
Enzyme-Linked Immunosorbent Spot Assay for the Detection of Wilms’ Tumor 1-Specific T Cells Induced by Dendritic Cell Vaccination

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patient Population
2.3. Isolation of Peripheral Blood Mononuclear Cells (PBMCs)
2.4. Interferon (IFN)-γ ELISpot Assay
2.5. Tetramer Analysis
2.6. Statistical Analyses
3. Results
3.1. Reproducibility of the ELISpot Assay

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| (a) Assay Reproducibility | |||
|---|---|---|---|
| Sample | A | B | C |
| Mean | 73.5 | 15.0 | 22.2 |
| Median | 73.0 | 14.0 | 24.0 |
| SD | 5.4 | 3.1 | 3.6 |
| CV (%) | 7.4 | 11.8 | 16.3 |
| (b) Daily Precision | |||
| Sample | A | B | C |
| Mean | 77.4 | 24.6 | 20.1 |
| Median | 77.5 | 24.3 | 20.5 |
| SD | 3.9 | 4.3 | 3.1 |
| CV (%) | 5.0 | 17.3 | 15.7 |
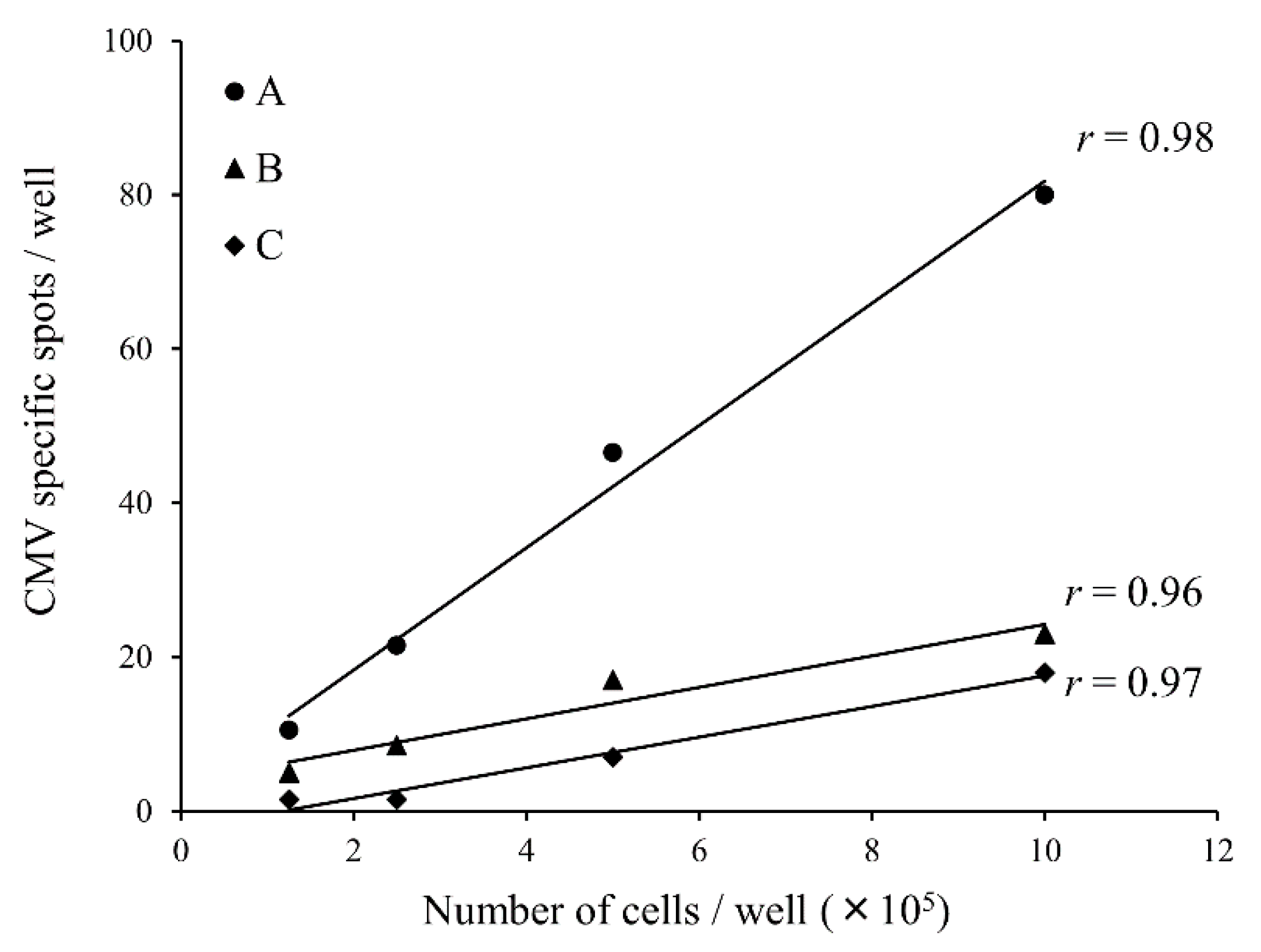
3.2. Dilution Linearity

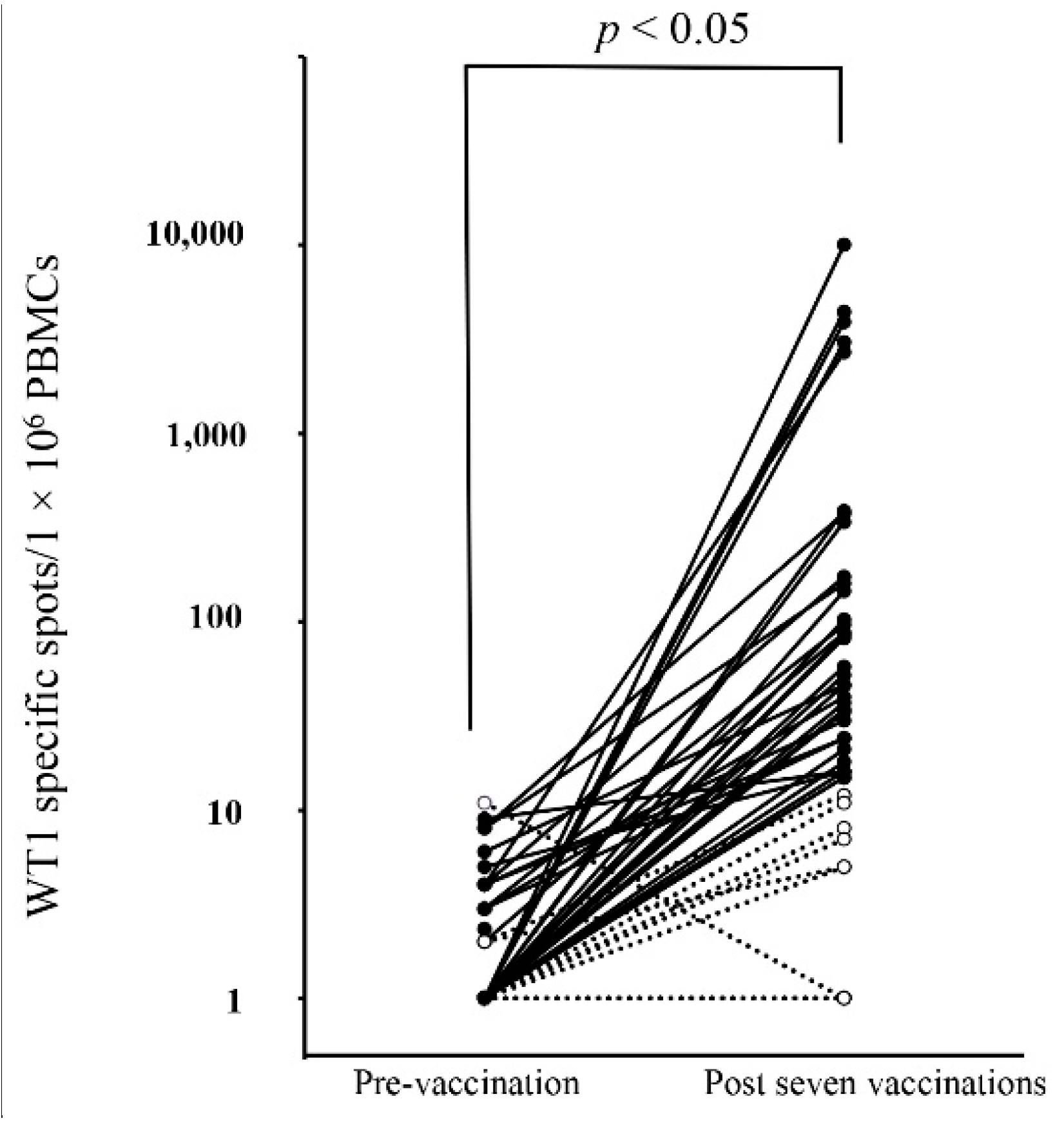
3.3. Detection of WT1-Specific Immune Response by ELISpot Assay


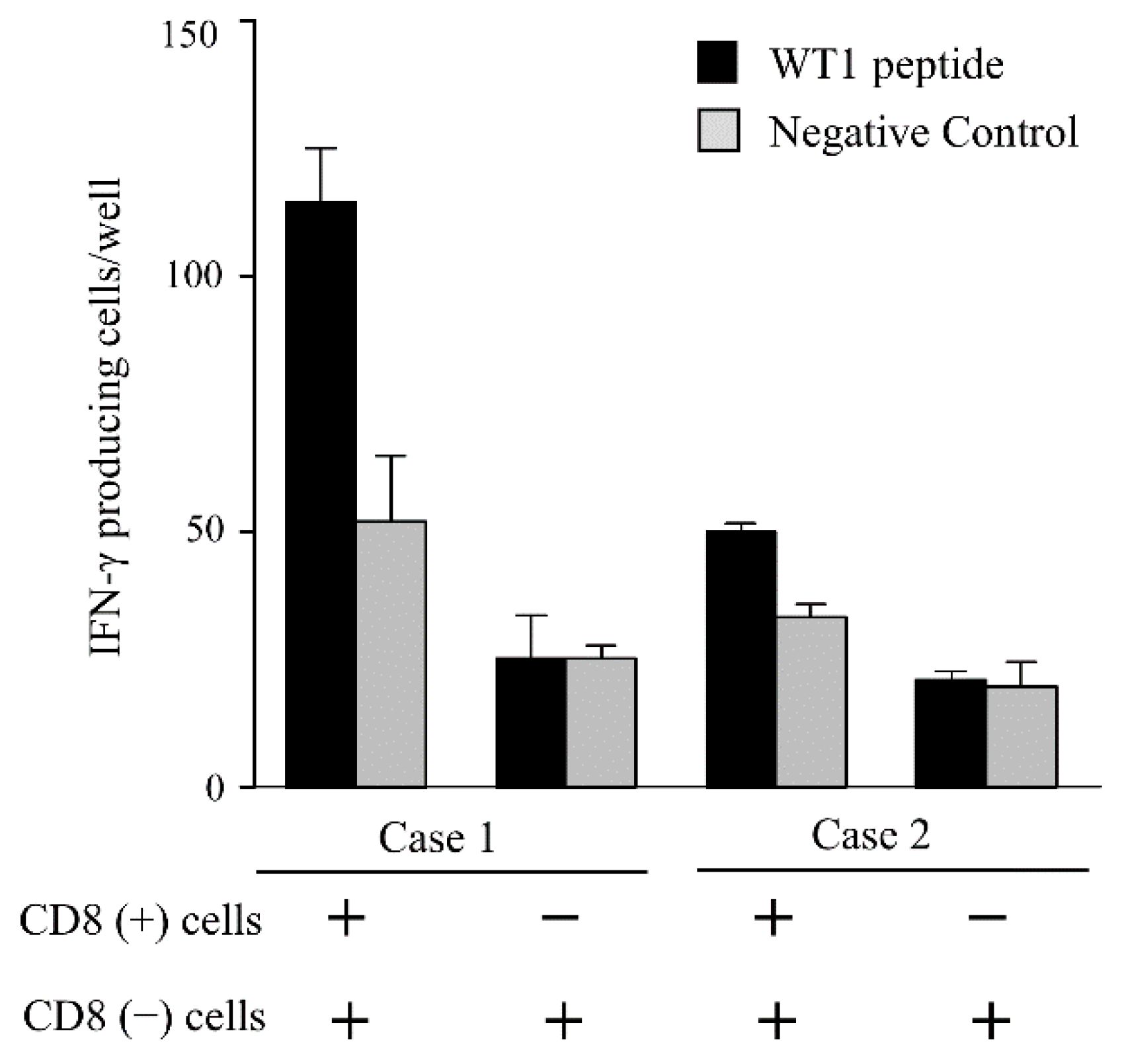
3.4. IFN-γ Producing Cells in the PBMCs

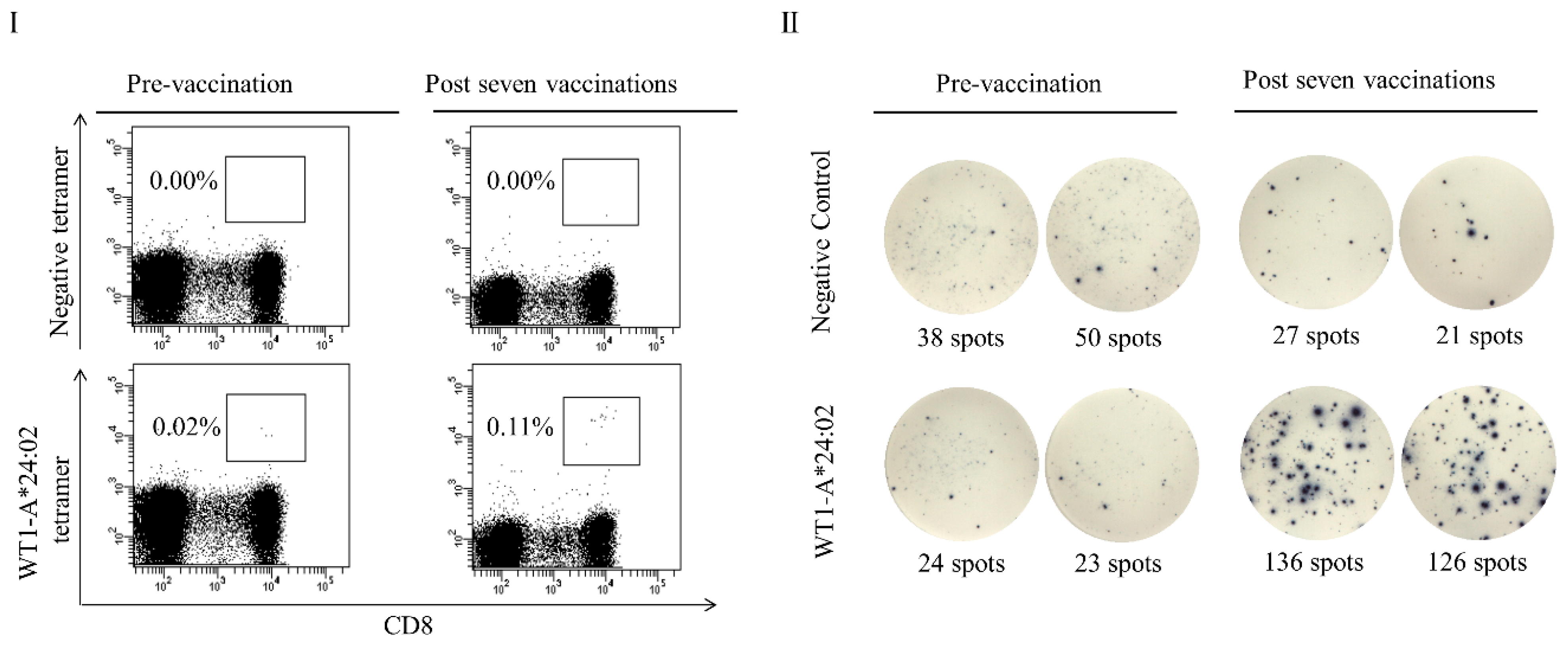
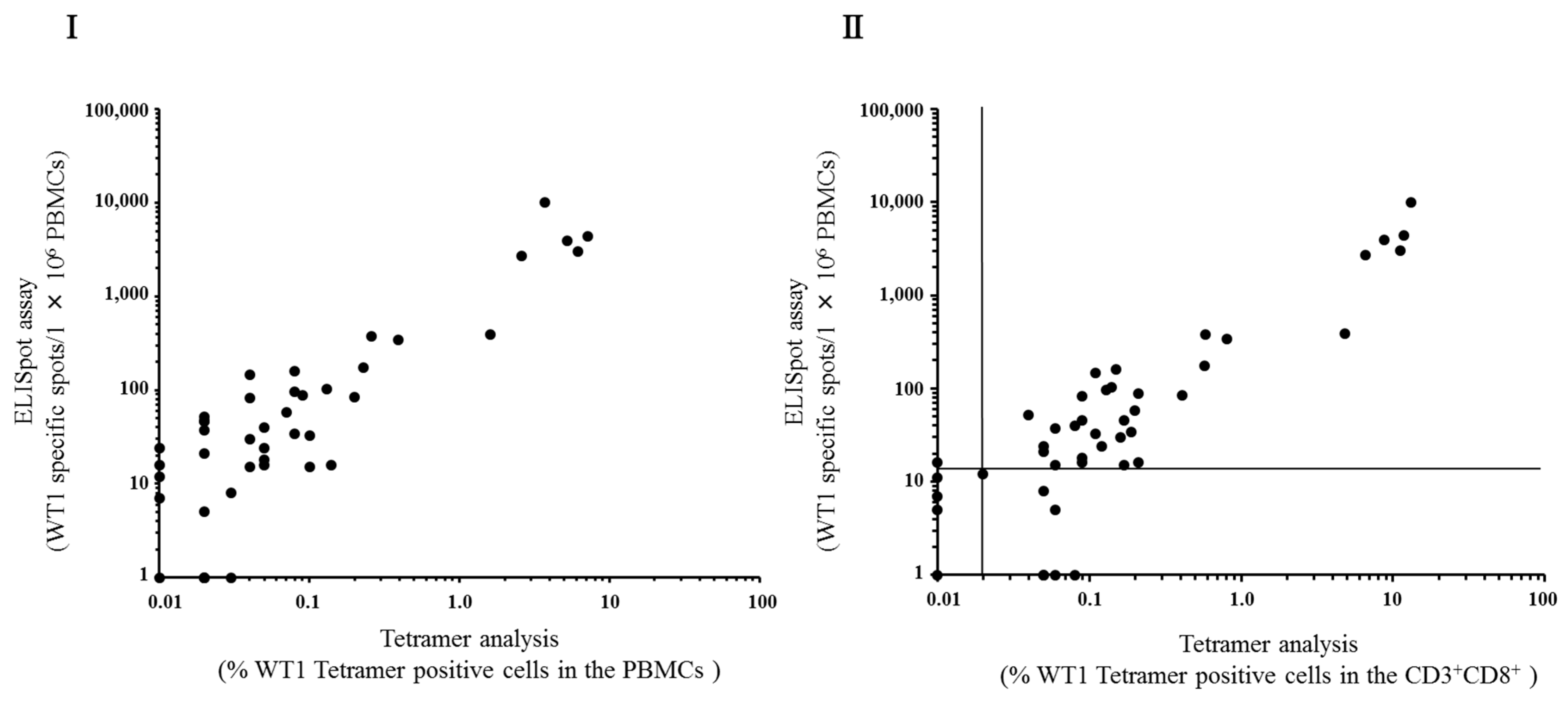
3.5. Correlation between ELISpot Assay and Tetramer Analysis

| - | ELISpot | |||
|---|---|---|---|---|
| + | − | Total | ||
