
PCOS: A Chronic Disease That Fails to Produce Adequately Specialized Pro-Resolving Lipid Mediators (SPMs)

 , ,
, ,
Abstract
:1. Introduction
Obesity, Insulin Resistance, and Inflammation
2. Material and Methods
2.1. Human Plasma and Serum of PCOS Patients
2.2. Ethical Approval
2.3. Blood Sample Analyses
2.4. Lipid Mediator Extraction and Profiling (LC-MS/MS)
2.5. Targeted LC-MS/MS Acquisition Parameters
2.6. Statistical Analyses
2.7. Evaluated Parameters
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Ehrmann, D.A. Polycystic ovary syndrome. N. Engl. J. Med. 2005, 352, 1223–1236. [Google Scholar] [CrossRef] [PubMed]
- Homburg, R. Polycystic ovary syndrome—From gynecological curiosity to multisystem endocrinopathy. Hum. Reprod. 1996, 11, 29–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Diamanti-Kandarakis, E.; Kandarakis, H.; Legro, R.S. The role of genes and environment in the etiology of PCOS. Endocrine 2006, 30, 19–26. [Google Scholar] [CrossRef]
- Rotterdam ESHRE/ASRM-Sponsored PCOS Consensus Workshop Group. Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum. Reprod. 2004, 19, 41–47. [Google Scholar] [CrossRef] [Green Version]
- Sam, S. Obesity and Polycystic Ovary Syndrome. Obes Manag. 2007, 3, 69–73. [Google Scholar] [CrossRef]
- Ehrmann, D.A.; Barnes, R.B.; Rosenfield, R.L.; Cavaghan, M.K.; Imperial, J. Prevalence of impaired glucose tolerance and diabetes in women with polycystic ovary syndrome. Diabetes Care 1999, 22, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Ciampelli, M.; Fulghesu, A.M.; Cucinelli, F.; Pavone, V.; Ronsisvalle, E.; Guido, M.; Caruso, A.; Lanzone, A. Impact of insulin and body mass index on metabolic and endocrine variables in polycystic ovary syndrome. Metab. Clin. Exp. 1999, 48, 167–172. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin Resistance and the Polycystic Ovary Syndrome Revisited: An Update on Mechanisms and Implications. Endocr. Rev. 2012, 33, 981–1030. [Google Scholar] [CrossRef]
