
The Immunogenicity and Safety of Three Types of SARS-CoV-2 Vaccines in Adult Patients with Immune-Mediated Inflammatory Diseases: A Longitudinal Cohort Study

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
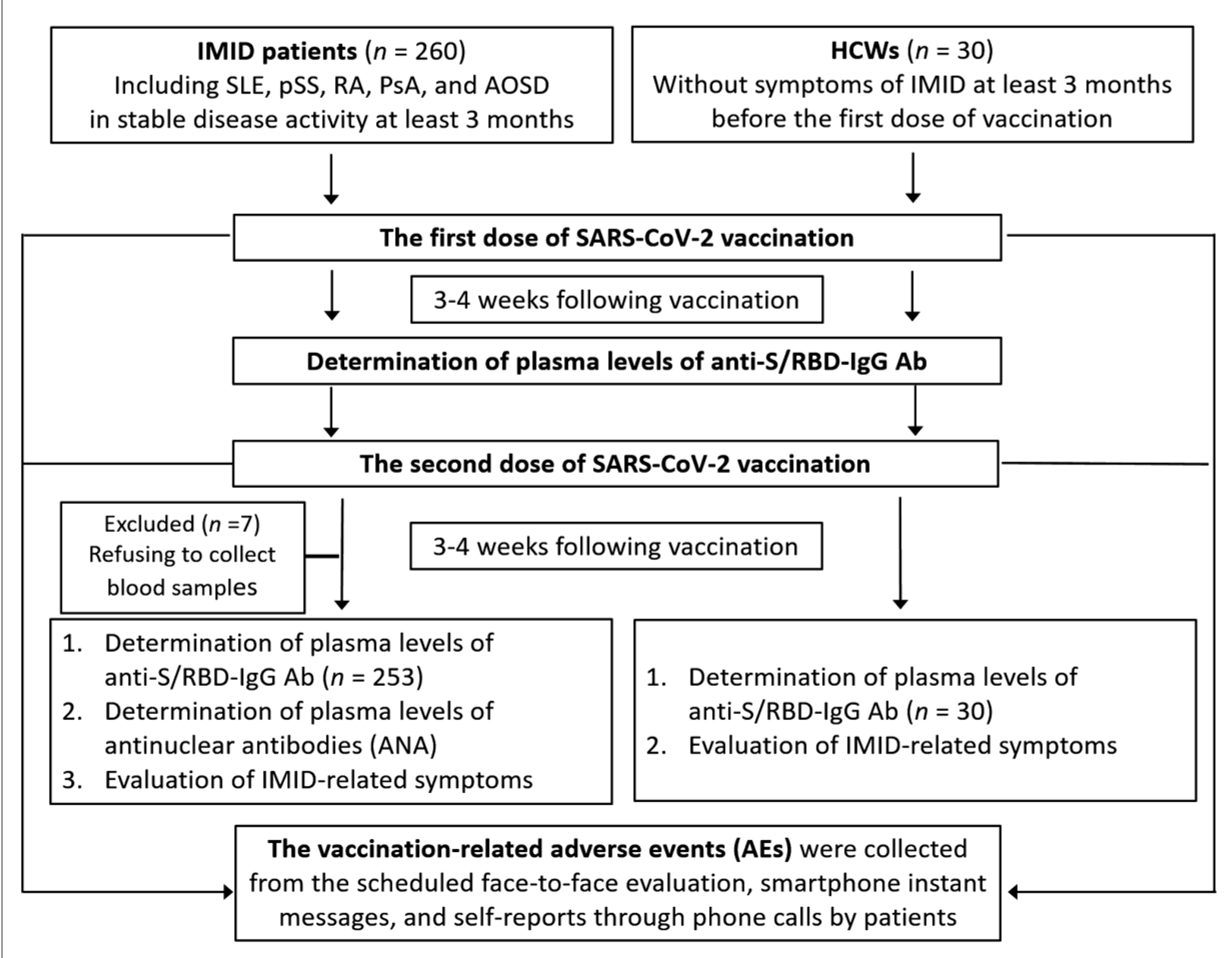
2.1. Patients and Study Design
2.2. Determination of Plasma Levels of SARS-CoV-2 Antibody-IgG
2.3. Determination of Antinuclear Antibodies (ANA) and Anti-Platelet Factor 4 (PF4) Antibodies
2.4. The Adverse Events during the 6-Month Follow-up Period after the First-Dose Vaccine
2.5. Statistical Analysis
3. Results
3.1. Demographic Data and Clinical Characteristics of the Enrolled Subjects
3.2. Comparisons of Anti-S/RBD-IgG Positive Rates and Titers among Different Groups
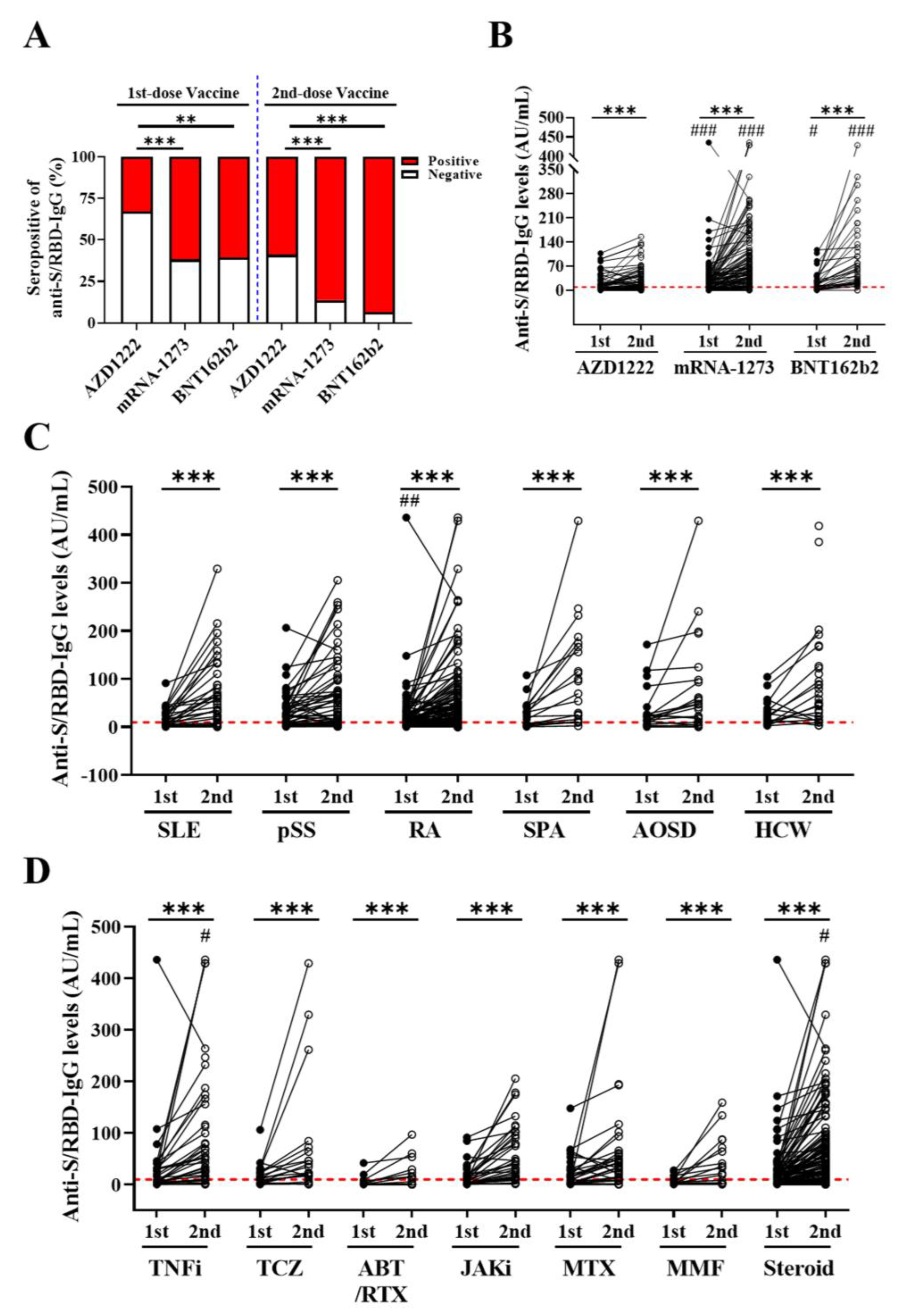
3.2.1. Comparisons of Anti-S/RBD-IgG Positive Rates and Titers among the Different Types of SARS-CoV-2 Vaccines
3.2.2. Comparisons of Anti-S/RBD-IgG Positive Rates and Titers among the Different Groups of Participants
3.2.3. Comparisons of the Anti-S/RBD-IgG Positive Rates and Titers in Patients Receiving Different the Immunosuppressants, csDMARDs, bDMARDs, and tsDMARDs
3.3. Logistic Regression Analysis for Predicting the Lack of Immunogenicity in IMID Patients
3.4. Safety of COVID-19 Vaccines in IMID Patients
