
Expression and Prognostic Implication of PD-L1 in Patients with Urothelial Carcinoma with Variant Histology (Squamous Differentiation or Micropapillary) Undergoing Radical Cystectomy


Abstract
:1. Introduction
2. Materials and Methods
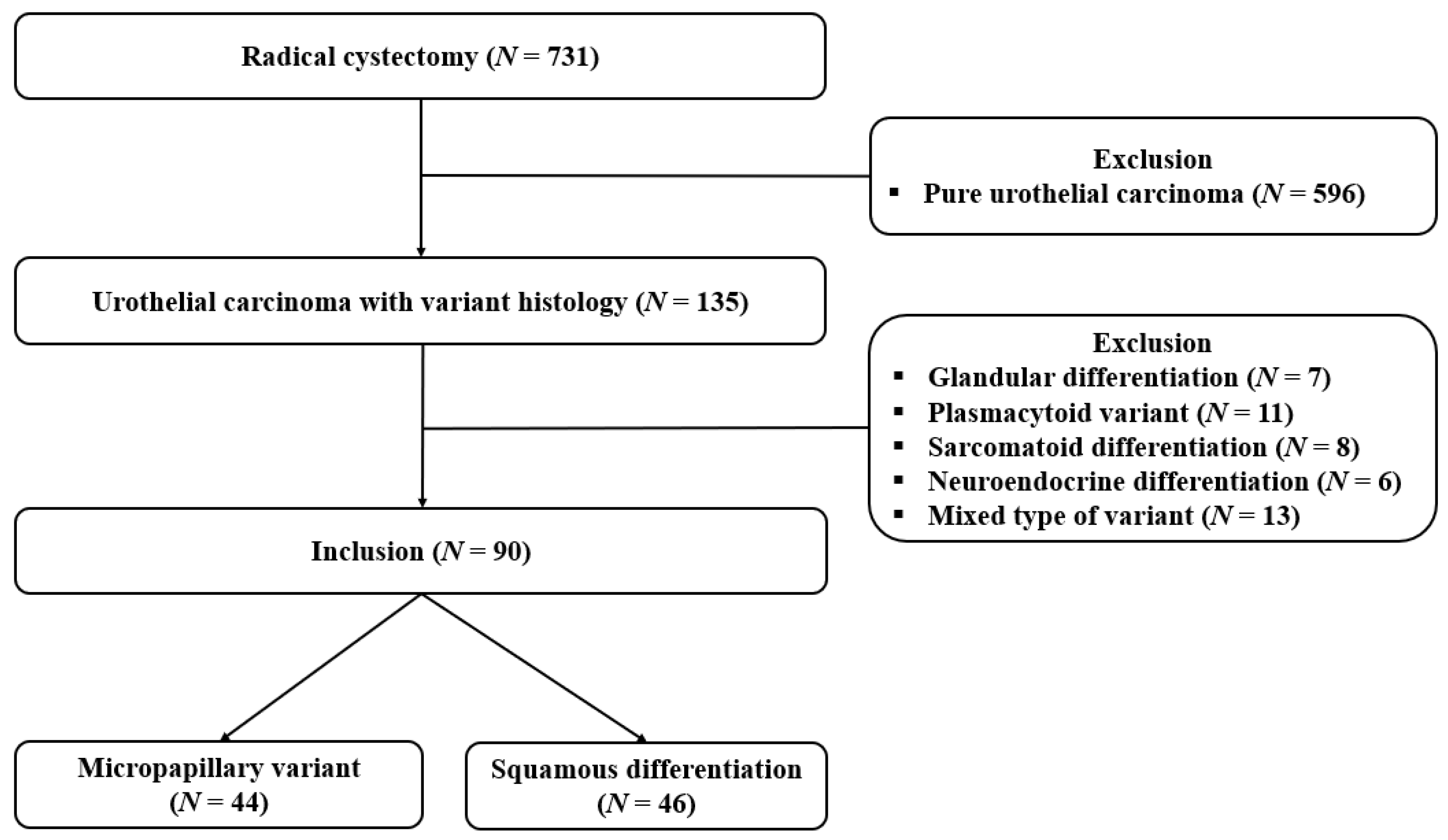
2.1. Study Population
2.2. Data Collection
2.3. Histologic Assessment
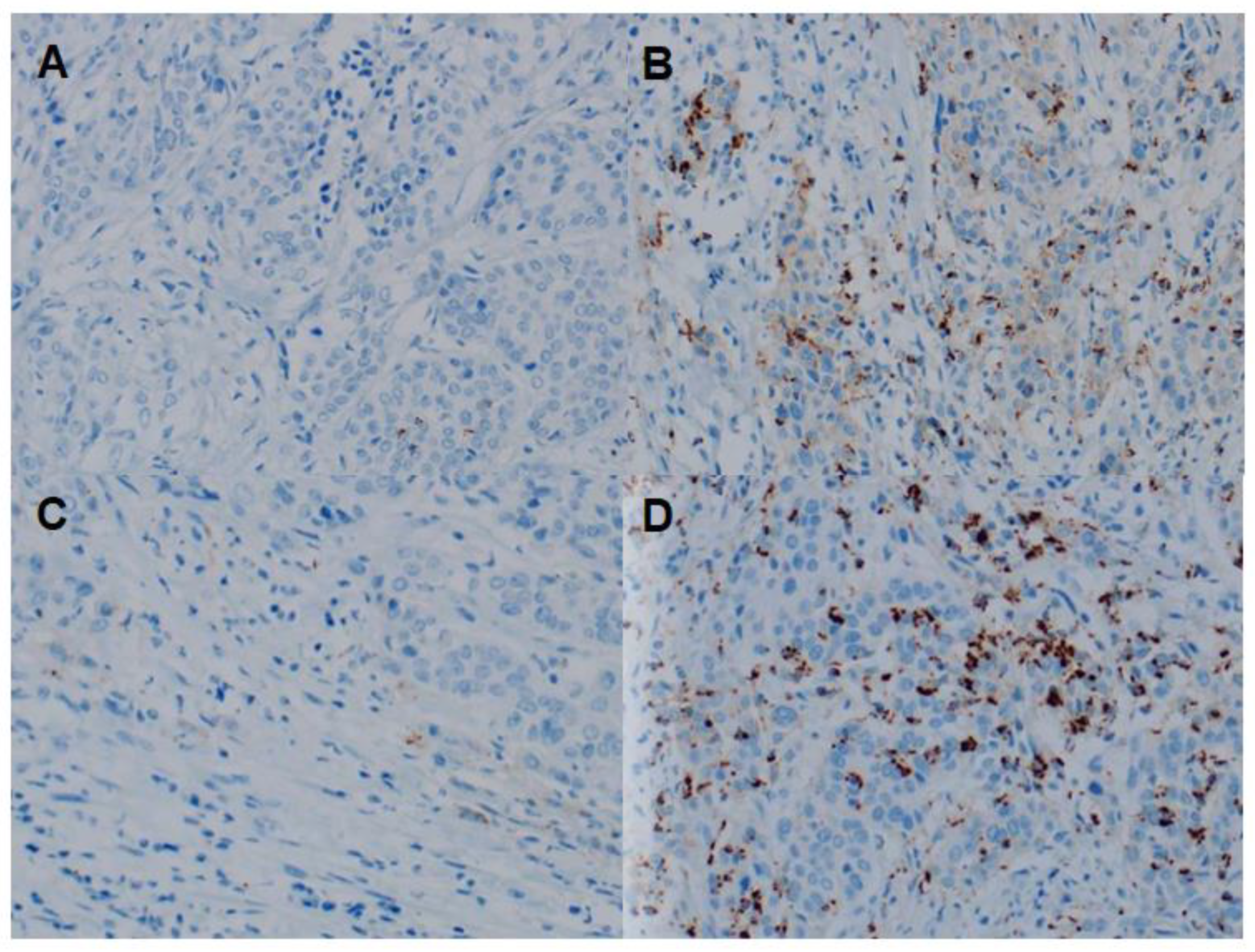
2.4. IHC Assay and Scoring
2.5. Follow-up Protocol
2.6. Statistical Analysis
3. Results
3.1. Demographic and Tumor Characteristics
3.2. Relationship between PD-L1 Expression and Clinicopathological Features
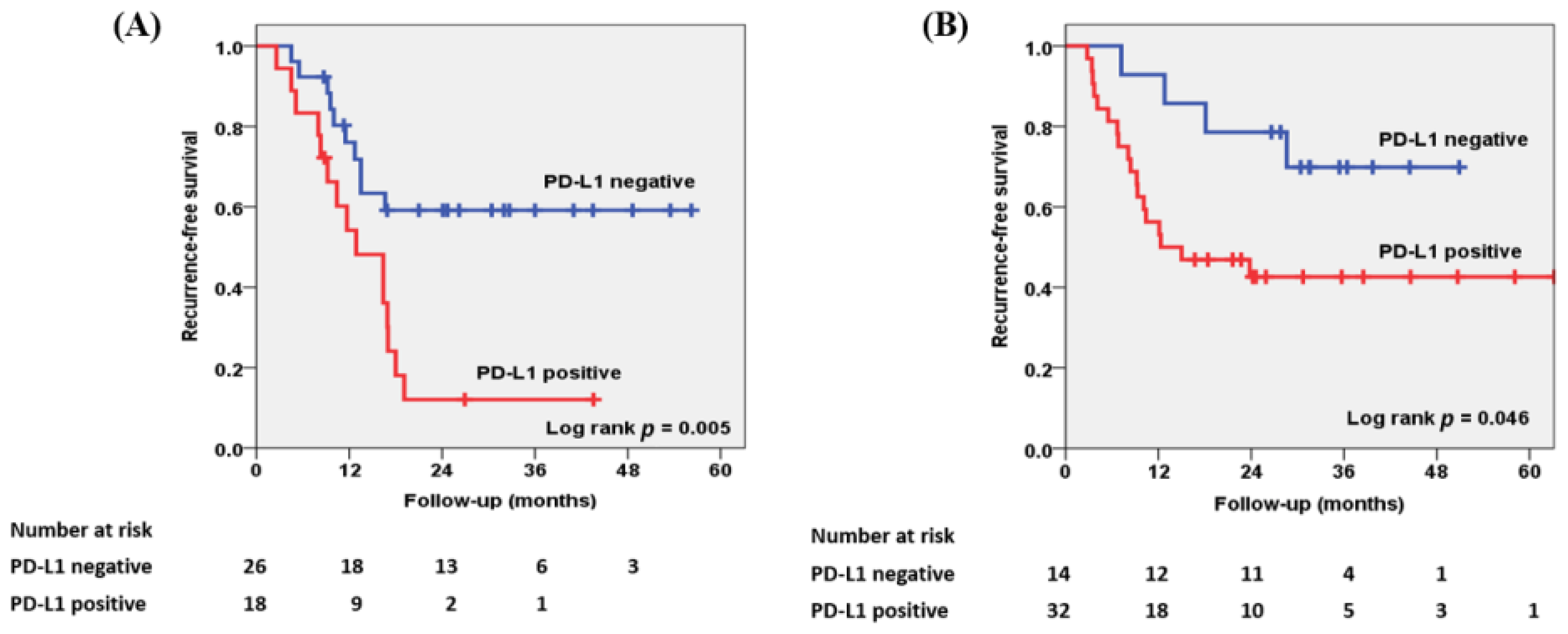
3.3. Relationship between PD-L1 Expression and RFS
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bellmunt, J.; Powles, T.; Vogelzang, N.J. A review on the evolution of PD-1/PD-L1 immunotherapy for bladder cancer: The future is now. Cancer Treat Rev. 2017, 54, 58–67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Apolo, A.B.; Grossman, H.B.; Bajorin, D.; Steinberg, G.; Kamat, A.M. Practical use of perioperative chemotherapy for muscle-invasive bladder cancer: Summary of session at the Society of Urologic Oncology annual meeting. Urol. Oncol. Semin. Orig. Investig. 2012, 30, 772–780. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reis, H.; Serrette, R.; Posada, J.; Lu, V.; Chen, Y.B.; Gopalan, A.; Fine, S.W.; Tickoo, S.K.; Sirintrapun, S.J.; Iyer, G.; et al. PD-L1 Expression in Urothelial Carcinoma with Predominant or Pure Variant Histology: Concordance among 3 Commonly Used and Commercially Available Antibodies. Am. J. Surg. Pathol. 2019, 43, 920–927. [Google Scholar] [CrossRef] [PubMed]
