Primary Membranous Glomerulonephritis: The Role of Serum and Urine Biomarkers in Patient Management



Abstract
:1. Introduction
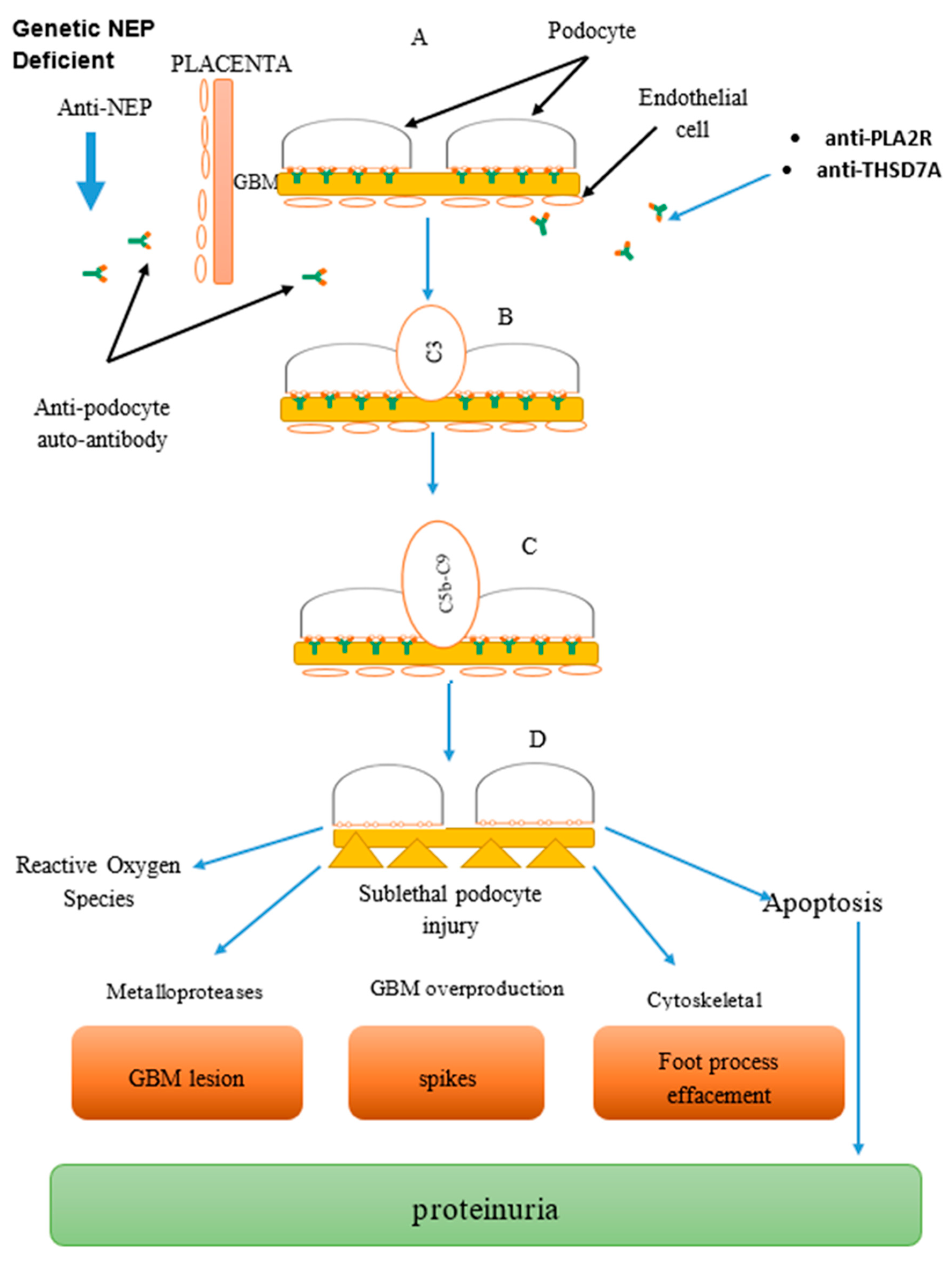
2. Pathogenesis
3. Materials and Methods
3.1. The Biomarkers
3.1.1. Clinical Feature
3.1.2. PLA2R-Related Sarcoidosis and Hepatitis B Virus (HBV) Infection
3.1.3. THSD7A and Malignancy
3.1.4. Role of Biomarkers in Kidney Transplant
3.2. Detection of Biomarkers
3.2.1. Western Blot Technique
3.2.2. Recombinant Cell-Indirect Immunoassay (RC-IFA)
3.2.3. Time-Resolved Fluoroimmunoassay (TRFIA)
3.2.4. Laser Bead Immunoassay (ALBIA)
3.2.5. Luciferase Immunoprecipitation System (LIPS)
3.2.6. Enzyme-Linked Immunosorbent Assay (ELISA)
3.2.7. Detection of Anti-PLA2R and Anti-THSD7A in Serum
3.2.8. Detection of Anti-PLA2R and Anti-THSD7A in Urine
3.3. Diagnosis
3.4. Treatment of Idiopathic MGN and Further Therapy
3.5. Prognosis
4. Conclusions
Funding
Conflicts of Interest
References
- Larsen, C.P.; Messias, N.C.; Silva, F.G.; Messias, E.; Walker, P.D. Determination of primary versus secondary membranous glomerulopathy utilizing phospholipase A2 receptor staining in renal biopsies. Modern Pathol. 2012, 26, 709–715. [Google Scholar] [CrossRef] [Green Version]
- Fogo, A.B.; Lusco, M.A.; Najafian, B. AJKD atlas of renal pathology: Membranous nephropathy. Nephrol. Dial. Transplant. 2011, 26, 3425–3426. [Google Scholar] [CrossRef]
- Salant, D.J. Membranous nephropathy. Port. J. Nephrol. Hypert. 2015, 33, 239–251. [Google Scholar]
