
Chronic Nicotine Exposure Increases Hematoma Expansion following Collagenase-Induced Intracerebral Hemorrhage in Rats

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Animals
2.2. Nicotine Administration
2.3. Determination of the Stage of the Estrous Cycle
2.4. sICH Induction
2.5. Neurological Score Assessment
2.6. Animal Perfusion and Brain Isolation
2.7. Quantification of Hematoma Volume
2.8. Experimental Protocol
2.9. Collagenase Activity Assay
2.10. Statistical Analysis
3. Results
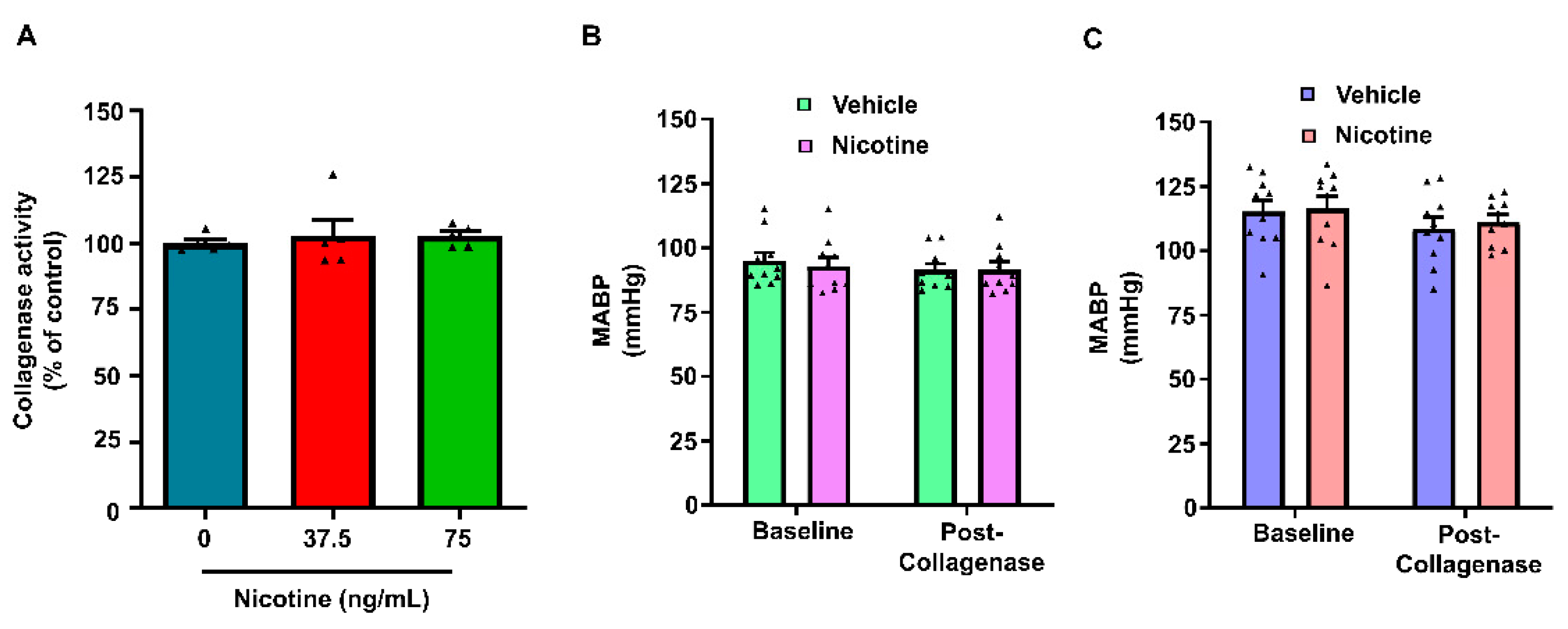
3.1. Physiological Parameters
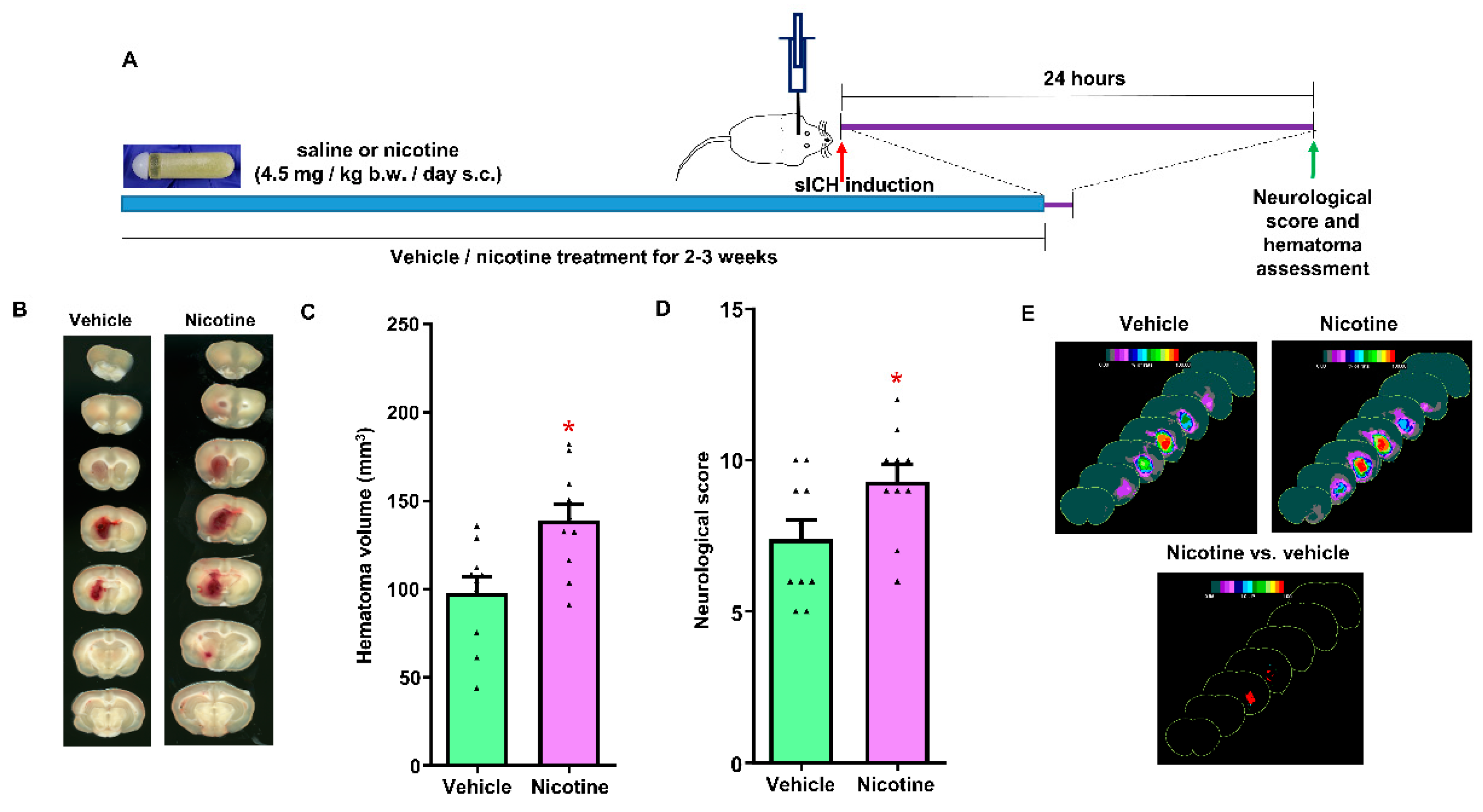
3.2. The Effect of Chronic Nicotine Exposure on Hematoma Growth following sICH in Young Male Rats
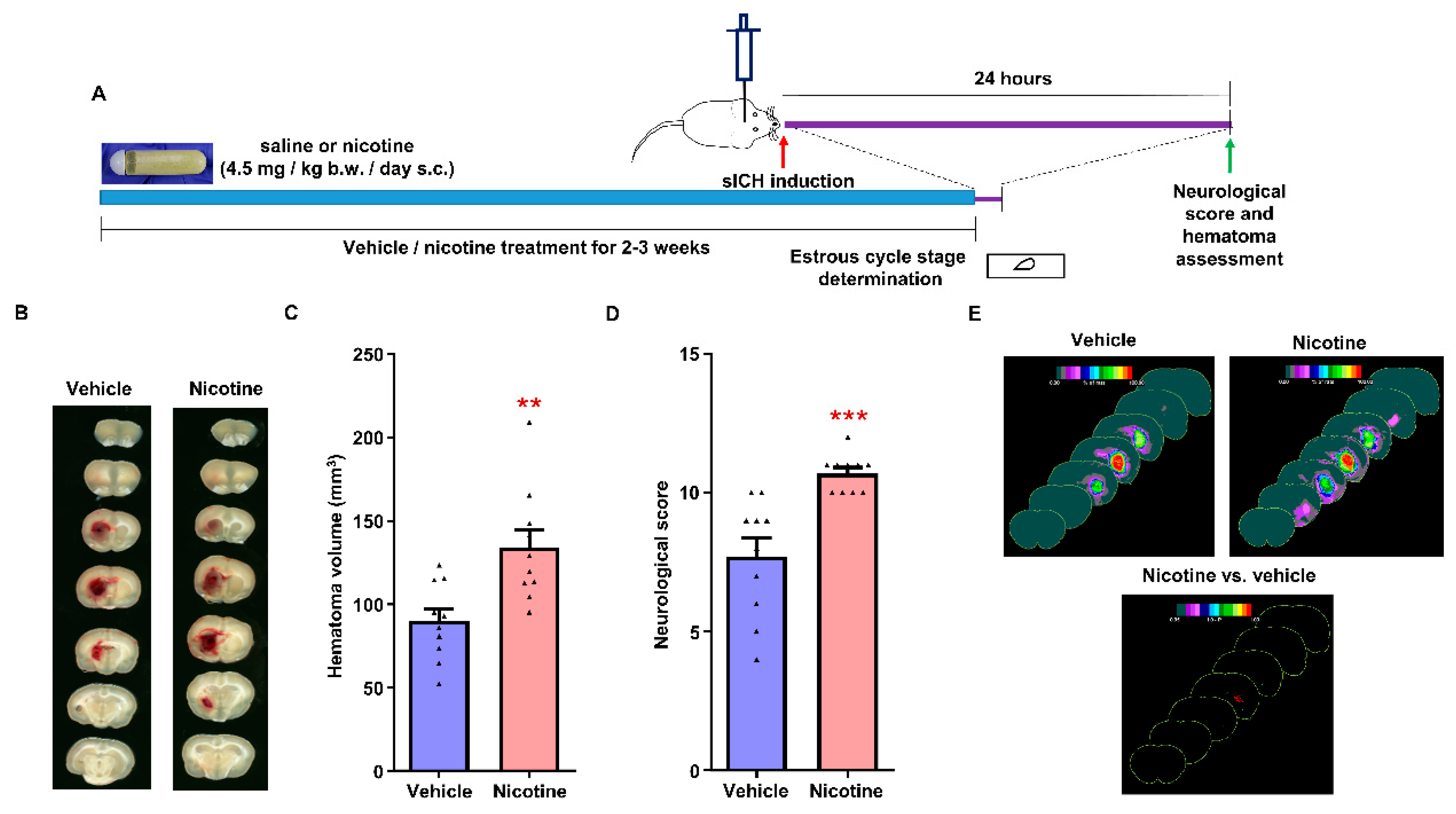
3.3. The Effect of Chronic Nicotine Exposure on Hematoma Growth following sICH in Female Rats
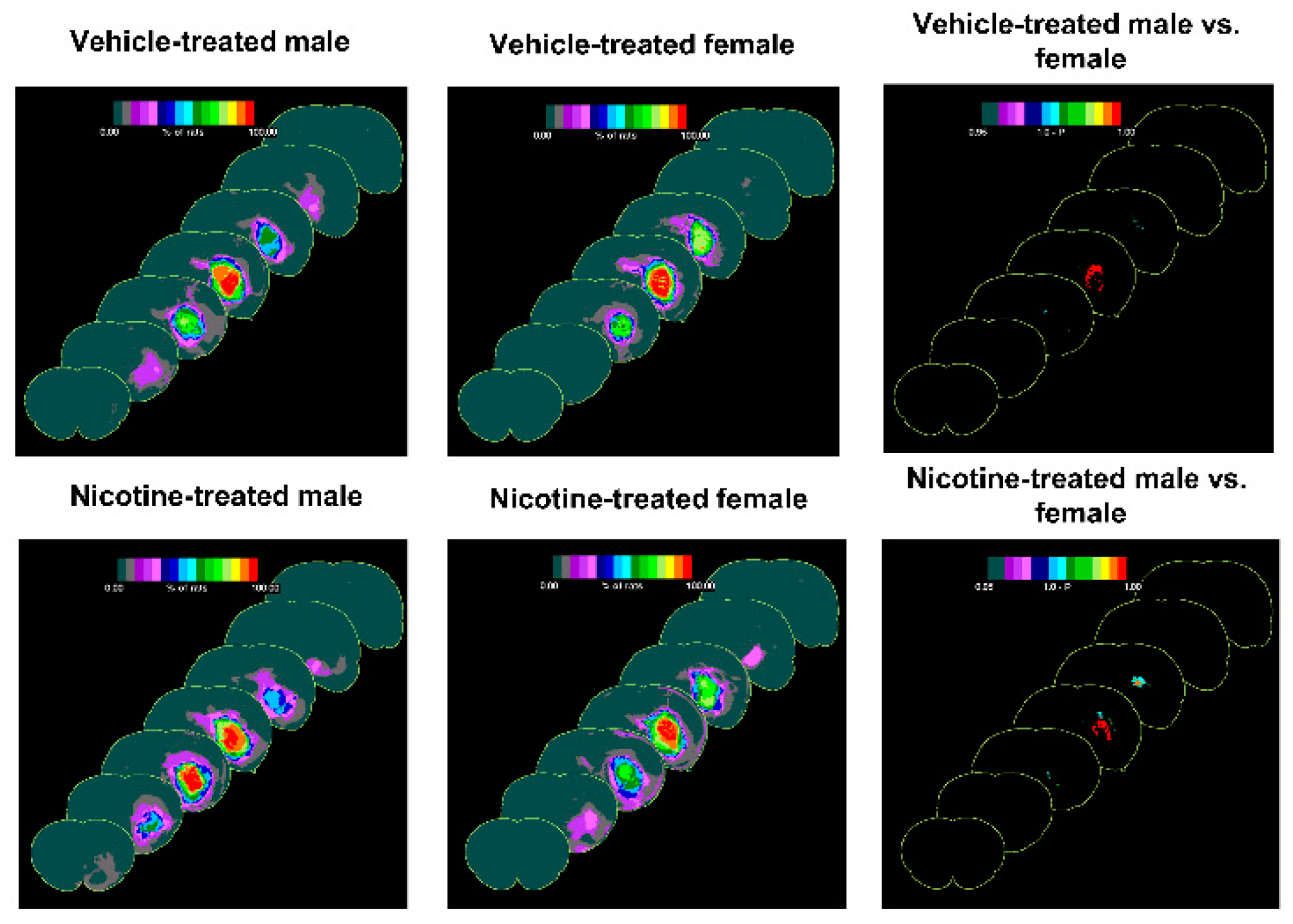
3.4. The Difference of the Effect of Treatments on Outcome following sICH in Male and Female Rats
3.5. The Effect of Nicotine on Collagenase Activity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sacco, R.L.; Kasner, S.E.; Broderick, J.P.; Caplan, L.R.; Connors, J.J.; Culebras, A.; Elkind, M.S.; George, M.G.; Hamdan, A.D.; Higashida, R.T.; et al. An updated definition of stroke for the 21st century: A statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2013, 44, 2064–2089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef]
- Dennis, M.S.; Burn, J.P.; Sandercock, P.A.; Bamford, J.M.; Wade, D.T.; Warlow, C.P. Long-term survival after first-ever stroke: The Oxfordshire Community Stroke Project. Stroke 1993, 24, 796–800. [Google Scholar] [CrossRef] [Green Version]