- Bellmunt, J.; De Wit, R.; Vaughn, D.J.; Fradet, Y.; Lee, J.-L.; Fong, L.; Vogelzang, N.J.; Climent, M.A.; Petrylak, D.P.; Choueiri, T.K.; et al. Pembrolizumab as Second-Line Therapy for Advanced Urothelial Carcinoma. N. Engl. J. Med. 2017, 376, 1015–1026. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, J.E.; Hoffman-Censits, J.; Powles, T.; van der Heijden, M.S.; Balar, A.V.; Necchi, A.; Dawson, N.; O’Donnell, P.H.; Balmanoukian, A.; Loriot, Y.; et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: A single-arm, multicentre, phase 2 trial. Lancet 2016, 387, 1909–1920. [Google Scholar] [CrossRef] [Green Version]
- Sharma, P.; Retz, M.; Siefker-Radtke, A.; Baron, A.; Necchi, A.; Bedke, J.; Plimack, E.R.; Vaena, D.; Grimm, M.-O.; Bracarda, S.; et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (CheckMate 275): A multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017, 18, 312–322. [Google Scholar] [CrossRef]
- Pardoll, D.M. The blockade of immune checkpoints in cancer immunotherapy. Nat. Rev. Cancer 2012, 12, 252–264. [Google Scholar] [CrossRef] [Green Version]
- Powles, T.; Eder, J.P.; Fine, G.D.; Braiteh, F.S.; Loriot, Y.; Cruz, C.; Bellmunt, J.; Burris, H.A.; Petrylak, D.P.; Teng, S.-L.; et al. MPDL3280A (anti-PD-L1) treatment leads to clinical activity in metastatic bladder cancer. Nature 2014, 515, 558–562. [Google Scholar] [CrossRef]
- Nakanishi, J.; Wada, Y.; Matsumoto, K.; Azuma, M.; Kikuchi, K.; Ueda, S. Overexpression of B7-H1 (PD-L1) significantly associates with tumor grade and postoperative prognosis in human urothelial cancers. Cancer Immunol. Immunother. 2007, 56, 1173–1182. [Google Scholar] [CrossRef]
- Humphrey, P.A.; Moch, H.; Cubilla, A.L.; Ulbright, T.M.; Reuter, V.E. The 2016 WHO Classification of Tumours of the Urinary System and Male Genital Organs—Part B: Prostate and Bladder Tumours. Eur. Urol. 2016, 70, 106–119. [Google Scholar] [CrossRef] [Green Version]