- Teede, H.; Deeks, A.; Moran, L. Polycystic ovary syndrome: A complex condition with psychological, reproductive and metabolic manifestations that impacts on health across the lifespan. BMC Med. 2010, 8, 41. [Google Scholar] [CrossRef] [Green Version]
- Rojas, J.; Chávez, M.; Olivar, L.C.; Rojas, M.; Morillo, J.; Mejías, J.; Calvo, M.; Bermudez, V. Polycystic Ovary Syndrome, Insulin Resistance, and Obesity: Navigating the Pathophysiologic Labyrinth. Int. J. Reprod. Med. 2014, 2014, 719050. [Google Scholar] [CrossRef]
- Rudnicka, E.; Kunicki, M.; Suchta, K.; Machura, P.; Grymowicz, M.; Smolarczyk, R. Inflammatory Markers in Women with Polycystic Ovary Syndrome. BioMed Res. Int. 2020, 2020, 4092470. [Google Scholar] [CrossRef] [PubMed]
- Serhan, C.N. Pro-resolving lipid mediators are leads for resolution physiology. Nature 2014, 510, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastard, J.-P.; Jardel, C.; Bruckert, E.; Blondy, P.; Capeau, J.; Laville, M.; Vidal, H.; Hainque, B. Elevated Levels of Interleukin 6 Are Reduced in Serum and Subcutaneous Adipose Tissue of Obese Women after Weight Loss. J. Clin. Endocrinol. Metab. 2000, 85, 3338–3342. [Google Scholar] [PubMed]
- O’Rourke, R.W.; Kay, T.; Lyle, E.A.; Traxler, S.A.; Deveney, C.W.; Jobe, B.A.; Roberts, C.T.; Marks, D.; Rosenbaum, J.T. Alterations in peripheral blood lymphocyte cytokine expression in obesity. Clin. Exp. Immunol. 2006, 146, 39–46. [Google Scholar] [CrossRef]
