1. Introduction
Arthrodesis of the first metatarsophalangeal joint (MTPJ) is a well-established surgical procedure employed to address various conditions such as hallux rigidus, severe hallux valgus, neuromuscular instability, and articular changes associated with rheumatoid arthritis. The primary objective of this procedure is to achieve stable fusion, ultimately leading to an enhancement in patients’ daily activities. Hallux rigidus, characterized by degenerative changes in the MTPJ, causes pain, limited range of motion, and functional impairment. Severe hallux valgus, on the other hand, involves significant deformity of the joint and can result in pain, instability, and difficulty in wearing regular footwear. Neuromuscular instability and articular changes due to rheumatoid arthritis also necessitate interventions to restore stability and alleviate symptoms. Arthrodesis offers a reliable solution by providing a rigid and stable fusion of the joint, effectively reducing pain, improving joint function, and enabling patients to resume their regular activities with greater comfort [
1,
2,
3].
Arthrodesis of the first MTPJ was first reported in 1894 by Clutton as a surgical procedure for severe hallux valgus [
4]. Over the years, the procedure has been considerably modified regarding technique and indication for surgery [
5,
6,
7]. Non-union is considered a major complication of MTPJ arthrodesis with reports in the literature ranging from 2% to 23.5% [
6,
8,
9]. In their systematic review of 2818 first MTPJ arthrodesis cases, Roukis et al. demonstrated an overall incidence of non-union of 5.4% [
10]. The etiology of non-union following first metatarsophalangeal joint (MTPJ) arthrodesis is complex and influenced by multiple factors. Patient-related factors, including smoking and comorbidities, play a significant role in the development of non-union. Smoking has been associated with compromised vascularity and impaired bone healing, which can hinder the fusion process. Comorbidities such as diabetes mellitus and peripheral vascular disease can also contribute to poor bone healing and increase the risk of non-union [
8]. In addition to patient-related factors, surgery-related factors can impact the occurrence of non-union. The technique of joint preparation plays a crucial role in achieving successful fusion. Inadequate removal of cartilage and subchondral bone, as well as insufficient exposure of the joint surfaces, can impede the establishment of a solid bony union. Furthermore, the choice of osteosynthesis, such as the type of fixation hardware used, can influence the stability and ultimate success of the fusion. Improper positioning or failure of the hardware can result in micromotion at the fusion site, leading to non-union. Understanding the multifactorial nature of non-union in first MTPJ arthrodesis is essential for optimizing surgical outcomes. By identifying and addressing patient-related factors, such as smoking cessation and managing comorbidities like diabetes, vascular disease, and inflammatory arthritis, surgeons can minimize the risk of non-union. Diabetes leads to microvascular compromise and advanced glycation end products that interfere with bone healing. Peripheral vascular disease also contributes to poor wound healing and bone fusion due to reduced blood flow. Inflammatory arthritis such as rheumatoid arthritis create a chronic inflammatory state that impairs bone healing. In addition to managing these comorbidities, implementing meticulous surgical techniques with compression and rigid internal fixation is critical. By controlling patient risk factors and utilizing proper surgical methods, surgeons can improve the overall success rate of first MTPJ arthrodesis and reduce the chance of rigid hallux non-union [
11,
12].
Several techniques for joint preparation prior to osteosynthesis in first metatarsophalangeal joint (MTPJ) arthrodesis have been described. One technique that has gained popularity is the creation of ball and socket surfaces. This approach offers theoretical advantages, including reduced surgery time, increased cancellous bone contact surfaces, and the flexibility to fuse the joint at various angles [
13]. However, it is important to consider the potential drawbacks associated with this technique. The use of a reamer to create the ball and socket surfaces generates high kinetic energy, resulting in heat production during the process. This increase in temperature can have detrimental effects on the vitality of the cellular population within the bone. The local ischemia induced by heat, along with the potential damage to surrounding soft tissues, may contribute to non-union [
11].
The primary objective of this study was to assess whether the utilization of mechanical joint preparation with a high-velocity reamer in first metatarsophalangeal joint (MTPJ) arthrodesis leads to a higher non-union rate compared to the conventional manual osteotomy technique. This study aimed to provide valuable insights into the optimal approach for joint preparation in MTPJ arthrodesis, ultimately contributing to improved surgical outcomes and patient care.