- Linder, B.J.; Boorjian, S.A.; Cheville, J.C.; Sukov, W.R.; Thapa, P.; Tarrell, R.F.; Frank, I. The Impact of Histological Reclassification during Pathology Re-Review—Evidence of a Will Rogers Effect in Bladder Cancer? J. Urol. 2013, 190, 1692–1697. [Google Scholar] [CrossRef] [PubMed]
- Alanee, S.; Alvarado-Cabrero, I.; Murugan, P.; Kumar, R.; Nepple, K.; Paner, G.P.; Patel, M.I.; Raspollini, M.R.; Lopez-Beltran, A.; Konety, B.R. Update of the International Consultation on Urological Diseases on bladder cancer 2018: Non-urothelial cancers of the urinary bladder. World J. Urol. 2019, 37, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Moschini, M.; D’Andrea, D.; Korn, S.; Irmak, Y.; Soria, F.; Compérat, E.; Shariat, S.F. Characteristics and clinical significance of histological variants of bladder cancer. Nat. Rev. Urol. 2017, 14, 651–668. [Google Scholar] [CrossRef] [PubMed]
- Gordetsky, J.B.; Montgomery, K.W.; Giannico, G.A.; Rais-Bahrami, S.; Thapa, P.; Boorjian, S.; Frank, I.; Cheville, J. The Significance of Squamous Histology on Clinical Outcomes and PD-L1 Expression in Bladder Cancer. Int. J. Surg. Pathol. 2021, 30, 6–14. [Google Scholar] [CrossRef]
- Bajorin, D.F.; Witjes, J.A.; Gschwend, J.E.; Schenker, M.; Valderrama, B.P.; Tomita, Y.; Bamias, A.; Lebret, T.; Shariat, S.F.; Park, S.H.; et al. Adjuvant Nivolumab versus Placebo in Muscle-Invasive Urothelial Carcinoma. N. Engl. J. Med. 2021, 384, 2102–2114. [Google Scholar] [CrossRef]
- Bellmunt, J.; Hussain, M.; Gschwend, J.E.; Albers, P.; Oudard, S.; Castellano, D.; Daneshmand, S.; Nishiyama, H.; Majchrowicz, M.; Degaonkar, V.; et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021, 22, 525–537. [Google Scholar] [CrossRef]
- Powles, T.; Park, S.H.; Voog, E.; Caserta, C.; Valderrama, B.P.; Gurney, H.; Kalofonos, H.; Radulović, S.; Demey, W.; Ullén, A.; et al. Avelumab Maintenance Therapy for Advanced or Metastatic Urothelial Carcinoma. N. Engl. J. Med. 2020, 383, 1218–1230. [Google Scholar] [CrossRef]