- Festa, A.; D’Agostino, R., Jr.; Williams, K.; Karter, A.J.; Mayer-Davis, E.J.; Tracy, R.P.; Haffner, S.M. The relation of body fat mass and distribution to markers of chronic inflammation. Int. J. Obes. 2001, 25, 1407–1415. [Google Scholar] [CrossRef] [Green Version]
- Diehl, A.M. Nonalcoholic steatosis and steatohepatitis IV. Nonalcoholic fatty liver disease abnormalities in macrophage function and cytokines. Am. J. Physiol. 2002, 282, G1–G5. [Google Scholar]
- Arkan, M.C.; Hevener, A.L.; Greten, F.; Maeda, S.; Li, Z.-W.; Long, J.M.; Wynshaw-Boris, A.; Poli, G.; Olefsky, J.; Karin, M. IKK-β links inflammation to obesity-induced insulin resistance. Nat. Med. 2005, 11, 191–198. [Google Scholar] [CrossRef]
- Schönbeck, U.; Mach, F.; Sukhova, G.K.; Herman, M.; Graber, P.; Kehry, M.R.; Libby, P. CD40 Ligation Induces Tissue Factor Expression in Human Vascular Smooth Muscle Cells. Am. J. Pathol. 2000, 156, 7–14. [Google Scholar] [CrossRef] [Green Version]
- Reardon, C.A.; Getz, G.S. Mouse models of atherosclerosis. Curr. Opin. Lipidol. 2001, 12, 167–173. [Google Scholar] [CrossRef]
- Michelsen, K.S.; Wong, M.H.; Shah, P.K.; Zhang, W.; Yano, J.; Doherty, T.M.; Akira, S.; Rajavashisth, T.B.; Arditi, M. Lack of Toll-like receptor 4 or myeloid differentiation factor 88 reduces atherosclerosis and alters plaque phenotype in mice deficient in apolipoprotein E. Proc. Natl. Acad. Sci. USA 2004, 101, 10679–10684. [Google Scholar] [CrossRef] [Green Version]
- Cancello, R.; Tordjman, J.; Poitou, C.; Guilhem, G.; Bouillot, J.L.; Hugol, D.; Coussieu, C.; Basdevant, A.; Bar Hen, A.; Bedossa, P.; et al. Increased Infiltration of Macrophages in Omental Adipose Tissue Is Associated With Marked Hepatic Lesions in Morbid Human Obesity. Diabetes 2006, 55, 1554–1561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, J.E.; Gabler, N.K.; Walker-Daniels, J.; Spurlock, M.E. Tlr-4 Deficiency Selectively Protects Against Obesity Induced by Diets High in Saturated Fat. Obesity 2008, 16, 1248–1255. [Google Scholar] [CrossRef] [PubMed]
