
Deep Learning-Based Computer-Aided Diagnosis of Rheumatoid Arthritis with Hand X-ray Images Conforming to Modified Total Sharp/van der Heijde Score

 ,
,  , , and
, , and
Abstract
:1. Introduction
1.1. AI in Imaging in RA
1.2. DL Applied to RA
2. Method and Materials
2.1. Image Collection and Deidentification Process
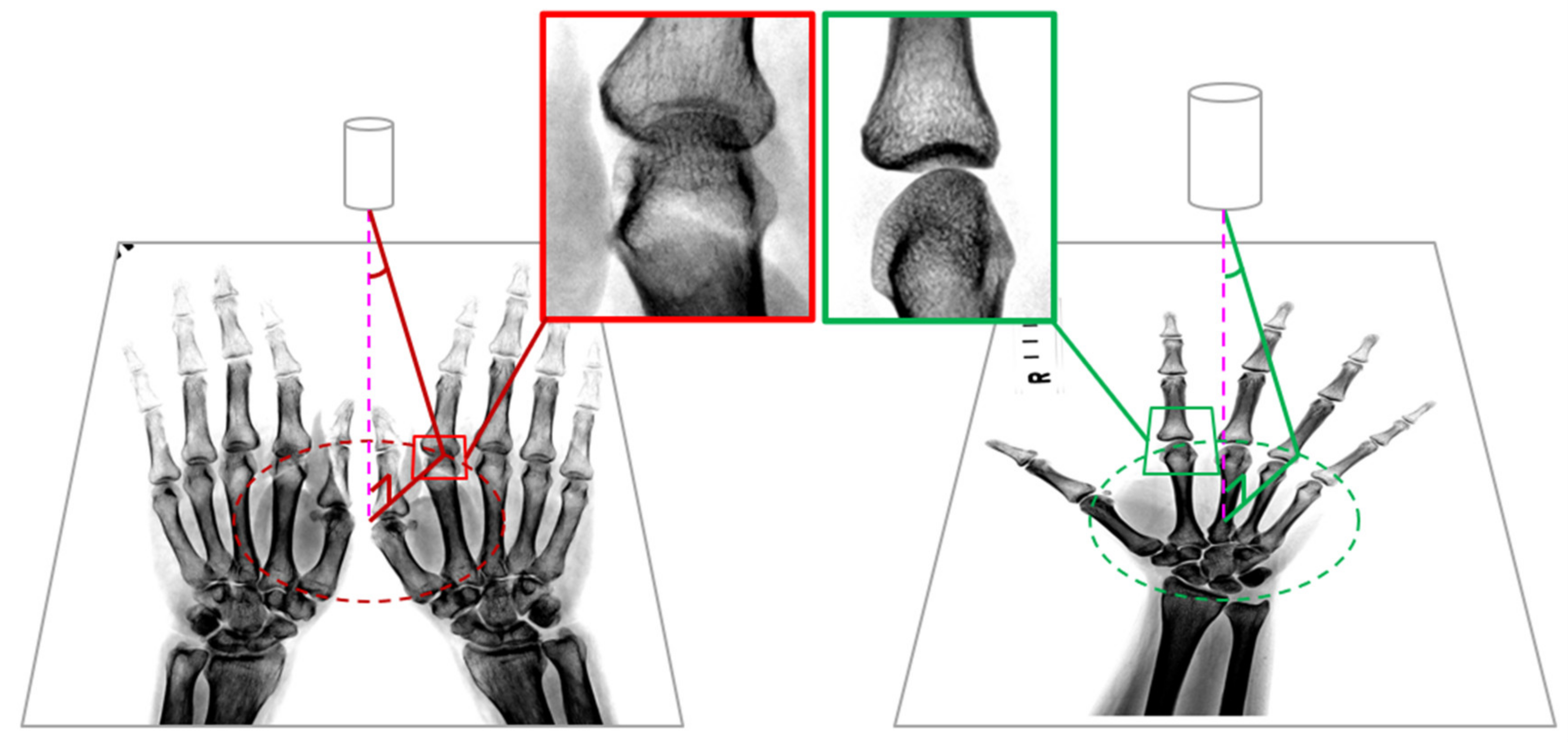
2.2. Definition of ROI
2.2.1. The Strategy of Labeling ROI
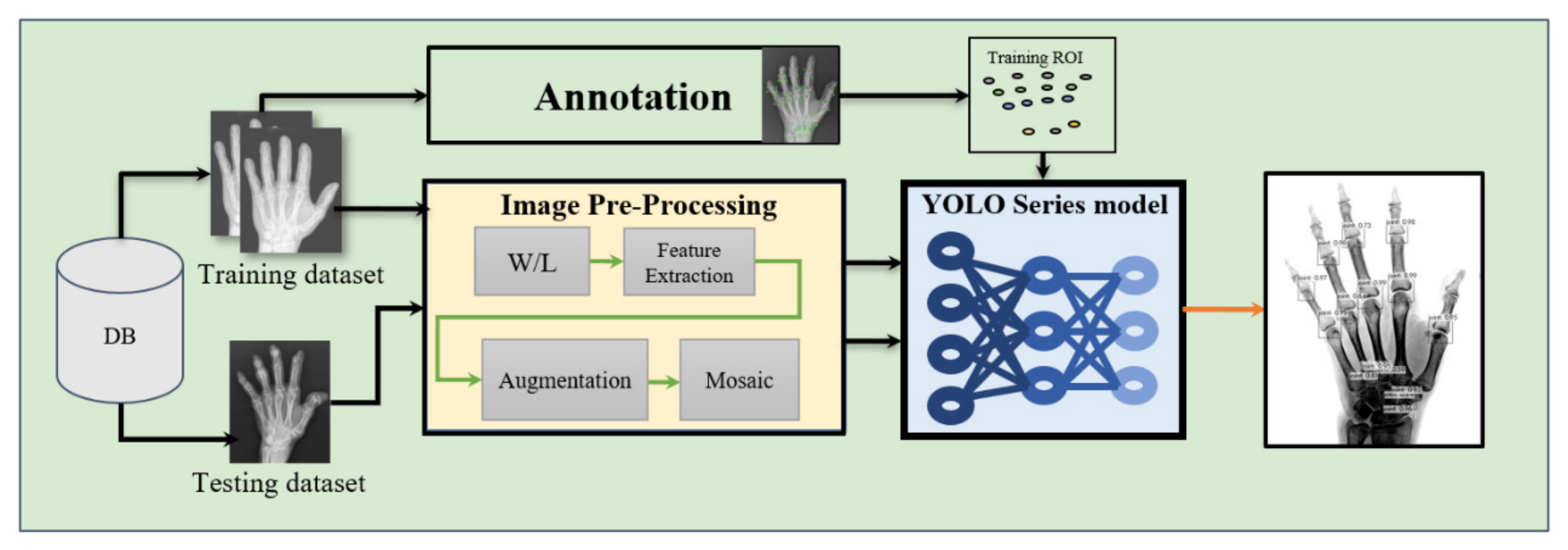
2.2.2. Image Preprocessing
2.2.3. Data Augmentation
2.2.4. DL Detection Model
2.2.5. Modified YOLO Model
- IoU loss, . This is simply the difference between 1 and the intersection of prediction box A and real box B.
- Generalized IoU (GIoU)-loss, GIoU-loss is used to alleviate the gradient problem of the above IoU loss when the detection frame does not overlap.
- Distance IoU (DIoU)-loss, DIoU-loss is a simple penalty added to minimize the standardized distance between the center points of the two detection frames, which can accelerate the convergence process of the loss.
- Completed IoU (CIoU)-loss, . Compared with DIoU-loss, CIoU-loss considers the aspect ratio information.