- Witjes, J.A.; Bruins, H.M.; Cathomas, R.; Compérat, E.M.; Cowan, N.C.; Gakis, G.; Hernández, V.; Espinós, E.L.; Lorch, A.; Neuzillet, Y.; et al. European Association of Urology Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2020 Guidelines. Eur. Urol. 2021, 79, 82–104. [Google Scholar] [CrossRef]
- Mukherji, D.; Jabbour, M.N.; Saroufim, M.; Temraz, S.; Nasr, R.; Charafeddine, M.; Assi, R.; Shamseddine, A.; Tawil, A.N. Programmed Death-Ligand 1 Expression in Muscle-Invasive Bladder Cancer Cystectomy Specimens and Lymph Node Metastasis: A Reliable Treatment Selection Biomarker? Clin. Genitourin. Cancer 2016, 14, 183–187. [Google Scholar] [CrossRef]
- Baras, A.S.; Drake, C.; Liu, J.-J.; Gandhi, N.; Kates, M.; Hoque, M.O.; Meeker, A.; Hahn, N.; Taube, J.M.; Schoenberg, M.P.; et al. The ratio of CD8 to Treg tumor-infiltrating lymphocytes is associated with response to cisplatin-based neoadjuvant chemotherapy in patients with muscle invasive urothelial carcinoma of the bladder. OncoImmunology 2016, 5, e1134412. [Google Scholar] [CrossRef] [Green Version]
- Inman, B.A.; Sebo, T.J.; Frigola, X.; Dong, H.; Bergstralh, E.J.; Fradet, Y.; Lacombe, L.; Kwon, E.D. 879: PD-L1 (B7-H1) Expression by Urothelial Carcinoma of the Bladder and BCG-Induced Granulomata: Associations with Localized Stage Progression. J. Urol. 2007, 177, 292. [Google Scholar] [CrossRef]
- Nechifor-Boilă, I.; Loghin, A.; Nechifor-Boilă, A.; Decaussin-Petrucci, M.; Voidăzan, S.; Chibelean, B.; Martha, O.; Borda, A. PD-L1 Expression in Muscle Invasive Urothelial Carcinomas as Assessed via Immunohistochemistry: Correlations with Specific Clinical and Pathological Features, with Emphasis on Prognosis after Radical Cystectomy. Life 2021, 11, 404. [Google Scholar] [CrossRef] [PubMed]