| Tetramer | + | 33 | 7 | 40 |
| − | 1 | 5 | 6 | |
| Total | 34 | 12 | 46 | |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Steinman, R.M. The dendritic Cell and its role in immunogenicity. Annu. Rev. Immunol. 1991, 9, 271–296. [Google Scholar] [CrossRef] [PubMed]
- Saito, S.; Yanagisawa, R.; Yoshikawa, K.; Higuchi, Y.; Koya, T.; Yoshizawa, K.; Tanaka, M.; Sakashita, K.; Kobayashi, T.; Kurata, T.; et al. Safety and tolerability of allogeneic dendritic cell vaccination with induction of WT1-specific T cells in a pediatric donor and pediatric patient with relapsed leukemia: A case report and review of the literature. Cytotherapy 2015, 17, 330–335. [Google Scholar] [CrossRef] [PubMed]
- Oka, Y.; Tsuboi, A.; Taguchi, T.; Osaki, T.; Kyo, T.; Nakajima, H.; Elisseeva, O.A.; Oji, Y.; Kawakami, M.; Ikegame, K.; et al. Induction of WT1 (Wilms’ tumor gene)-specific cytotoxic T lymphocytes by WT1 peptide vaccine and the resultant cancer regression. Proc. Natl. Acad. Sci. USA 2004, 21, 13885–13890. [Google Scholar] [CrossRef] [PubMed]
- Koido, S.; Homma, S.; Okamoto, M.; Takakura, K.; Mori, M.; Yoshizaki, S.; Tsukinaga, S.; Odahara, S.; Koyama, S.; Imazu, H.; et al. Treatment with chemotherapy and dendritic cells pulsed with multiple Wilms’ tumor 1 (WT1)-specific MHC class I/II-restricted epitopes for pancreatic cancer. Clin. Cancer Res. 2014, 20, 4228–4239. [Google Scholar] [CrossRef] [PubMed]