- Cattran, D.C.; Brenchley, P.E. Membranous nephropathy: Integrating basic science into improved clinical management. Kidney Int. 2017, 566–574. [Google Scholar] [CrossRef]
- Cattran, D.; Brenchley, P. Membranous nephropathy: Thinking through the therapeutic options. Nephrol. Dial. Transpl. 2017, 32, i22–i29. [Google Scholar] [CrossRef]
- Seitz-Polski, B.; Dolla, G.; Payre, C.; Girard, C.A.; Polidori, J.; Zorzi, K.; Birgy-Barelli, E.; Jullien, P.; Courivaud, C.; Krummel, T.; et al. Epitope Spreading of Autoantibody Response to PLA2R Associates with Poor Prognosis in Membranous Nephropathy. J. Am. Soc. Nephrol. 2016, 27, 1517–1533. [Google Scholar] [CrossRef]
- Feng, Z.; Wang, S.; Huang, Y.; Liang, X.; Shi, W.; Zhang, B. A follow-up analysis of positron emission tomography/computed tomography in detecting hidden malignancies at the time of diagnosis of membranous nephropathy. Oncotarget 2016, 7, 9645. [Google Scholar] [CrossRef]
- Zeng, C.H.; Chen, H.M.; Wang, R.S.; Chen, Y.; Zhang, S.H.; Liu, L.; Li, L.S.; Liu, Z.H. Etiology and Clinical Characteristics of Membranous Nephropathy in Chinese Patients. Am. J. Kidney Dis. 2008, 52, 691–698. [Google Scholar] [CrossRef]
- Lefaucheur, C.; Stengel, B.; Nochy, D.; Martel, P.; Hill, G.S.; Jacquot, C.; Rossert, J. Membranous nephropathy and cancer: Epidemiologic evidence and determinants of high-risk cancer association. Kidney Int. 2006, 70, 1510–1517. [Google Scholar] [CrossRef] [Green Version]
- KDIGO Clinical Practice Guideline for Glomerulonephritis. Available online: https://www.theisn.org/education-home/gop-articles/item/594-kdigogn (accessed on 28 March 2014).