- Holland, B.C.; Sood, A.; Delfino, K.; Dynda, D.I.; Ran, S.; Freed, N.; Alanee, S. Age and sex have no impact on expression levels of markers of immune cell infiltration and immune checkpoint pathways in patients with muscle-invasive urothelial carcinoma of the bladder treated with radical cystectomy. Cancer Immunol. Immunother. 2019, 68, 991–997. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Pan, W.; Yang, M.; Yang, W.; He, W.; Chen, X.; Bi, J.; Jiang, N.; Huang, J.; Lin, T. Programmed death ligand-1 is associated with tumor infiltrating lymphocytes and poorer survival in urothelial cell carcinoma of the bladder. Cancer Sci. 2019, 110, 489–498. [Google Scholar] [CrossRef]
- Patel, S.P.; Kurzrock, R. PD-L1 Expression as a Predictive Biomarker in Cancer Immunotherapy. Mol. Cancer Ther. 2015, 14, 847–856. [Google Scholar] [CrossRef] [Green Version]
- Ribas, A.; Wolchok, J.D. Cancer immunotherapy using checkpoint blockade. Science 2018, 359, 1350–1355. [Google Scholar] [CrossRef] [Green Version]
- Pichler, R.; Fritz, J.; Lackner, F.; Sprung, S.; Brunner, A.; Horninger, W.; Loidl, W.; Pircher, A.; Heidegger, I. Prognostic Value of Testing PD-L1 Expression After Radical Cystectomy in High-risk Patients. Clin. Genitourin. Cancer 2018, 16, e1015–e1024. [Google Scholar] [CrossRef]
- Lee, D.H.; Jeong, J.Y.; Song, W. Prognostic Value of Programmed Death Ligand-1 Expression on Tumor-Infiltrating Immune Cells in Patients Treated with Cisplatin-Based Combination Adjuvant Chemotherapy Following Radical Cystectomy for Muscle-Invasive Bladder Cancer: A Retrospective Cohort Study. OncoTargets Ther. 2021, 14, 845–855. [Google Scholar] [CrossRef]
- Lee, C.U.; Lee, D.H.; Song, W. Prognostic Role of Programmed Death Ligand-1 on Tumor-Infiltrating Immune Cells in “High-Risk” Patients Following Radical Cystectomy: A Retrospective Cohort Study. Front. Oncol. 2021, 11, 706503. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Parameters | Total | Variant Histology | p | |