- Schaeffler, A.; Gross, P.; Buettner, R.; Bollheimer, C.; Buechler, C.; Neumeier, M.; Kopp, A.; Schoelmerich, J.; Falk, W. Fatty acid-induced induction of Toll-like receptor- 4/nuclear factor-κB pathway in adipocytes links nutritional signalling with innate immunity. Immunology 2009, 126, 233–245. [Google Scholar] [CrossRef]
- Charrière, G.; Cousin, B.; Arnaud, E.; André, M.; Bacou, F.; Penicaud, L.; Casteilla, L. Preadipocyte conversion to macrophage: Evidence of plasticity. J. Biol. Chem. 2003, 278, 9850–9855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloomgarden, Z.T. Inflammation and insulin resistance. Diabetes Care 2003, 26, 1922–1926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frishman, W. Biologic markers as predictors of cardiovascular disease. Am. J. Med. 1998, 104, 18S–27S. [Google Scholar] [CrossRef]
- Orio Jr, F.; Palomba, S.; Cascella, T.; Di Biase, S.; Manguso, F.; Tauchmanovà, L.; Nardo, L.G.; Labella, D.; Savastano, S.; Russo, T.; et al. The increase of leukocytes as a new putative marker of low-grade chronic inflammation and early cardiovascular risk in polycystic ovary syndrome. J. Clin. Endocrinol. Metab. 2005, 90, 2–5. [Google Scholar] [CrossRef] [Green Version]
- Flower, R.J. Prostaglandins, bioassay, and inflammation. Br. J. Pharmacol. 2006, 147 (Suppl.1), S82–S192. [Google Scholar] [CrossRef]
- Chiurchiù, V.; Leuti, A.; Maccarrone, M. Bioactive Lipids and Chronic Inflammation: Managing the Fire Within. Front. Immunol. 2018, 9, 38. [Google Scholar] [CrossRef] [Green Version]