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Khoury, J.; Moomaw, C.J.; Alwell, K.; Woo, D.; Flaherty, M.L.; Khatri, P.; Adeoye, O.; Ferioli, S.; Broderick, J.P.; et al. Stroke incidence is decreasing in whites but not in blacks: A population-based estimate of temporal trends in stroke incidence from the Greater Cincinnati/Northern Kentucky Stroke Study. Stroke 2010, 41, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- van Asch, C.J.; Luitse, M.J.; Rinkel, G.J.; van der Tweel, I.; Algra, A.; Klijn, C.J. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 167–176. [Google Scholar] [CrossRef]
- Davis, S.M.; Broderick, J.; Hennerici, M.; Brun, N.C.; Diringer, M.N.; Mayer, S.A.; Begtrup, K.; Steiner, T. Hematoma growth is a determinant of mortality and poor outcome after intracerebral hemorrhage. Neurology 2006, 66, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, M.J.; Xavier, D.; Liu, L.; Zhang, H.; Chin, S.L.; Rao-Melacini, P.; Rangarajan, S.; Islam, S.; Pais, P.; McQueen, M.J.; et al. Risk factors for ischaemic and intracerebral haemorrhagic stroke in 22 countries (the INTERSTROKE study): A case-control study. Lancet 2010, 376, 112–123. [Google Scholar] [CrossRef]
- An, S.J.; Kim, T.J.; Yoon, B.W. Epidemiology, Risk Factors, and Clinical Features of Intracerebral Hemorrhage: An Update. J. Stroke 2017, 19, 3–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Virani, S.S.; Alonso, A.; Aparicio, H.J.; Benjamin, E.J.; Bittencourt, M.S.; Callaway, C.W.; Carson, A.P.; Chamberlain, A.M.; Cheng, S.; Delling, F.N.; et