3.5. Logistic Regression Analysis for Predicting the Occurrence of AEs in IMID Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sadarangani, M.; Marchant, A.; Kollmann, T.R. Immunological mechanisms of vaccine-induced protection against COVID-19 in humans. Nat. Rev. Immunol. 2021, 21, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARSCoV-2: A preliminary report of a phase 1/2, single-blind, randomized controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Jackson, L.A.; Anderson, E.J.; Rouphael, N.G.; Roberts, P.C.; Makhene, M.; Coler, R.N.; McCullough, M.P.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; et al. An mRNA vaccine against SARS-CoV-2 -preliminary report. N. Engl. J. Med. 2020, 383, 1920–1931. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.C.; Guan, X.H.; Li, Y.H.; Huang, J.Y.; Jiang, T.; Hou, L.H.; Li, J.X.; Yang, B.F.; Wang, L.; Wang, W.J.; et al. Immunogenicity and safety of a recombinant adenovirus type-5-vectored COVID-19 vaccine in healthy adults aged 18 years or older: A randomized, double-blind, placebo controlled, phase 2 trial. Lancet 2020, 396, 479–488. [Google Scholar] [CrossRef]
- MHRA. Public Assessment Report, National Procedure, Vaxzevria (Previously COVID-19 Vaccine AstraZeneca, Suspension for Injection) COVID-19 Vaccine (ChAdOx1-S [Recombinant]). 19 July 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1003840/CMA_UKPAR_COVID_19_Vaccine_AstraZeneca_PAR_16.07.2021.pdf (accessed on 9 August 2021).