- Dinarello, C.A. Anti-inflammatory Agents: Present and Future. Cell 2010, 140, 935–950. [Google Scholar] [CrossRef] [Green Version]
- Patel, S. Polycystic ovary syndrome (PCOS), an inflammatory, systemic, lifestyle endocrinopathy. J. Steroid Biochem. Mol. Biol. 2018, 182, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Wellen, K.E.; Hotamisligil, G.S. Inflammation, stress, and diabetes. J. Clin. Investig. 2005, 115, 1111–1119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schwab, U.; Lauritzen, L.; Tholstrup, T.; Haldorsson, T.I.; Riserus, U.; Uusitupa, M.; Becker, W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: A systematic review. Food Nutr. Res. 2014, 58, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calder, P.C. Omega-3 polyunsaturated fatty acids and inflammatory processes: Nutrition or pharmacology? Br. J. Clin. Pharmacol. 2013, 75, 645–662. [Google Scholar] [CrossRef] [Green Version]
- Regidor, P.-A.; Mueller, A.; Sailer, M.; Santos, F.G.; Rizo, J.M.; Egea, F.M. Chronic Inflammation in PCOS: The Potential Benefits of Specialized Pro-Resolving Lipid Mediators (SPMs) in the Improvement of the Resolutive Response. Int. J. Mol. Sci. 2020, 22, 384. [Google Scholar] [CrossRef]
- López-Vicario, C.; Rius, B.; Alcaraz-Quiles, J.; García-Alonso, V.; Lopategi, A.; Titos, E.; Clària, J. Pro-resolving mediators produced from EPA and DHA: Overview of the pathways involved and their mechanisms in metabolic syndrome and related liver diseases. Eur. J. Pharmacol. 2016, 785, 133–143. [Google Scholar] [CrossRef]
- Hansen, T.V.; Vik, A.; Serhan, C.N. The Protectin Family of Specialized Pro-resolving Mediators: Potent Immunoresolvents Enabling Innovative Approaches to Target Obesity and Diabetes. Front. Pharmacol. 2019, 9, 1582. [Google Scholar] [CrossRef]