al. Heart Disease and Stroke Statistics-2021 Update: A Report From the American Heart Association. Circulation 2021, 143, e254–e743. [Google Scholar] [CrossRef]
- Ariesen, M.J.; Claus, S.P.; Rinkel, G.J.; Algra, A. Risk factors for intracerebral hemorrhage in the general population: A systematic review. Stroke 2003, 34, 2060–2065. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.; Rehni, A.K.; Dave, K.R. Tobacco Use: A Major Risk Factor of Intracerebral Hemorrhage. J. Stroke 2021, 23, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Hauer, A.J.; Ruigrok, Y.M.; Algra, A.; van Dijk, E.J.; Koudstaal, P.J.; Luijckx, G.J.; Nederkoorn, P.J.; van Oostenbrugge, R.J.; Visser, M.C.; Wermer, M.J.; et al. Age-Specific Vascular Risk Factor Profiles According to Stroke Subtype. J. Am. Heart Assoc. 2017, 6, e005090. [Google Scholar] [CrossRef] [PubMed]
- Bateman, B.T.; Schumacher, H.C.; Bushnell, C.D.; Pile-Spellman, J.; Simpson, L.L.; Sacco, R.L.; Berman, M.F. Intracerebral hemorrhage in pregnancy: Frequency, risk factors, and outcome. Neurology 2006, 67, 424–429. [Google Scholar] [CrossRef]
- Nakamura, K.; Barzi, F.; Lam, T.H.; Huxley, R.; Feigin, V.L.; Ueshima, H.; Woo, J.; Gu, D.; Ohkubo, T.; Lawes, C.M.; et al. Cigarette smoking, systolic blood pressure, and cardiovascular diseases in the Asia-Pacific region. Stroke 2008, 39, 1694–1702. [Google Scholar] [CrossRef] [PubMed]