- Ewer, K.J.; Barrett, J.R.; Belij-Rammerstorfer, S.; Sharpe, H.; Makinson, R.; Morter, R.; Flaxman, A.; Wright, D.; Bellamy, D.; Bittaye, M.; et al. T cell and antibody responses induced by a single dose of ChAdOx1 nCoV-19 (AZD1222) vaccine in a phase 1/2 clinical trial. Nat. Med. 2021, 27, 270–278. [Google Scholar] [CrossRef] [PubMed]
- Barrett, J.R.; Belij-Rammerstorfer, S.; Dold, C.; Ewer, K.J.; Folegatti, P.M.; Gilbride, C.; Halkerston, R.; Hill, J.; Jenkin, D.; Stockdale, L.; et al. Phase 1/2 trial of SARS-CoV-2 vaccine ChAdOx1 nCoV-19 with a booster dose induces multifunctional antibody responses. Nat. Med. 2021, 27, 279–288. [Google Scholar] [CrossRef]
- Anderson, E.J.; Rouphael, N.G.; Widge, A.T.; Jackson, L.A.; Roberts, P.C.; Makhene, M.; Chappell, J.D.; Denison, M.R.; Stevens, L.J.; Pruijssers, A.J.; et al. Safety and immunogenicity of SARS-CoV-2 mRNA-1273 vaccine in older adults. N. Engl. J. Med. 2020, 383, 2427–2438. [Google Scholar] [CrossRef]
- Mulligan, M.J.; Lyke, K.E.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Raabe, V.; Bailey, R.; Swanson, K.A.; et al. Phase I/II study of COVID-19 RNA vaccine BNT162b1 in adults. Nature 2020, 586, 589–593. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W., Jr.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and immunogenicity of two RNA-based Covid-19 vaccine candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Medeiros-Ribeiro, A.C.; Aikawa, N.E.; Saad, C.G.S.; Yuki, E.F.N.; Pedrosa, T.; Fusco, S.R.G.; Rojo, P.T.; Pereira, R.M.R.; Shinjo, S.K.; Andrade, D.C.O.; et al. Immunogenicity and safety of the CoronVac inactivated vaccine in patients with autoimmune rheumatic diseases: A phase 4 trial. Nat. Med. 2021, 27, 1744–1751. [Google Scholar] [CrossRef]
- Shinjo, S.K.; de Souza, F.H.C.; Borges, I.B.P.; Dos Santos, A.M.; Miossi, R.; Misse, R.G.; Medeiros-Ribeiro, A.C.; Saad, C.G.S.; Yuki, E.F.N.; Pasoto, S.G.; et al. Systemic autoimmune myopathies: A prospective phase 4 controlled trial of an inactivated virus vaccine against SARS-CoV-2. Rheumatology 2021. [Google Scholar] [CrossRef] [PubMed]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicenter study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Arnold, J.; Winthrop, K.; Emery, P. COVID-19 vaccination and antirheumatic therapy. Rheumatology 2021, 60, 3496–3502. [Google Scholar] [CrossRef] [PubMed]
- Prendecki, M.; Clarke, C.; Edwards, H.; McIntyre, S.; Mortimer, P.; Gleeson, S.; Martin, P.; Thomson, T.; Randell, P.; Shah, A.; et al. Humoral and T-cell responses to SARS-CoV-2 vaccination in patients receiving immunosuppression. Ann. Rheum. Dis. 2021, 80, 1322–1329. [Google Scholar] [CrossRef]
- Malipiero, G.; Moratto, A.; Infantino, M.; D’Agaro, P.; Piscianz, E.; Manfredi, M.; Grossi, V.; Benvenuti, E.; Bulgaresi, M.; Benucci, M.; et al. Assessment of humoral and cellular immunity induced by the BNT162b2 SARS-CoV-2 vaccine in healthcare workers, elderly people, and immunosuppressed patients with autoimmune disease. Immunological. Res. 2021, 69, 576–583. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.; Betschel, S.D.; Cheung, M.; Hicks, L.K. Vaccine response following anti-CD20 therapy: A systemic review and meta-analysis of 905 patients. Blood Adv. 2021, 5, 2624. [Google Scholar] [CrossRef]
- Geisen, U.M.; Berner, D.K.; Tran, F.; Sümbül, M.; Vullriede, L.; Ciripoi, M.; Reid, H.M.; Schaffarzyk, A.; Longardt, A.C.; Franzenburg, J.; et al. Immunogenicity and safety of anti-SARS-CoV-2 mRNA vaccines in patients with chronic inflammatory conditions and immunosuppressive therapy in a monocentric cohort. Ann. Rheum. Dis. 2021, 80, 1306–1311. [Google Scholar] [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1997, 40, 1725. [Google Scholar] [CrossRef]