2. Materials and Methods
2.1. Patients
Following institutional review board approval, a retrospective study was conducted at an orthopedic division in a single tertiary center. Database from the patient medical chart was reviewed for all patients who underwent the first MTPJ arthrodesis between 2010 and 2015. All surgeries were performed by one of four foot and ankle fellowship-trained surgeons in our medical center. Data included demographic characteristics such as comorbidities, indication for surgery, and the type of joint preparation and fixation. Exclusion criteria were patients aged <18 years and any neuromuscular disorders (i.e., Parkinson’s disease, which may affect the tension across the union joint), and patients who had not completed a minimum 2-year follow-up.
The patients were divided into two groups. Group 1 used traditional manual joint preparation, and Group 2 used mechanical ball and socket high-velocity reamer joint preparation.
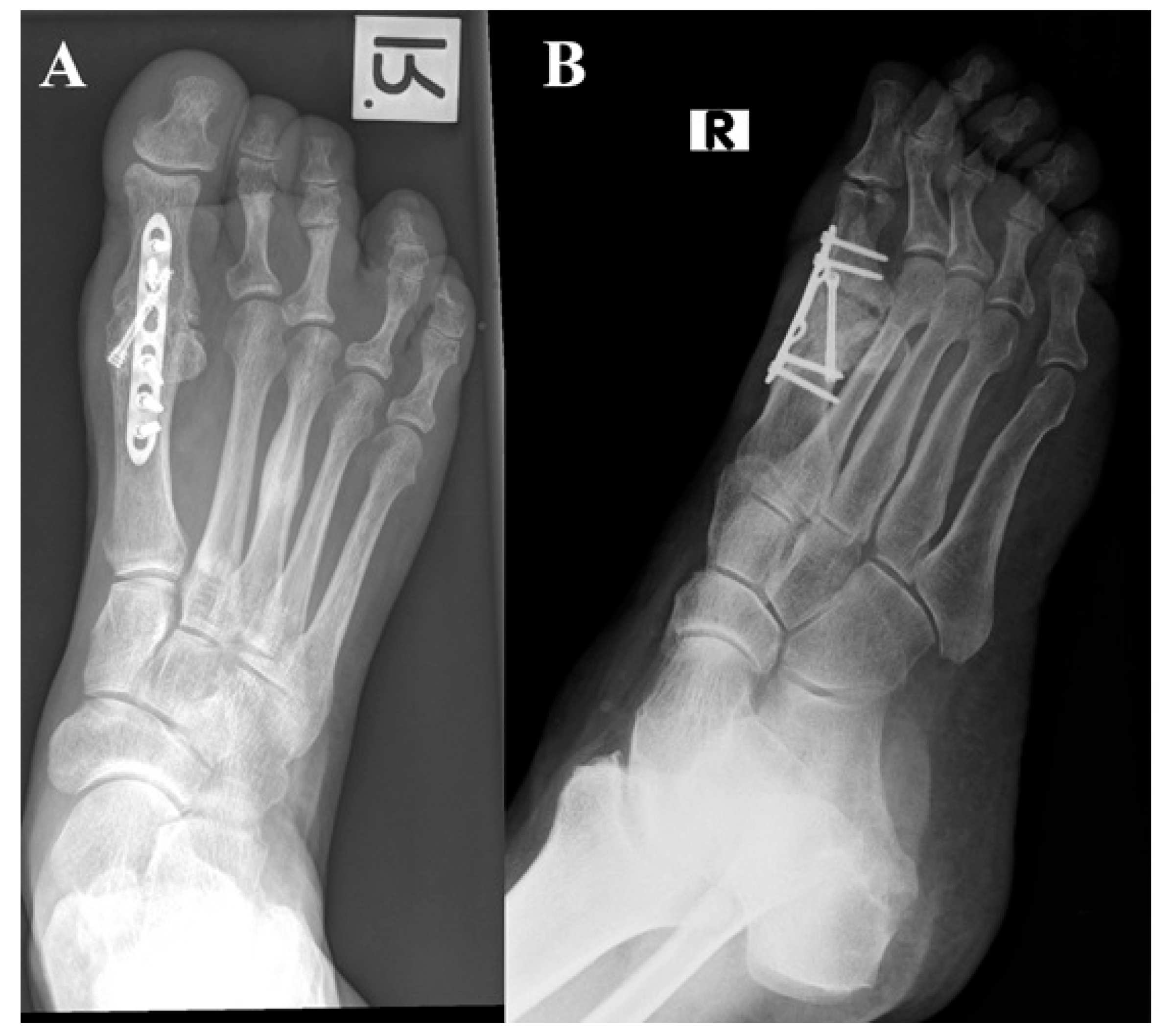
The primary outcome of this study focused on the occurrence of non-union at the fusion site. Non-union was assessed by the treating surgeon in the outpatient clinic, considering both clinical and radiographic findings (as illustrated in
Figure 1). Clinically, non-union was defined as movement in the first metatarsophalangeal joint (MTPJ) with or without associated pain. Radiologically, non-union was characterized by the absence of bone bridging, as well as the