- Faigle, R.; Marsh, E.B.; Llinas, R.H.; Urrutia, V.C.; Gottesman, R.F. Race-Specific Predictors of Mortality in Intracerebral Hemorrhage: Differential Impacts of Intraventricular Hemorrhage and Age Among Blacks and Whites. J. Am. Heart Assoc. 2016, 5, e003540. [Google Scholar] [CrossRef] [Green Version]
- Go, G.O.; Park, H.; Lee, C.H.; Hwang, S.H.; Han, J.W.; Park, I.S. The outcomes of spontaneous intracerebral hemorrhage in young adults—A clinical study. J. Cereb. Endovasc. Neurosurg. 2013, 15, 214–220. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.L.; Burbank, A.D. Cardiovascular toxicity of nicotine: Implications for electronic cigarette use. Trends Cardiovasc. Med. 2016, 26, 515–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murrin, L.C.; Ferrer, J.R.; Zeng, W.Y.; Haley, N.J. Nicotine administration to rats: Methodological considerations. Life Sci. 1987, 40, 1699–1708. [Google Scholar] [CrossRef]
- Raval, A.P.; Hirsch, N.; Dave, K.R.; Yavagal, D.R.; Bramlett, H.; Saul, I. Nicotine and estrogen synergistically exacerbate cerebral ischemic injury. Neuroscience 2011, 181, 216–225. [Google Scholar] [CrossRef]
- Wang, L.; Kittaka, M.; Sun, N.; Schreiber, S.S.; Zlokovic, B.V. Chronic nicotine treatment enhances focal ischemic brain injury and depletes free pool of brain microvascular tissue plasminogen activator in rats. J. Cereb. Blood Flow Metab. 1997, 17, 136–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diaz, F.; Raval, A.P. Simultaneous nicotine and oral contraceptive exposure alters brain energy metabolism and exacerbates ischemic stroke injury in female rats. J. Cereb. Blood Flow Metab. 2021, 41, 793–804. [Google Scholar] [CrossRef]