- Vitali, C.; Bombardieri, S.; Jonsson, R.; Moutsopoulos, H.M.; Alexander, E.L.; Carsons, S.E.; Daniels, T.E.; Fox, P.C.; Fox, R.I.; Kassan, S.S.; et al. Classification criteria for Sjogren’s syndrome: A revised version of the European criteria proposed by the American-European Consensus Group. Ann. Rheum. Dis. 2002, 61, 554–558. [Google Scholar] [CrossRef] [Green Version]
- Aletaha, D.; Neogi, T.; Silman, A.J.; Funovits, J.; Felson, D.T.; Bingham, C.O., 3rd; Birnbaum, N.S.; Burmester, G.R.; Bykerk, V.P.; Cohen, M.D.; et al. 2010 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010, 62, 2569–2581. [Google Scholar] [CrossRef]
- Van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis: A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.; Gladman, D.; Helliwell, P.; Marchesoni, A.; Mease, P.; Mielants, H.; CASPAR Study Group. Classification criteria for psoriatic arthritis: Development of New Criteria from a Large International Study. Arthritis Rheum. 2006, 54, 2665–2673. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, M.; Ohta, A.; Tsunematsu, T.; Kasukawa, R.; Mizushima, Y.; Kashiwagi, H.; Kashiwazaki, S.; Tanimoto, K.; Matsumoto, Y.; Ota, T.; et al. Preliminary criteria for classification of adult Still’s disease. J. Rheumatol. 1992, 19, 424–430. [Google Scholar] [PubMed]
- Poland, G.A.; Ovsyannikova, I.G.; Crooke, N.; Kennedy, R.B. SARS-CoV-2 Vaccine Development: Current Status. Mayo Clin Proc. 2020, 95, 2172–2188. [Google Scholar] [CrossRef]
- Tai, W.; Zhang, X.; Drelich, A.; Shi, J.; Hsu, J.C.; Luchsinger, L.; Hillyer, C.D.; Tseng, C.K.; Jiang, S.; Du, L. A novel receptor binding domain (RBD)-based mRNA vaccine against SARS-CoV-2. Cell Res. 2020, 30, 932–935. [Google Scholar] [CrossRef]
- CTEP Cancer Therapy Evaluation Program. Common Terminology Criteria for Adverse Events (CTCAE) Versions 5.0. National Cancer Institute. 2017. Available online: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm#ctc_50 (accessed on 24 February 2022).
- Yang, J.; Wang, W.; Chen, Z.; Lu, S.; Yang, F.; Bi, Z.; Bao, L.; Mo, F.; Li, X.; Huang, Y.; et al. A vaccine targeting the RBD of the S protein of SARS-CoV-2 induces protective immunity. Nature 2020, 586, 572–577. [Google Scholar] [CrossRef]
- Curtis, J.R.; Johnson, S.R.; Anthony, D.D.; Arasaratnam, R.J.; Baden, L.R.; Bass, A.R.; Calabrese, C.; Gravallese, E.M.; Harpaz, R.; Sadun, R.E.; et al. American College of rheumatology guidance for COVID-19 vaccination in patients with rheumatic and musculoskeletal diseases: Version 1. Arthritis Rheumatol. 2021, 73, 1093–1107. [Google Scholar] [CrossRef]
- Naranbhai, V.; Garcia-Beltran, W.F.; Chang, C.C.; Mairena, C.B.; Thierauf, J.C.; Kirkpatrick, G.; Onozato, M.L.; Cheng, J.; St Denis, K.J.; Lam, E.C.; et al. Comparative immunogenicity and effectiveness of mRNA-1273, BNT16%2b2, and Ad26.COV2.S CoV-19 vaccines. J. Infect. Dis. 2021, 593, jiab593. [Google Scholar]
- Sablerolles, R.S.G.; Rietdijk, W.J.R.; Goorhuis, A.; Postma, D.F.; Visser, L.G.; Geers, D.; Schmitz, K.S.; Garcia Garrido, H.M.; Koopmans, M.P.G.; Dalm, V.A.S.H.; et al. Immunogenicity and reactogenicity of booster vaccinations after Ad26.COV2.S priming. N. Engl. J. Med. 2022, 386, 951–963. [Google Scholar] [CrossRef]