|---|---|---|---|---|
| Micropapillary | Squamous Differentiation | |||
| No. of patients | 90 (100.0) | 44 (48.9) | 46 (51.1) | |
| Age at surgery, years | 0.529 | |||
| Median (IQR) | 68.0 (61.8–73.0) | 68.5 (62.3–70.8) | 66.5 (58.3–74.3) | |
| Mean (SD) | 66.0 (10.1) | 66.7 (7.9) | 65.3 (11.8) | |
| Sex, n (%) | 0.831 | |||
| Male | 77 (85.6) | 38 (86.4) | 39 (84.8) | |
| Female | 13 (14.4) | 6 (13.6) | 7 (15.2) | |
| Pathologic T stage at RC, n (%) | 0.013 | |||
| ≤pT1 | 16 (17.8) | 13 (29.5) | 3 (6.5) | |
| pT2 | 20 (22.2) | 7 (16.0) | 13 (28.3) | |
| pT3/4 | 54 (60.0) | 24 (54.5) | 30 (65.2) | |
| Concomitant CIS at RC, n (%) | 0.057 | |||
| Yes | 46 (51.1) | 27 (61.4) | 19 (41.3) | |
| No | 44 (48.8) | 17 (38.6) | 27 (58.7) | |
| LVI at RC, n (%) | 0.090 | |||
| Yes | 47 (52.2) | 27 (61.4) | 20 (43.5) | |
| No | 43 (47.8) | 17 (38.6) | 26 (56.5) | |
| No. of resected LNs at RC | 0.112 | |||
| Median (IQR) | 20.0 (14.0–29.0) | 21.0 (14.3–30.5) | 18.5 (13.0–25.3) | |
| Mean (SD) | 22.5 (10.9) | 24.4 (11.8) | 20.8 (9.7) | |
| Pathologic N status at RC, n (%) | 0.093 | |||
| Negative | 47 (52.2) | 19 (43.2) | 28 (60.9) | |
| Positive | 43 (47.8) | 25 (56.8) | 18 (39.1) | |
| Surgical margin status, n (%) | 0.210 | |||
| Negative | 76 (84.4) | 35 (79.5) | 41 (89.1) | |
| Positive | 14 (15.6) | 9 (20.5) | 5 (10.9) | |
| Type of urinary diversion, n (%) | 0.283 | |||
| Ileal conduit | 14 (15.6) | 5 (11.4) | 9 (19.6) | |
| Orthotopic neobladder | 76 (84.8) | 39 (88.6) | 37 (80.4) | |
| Neoadjuvant chemotherapy, n (%) | 0.022 | |||
| Yes | 15 (16.7) | 3 (6.8) | 12 (26.1) | |
| No | 75 (83.3) | 41 (93.2) | 34 (73.9) | |
| Adjuvant chemotherapy, n (%) | 0.766 | |||
| Yes | 60 (66.7) | 30 (68.2) | 30 (65.2) | |
| No | 30 (33.3) | 14 (31.8) | 16 (34.8) | |