- Tourki, B.; Kain, V.; Pullen, A.B.; Norris, P.C.; Patel, N.; Arora, P.; Leroy, X.; Serhan, C.N.; Halade, G.V. Lack of resolution sensor drives age-related cardiometabolic and cardiorenal defects and impedes inflammation-resolution in heart failure. Mol. Metab. 2020, 31, 138–149. [Google Scholar] [CrossRef]
- López-Vicario, C.; Titos, E.; Walker, M.E.; Alcaraz-Quiles, J.; Casulleras, M.; Durán-Güell, M.; Flores-Costa, R.; Pérez-Romero, N.; Forné, M.; Dalli, J.; et al. Leukocytes from obese individuals exhibit an impaired SPM signature. FASEB J. 2019, 33, 7072–7083. [Google Scholar] [CrossRef] [Green Version]
- Paul, C.; Laganà, A.S.; Maniglio, P.; Triolo, O.; Brady, D.M. Inositol’s and other nutraceuticals’ synergistic actions counteract insulin resistance in polycystic ovarian syndrome and metabolic syndrome: State-of-the-art and future perspectives. Gynecol. Endocrinol. 2016, 32, 431–438. [Google Scholar] [CrossRef]
- Laganà, A.S.; Rossetti, P.; Buscema, M.; La Vignera, S.; Condorelli, R.A.; Gullo, G.; Granese, R.; Triolo, O. Metabolism and Ovarian Function in PCOS Women: A Therapeutic Approach with Inositols. Int. J. Endocrinol. 2016, 2016, 6306410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duleba, A.J.; Dokras, A. Is PCOS an inflammatory process? Fertil. Steril. 2012, 97, 7–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- European Society of Human Reproduction and Embryology. International Evidence-Based Guideline for the Assessment and Management of Polycystic Ovary Syndrome 2018. Available online: https://www.eshre.eu/Guidelines-and-Legal/Guidelines/Polycystic-Ovary-Syndrome (accessed on 12 August 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Healthy (n = 5) | PCOS (n = 15) | |