- Boyarsky, B.J.; Ruddy, J.A.; Connolly, C.M.; Ou, M.T.; Werbel, W.A.; Garonzik-Wang, J.M.; Segev, D.L.; Paik, J.J. Antibody response to a single dose of SARS-CoV-2 mRNA vaccine in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1098–1099. [Google Scholar] [CrossRef]
- Ciarambino, T.; Barbagelata, E.; Corbi, G.; Ambrosino, I.; Politi, C.; Lavalle, F.; Ruggieri, A.; Maretti, A.M. Gender differences in vaccine therapy: Where are we in COVID-19 pandemic? Monaldi. Arch. Chest. Dis. 2021, 91, 1669. [Google Scholar] [CrossRef] [PubMed]
- Ruddy, J.A.; Connolly, C.M.; Boyarsky, B.J.; Werbel, W.A.; Christopher-Stine, L.; Garonzik-Wang, J.; Segev, D.L.; Paik, J.J. High antibody response to two-dose SARS-CoV-2 messenger RNA vaccination in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1351–1352. [Google Scholar] [CrossRef] [PubMed]
- Braun-Moscovici, Y.; Kaplan, M.; Braun, M.; Markovits, D.; Giryes, S.; Toledano, K.; Tavor, Y.; Dolnikov, K.; Balbir-Gurman, A. Disease activity and humoral response in patients with inflammatory rheumatic diseases after two doses of the Pfizer mRNA vaccine against SARS-CoV-2. Ann. Rheumd. Dis. 2021, 80, 1317–1321. [Google Scholar] [CrossRef] [PubMed]
- D’Amelio, R.; Asero, R.; Cassatella, M.A.; Laganà, B.; Lunardi, C.; Migliorini, P.; Nisini, R.; Parronchi, P.; Quinti, I.; Racanelli, V.; et al. Anti-COVID-19 vaccination in patients with autoimmune-autoinflammatory disorders and primary/secondary immunodeficiencies: The position of the Task Force on behalf of the Italian Immunological Societies. Biomedicines 2021, 9, 1163. [Google Scholar] [CrossRef] [PubMed]
- Murdaca, G.; Noberasco, G.; Olobardi, D.; Lunardi, C.; Maule, M.; Delfino, L.; Triggiani, M.; Cardamone, C.; Benfaremo, D.; Moroncini, G.; et al. Current take on systemic sclerosis patients’ vaccination recommendations. Vaccines 2021, 9, 1426. [Google Scholar] [CrossRef]
- Firinu, D.; Perra, A.; Campagna, M.; Littera, R.; Fenu, G.; Meloni, F.; Cipri, S.; Sedda, F.; Conti, M.; Miglianti, M.; et al. Evaluation of antibody response to BNT162b2 mRNA COVID-19 vaccine in patients affected by immune-mediated inflammatory disease up to 5 months after vaccination. Clin. Exp. Med. 2021, 1–9. [Google Scholar] [CrossRef]
- Seror, R.; Camus, M.; Salmon, J.H.; Roux, C.; Dernis, E.; Basch, A.; Germain, V.; Leske, C.; Brousseau, S.; Truchetet, M.E.; et al. Do JAK inhibitors affect immune response to COVID-19 vaccination? Data from the MAJIK-SFR Registry. Lancet Rheumatol. 2022, 4, e8–e10. [Google Scholar] [CrossRef]
- Haberman, R.H.; Herati, R.; Simon, D.; Samanovic, M.; Blank, R.B.; Tuen, M.; Koralov, S.B.; Atreya, R.; Tascilar, K.; Allen, J.R.; et al. Methotrexate hampers immunogenicity to BNT162b2 mRNA COVID-19 vaccine in immune-mediated inflammatory disease. Ann. Rheum. Dis. 2021, 80, 1339–1344. [Google Scholar] [CrossRef]
- Tang, W.; Gartshteyn, Y.; Ricker, E.; Inzerillo, S.; Murray, S.; Khalili, L.; Askanase, A. The use of COVID-19 vaccines in patients with SLE. Curr. Rheumatol. Rep. 2021, 23, 79. [Google Scholar] [CrossRef]
- Plymate, L.C.; Pepper, G.; Krist, M.P.; Koelle, D.M. Immunogenicity of repeat COVID-19 mRNA vaccinations in a patient with myasthenia gravis receiving mycophenolate, prednisone, and eculizuma. J. Transl. Autoimmun. 2021, 4, 100114. [Google Scholar] [CrossRef]
- Connolly, C.M.; Ruddy, J.A.; Boyarsky, B.J.; Avery, R.K.; Werbel, W.A.; Segev, D.L.; Garonzik-Wang, J.; Paik, J.J. Safety of the first dose of mRNA SARS-CoV-2 vaccines in patients with rheumatic and musculoskeletal diseases. Ann. Rheum. Dis. 2021, 80, 1100–1101. [Google Scholar] [CrossRef] [PubMed]