- Marini, S.; Morotti, A.; Ayres, A.M.; Crawford, K.; Kourkoulis, C.E.; Lena, U.K.; Gurol, E.M.; Viswanathan, A.; Goldstein, J.N.; Greenberg, S.M.; et al. Sex differences in intracerebral hemorrhage expansion and mortality. J. Neurol. Sci. 2017, 379, 112–116. [Google Scholar] [CrossRef]
- Shigematsu, K.; Watanabe, Y.; Nakano, H.; Kyoto Stroke Registry Committee. Lower hazard ratio for death in women with cerebral hemorrhage. Acta Neurol. Scand 2015, 132, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Raval, A.P.; Saul, I.; Dave, K.R.; DeFazio, R.A.; Perez-Pinzon, M.A.; Bramlett, H. Pretreatment with a single estradiol-17beta bolus activates cyclic-AMP response element binding protein and protects CA1 neurons against global cerebral ischemia. Neuroscience 2009, 160, 307–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLellan, C.L.; Silasi, G.; Poon, C.C.; Edmundson, C.L.; Buist, R.; Peeling, J.; Colbourne, F. Intracerebral hemorrhage models in rat: Comparing collagenase to blood infusion. J. Cereb. Blood Flow Metab. 2008, 28, 516–525. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Cho, S.; Rehni, A.K.; Quero, H.N.; Dave, K.R.; Zhao, W. Automated Assessment of Hematoma Volume of Rodents Subjected to Experimental Intracerebral Hemorrhagic Stroke by Bayes Segmentation Approach. Transl. Stroke Res. 2020, 11, 789–798. [Google Scholar] [CrossRef] [PubMed]
- Belayev, L.; Alonso, O.F.; Busto, R.; Zhao, W.; Ginsberg, M.D. Middle cerebral artery occlusion in the rat by intraluminal suture. Neurological and pathological evaluation of an improved model. Stroke 1996, 27, 1616–1623. [Google Scholar] [CrossRef]