|---|---|---|
| Sex | Female (5) | Female (15) |
| Age (years) | 32 (29–34) | 31 (24–42) |
| Weight (kg) | 60.7 (50–76) | 85.8 (54–110) |
| High (cm) | 167.4 (162–173) | 164.9 (150–175) |
| BMI (kg/m2) | 21.5 (17.9–28.3) | 31.7 (19.8–41.9) |
| PCOS | NA | +(15) |
| PCOS | PCOS | Healthy | Healthy | PCOS | PCOS | Healthy | Healthy | |
|---|---|---|---|---|---|---|---|---|
| Plasma | Plasma | Plasma | Plasma | Serum | Serum | Serum | Serum | |
| Averages | SD | Averages | SD | Averages | SD | Averages | SD | |
| Markers | ||||||||
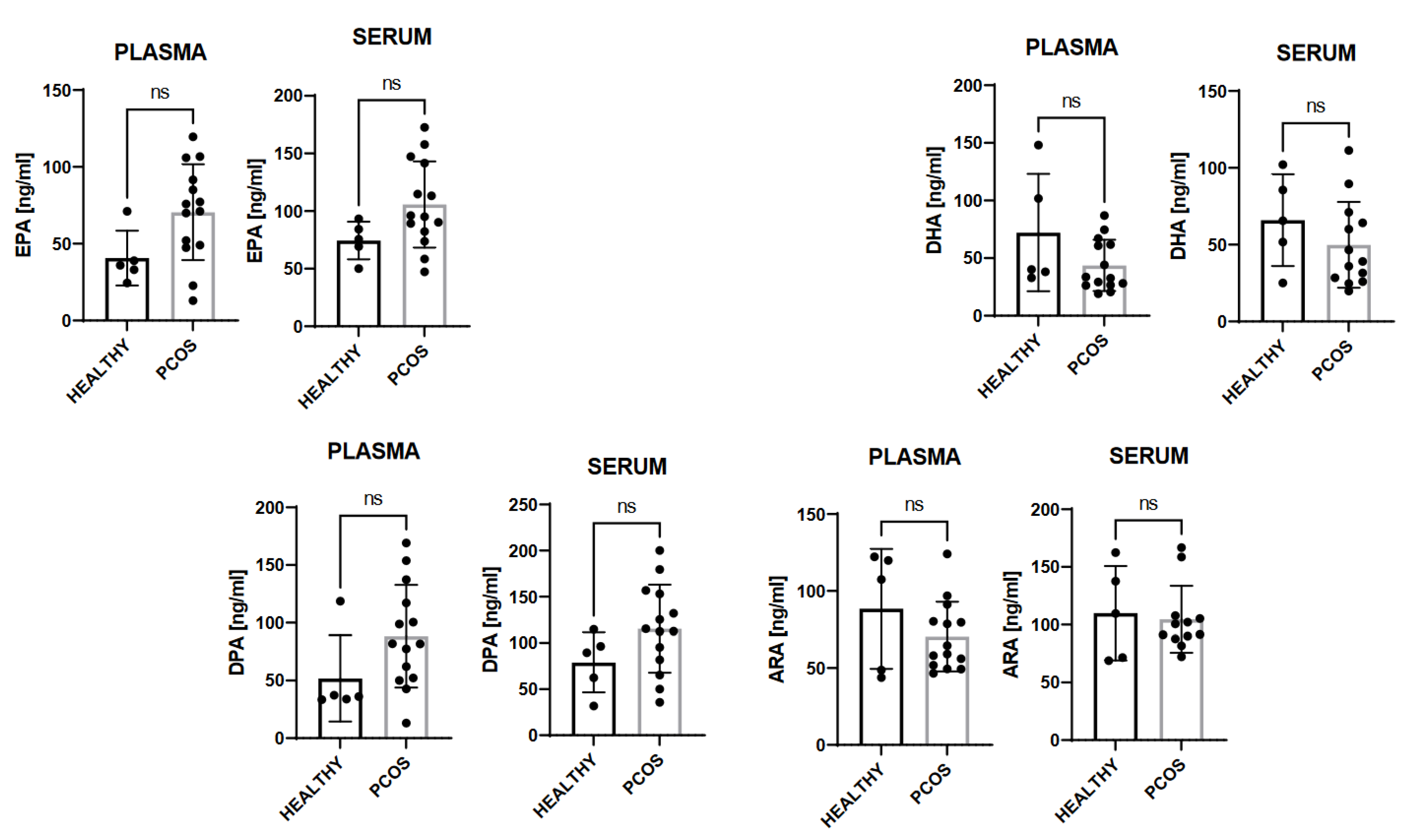
| EPA (ng/mL) | 70.1 | 29.1 | 42.7 | 15.2 | 103.6 | 35.8 | 77.0 | 14.5 |
| DHA (ng/mL) | 42.2 | 21.3 | 67.5 | 42.9 | 54.6 | 35.4 | 65.1 | 24.4 |
| DPA (ng/mL) | 89.0 | 41.5 | 57.4 | 33.0 | 113.8 | 44.7 | 85.0 | 29.7 |
| ARA (ng/mL) | 69.9 | 21.0 | 82.7 | 34.2 | 124.9 | 64.6 | 105.8 | 34.7 |
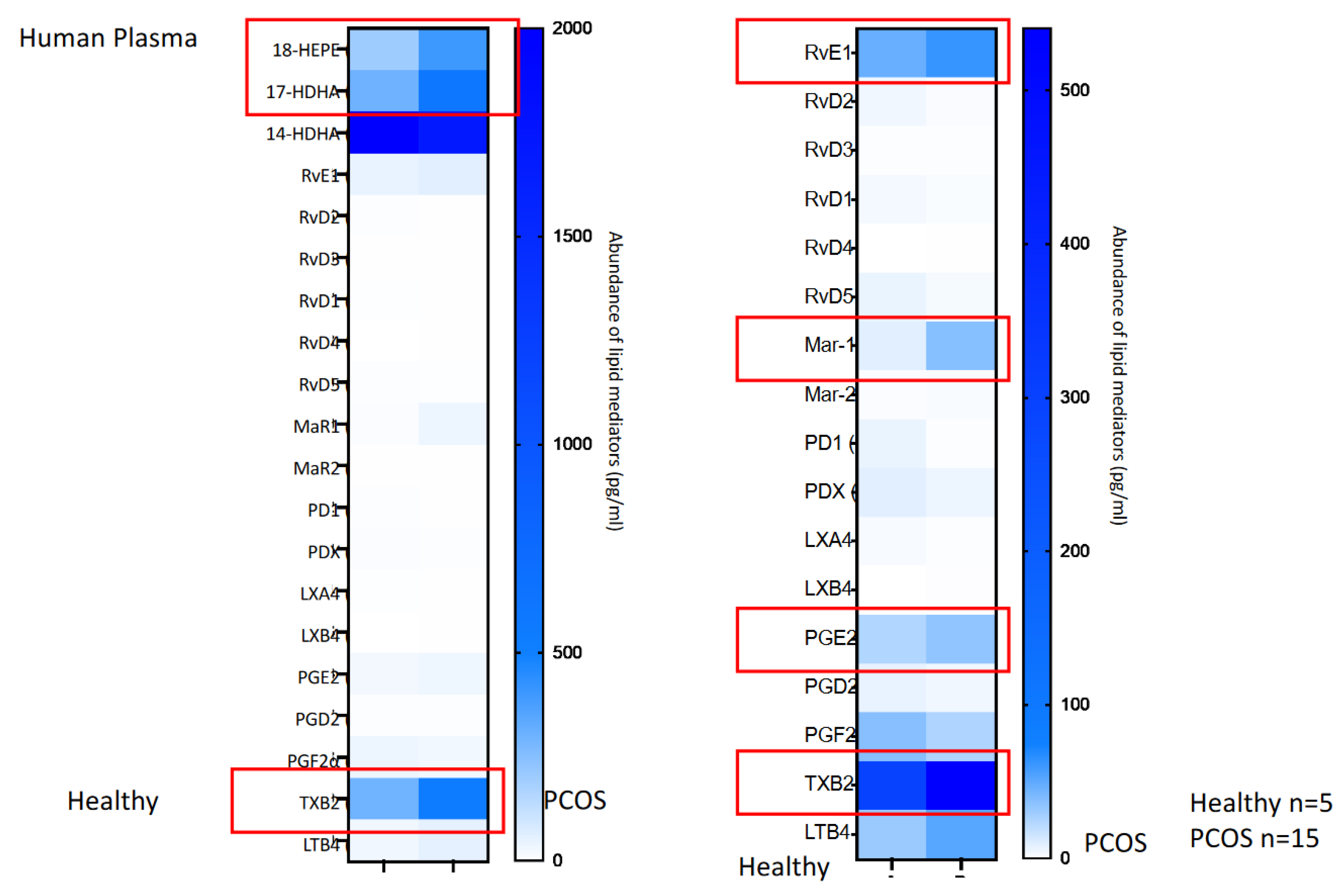
| 18-HEPE (ng/mL) | 0.4 | 0.2 | 0.2 | 0.1 | 4.0 | 3.6 | 2.4 | 1.3 |
| 17-HDHA (ng/mL) | 0.6 | 0.3 | 0.3 | 0.2 | 11.8 | 5.9 | 7.1 | 3.0 |
| 14-HDHA (ng/mL) | 1.6 | 1.2 | 2.0 | 1.3 | 79.8 | 31.8 | 61.2 | 27.4 |
| RvE1 (pg/mL) | 97.6 | 254.0 | 39.1 | 87.4 | 188.4 | 317.1 | 170.4 | 381.1 |
| RvD2 (pg/mL) | 1.9 | 2.1 | 3.7 | 8.3 | 4.8 | 13.1 | 0.0 | 0.0 |
| RvD3 (pg/mL) | 1.1 | 0.9 | 0.7 | 1.7 | 0.7 | 1.4 | 0.9 | 1.4 |
| RvD1 (pg/mL) | 1.9 | 2.1 | 3.2 | 6.0 | 3.9 | 5.1 | 2.5 | 3.8 |
| RvD4 (pg/mL) | 0.3 | 0.6 | 0.0 | 0.0 | 1.1 | 2.4 | 0.0 | 0.0 |
| RvD5 (pg/mL) | 2.7 | 3.2 | 5.7 | 5.9 | 83.7 | 44.4 | 34.2 | 13.1 |
| Mar-1 (pg/mL) | 38.0 | 36.4 | 7.7 | 11.7 | 81.8 | 77.3 | 21.5 | 27.9 |
| Mar-2 (pg/mL) | 2.5 | 2.7 | 1.2 | 1.8 | 231.0 | 164.8 | 93.0 | 51.4 |