- Mastroianni-Kirsztajn, G.; Hornig, N.; Schlumberger, W. Autoantibodies in renal diseases-clinical significance and recent developments in serological detection. Front. Immunol. 2015, 6, 1–6. [Google Scholar] [CrossRef]
- Ling, W.; Hao, T.; Chen, P.M.; Chan, C.K.; Chiang, W.C.; Chen, Y.M.; Wu, K.D. Science Direct Membranous nephropathy: A review on the pathogenesis, diagnosis, and treatment. J. Formos. Med. Assoc. 2015, 114, 102–111. [Google Scholar]
- Shlomchik, M.J.; Madaio, M.P. The role of antibodies and B cells in the pathogenesis of lupus nephritis. Springer Semin. Immunopathol. 2003, 24, 363–375. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, T.; Hirshkowitz, A. The role of B cells in Lupus pathogenesis. Int. J. Biochem. Cell Biol. 2010, 42, 543–550. [Google Scholar]
- Bhimma, R.; Coovadia, H.M. Hepatitis B virus-associated nephropathy. Am. J. Nephrol. 2004, 24, 198–211. [Google Scholar] [CrossRef]
- Moon, J.Y.; Lee, S.H. Treatment of Hepatitis B Virus-Associated Membranous Nephropathy: Lamivudine Era versus Post-Lamivudine Era. Korean J. Intern. Med. 2012, 27, 394–396. [Google Scholar] [CrossRef]
- Sandri, A.M.; Elewa, U.; Poterucha, J.J.; Fervenza, F.C. Treatment of hepatitis C-mediated glomerular disease. Nephron. Clin. Pract. 2011, 119, 121–130. [Google Scholar] [CrossRef]
- Morales, J.M.; Kamar, N.; Rostaing, L. Hepatitis C and renal disease: Epidemiology, diagnosis, pathogenesis. Hepat. C Ren. Dis. Hemodial. Transplant. 2012, 176, 10–23. [Google Scholar]
- Dede, F.; Ayli, D.; Gonul, I.; Yuksel, O.; Ozturk, R.; Yildiz, A.; Yenigun, E.; Piskinpasa, S.; Turgut, D.; Koc, E.; et al. The effect of Helicobacter pylori eradication on proteinuria in patients with primary glomerulonephritis. Arch. Med. Sci. 2015, 11, 764–769. [Google Scholar] [CrossRef] [Green Version]
- Lien, Y.H. Pathogenesis, diagnosis and management of paraneoplastic glomerulonephritis. Nat. Rev. Nephrol. 2011, 7, 85–95. [Google Scholar] [CrossRef]
- Beck, L.H.; Salant, D.J. Membranous nephropathy: Recent travels and new roads ahead. Kidney Int. 2010, 77, 765–770. [Google Scholar] [CrossRef]
- Heymann, W.; Hackel, D.B.; Harwood, S.; Wilson, S.G. Production of nephrotic syndrome in rats by Freund’s adjuvants and rat kidney suspensions. Proc. Soc. Exp. Biol. Med. 1959, 100, 660–664. [Google Scholar] [CrossRef] [PubMed]
- Farquhar, M.G.; Saito, A.; Kerjaschki, D. The Heymann nephritis antigenic complex: Megalin (gp330) and RAP. J. Am. Soc. Nephrol. 1995, 6, 35–47. [Google Scholar] [CrossRef] [PubMed]
- Ronco, P.; Debiec, H. Pathophysiological advances in membranous nephropathy: Time for a shift in patient’s care. Lancet 2015, 385, 1983–1992. [Google Scholar] [CrossRef]
- Hu, P.; Xuan, Q.; Hu, B.; Lu, L.; Qin, Y.H. Anti-neutral endopeptidase natriuretic peptides, disarrangement and proteinuria onset in membranous nephropathy. Mol. Biol. Rep. 2013, 40, 2963–2967. [Google Scholar] [CrossRef]