- De Ryck, M.; Van Reempts, J.; Borgers, M.; Wauquier, A.; Janssen, P.A. Photochemical stroke model: Flunarizine prevents sensorimotor deficits after neocortical infarcts in rats. Stroke 1989, 20, 1383–1390. [Google Scholar] [CrossRef] [Green Version]
- Tang, X.N.; Berman, A.E.; Swanson, R.A.; Yenari, M.A. Digitally quantifying cerebral hemorrhage using Photoshop and Image J. J. Neurosci. Methods 2010, 190, 240–243. [Google Scholar] [CrossRef] [Green Version]
- Van Wart, H.E.; Steinbrink, D.R. A continuous spectrophotometric assay for Clostridium histolyticum collagenase. Anal. Biochem. 1981, 113, 356–365. [Google Scholar] [CrossRef]
- Malkawi, A.H.; Al-Ghananeem, A.M.; de Leon, J.; Crooks, P.A. Nicotine exposure can be detected in cerebrospinal fluid of active and passive smokers. J. Pharm. Biomed. Anal. 2009, 49, 129–132. [Google Scholar] [CrossRef] [PubMed]
- Koob, G.F.; Le Moal, M. Nicotine. In Neurobiology of Addiction; Koob, G.F., Le Moal, M., Eds.; Elsevier Academic: London, UK, 2006; pp. 243–287. [Google Scholar]
- Jha, P.; Ramasundarahettige, C.; Landsman, V.; Rostron, B.; Thun, M.; Anderson, R.N.; McAfee, T.; Peto, R. 21st-century hazards of smoking and benefits of cessation in the United States. N. Engl. J. Med. 2013, 368, 341–350. [Google Scholar] [CrossRef] [Green Version]
- Villarroel, M.A.; Cha, A.E.; Vahratian, A. Electronic Cigarette Use Among U.S. Adults. Available online: https://www.cdc.gov/nchs/products/databriefs/db365.htm (accessed on 10 July 2021).
