallmann, B.; Gottschalk, M.; Grauer, O.; Rieckmann, P.; Trenkwalder, C.; Toyka, K.V. Fatigue in multiple sclerosis: A comparison of different rating scales and correlation to clinical parameters. Mult. Scler. 2002, 8, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Greeke, E.E.; Chua, A.S.; Healy, B.C.; Rintell, D.J.; Chitnis, T.; Glanz, B.I. Depression and fatigue in patients with multiple sclerosis. J. Neurol. Sci. 2017, 380, 236–241. [Google Scholar] [CrossRef] [PubMed]
- Beck, A.T.; Ward, C.H.; Mendelson, M.; Mock, J.; Erbaugh, J. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cepok, S.; Schreiber, H.; Hoffmann, S.; Zhou, D.; Neuhaus, O.; Von Geldern, G.; Hochgesand, S.; Nessler, S.; Rothhammer, V.; Lang, M.; et al. Enhancement of chemokine expression by interferon beta therapy in patients with multiple sclerosis. Arch. Neurol. 2009, 66, 1216–1223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malekzadeh, A.; Van de Geer-Peeters, W.; De Groot, V.; Teunissen, C.E.; Beckerman, H.; TREFAMS-ACE Study Group. Fatigue in patients with multiple sclerosis: Is it related to pro- and anti-inflammatory cytokines? Dis. Markers 2015. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Parameter | Baseline Visit | Last Follow-Up Visit |
|---|---|---|
| Age (years) | 41.9 ± 8.0 (22.5–55.4) | |
| Gender | f:m = 80:20 | |
| Time since diagnosis (months) | 56.8 ± 69.3 (0.4–270.6) | |
| Number of relapses since diagnosis | 4.8 ± 4.3 | |
| Number of relapses in previous 2 years | 1.8 ± 1.0 | |
| Number of relapses during therapy | 0.7 ± 0.7 | |
| Annualized relapse rate | 0.9 | 0.8 (n.s.) |
| EDSS | 2.4 ± 1.1 (1.0–4.5) | 2.5 ± 0.9 (1.0–4.0, n.s.) |
| BDI | 10.6 ± 4.7 (1–16) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Neuhaus, O.; Köhler, W.; Then Bergh, F.; Kristoferitsch, W.; Faiss, J.; Rosenkranz, T.; Reske, D.; Patejdl, R.; Hartung, H.-P.; Zettl, U.K. Glatiramer Acetate Treatment in Multiple Sclerosis-Associated Fatigue—Beneficial Effects on Self-Assessment Scales But Not on Molecular Markers. Biomolecules 2021, 11, 393. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11030393
Neuhaus O, Köhler W, Then Bergh F, Kristoferitsch W, Faiss J, Rosenkranz T, Reske D, Patejdl R, Hartung H-P, Zettl UK. Glatiramer Acetate Treatment in Multiple Sclerosis-Associated Fatigue—Beneficial Effects on Self-Assessment Scales But Not on Molecular Markers. Biomolecules. 2021; 11(3):393. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11030393
Chicago/Turabian StyleNeuhaus, Oliver, Wolfgang Köhler, Florian Then Bergh, Wolfgang Kristoferitsch, Jürgen Faiss, Thorsten Rosenkranz, Dirk Reske, Robert Patejdl, Hans-Peter Hartung, and Uwe K. Zettl. 2021. "Glatiramer Acetate Treatment in Multiple Sclerosis-Associated Fatigue—Beneficial Effects on Self-Assessment Scales But Not on Molecular Markers" Biomolecules 11, no. 3: 393. https://0-doi-org.brum.beds.ac.uk/10.3390/biom11030393