2.3. Joint Classification
2.3.1. DL Classification Model
2.3.2. Explainable Models
3. Results
3.1. Joint Localization
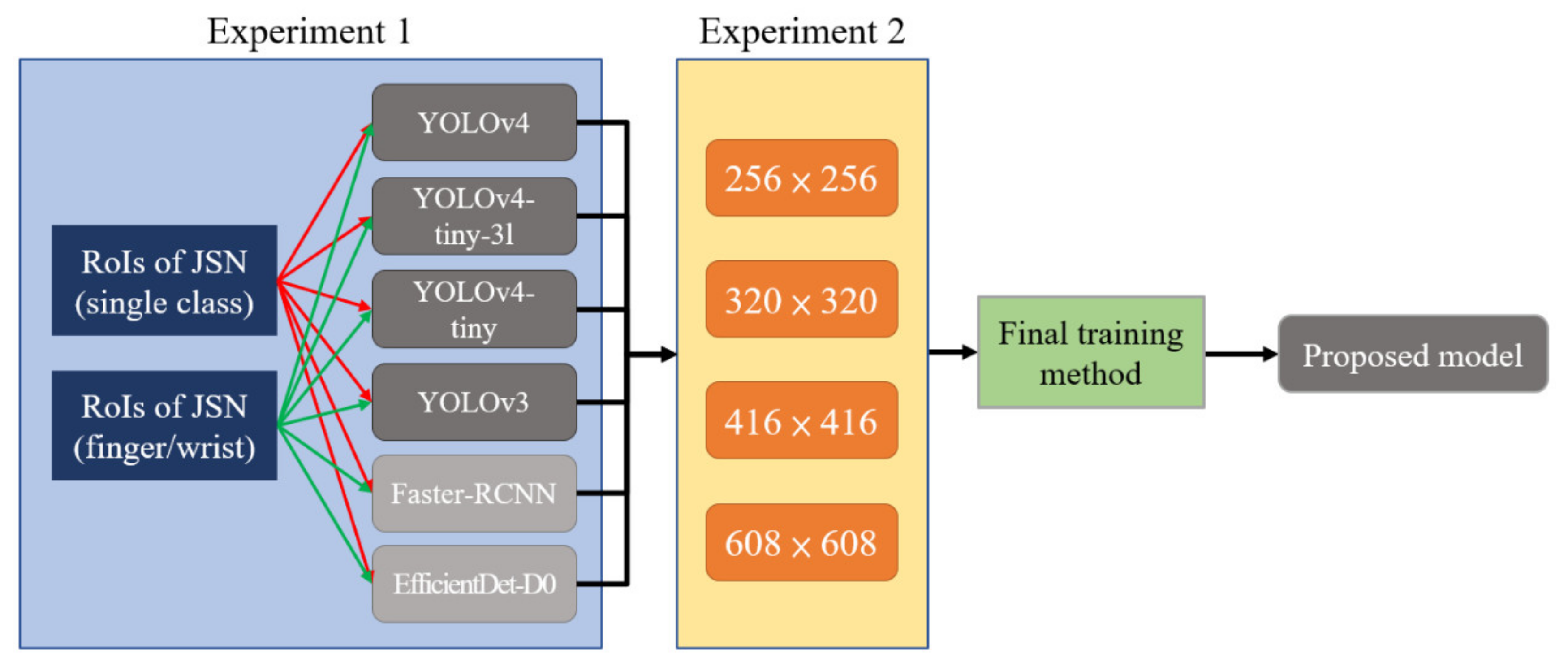
3.1.1. Comparison of Training Results
3.1.2. Model Testing and Analysis
3.2. Joint Classification
4. Discussion
5. Conclusions
- DL was used to establish a state-of-the-art model for automatically locating all hand joints of ROIs of JSN in “mTSS”.
- CIoU-loss was converted to the previous version of DIoU-loss when facing non-artificial objects and other materials where the aspect ratio does not need to be considered, thus helping improve the model accuracy.
- Experimental results showed that, considering the human visual ability to identify data quantity or quality, training the models on a dataset that labeled all hand joints as a single class yielded better performance than training them on a dataset that labeled hand joints as finger and wrist joint classes.