- Higuchi, Y.; Koya, T.; Yuzawa, M.; Yamaoka, N.; Mizuno, Y.; Yoshizawa, K.; Takahashi, K.; Soneda, M.; Horiuchi, K.; Hirabayashi, K.; et al. Detection of specific immune response by dendritic cell-based cancer immunotherapy. J. Jpn. Soc. Transfus. Med. Cell Ther. 2015, 61, 401–402. [Google Scholar] [CrossRef]
- Nakatsuka, S.; Oji, Y.; Horiuchi, T.; Kanda, T.; Kitagawa, M.; Takeuchi, T.; Kawano, K.; Kuwae, Y.; Yamauchi, A.; Okumura, M.; et al. Immunohistochemical detection of WT1 protein in a variety of cancer cells. Mod. Pathol. 2006, 19, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Cheever, M.A.; Allison, J.P.; Ferris, A.S.; Finn, O.J.; Hastings, B.M.; Hecht, T.T.; Mellman, I.; Prindiville, S.A.; Viner, J.L.; Weiner, L.M.; et al. The Prioritization of Cancer Antigens: A National Cancer Institute Pilot Project for the Acceleration of Translational Research. Clin. Cancer Res. 2009, 15, 5323–5337. [Google Scholar] [CrossRef] [PubMed]
- Clay, T.M.; Hobeika, A.C.; Mosca, P.J.; Lyerly, H.K.; Morse, M.A. Assays for Monitoring Cellular Immune Responses to Active Immunotherapy of Cancer. Clin. Cancer Res. 2001, 7, 1127–1135. [Google Scholar] [PubMed]