- Hernández, A.F.; Calina, D.; Poulas, K.; Docea, A.O.; Tsatsakis, A.M. Safety of COVID-19 vaccines administered in the EU: Should we be concerned? Toxicol. Rep. 2021, 8, 871–879. [Google Scholar] [CrossRef] [PubMed]
- Rotondo, C.; Cantatore, F.P.; Fornaro, M.; Colia, R.; Busto, G.; Rella, V.; Sciacca, S.; Lops, L.; Cici, D.; Maruotti, N.; et al. Preliminary data on post market safety profile of CVID-19 vaccines in rheumatic diseases: Assessment on various vaccines in use, different rheumatic disease subtypes, and immunosuppressive therapies: A two-centers study. Vaccines 2021, 9, 730. [Google Scholar] [CrossRef] [PubMed]
- Watad, A.; De Marco, G.; Mahajna, H.; Druyan, A.; Eltity, M.; Hijazi, N.; Haddad, A.; Elias, M.; Zisman, D.; Naffaa, M.E.; et al. Immune-mediated disease flares or new-onset disease in 27 subjects following mRNA/DNA SARS-CoV-2 vaccination. Vaccines 2021, 9, 435. [Google Scholar] [CrossRef]
- Gentiloni, M.M.L.; Paci, V.; Marconi, V.; Gigli, M.; Benfaremo, D.; Sordillo, R.; Macchini, C.; Massaccesi, L.; Perna, G.P.; Offidani, A.M.; et al. SARS-COV-2 Infection, vaccination, and immune-mediated diseases: Results of a single-center retrospective study. Front. Immunol. 2022, 13, 859550. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | SLE (n = 36) | pSS (n = 60) | RA (n = 110) | SpA (n = 23) | AOSD (n = 24) | HCWs (n = 30) |
|---|---|---|---|---|---|---|
| Age at study entry, years | 44.6 ± 14.3 | 61.2 ± 12.2 ***,# | 61.2 ± 12.9 ***,#,$ | 50.0 ± 16.6 | 49.9 ± 15.2 | 44.1 ± 15.4 |
| Female proportion, n (%) | 35 (97.2%) | 56 (93.3%) | 94 (85.5%) | 11 (47.8%) | 19 (79.2%) | 23 (76.7%) |
| BMI, kg/m2 | 22.7 ± 3.8 | 23.1 ± 3.4 | 23.2 ± 3.5 | 24.2 ± 4.2 | 24.0 ± 4.6 | 24.6 ± 7.0 |
| SARS-CoV-2 vaccine type | ||||||
| AZD1222/ChAdOx1 | 14 (38.9%) | 33 (55.0%) | 36 (32.7%) | 7 (30.4%) | 9 (37.5%) | 14 (46.7%) |
| The mRNA-1273 | 14 (38.9%) | 26 (43.3%) | 56 (50.9%) | 9 (39.2%) | 9 (37.5%) | 15 (50.0%) |
| BNT162b2 | 8 (22.2%) | 1 (1.7%) | 18 (16.4%) | 7 (30.4%) | 6 (25.0%) | 1 (3.3%) |
| Seropositive rate, n (%) after 1st dose-vaccine | 16 (44.4%) | 31 (51.7%) | 41 (37.3%) | 11 (47.8%) | 14 (58.3%) | 9 (30.0%) |
| Anti-S/RBD-IgG, AU/mL, after 1st-dose vaccine | 12.8 (2.8–30.7) | 21.5 (3.4–43.0) §§ | 6.1 (1.6–19.6) | 26.8 (5.8–43.5) §§ | 20.7 (6.2–41.7) | 21.4 (8.6–7.3) |
| Seropositive rate, n (%) after 2nd-dose vaccine | 29 (80.6%) | 47 (78.3%) | 81 (73.6%) | 21 (91.3%) | 19 (79.2%) | 26 (86.7%) |
| Anti-S/RBD-IgG, AU/mL, after 2nd dose-vaccine | 50.3 (17.3–104.9) ††† | 46.5 (11.6–99.1) ††† | 29.8 (9.0–72.9) ††† | 69.5 (15.6–166.5) ††† | 44.2 (10.6–96.9) †† | 54.0 (19.9–123.4) † |
| The used corticosteroids | ||||||
| Prednisolone ≤ 15 mg/day | 30 (83.3%) | 10 (16.7%) | 58 (52.7%) | 5 (21.7%) | 15 (62.5%) | NA |
| Prednisolone >15 mg/day | 4 (11.1%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 1 (4.2%) | NA |
| The used csDMARDs | ||||||
| Methotrexate | 0 (0%) | 0 (0.0%) | 24 (21.8%) | 2 (8.7%) | 10 (41.7%) | NA |
| Hydroxychloroquine | 34 (94.4%) | 55 (91.7%) | 50 (45.5%) | 0 (0.0%) | 19 (79.2%) | NA |
| Azathioprine | 14 (38.9%) | 1 (1.7%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | NA |
| Cyclosporine | 5 (13.9%) | 1 (1.7%) | 2 (1.8%) | 0 (0.0%) | 2 (8.3%) | NA |
| MMF ≤ 2 gm/day | 12 (33.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | NA |
| MMF >2 gm/day | 3 (8.3%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | NA |
| The used biologics | ||||||
| TNF-α inhibitors | 0 (0.0%) | 0 (0.0%) | 35 (31.8%) | 13 (56.5%) | 0 (0.0%) | NA |
| IL-6R inhibitor | 0 (0.0%) | 0 (0.0%) | 23 (20.9%) | 0 (0.0%) | 4 (16.7%) | NA |