- DL was used to propose an efficient mTSS-based classification model, explaining the plausibility of using Grad-CAM to validate the AI results in the joint area, which can assist physicians to screen RA severities in a very short time.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Almutairi, K.; Nossent, J.; Preen, D.; Keen, H.; Inderjeeth, C. The global prevalence of rheumatoid arthritis: A meta-analysis based on a systematic review. Rheumatol. Int. 2021, 41, 863–877. [Google Scholar] [CrossRef] [PubMed]
- Taylor, P.C.; Keystone, E.C.; van der Heijde, D.; Weinblatt, M.E.; Del Carmen Morales, L.; Reyes Gonzaga, J.; Yakushin, S.; Ishii, T.; Emoto, K.; Beattie, S.; et al. Baricitinib versus Placebo or Adalimumab in Rheumatoid Arthritis. N. Engl. J. Med. 2017, 376, 652–662. [Google Scholar] [CrossRef] [PubMed]
- Lin, J.-Z.; Liang, J.-J.; Ma, J.-D.; Li, Q.-H.; Mo, Y.-Q.; Cheng, W.-M.; He, X.-L.; Li, N.; Cao, M.-H.; Xu, D.; et al. Myopenia is associated with joint damage in rheumatoid arthritis: A cross-sectional study. J. Cachexia Sarcopenia Muscle 2019, 10, 355–367. [Google Scholar] [CrossRef] [PubMed]
- Ruyssen-Witrand, A.; Guernec, G.; Nigon, D.; Tobon, G.; Jamard, B.; Rat, A.-C.; Vittecoq, O.; Cantagrel, A.; Constantin, A. Aiming for SDAI remission versus low disease activity at 1 year after inclusion in ESPOIR cohort is associated with better 3-year structural outcomes. Ann. Rheum. Dis. 2015, 74, 1676–1683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemalatha, R.J.; Vijaybaskar, V.; Thamizhvani, T.R. Automatic localization of anatomical regions in medical ultrasound images of rheumatoid arthritis using deep learning. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2019, 233, 657–667. [Google Scholar] [CrossRef] [PubMed]
- Norgeot, B.; Glicksberg, B.S.; Trupin, L.; Lituiev, D.; Gianfrancesco, M.; Oskotsky, B.; Schmajuk, G.; Yazdany, J.; Butte, A.J. Assessment of a Deep Learning Model Based on Electronic Health Record Data to Forecast Clinical Outcomes in Patients with Rheumatoid Arthritis. JAMA Netw. Open 2019, 2, e190606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dang, S.D.H.; Allison, L. Using Deep Learning to Assign Rheumatoid Arthritis Scores. In Proceedings of the 2020 IEEE 21st International Conference on Information Reuse and Integration for Data Science (IRI), Las Vegas, NV, USA, 11–13 August 2020; pp. 399–402. [Google Scholar]
- Rohrbach, J.; Reinhard, T.; Sick, B.; Dürr, O. Bone erosion scoring for rheumatoid arthritis with deep convolutional neural networks. Comput. Electr. Eng. 2019, 78, 472–481. [Google Scholar] [CrossRef]
- Üreten, K.; Erbay, H.; Maraş, H.H. Detection of rheumatoid arthritis from hand radiographs using a convolutional neural network. Clin. Rheumatol. 2020, 39, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Murakami, S.; Hatano, K.; Tan, J.; Kim, H.; Aoki, T. Automatic identification of bone erosions in rheumatoid arthritis from hand radiographs based on deep convolutional neural network. Multimed. Tools Appl. 2018, 77, 10921–10937. [Google Scholar] [CrossRef]
- Hirano, T.; Nishide, M.; Nonaka, N.; Seita, J.; Ebina, K.; Sakurada, K.; Kumanogoh, A. Development and validation of a deep-learning model for scoring of radiographic finger joint destruction in rheumatoid arthritis. Rheumatol. Adv. Pract. 2019, 3, rkz047. [Google Scholar] [CrossRef] [PubMed]