- Xu, Y.; Theobald, V.; Sung, C.; DePalma, K.; Atwater, L.; Seiger, K.; Perricone, M.A.; Richards, S.M. Validation of a HLA-A2 tetramer flow cytometric method, IFNγ real time RT-PCR, and IFNγ ELISPOT for detection of immunologic response to gp100 and MelanA/MART-1 in melanoma patients. J. Transl. Med. 2008, 6, 61. [Google Scholar] [CrossRef] [PubMed]
- Keilholz, U.; Weber, J.; Finke, J.H.; Gabrilovich, D.I.; Kast, W.M.; Disis, ML.; Kirkwood, J.M.; Scheibenbogen, C.; Schlom, J.; Maino, V.C.; et al. Immunologic monitoring of cancer vaccine therapy: results of a workshop sponsored by the Society for Biological Therapy. J. Immunother. 2002, 25, 97–138. [Google Scholar] [CrossRef] [PubMed]
- Godard, B.; Gazagne, A.; Gey, A.; Baptiste, M.; Vingert, B.; Pegaz-Fiornet, B.; Strompf, L.; Fridman, W.H.; Glotz, D.; Tartour, E. Optimization of an elispot assay to detect cytomegalovirus-specific CD8+ T lymphocytes. Hum. Immunol. 2004, 65, 1307–1318. [Google Scholar] [CrossRef] [PubMed]
- Scheibebogen, C.; Letsch, A.; Thiel, E.; Schmittel, A.; Mailaender, V.; Baerwolf, S.; Nagorsen, D.; Keilholz, U. CD8 T-cell responses to Wilms tumor gene product WT1 and proteinase 3 in patients with acute myeloid leukemia. Blood 2002, 100, 2132–2137. [Google Scholar] [CrossRef] [PubMed]