- Vindhyal, M.R.; Okut, H.; Ablah, E.; Ndunda, P.M.; Kallail, K.J.; Choi, W.S. Cardiovascular Outcomes Associated with Adult Electronic Cigarette Use. Cureus 2020, 12, e9618. [Google Scholar] [CrossRef] [PubMed]
- Kaisar, M.A.; Villalba, H.; Prasad, S.; Liles, T.; Sifat, A.E.; Sajja, R.K.; Abbruscato, T.J.; Cucullo, L. Offsetting the impact of smoking and e-cigarette vaping on the cerebrovascular system and stroke injury: Is Metformin a viable countermeasure? Redox Biol. 2017, 13, 353–362. [Google Scholar] [CrossRef]
- Benowitz, N.L.; Fraiman, J.B. Cardiovascular effects of electronic cigarettes. Nat. Rev. Cardiol. 2017, 14, 447–456. [Google Scholar] [CrossRef]
- Kurth, T.; Kase, C.S.; Berger, K.; Gaziano, J.M.; Cook, N.R.; Buring, J.E. Smoking and risk of hemorrhagic stroke in women. Stroke 2003, 34, 2792–2795. [Google Scholar] [CrossRef] [Green Version]
- Zhou, J.F.; Wang, J.Y.; Luo, Y.E.; Chen, H.H. Influence of hypertension, lipometabolism disorders, obesity and other lifestyles on spontaneous intracerebral hemorrhage. Biomed. Environ. Sci. 2003, 16, 295–303. [Google Scholar]
- Delcourt, C.; Huang, Y.; Arima, H.; Chalmers, J.; Davis, S.M.; Heeley, E.L.; Wang, J.; Parsons, M.W.; Liu, G.; Anderson, C.S.; et al. Hematoma growth and outcomes in intracerebral hemorrhage: The INTERACT1 study. Neurology 2012, 79, 314–319. [Google Scholar] [CrossRef]
- Kazui, S.; Naritomi, H.; Yamamoto, H.; Sawada, T.; Yamaguchi, T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke 1996, 27, 1783–1787. [Google Scholar] [CrossRef]
- Qureshi, A.I.; Mendelow, A.D.; Hanley, D.F. Intracerebral haemorrhage. Lancet 2009, 373, 1632–1644. [Google Scholar] [CrossRef] [Green Version]
- Csordas, A.; Bernhard, D. The biology behind the atherothrombotic effects of cigarette smoke. Nat. Rev. Cardiol. 2013, 10, 219–230. [Google Scholar] [CrossRef] [PubMed]
- Elkhatib, T.H.M.; Shehta, N.; Bessar, A.A. Hematoma Expansion Predictors: Laboratory and Radiological Risk Factors in Patients with Acute Intracerebral Hemorrhage: A Prospective Observational Study. J. Stroke Cerebrovasc. Dis. 2019, 28, 2177–2186. [Google Scholar] [CrossRef] [PubMed]
- Broderick, J.P.; Brott, T.G.; Duldner, J.E.; Tomsick, T.; Huster, G. Volume of intracerebral hemorrhage. A powerful and easy-to-use predictor of 30-day mortality. Stroke 1993, 24, 987–993. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.; Xu, Y.; Siwila-Sackman, E.; Wu, B.; Selim, M. The HEP Score: A Nomogram-Derived Hematoma Expansion Prediction Scale. Neurocrit. Care 2015, 23, 179–187. [Google Scholar] [CrossRef]
- Mannami, T.; Iso, H.; Baba, S.; Sasaki, S.; Okada, K.; Konishi, M.; Tsugane, S.; Japan Public Health Center Based Prospective Study on Cancer Cardiovascular Disease Group. Cigarette smoking and risk of stroke and its subtypes among middle-aged Japanese men and women: The JPHC Study Cohort I. Stroke 2004, 35, 1248–1253. [Google Scholar] [CrossRef] [Green Version]