| Parameters | Variant Histologies | |||||||
|---|---|---|---|---|---|---|---|---|
| Micropapillary | Squamous Differentiation | |||||||
| Total | PD-L1 Score on TICs | p | Total | PD-L1 Score on TICs | p | |||
| Negative | Positive | Negative | Positive | |||||
| N | 44 (100.0) | 26 (59.1) | 18 (40.1) | 46 (100.0) | 14 (30.4) | 32 (69.6) | ||
| Age | 0.888 | 0.371 | ||||||
| <68.0 | 19 (43.2) | 11 (57.9) | 8 (42.1) | 25 (54.3) | 9 (36.0) | 16 (60.0) | ||
| ≥68.0 | 25 (56.8) | 15 (60.0) | 10 (40.0) | 21 (45.7) | 5 (23.8) | 16 (72.2) | ||
| Sex | 0.375 | 1.000 | ||||||
| Male | 38 (86.4) | 21 (55.3) | 17 (44.7) | 39 (84.8) | 12 (30.8) | 27 (69.2) | ||
| Female | 6 (13.6) | 5 (83.3) | 1 (16.7) | 7 (15.2) | 2 (28.6) | 5 (71.4) | ||
| Tumor stage | 0.467 | 0.005 | ||||||
| ≤pT2 | 20 (45.5) | 13 (65.0) | 7 (35.0) | 16 (34.8) | 9 (56.2) | 7 (43.8) | ||
| ≥pT3 | 24 (54.5) | 13 (54.2) | 11 (45.8) | 30 (65.2) | 5 (16.7) | 25 (83.3) | ||
| Concomitant CIS | 0.510 | 0.611 | ||||||
| Yes | 27 (61.4) | 17 (63.0) | 10 (37.0) | 19 (41.3) | 5 (26.3) | 14 (73.7) | ||
| No | 17 (38.6) | 9 (52.9) | 8 (47.1) | 27 (58.7) | 9 (33.3) | 18 (66.7) | ||
| LVI | 0.977 | 0.555 | ||||||
| Yes | 27 (61.4) | 16 (59.3) | 11 (40.7) | 20 (43.5) | 7 (35.0) | 13 (65.0) | ||
| No | 17 (38.6) | 10 (58.8) | 7 (41.2) | 26 (56.5) | 7 (26.9) | 19 (73.1) | ||
| Lymph node positivity | 0.030 | 0.188 | ||||||
| Negative | 19 (43.2) | 15 (78.9) | 4 (21.1) | 28 (60.9) | 11 (39.3) | 17 (60.7) | ||
| Positive | 25 (56.8) | 11 (44.0) | 14 (56.0) | 18 (39.1) | 3 (16.7) | 15 (83.3) | ||
| Variables | Micropapillary | Squamous Differentiation | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p | HR | 95% CI | p | |
| Age | ||||||
| <68.0 | ref. | ref. | ||||
| ≥68.0 | 1.01 | 0.992–1.043 | 0.151 | 1.04 | 0.963–1.082 | 0.260 |
| Sex | ||||||
| Male | ref. | ref. | ||||