- Abu-Khader, A.; Krause, S. Rapid monitoring of immune reconstitution after allogeneic stem cell transplantation—a comparison of different assays for the detection of cytomegalovirus-specific T cells. Eur. J. Haematol. 2013, 91, 534–545. [Google Scholar] [CrossRef] [PubMed]
- Chudley, L.; McCann, K.J.; Coleman, A.; Cazaly, A.M.; Bidmon, N.; Britten, C.M.; van der Burg, S.H.; Gouttefangeas, C.; Jandus, C.; Laske, K.; et al. Harmonisation of short-term in vitro culture for the expansion of antigen-specific CD8+ T cells with detection by ELISPOT and HLA-multimer staining. Cancer Immunol. Immunother. 2014, 63, 1199–1211. [Google Scholar] [CrossRef] [PubMed]
- Britten, C.M.; Gouttefangeas, C.; Welters, M.J.; Pawelec, G.; Koch, S.; Ottensmeier, C.; Mander, A.; Walter, S.; Paschen, A.; Müller-Berghaus, J.; et al. The CIMT-monitoring panel: a two-step approach to harmonize the enumeration of antigen-specific CD8+ T lymphocytes by structural and functional assays. Cancer Immunol. Immunother. 2008, 57, 289–302. [Google Scholar] [CrossRef] [PubMed]