presence of osteolysis, hardware migration, and lucency, all of which were evaluated at the 9-month post-surgery mark. To ensure accuracy, all radiographs were thoroughly re-evaluated by the senior authors to confirm the presence of non-union. Secondary outcomes of this study encompassed other complications that may have arisen and the occurrence of revision surgeries.
2.2. Surgical Technique
Surgery was performed under general and local anesthesia, with the patient in a supine position. Prophylactic IV antibiotics were administered, and a tourniquet was applied at the level of the thigh in all cases. All patients were operated utilizing a dorsomedial approach to the first MTPJ to preserve the vasculature and innervation. Osteophytes were removed with a rounger, followed by joint arthrotomy. Two joint preparation techniques were used in our foot and ankle unit between 2010 and 2015.
Technique 1: Manual Preparation
Osteophytes were removed with a rounger, followed by joint arthrotomy. Articular surfaces were prepared for joint fusion by manually removing cartilage and subchondral bone using an osteotome and rongeur, creating two clear surfaces. Subchondral bone was drilled using a 2 mm drill to promote joint fusion.
Technique 2: Mechanical Preparation
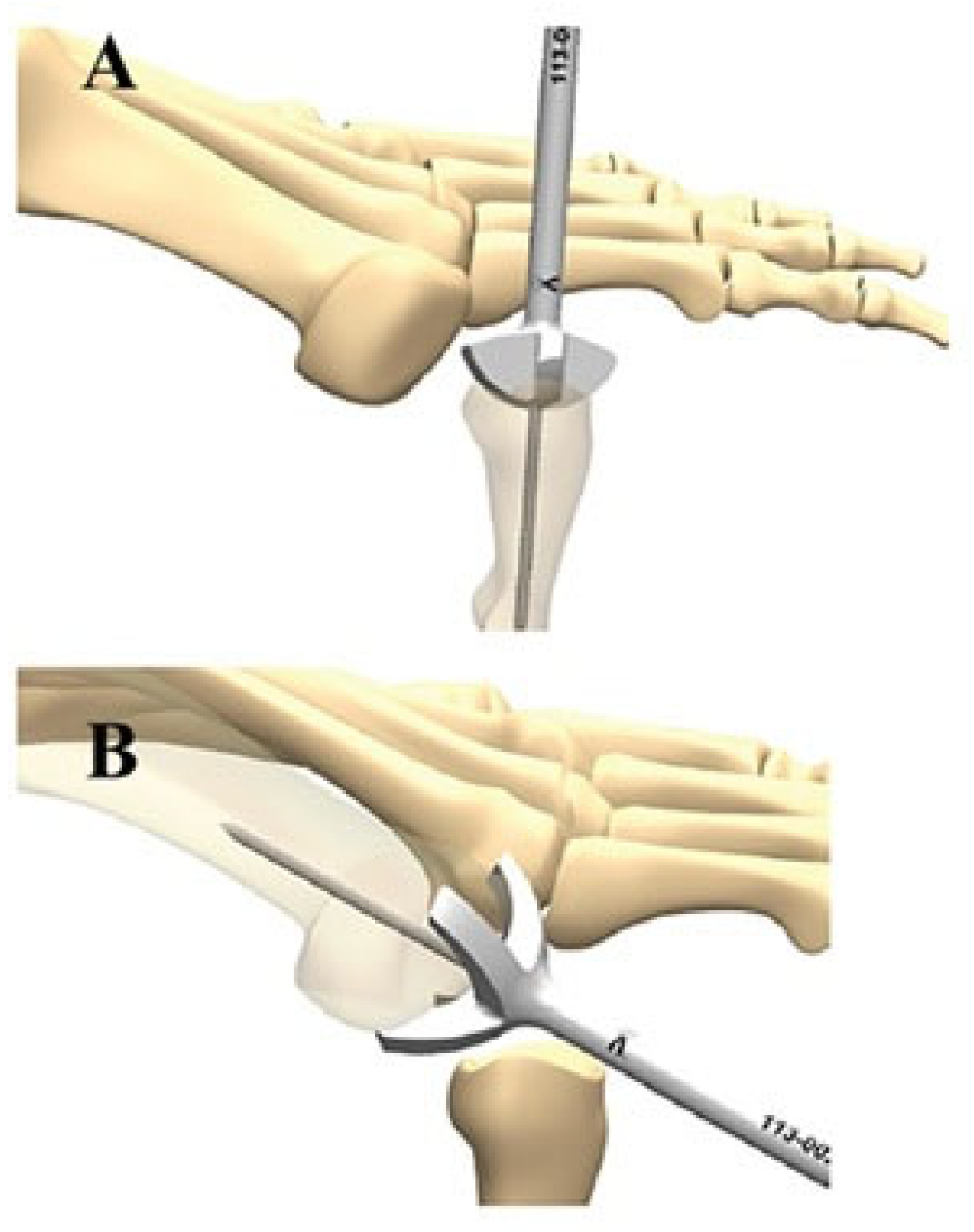
The mechanical ball and socket reamer (AIRLOCK (c), Novastep, NY, USA) was used to create a ball and socket surface on the articular surfaces (