- Girshick, R.; Donahue, J.; Darrell, T.; Malik, J. Rich feature hierarchies for accurate object detection and semantic segmentation. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Columbus, OH, USA, 23–28 June 2014; pp. 580–587. [Google Scholar]
- Girshick, R. Fast r-cnn. In Proceedings of the IEEE International Conference on Computer Vision, Santiago, Chile, 7–13 December 2015; pp. 1440–1448. [Google Scholar]
- Ren, S.; He, K.; Girshick, R.; Sun, J. Faster R-CNN: Towards real-time object detection with region proposal networks. IEEE Trans. Pattern Anal. Mach. Intell. 2016, 39, 1137–1149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bochkovskiy, A.; Wang, C.-Y.; Liao, H.-Y.M. Yolov4: Optimal speed and accuracy of object detection. arXiv 2020, arXiv:2004.10934. [Google Scholar]
- Redmon, J.; Farhadi, A. Yolov3: An incremental improvement. arXiv 2018, arXiv:1804.02767. [Google Scholar]
- Redmon, J.; Divvala, S.; Girshick, R.; Farhadi, A. You only look once: Unified, real-time object detection. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Las Vegas, NV, USA, 27–30 June 2016; pp. 779–788. [Google Scholar]
- Redmon, J.; Farhadi, A. YOLO9000: Better, faster, stronger. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Honolulu, Hi, USA, 21–26 July 2017; pp. 7263–7271. [Google Scholar]
- Hioki, Y.; Makino, K.; Koyama, K.; Haro, H.; Terada, H. Evaluation Method of Rheumatoid Arthritis by the X-ray Photograph using Deep Learning. In Proceedings of the 2021 IEEE 3rd Global Conference on Life Sciences and Technologies (LifeTech), Nara, Japan, 9–11 March 2021; pp. 444–447. [Google Scholar]
- Fan, F.-L.; Xiong, J.; Li, M.; Wang, G. On interpretability of artificial neural networks: A survey. IEEE Trans. Radiat. Plasma Med. Sci. 2021, 5, 741–760. [Google Scholar] [CrossRef] [PubMed]
- Avramidis, G.P.; Avramidou, M.P.; Papakostas, G.A. Rheumatoid arthritis diagnosis: Deep learning vs. humane. Appl. Sci. 2021, 12, 10. [Google Scholar] [CrossRef]
- D.I.a.C.i.M. (DICOM). Supplement 142: Clinical Trial De-Identification Profiles, DICOM Standards Committee, Working Group 18 Clinical Trials, 1300 N. 17th Street, Suite 1752, Rosslyn, VA, USA, 2011. Available online: https://www.dicomstandard.org/News-dir/ftsup/docs/sups/sup142.pdf (accessed on 7 June 2022).
- OFFIS; DCMTK. DICOM Toolkit. 2022. Available online: https://dicom.offis.de/dcmtk.php.en (accessed on 7 June 2022).
- Zheng, Z.; Wang, P.; Liu, W.; Li, J.; Ye, R.; Ren, D. Distance-IoU loss: Faster and better learning for bounding box regression. In Proceedings of the AAAI Conference on Artificial Intelligence, New York, NY, USA, 7–12 February 2020; pp. 12993–13000. [Google Scholar]
- Tan, M.; Le, Q. Efficientnet: Rethinking model scaling for convolutional neural networks. In Proceedings of the International Conference on Machine Learning, PMLR, Long Beach, CA, USA, 9–15 June 2019; pp. 6105–6114. [Google Scholar]
- Selvaraju, R.R.; Cogswell, M.; Das, A.; Vedantam, R.; Parikh, D.; Batra, D. Grad-cam: Visual explanations from deep networks via gradient-based localization. In Proceedings of the IEEE International Conference on Computer Vision, Venice, Italy, 22–29 October 2017; pp. 618–626. [Google Scholar]