- Britten, C.M.; Janetzki, S.; Ben-Porat, L.; Clay, T.M.; Kalos, M.; Maecker, H.; Odunsi, K.; Pride, M.; Old, L.; Hoos, A.; et al. Harmonization guidelines for HLA-peptide multimer assays derived from results of a large scale international proficiency panel of the Cancer Vaccine Consortium. Cancer Immunol. Immunother. 2009, 58, 1701–1713. [Google Scholar] [CrossRef] [PubMed]
- Lehmann, P.V.; Zhang, W. Unique strengths of ELISPOT for T cell diagnostics. In Handbook of ELISPOT: Methods and protocols, Methods in molecular biology, 2nd ed.; Kalyuzhny, A.E., Ed.; Humana Press: New York City, NY, USA, 2012; Volume 792, pp. 3–23. [Google Scholar]
- Miyahara, Y.; Murata, K.; Rodriguez, D.; Rodriguez, JR.; Esteban, M.; Rodrigues, M.M.; Zavala, F. Quantification of antigen specific CD8+ T cells using an ELISPOT assay. J. Immunol. Methods 1995, 181, 45–54. [Google Scholar] [CrossRef]
- Karlsson, A.C.; Martin, J.N.; Younger, S.R.; Bredt, B.M.; Epling, L.; Ronquillo, R.; Varma, A.; Deeks, S.G.; McCune, J.M.; Nixon, D.F.; et al. Comparison of the ELISPOT and cytokine flow cytometry assays for the enumeration of antigen-specific T cells. J. Immunol. Methods 2003, 283, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Shibamoto, Y.; Okamoto, M.; Kobayashi, M.; Ayakawa, S.; Iwata, H.; Sugie, C.; Mitsuishi, Y.; Takahashi, H. Immune-maximizing (IMAX) therapy for cancer: Combination of dendritic cell vaccine and intensity-modulated radiation. Mol. Clin. Oncol. 2013, 1, 649–654. [Google Scholar] [CrossRef] [PubMed]