Figure 2). The reamer was applied at a low rotational speed of 350 RPM (Rotations Per Minute) and low torque of 3 Ncm (Newton centimeters) to prevent overheating of the bone surfaces. To further prevent heat formation, ample saline irrigation was applied continuously during reaming. After preparing the surfaces, subchondral bone was drilled using a 2 mm drill to promote joint fusion.
Fixation of the MTPJ was performed by plate and screws crossing the joint. Arthrodesis was carried out only after contact of the great toe on a planar surface was confirmed. The post-operative physiotherapy protocol for all patients included 3 days in a well-padded bandage and non-weight bearing, followed by full weight bearing on an elevated heel solid sole shoe for 6 weeks. The wound was inspected at the clinic 1 week post-operatively, and stitches were removed at 2 weeks. Normal footwear was allowed at 6 weeks. Patients were reviewed post-operatively in the outpatient clinic by their respective surgeons, and the routine follow-up time was 9 months.
2.3. Statistical Analysis
Data were analyzed with the SPSS for Windows Version 17.0 (SPSS Inc., Chicago, IL, USA). Means and standard deviations (SDs) were used to describe continuous variables, and categorical variables are presented as numbers (percentages). Univariate analyses were performed with the Fisher exact test for categorical data and the Student’s t-test for continuous variables. The level of significance was set at p = 0.05.