- Murdaca, G.; Caprioli, S.; Tonacci, A.; Billeci, L.; Greco, M.; Negrini, S.; Cittadini, G.; Zentilin, P.; Spagnolo, E.V.; Gangemi, S. A Machine Learning Application to Predict Early Lung Involvement in Scleroderma: A Feasibility Evaluation. Diagnostics 2021, 11, 1880. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Training as 1 Class | 2 Classes | Simplification | Full Name |
|---|---|---|---|
| ROIs | Finger | PIP | Proximal interphalangeal joint |
| MCP | Metacarpophalangeal joint | ||
| Wrist | CMC | Carpometacarpal joint | |
| TPM | Trapezium | ||
| SCP | Scaphoid | ||
| LUN | Lunate | ||
| RAD | Radius | ||
| UNA | Ulnar | ||
| SC | Scaphoid–capitate joint | ||
| SR | Scaphoid–radius joint | ||
| ST | Scaphoid–trapezium joint |
| Parameters | Value | Parameters | Value |
|---|---|---|---|
| Batch | 64 | Decay | 0.0005 |
| Subdivisions | 32 | Learning rate | 0.001 |
| Width * | 416 | Max batches | 6000 |
| Height * | 416 | Policy | 4800, 5400 |
| Momentum | 0.949 | Scales | 0.1, 0.1 |
| YOLO4 | YOLOv3 | YOLOv4-tiny-3l | YOLOv4-tiny | Faster-RCNN | EfficientDet-D0 | |
|---|---|---|---|---|---|---|
| Dataset I | 0.71 | 0.66 | 0.65 | 0.61 | 0.65 | 0.63 |
| Dataset II | 0.63 | 0.58 | 0.61 | 0.55 | 0.59 | 0.58 |
| Model | Resolution | JSN [email protected] |
|---|---|---|
| YOLOv4 | 256 × 256 | 0.68 |
| 320 × 320 | 0.68 | |
| 416 × 416 | 0.70 | |
| 608 × 608 | 0.71 |
| Evaluation | JSN | ||||
|---|---|---|---|---|---|
| YOLO v4 Model | Original | With WL | With WL + Mosaic | With WL+ IoU and NMS | Proposed Method |
| [email protected] | 0.71 | 0.75 | 0.78 | 0.8 | 0.92 |
| Precision | 0.67 | 0.72 | 0.76 | 0.77 | 0.95 |
| Recall | 0.86 | 0.88 | 0.91 | 0.92 | 0.94 |
| F1-Score | 0.75 | 0.79 | 0.83 | 0.84 | 0.94 |
| Evaluation | Precision | Recall | F1-Score | Support |
|---|---|---|---|---|
| Healthy | 0.91 | 0.98 | 0.94 | 166 |
| Mild | 0.79 | 0.72 | 0.75 | 103 |
| Severe | 0.9 | 0.89 | 0.89 | 276 |
| Accuracy | - | - | 0.88 | 545 |
| Macro avg | 0.87 | 0.86 | 0.86 | 545 |
| Weighted avg | 0.88 | 0.88 | 0.88 | 545 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, H.-J.; Su, C.-P.; Lai, C.-C.; Chen, W.-R.; Chen, C.; Ho, L.-Y.; Chu, W.-C.; Lien, C.-Y. Deep Learning-Based Computer-Aided Diagnosis of Rheumatoid Arthritis with Hand X-ray Images Conforming to Modified Total Sharp/van der Heijde Score. Biomedicines 2022, 10, 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061355
Wang H-J, Su C-P, Lai C-C, Chen W-R, Chen C, Ho L-Y, Chu W-C, Lien C-Y. Deep Learning-Based Computer-Aided Diagnosis of Rheumatoid Arthritis with Hand X-ray Images Conforming to Modified Total Sharp/van der Heijde Score. Biomedicines. 2022; 10(6):1355. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061355
Chicago/Turabian StyleWang, Hao-Jan, Chi-Ping Su, Chien-Chih Lai, Wun-Rong Chen, Chi Chen, Liang-Ying Ho, Woei-Chyn Chu, and Chung-Yueh Lien. 2022. "Deep Learning-Based Computer-Aided Diagnosis of Rheumatoid Arthritis with Hand X-ray Images Conforming to Modified Total Sharp/van der Heijde Score" Biomedicines 10, no. 6: 1355. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines10061355