- Shimodaira, S.; Kobayashi, T.; Hirabayashi, K.; Horiuchi, K.; Koya, T.; Mizuno, Y.; Yamaoka, N.; Yuzawa, M.; Ishikawa, S.; Higuchi, Y.; et al. Induction of Antigen-Specific Cytotoxic T Lymphocytes by Chemoradiotherapy in Patients Receiving Wilms Tumor 1-Targetted Dendritic Cell Vaccinations for Pancreatic Cancer. OMICS J. Radiol. 2015, 4. [Google Scholar] [CrossRef]
- Johung, K.; Saif, M.W.; Chang, B.W. Treatment of locally advanced pancreatic cancer: The role of radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 508–518. [Google Scholar] [CrossRef] [PubMed]
- Mayanagi, S.; Kitago, M.; Sakurai, T.; Matsuda, T.; Fujita, T.; Higuchi, H.; Taguchi, J.; Takeuchi, H.; Itano, O.; Aiura, K.; et al. Phase I pilot study of Wilms tumor gene 1 peptide-pulsed dendritic cell vaccination combined with gemcitabine in pancreatic cancer. Cancer Sci. 2015, 106, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Shimodaira, S.; Maejima, S.; Udagawa, N.; Sano, K.; Higuchi, Y.; Koya, T.; Ochiai, T.; Koide, M.; Uehara, S.; et al. Dendritic cell-based immunotherapy targeting Wilms’ Tumor 1 (WT1) in patients with relapsed malignant glioma. J. Neurosurg. 2015, 7, 1–9. [Google Scholar]