- Honjo, K.; Iso, H.; Tsugane, S.; Tamakoshi, A.; Satoh, H.; Tajima, K.; Suzuki, T.; Sobue, T. The effects of smoking and smoking cessation on mortality from cardiovascular disease among Japanese: Pooled analysis of three large-scale cohort studies in Japan. Tob. Control 2010, 19, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Appelros, P.; Stegmayr, B.; Terent, A. Sex differences in stroke espidemiology: A systematic review. Stroke 2009, 40, 1082–1090. [Google Scholar] [CrossRef] [PubMed]
- Gill, J.S.; Shipley, M.J.; Tsementzis, S.A.; Hornby, R.; Gill, S.K.; Hitchcock, E.R.; Beevers, D.G. Cigarette smoking. A risk factor for hemorrhagic and nonhemorrhagic stroke. Arch. Intern. Med. 1989, 149, 2053–2057. [Google Scholar] [CrossRef] [PubMed]
- Anan, J.; Hijioka, M.; Kurauchi, Y.; Hisatsune, A.; Seki, T.; Katsuki, H. Cortical hemorrhage-associated neurological deficits and tissue damage in mice are ameliorated by therapeutic treatment with nicotine. J. Neurosci. Res. 2017, 95, 1838–1849. [Google Scholar] [CrossRef] [PubMed]
- Hijioka, M.; Matsushita, H.; Hisatsune, A.; Isohama, Y.; Katsuki, H. Therapeutic effect of nicotine in a mouse model of intracerebral hemorrhage. J. Pharmacol. Exp. Ther. 2011, 338, 741–749. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heishman, S.J.; Kleykamp, B.A.; Singleton, E.G. Meta-analysis of the acute effects of nicotine and smoking on human performance. Psychopharmacology 2010, 210, 453–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hijioka, M.; Matsushita, H.; Ishibashi, H.; Hisatsune, A.; Isohama, Y.; Katsuki, H. α7 Nicotinic acetylcholine receptor agonist attenuates neuropathological changes associated with intracerebral hemorrhage in mice. Neuroscience 2012, 222, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Krafft, P.R.; Altay, O.; Rolland, W.B.; Duris, K.; Lekic, T.; Tang, J.; Zhang, J.H. α7 nicotinic acetylcholine receptor agonism confers neuroprotection through GSK-3beta inhibition in a mouse model of intracerebral hemorrhage. Stroke 2012, 43, 844–850. [Google Scholar] [CrossRef] [Green Version]




Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rehni, A.K.; Cho, S.; Zhang, Z.; Zhao, W.; Raval, A.P.; Perez-Pinzon, M.A.; Dave, K.R. Chronic Nicotine Exposure Increases Hematoma Expansion following Collagenase-Induced Intracerebral Hemorrhage in Rats. Biomolecules 2022, 12, 621. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12050621
Rehni AK, Cho S, Zhang Z, Zhao W, Raval AP, Perez-Pinzon MA, Dave KR. Chronic Nicotine Exposure Increases Hematoma Expansion following Collagenase-Induced Intracerebral Hemorrhage in Rats. Biomolecules. 2022; 12(5):621. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12050621
Chicago/Turabian StyleRehni, Ashish K., Sunjoo Cho, Zhexuan Zhang, Weizhao Zhao, Ami P. Raval, Miguel A. Perez-Pinzon, and Kunjan R. Dave. 2022. "Chronic Nicotine Exposure Increases Hematoma Expansion following Collagenase-Induced Intracerebral Hemorrhage in Rats" Biomolecules 12, no. 5: 621. https://0-doi-org.brum.beds.ac.uk/10.3390/biom12050621