| Abatacept | 1 (2.7%) | 0 (0.0%) | 11 (10.0%) | 0 (0.0%) | 1 (4.2%) | NA |
| Rituximab | 1 (2.7%) | 1 (1.7%) | 5 (4.5%) | 0 (0.0%) | 0 (0.0%) | NA |
| The used JAKi | 0 (0.0%) | 0 (0.0%) | 38 (34.5%) | 1 (4.3%) | 0 (0.0%) | NA |
| Comorbidities | ||||||
| Hypertension | 11 (30.6%) | 10 (16.7%) | 21 (19.1%) | 4 (17.4%) | 3 (12.5%) | 0 (0.0%) |
| Diabetes mellitus | 3 (8.3%) | 5 (8.3%) | 10 (9.1%) | 1 (4.3%) | 1 (4.2%) | 0 (0.0%) |
| Current smoker | 2 (5.6%) | 4 (6.7%) | 8 (7.3%) | 1 (4.3%) | 1 (4.2%) | 0 (0.0%) |
| Baseline Variables | Univariate Model | Multivariate Model | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |||
| Age at entry, years | 1.03 | (1.01- | 1.05) | 0.012 | ||||
| Gender | ||||||||
| Male | ref. | |||||||
| Female | 0.36 | (0.17- | 0.75) | 0.007 | 0.34 | (0.14- | 0.80) | 0.014 |
| Disease groups | 0.97 | (0.74- | 1.27) | 0.837 | ||||
| CKD | 5.64 | (2.46- | 12.95) | 0.001 | ||||
| The estimated GFR | 0.98 | (0.97- | 0.99) | 0.001 | ||||
| BMI, kg/m2 | 1.02 | (0.94- | 1.11) | 0.593 | ||||
| The used medications | ||||||||
| TNF-α inhibitors | 0.70 | (0.27- | 1.77) | 0.445 | ||||
| Tocilizumab | 1.27 | (0.48- | 3.39) | 0.633 | ||||
| ABT/RTX | 2.98 | (1.06- | 8.42) | 0.039 | 4.19 | (1.25- | 14.09) | 0.021 |
| JAK inhibitors | 0.51 | (0.19- | 1.37) | 0.178 | ||||
| Methotrexate | 1.21 | (0.53- | 2.74) | 0.655 | ||||
| Mycophenolate | 2.03 | (0.71- | 5.76) | 0.183 | ||||
| Corticosteroids | 0.89 | (0.49- | 1.62) | 0.771 | ||||
| Type of vaccines | ||||||||
| AZ12222 | 5.29 | (2.80- | 10.00) | 0.001 | 7.21 | (1.96- | 26.57) | 0.003 |
| mRNA-1273 | 0.38 | (0.20- | 0.72) | 0.003 | ||||
| BNT162b2 | 0.20 | (0.06- | 0.68) | 0.01 | ||||
| Adverse Events (AEs) | AZD1222 (n = 90) N (%) Interval (Days) | mRNA-1273 (n = 117) N (%) Interval (Days) | BNT162b2 (n = 46) N (%) Interval (Days) | |||
|---|---|---|---|---|---|---|
| Injection site pain/skin rash | ||||||
| Grade 1 or 2 | 9 (10.0%) | 1.0 (0.7–1.5) | 16 (13.7%) | 1.0 (0.8–1.4) | 8 (17.4%) | 1.0 (1.0–1.3) |
| Grade 3 | 2 (2.2%) | 1.8 (1.6–2.0) | 3 (2.6%) | 1.5 (1.3–1.5) | 2 (4.3%) | 1.8 (1.6–1.9) |
| Grade 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Flu-like symptoms a Grade 1 or 2 Grade 3 Grade 4 Allergic reaction b | 8 (8.9%) 2 (2.2%) 0 (0.0%) | 1.5 (1.0–1.5) 1.3 (1.1–1.4) | 10 (8.5%) 2 (1.7%) 0 (0.0%) | 1.5 (1.1–1.9) 1.8 (1.6–1.9) | 4 (8.7%) 1 (2.2%) 0 (0.0%) | (1.0–1.3) 1.5 |
| Grade 1 or 2 | 3 (3.3%) | 1.0 (0.8–1.3) | 6 (5.1%) | 0.9 (0.7–1.0) | 2 (4.3%) | 0.9 (0.9–1.0) |
| Grade 3 Grade 4 Gastrointestinal symptoms c Grade 1 or 2 Grade 3 Grade 4 Neurological symptoms d Grade 1 or 2 Grade 3 | 1 (1.1%) 0 (0.0%) 4 (4.4%) 2 (2.2%) 0 (0.0%) 0 (0.0%) 1 (1.1%) | 1.5 1.8 (1.4–2.0) 1.8 (1.6–1.9) 14.0 | 0 (0.0%) 0 (0.0%) 4 (3.4%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) | 1.8 (1.4–2.0) | 0 (0.0%) 0 (0.0%) 1 (2.2%) 0 (0.0%) 0 (0.0%) 0 (0.0%) 0 (0.0%) | 2.0 |
| Grade 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Cardiovascular symptoms e | ||||||
| Grade 1 or 2 | 1 (1.1%) | 2.5 | 6 (5.1%) | 2.0 (1.6–2.4) | 2 (4.3%) | 2.3 (2.1–2.4) |
| Grade 3 | 0 (0.0%) | 2 (1.7%) | 2.8 (2.7–2.9) | 1 (2.2%) | 3.0 | |
| Grade 4 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| VITT f | ||||||
| Grade 1 or 2 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Grade 3 | 0 (0.0%) | 0 (0.0%) | 0 (0.0%) | |||
| Grade 4 | 1 (1.1%) | 14.0 | 0 (0.0%) | 0 (0.0%) | ||
| Baseline Variables | Univariate Model | Multivariate Model | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |||
| Age at entry, years | 1.00 | (0.97- | 1.01) | 0.268 | ||||