3. Results
A total of 83 patients who underwent 92 primary first MTPJ arthrodesis were included in our cohort. Of these, 39 patients with 44 surgeries underwent traditional manual joint preparation (Group 1), while 44 patients with 48 surgeries underwent mechanical high-velocity ball and socket reamer joint preparation (Group 2). The mean follow-up time was 45.3 months (95% CI 41.7–49.0 months). The results of this study, as shown in
Table 1, provide insights into the comparison between manual preparation (Group 1) and high-velocity reamer (Group 2) in relation to various factors. The mean age of the participants in Group 1 was 64.86 years (95% CI 60.3–69.4 years), while in Group 2 it was 62.13 years (95% CI 58.1–66.2 years), with no statistically significant difference observed between the two groups (
p = 0.46). In terms of gender distribution, Group 1 comprised 33 females (84.6%) and 6 males (15.4%), whereas Group 2 consisted of 31 females (70.5%) and 13 males (29.5%). Although a higher proportion of females were present in Group 1, the difference did not reach statistical significance (
p = 0.12). The average follow-up time in months was 46.4 (95% CI 39.7–53.0 months) for Group 1 and 44.4 (95% CI 38.6–50.1 months) for Group 2, again demonstrating no significant variation between the two groups (
p = 0.33). Regarding comorbidities, the prevalence of diabetes mellitus was 33.3% (95% CI 18.0–48.7%) in Group 1 and 25% (95% CI 11.8–38.2%) in Group 2 (
p = 0.40), while the rates of smoking, ischemic heart disease, and peripheral vascular disease showed no significant differences between the two groups (
p = 0.91,
p = 0.82, and
p = 0.74, respectively). In terms of the indication for surgery, Group 1 had 50% cases of hallux rigidus, 40.9% cases of hallux valgus, and 2.2% cases of trauma, compared to 41.6%, 50%, and 4.2% in Group 2, respectively, with no statistically significant variations observed among the indications (
p = 0.42,
p = 0.38, and
p = 0.61, respectively). Union was achieved in 37 (84.1%) of cases in Group 1 and in 36 (75%) of cases in Group 2 (
p = 0.28).
The results presented in
Table 2 highlight the comparison between manual preparation (Group 1) and high-velocity reamer (Group 2) in terms of specific outcomes. In Group 1, out of 44 cases, 7 (15.9%) experienced non-union, whereas in Group 2, out of 48 cases, 12 (25%) encountered non-union. However, this difference was not statistically significant (
p = 0.28). Regarding surgical wound infection, Group 1 had 5 cases (11.3%), while Group 2 had 3 cases (6.8%), with no significant variation observed between the groups (
p = 0.38). Interestingly, the need for revision surgery differed significantly between the two groups. In Group 1, 10 cases (22.7%) required revision surgery, whereas in Group 2, 21 cases (43.7%) needed revision surgery. This difference was statistically significant (
p = 0.03), indicating a higher revision surgery rate in Group 2 compared to Group 1. In Group 1, ten cases (22.7%) required revision surgery for either painful non-union (4 cases) or symptomatic prominent hardware (6 cases). In Group 2, revision surgery was needed for either painful non-union (11 cases), prominent hardware (9 cases) or deep wound infection requiring debridement (1 case). All 15 patients from the two groups who had revision surgery due to non-union, achieved union and were pain free at the latest follow-up.
Surgical site infection was the second most common complication after surgery. Seven of the surgical site infections were superficial and treated with oral antibiotics with complete resolution. One case of deep infection, in a patient from Group 2, required surgical debridement and intravenous antibiotics.
4. Discussion
The primary objective of this study was to compare the efficacy of traditional manual reaming with high-velocity mechanical ball and socket reaming as techniques for joint preparation in MTPJ osteosynthesis. This study sought to evaluate and compare the outcomes associated with these two approaches. The main findings of this study revealed that the group undergoing high-speed mechanical reaming exhibited higher rates of non-union compared to the group utilizing standard manual reaming. Additionally, the high-velocity mechanical reaming group demonstrated a significantly higher revision rate in comparison to the group using the traditional manual reaming technique. These results highlight the potential limitations and drawbacks of employing high-speed mechanical reaming in MTPJ osteosynthesis.