| PD1 (pg/mL) | 1.3 | 2.3 | 5.9 | 8.1 | 3.7 | 4.3 | 7.4 | 3.2 |
| PDX (pg/mL) | 7.5 | 9.2 | 7.4 | 10.4 | 72.1 | 33.1 | 41.6 | 28.7 |
| LXA4 (pg/mL) | 1.0 | 1.1 | 2.2 | 2.6 | 1.3 | 2.4 | 1.6 | 1.6 |
| LXB4 (pg/mL) | 2.0 | 5.8 | 0.0 | 0.0 | 2.0 | 5.6 | 2.7 | 6.0 |
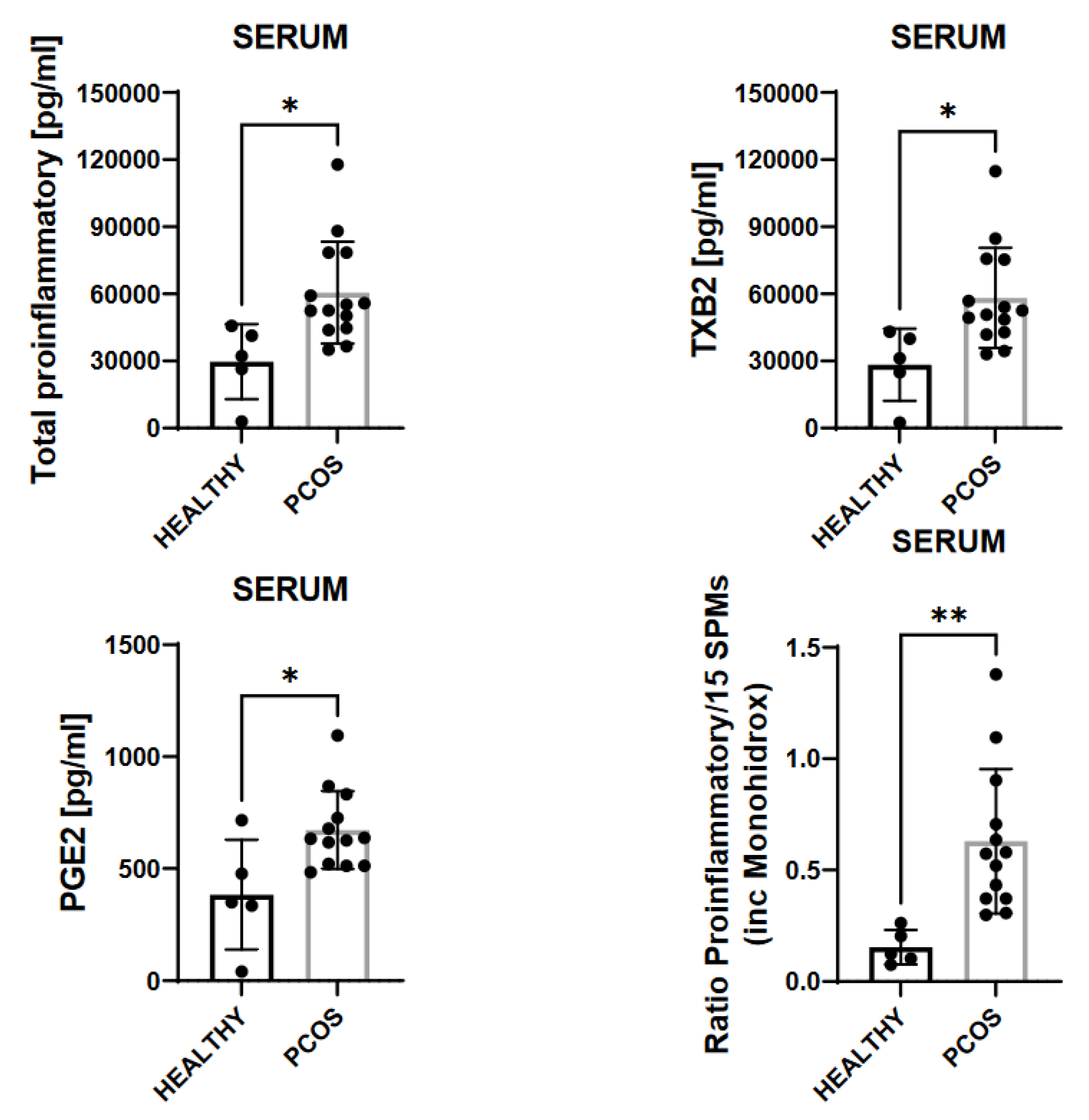
| PGE2 (pg/mL) | 32.9 | 46.9 | 21.5 | 15.6 | 716.3 | 295.6 | 525.8 | 375.0 |
| PGD2 (pg/mL) | 5.2 | 4.1 | 6.1 | 4.1 | 58.9 | 18.0 | 51.8 | 20.1 |
| PGF2α (pg/mL) | 25.6 | 14.6 | 33.1 | 44.7 | 1275.9 | 578.1 | 777.4 | 474.8 |
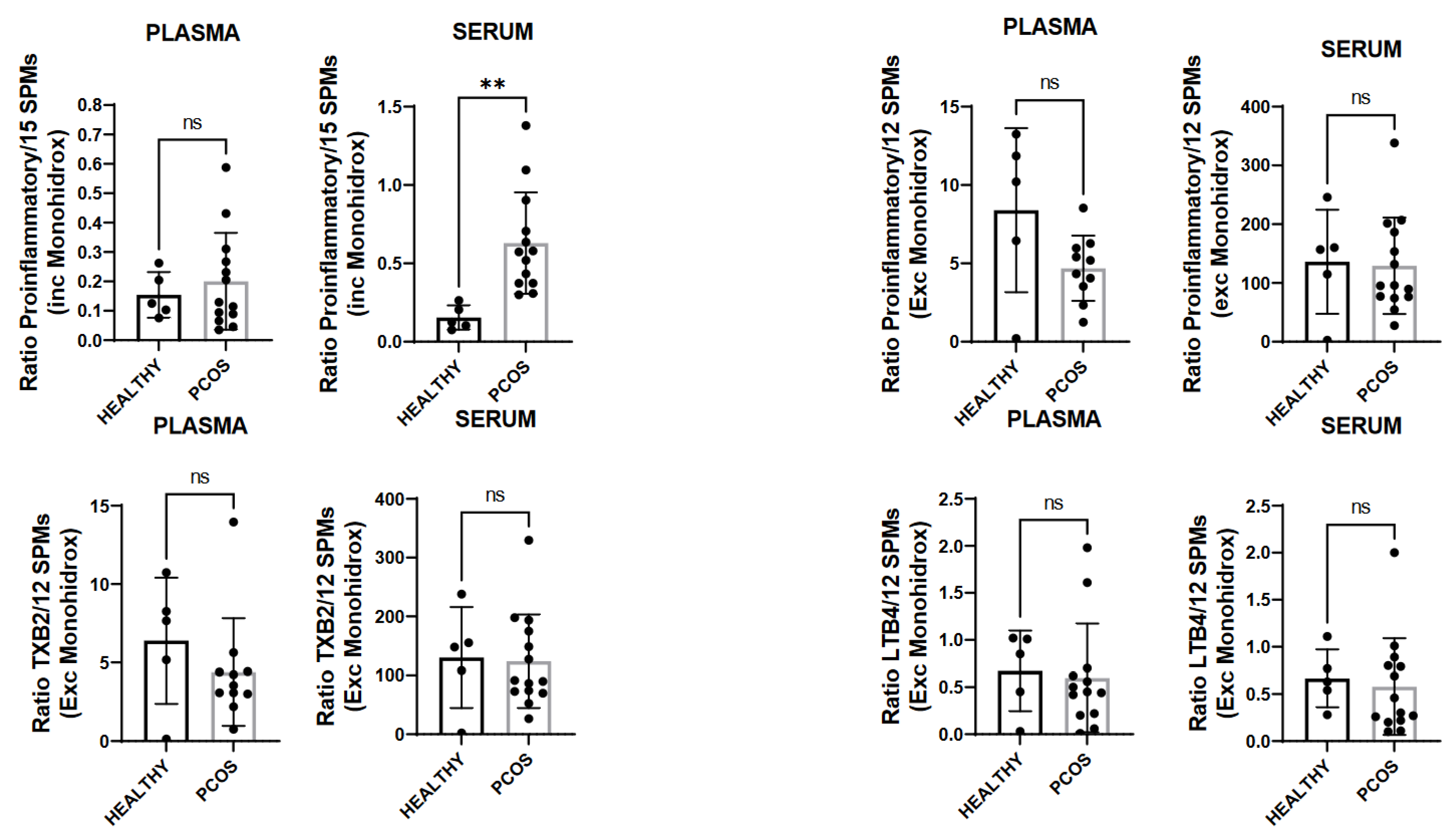
| TXB2 (pg/mL) | 511.7 | 592.1 | 275.4 | 147.5 | 54,730 | 24,475 | 32,555 | 16,236 |
| LTB4 (pg/mL) | 51.3 | 90.4 | 28.0 | 14.8 | 273.6 | 160.4 | 211.5 | 74.7 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Regidor, P.-A.; de la Rosa, X.; Müller, A.; Mayr, M.; Gonzalez Santos, F.; Gracia Banzo, R.; Rizo, J.M. PCOS: A Chronic Disease That Fails to Produce Adequately Specialized Pro-Resolving Lipid Mediators (SPMs). Biomedicines 2022, 10, 456. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020456
Regidor P-A, de la Rosa X, Müller A, Mayr M, Gonzalez Santos F, Gracia Banzo R, Rizo JM. PCOS: A Chronic Disease That Fails to Produce Adequately Specialized Pro-Resolving Lipid Mediators (SPMs). Biomedicines. 2022; 10(2):456. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020456
Chicago/Turabian StyleRegidor, Pedro-Antonio, Xavier de la Rosa, Anna Müller, Manuela Mayr, Fernando Gonzalez Santos, Rafael Gracia Banzo, and Jose Miguel Rizo. 2022. "PCOS: A Chronic Disease That Fails to Produce Adequately Specialized Pro-Resolving Lipid Mediators (SPMs)" Biomedicines 10, no. 2: 456. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10020456