| Gender | ||||||||
| Male | ref. | |||||||
| Female | 1.56 | (0.65- | 3.74) | 0.319 | ||||
| Disease groups | 0.86 | (0.66- | 1.11) | 0.247 | ||||
| CKD | 0.85 | (0.33- | 2.20) | 0.734 | ||||
| The estimated GFR | 1.00 | (0.99- | 1.02) | 0.507 | ||||
| BMI, kg/m2 | 1.04 | (0.96- | 1.12) | 0.304 | ||||
| The used medications | ||||||||
| TNF-α inhibitors | 0.062 | (0.01- | 0.47) | 0.007 | 0.07 | (0.01- | 0.53) | 0.010 |
| Tocilizumab | 0.82 | (0.29- | 2.32) | 0.713 | ||||
| ABT/RTX | 0.68 | (0.19- | 2.47) | 0.559 | ||||
| JAK inhibitors | 2.39 | (1.15- | 4.95) | 0.020 | ||||
| Methotrexate | 1.19 | (0.54- | 2.63) | 0.667 | ||||
| Mycophenolate | 1.28 | (0.43- | 3.78) | 0.657 | ||||
| Corticosteroids | 1.45 | (0.82- | 2.57) | 0.205 | ||||
| Type of vaccines | ||||||||
| AZ12222 | 1.38 | (0.77- | 2.48) | 0.277 | ||||
| mRNA-1273 | 0.83 | (0.47- | 1.48) | 0.534 | ||||
| BNT162b2 | 0.81 | (0.38- | 1.79) | 0.584 | ||||
| Baseline Variables | Univariate Model | Multivariate Model | ||||||
|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | p Value | OR | 95% CI | p Value | |||
| Age at entry, years | 1.00 | (0.98- | 1.02) | 0.707 | ||||
| Gender | ||||||||
| Male | ref. | |||||||
| Female | 2.53 | (1.00- | 6.41) | 0.05 | ||||
| Disease groups | ||||||||
| Systemic lupus erythematosus | 7.93 | (2.75- | 22.84) | 0.001 | 11.63 | (2.41- | 56.06) | 0.002 |
| Primary Sjögren’s syndrome | 0.63 | (0.32- | 1.24) | 0.182 | ||||
| Rheumatoid arthritis | 1.22 | (0.69- | 2.14) | 0.490 | ||||
| Spondyloarthropathies | 0.33 | (0.94- | 1.16) | 0.084 | ||||
| Adult-onset Still’s disease | 0.35 | (0.10- | 1.25) | 0.106 | ||||
| CKD | 0.50 | (0.18- | 1.40) | 0.189 | ||||
| The estimated GFR | 1.00 | (1.00 - | 1.02) | 0.199 | ||||
| BMI, kg/m2 | 0.95 | (0.88- | 1.03) | 0.186 | ||||
| The used medications | ||||||||
| TNF-α inhibitors | 1.26 | (0.61- | 2.60) | 0.536 | ||||
| Tocilizumab | 0.79 | (0.30- | 2.11) | 0.639 | ||||
| ABT/RTX | 1.32 | (0.46- | 3.79) | 0.606 | ||||
| JAK inhibitors | 0.47 | (0.19- | 1.12) | 0.090 | ||||
| Methotrexate | 1.09 | (0.50- | 2.40) | 0.827 | ||||
| Mycophenolate | 4.62 | (1.11- | 19.02) | 0.034 | ||||
| Corticosteroids | 1.03 | (0.59- | 1.81) | 0.919 | ||||
| Type of vaccines | ||||||||
| AZ12222 | 0.95 | (0.53- | 1.70) | 0.853 | ||||
| mRNA-1273 | 1.12 | (0.64- | 1.97) | 0.687 | ||||
| BNT162b2 | 0.88 | (0.40- | 1.96) | 0.756 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tien, N.; Chang, Y.-C.; Chen, P.-K.; Lin, H.-J.; Chang, S.-H.; Lan, J.-L.; Hsueh, P.-R.; Chang, C.-K.; Chen, D.-Y. The Immunogenicity and Safety of Three Types of SARS-CoV-2 Vaccines in Adult Patients with Immune-Mediated Inflammatory Diseases: A Longitudinal Cohort Study. Biomedicines 2022, 10, 911. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040911
Tien N, Chang Y-C, Chen P-K, Lin H-J, Chang S-H, Lan J-L, Hsueh P-R, Chang C-K, Chen D-Y. The Immunogenicity and Safety of Three Types of SARS-CoV-2 Vaccines in Adult Patients with Immune-Mediated Inflammatory Diseases: A Longitudinal Cohort Study. Biomedicines. 2022; 10(4):911. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040911
Chicago/Turabian StyleTien, Ni, Yu-Chang Chang, Po-Ku Chen, Hui-Ju Lin, Shih-Hsin Chang, Joung-Liang Lan, Po-Ren Hsueh, Ching-Kun Chang, and Der-Yuan Chen. 2022. "The Immunogenicity and Safety of Three Types of SARS-CoV-2 Vaccines in Adult Patients with Immune-Mediated Inflammatory Diseases: A Longitudinal Cohort Study" Biomedicines 10, no. 4: 911. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10040911