Arthrodesis of the first MTPJ has established itself as a dependable and predictable procedure for addressing various pathologies of the great toe. This surgical approach has consistently demonstrated positive outcomes and garnered high patient satisfaction rates. The reliable nature of MTPJ arthrodesis lies in its ability to effectively alleviate symptoms, restore joint stability, and enhance overall function and quality of life for individuals with conditions affecting the great toe [
1,
2]. By achieving a stable fusion of the MTPJ, arthrodesis provides long-lasting relief from pain, improves joint alignment, and allows patients to engage in daily activities with greater comfort and functionality. The high satisfaction reported by patients who undergo this procedure underscores its success in addressing a wide range of pathologies, including hallux rigidus, severe hallux valgus, neuromuscular instability, and articular changes related to conditions such as rheumatoid arthritis [
11,
14]. Commonly described methods for preparing the joint surfaces before the arthrodesis of the first MTPJ include the creation of a ball and socket configuration or a flat-on-flat configuration. These configurations can be achieved using either high-velocity and kinetic energy power tools or manual low-energy tools. The choice of the optimal technique for joint surface preparation in MTPJ arthrodesis remains an ongoing debate, and the gold standard has yet to be determined. Each method has its advantages and considerations. Creating a ball and socket configuration offers theoretical benefits such as shorter surgery times, larger cancellous bone surfaces, and the ability to fuse the joint at different angles, providing versatility in surgical planning. On the other hand, the flat-on-flat configuration allows for a more straightforward and reliable technique with less complexity [
15]. Our study reflects an advantage of the low-velocity flat-on-flat configuration compared to the high-velocity ball and socket, with regard to non-union and the need for revision surgeries, which are the most common complications of this procedure.
The congruent joint-like surface that is created by the ball and socket configuration has many advantages [
16]. This, in part, allows the repair of different pathologies such as valgus angulation, dorsiflexion, and pronation of the hallux. Achieving the ball and socket configuration is easy and reproducible with the conical reamer and is more technically demanding using osteotomes and rounger (
Figure 2) [
17].
The theory behind higher rates of non-union, following the first MTPJ arthrodesis with high-velocity joint preparation, has been addressed by Mahadevan et al. concluding that the ball and socket configuration was less prone to develop non-union when it was performed using low-energy tools (100% union with manual tools compared to 92.1% with high-velocity tools) [
11]. Power tools create kinetic energy and heat, which, in turn, might cause thermal necrosis of the cancellous bone cell population, prevent medullary blood vessel perfusion, and cause higher damage to the surrounding soft tissue, ending with the prevention of callus formation.
Scarano et al. further demonstrated that several factors could significantly influence the heat generated during bone site drilling, including the drill material. A statistically significant difference was observed in drilling time preparation between steel cylindrical drills (2 mm) and zirconia cylindrical drills [
18].
One method of preventing thermal necrosis is the use of saline irrigation during reaming. However, despite the routine use of saline irrigation in our practice when using power tools, the rates of non-union were still high [
10,
19].
The flat-on-flat joint configuration had been biomechanically proven to be more stable than the ball and socket configuration. Politi et al. argued that the improved stability of the flat-on-flat configuration can increase union rates [
20]. Although the findings in this study support the abovementioned hypothesis, numerous larger series did not demonstrate similar findings [
21,
22]. Regarding the osteosynthesis methods, Politi et al. [
20] have biomechanically proved that there is an improvement in stability when more bulky hardware such as plates and screws are used over screws alone. However, Roukis et el. demonstrated that despite improved stability, union rates were actually lower for the bulky hardware as compared to screws alone [
10]. The findings in this study did not prove an advantage to the type of implant to the occurrence of non-union.
Non-union rates in this study were high (20.6%) in both treatment groups. The reported rates in the literature vary considerably between 2 and 23.5% [
6,
8,
9]. Our findings are empirical but are based on streaked clinical and radiographical criteria of non-union. When trying to account for these large differences in non-union rates, several explanations come to mind. First, this study population—28.9% of our cohort had diabetes, which is a known risk factor for infections, non-union, and other complications [
23,
24,
25]. Second, cultural differences and perceptions of pain among the generally low socioeconomic status of the patients operated on in the public system, coupled with no out-of-pocket expenses for the patient for clinician visits, repeated imaging, and revision surgeries [
26]. Lastly, relatively low volume of the first MTPJ arthrodesis surgeries in our medical center during the data collection period.
There are several limitations regarding this study, including its retrospective nature and relatively small sample size, which may introduce bias. The follow-up time, which was mid-term in duration, did not allow for the detection of any long-term complications such as hardware failure. However, it was sufficient to detect non-union infections, which are among the most commonly cited complications of this procedure. A planar or ball and socket type of osteotomy might already have significantly different fusion percentages which may inherently alter the results. Another limitation to consider is the surgical indication, as there were no significant differences observed between the two groups. It is important to note that there is a fair possibility that the valgus group performed worse than the rigidus group, which may have influenced the overall results.






{kind=link}
{kind=link}