| Female | 1.23 | 0.535–2.231 | 0.532 | 1.44 | 0.441–2.753 | 0.762 |
| Tumor stage | ||||||
| ≤pT2 | ref. | ref. | ||||
| ≥pT3 | 2.24 | 1.430–4.262 | 0.022 | 2.03 | 1.421–3.757 | 0.010 |
| Concomitant CIS | ||||||
| No | ref. | ref. | ||||
| Yes | 1.30 | 0.692–2.433 | 0.410 | 1.17 | 0.716–1.632 | 0.343 |
| LVI | ||||||
| No | ref. | ref. | ||||
| Yes | 1.65 | 1.240–2.530 | 0.038 | 1.44 | 0.993–2.046 | 0.062 |
| Lymph node positivity | ||||||
| Negative | ref. | ref. | ||||
| Positive | 3.02 | 1.782–5.428 | 0.001 | 2.49 | 1.672–3.631 | 0.004 |
| Surgical margin status | ||||||
| Negative | ref. | ref. | ||||
| Positive | 1.32 | 0.970–2.026 | 0.092 | 1.46 | 0.820–2.382 | 0.264 |
| PD-L1 in TICs | ||||||
| Negative | ref. | ref. | ||||
| Positive | 1.85 | 1.323–2.672 | 0.017 | 1.58 | 1.162–2.780 | 0.032 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, J.-H.; Lee, C.-U.; Lee, D.-H.; Song, W. Expression and Prognostic Implication of PD-L1 in Patients with Urothelial Carcinoma with Variant Histology (Squamous Differentiation or Micropapillary) Undergoing Radical Cystectomy. Biomedicines 2022, 10, 910. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040910
Chung J-H, Lee C-U, Lee D-H, Song W. Expression and Prognostic Implication of PD-L1 in Patients with Urothelial Carcinoma with Variant Histology (Squamous Differentiation or Micropapillary) Undergoing Radical Cystectomy. Biomedicines. 2022; 10(4):910. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040910
Chicago/Turabian StyleChung, Jae-Hoon, Chung-Un Lee, Dong-Hyeon Lee, and Wan Song. 2022. "Expression and Prognostic Implication of PD-L1 in Patients with Urothelial Carcinoma with Variant Histology (Squamous Differentiation or Micropapillary) Undergoing Radical Cystectomy" Biomedicines 10, no. 4: 910. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040910