- Couzin-Frankel, J. Breakthrough of the year 2013, Cancer immunotherapy. Science 2013, 342, 1432–1433. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Higuchi, Y.; Koya, T.; Yuzawa, M.; Yamaoka, N.; Mizuno, Y.; Yoshizawa, K.; Hirabayashi, K.; Kobayashi, T.; Sano, K.; Shimodaira, S. Enzyme-Linked Immunosorbent Spot Assay for the Detection of Wilms’ Tumor 1-Specific T Cells Induced by Dendritic Cell Vaccination. Biomedicines 2015, 3, 304-315. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines3040304
Higuchi Y, Koya T, Yuzawa M, Yamaoka N, Mizuno Y, Yoshizawa K, Hirabayashi K, Kobayashi T, Sano K, Shimodaira S. Enzyme-Linked Immunosorbent Spot Assay for the Detection of Wilms’ Tumor 1-Specific T Cells Induced by Dendritic Cell Vaccination. Biomedicines. 2015; 3(4):304-315. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines3040304
Chicago/Turabian StyleHiguchi, Yumiko, Terutsugu Koya, Miki Yuzawa, Naoko Yamaoka, Yumiko Mizuno, Kiyoshi Yoshizawa, Koichi Hirabayashi, Takashi Kobayashi, Kenji Sano, and Shigetaka Shimodaira. 2015. "Enzyme-Linked Immunosorbent Spot Assay for the Detection of Wilms’ Tumor 1-Specific T Cells Induced by Dendritic Cell Vaccination" Biomedicines 3, no. 4: 304-315. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines3040304