- Debiec, H.; Nauta, J.; Coulet, F.; van der, B.M.; Guigonis, V.; Schurmans, T. Role of truncating mutations in MME gene in fetomaternal alloimmunisation and antenatal glomerulopathies. Lancet 2004, 364, 1252–1259. [Google Scholar] [CrossRef]
- Larsen, C.P.; Cossey, L.N.; Beck, L.H. THSD7A staining of membranous glomerulopathy in clinical practice reveals cases with dual autoantibody positivity. Mod. Pathol. 2016, 29, 421–426. [Google Scholar] [CrossRef] [Green Version]
- Gödel, M.; Grahammer, F.; Huber, T.B. Thrombospondin Type-1 Domain-Containing 7A in Idiopathic Membranous Nephropathy. N. Engl. J. Med. 2015, 372, 1073–1075. [Google Scholar] [Green Version]
- Hofstra, J.M.; Beck, L.H.; Beck, D.M.; Wetzels, J.F.; Salant, D.J. Anti-phospholipase a2 receptor antibodies correlatewith clinical status in idiopathic membranous nephropathy. Clin. J. Am. Soc. Nephrol. 2011, 6, 1286–1291. [Google Scholar] [CrossRef]
- Prunotto, M.; Carnevali, M.L.; Candiano, G.; Murtas, C.; Bruschi, M.; Corradini, E.; Trivelli, A.; Magnasco, A.; Petretto, A.; Santucci, L.; et al. Autoimmunity in membranous nephropathy targets aldose reductase and SOD2. J. Am. Soc. Nephrol. 2010, 21, 507–519. [Google Scholar] [CrossRef]
- Liu, L.Y.; Lin, M.; Lai, Z.; Jiang, J.; Huang, Y.; Jao, L. Motor neuron-derived Thsd7a is essential for zebrafish vascular development via the Notch-dll4 signaling pathway. J. Biomed. Sci. 2016, 23, 59. [Google Scholar] [CrossRef]
- Novel Nephrological Markers: Anti-PLA2R, anti-THSD7A and Uromodulin. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwj2gt-M88XlAhUXA4gKHR_cAcAQFjAAegQIABAC&url=https%3A%2F%2Fwww.euroimmun.com%2Ffileadmin%2Feuroimmun%2Fpdf%2Fnews%2Farticle%2FHA_1254_L_UK_B18.pdf&usg=AOvVaw32W_ClcC3eRyofbMQM4anO (accessed on June 2016).
- Kemp, W.L.; Burns, D.K.; Brown, T.G. Pathology of the Kidney and Bladder. In Pathology: The Big Picture; McGraw-Hill Medical: New York, NY, USA, 2008. [Google Scholar]
- Thompson, A.; Cattran, D.C.; Blank, M. Complete and partial remission as surrogate end points in membranous nephropathy. J. Am. Soc. Nephrol. 2015, 2930–2937. [Google Scholar] [CrossRef] [PubMed]
- Barbour, S.; Reich, H. Short-term complication of membranous nephropathy. Contrib. Nephrol. 2013, 143–151. [Google Scholar]
- Ponticelli, C.; Passerini, P. A randomized pilot trial comparing methylprednisolone plus a cytotoxic agent versus synthetic adrenocorticotropic hormone in idiopathic membranous nephropathy. Am. J. Kidney 2006, 47, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Nachman, P.H.; Jennette, J.C. Primary glomerular disease. In Brenner and Rector’s the Kidney, 9th ed.; Elsevier: London, UK, 2012; pp. 1100–1191. [Google Scholar]
- 5 rd Report of the Malaysian Registry of Renal Biopsy. Available online: https://www.google.com.hk/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=2ahUKEwiqmMae68flAhVUw4sBHfHyCFwQFjAAegQIAxAC&url=https%3A%2F%2Fwww.msn.org.my%2Fmsn%2FDoc%2FPublicDoc_PB%2FPublication%2Fmrrb_report2012%2FFULL_5th_2012.pdf&usg=AOvVaw0nKLz64bns7kA7epTCeYeO (accessed on June 2012).
- Ren, S.; Wu, C.; Zhang, Y.; Wang, A.Y.; Li, G.; Wang, L.; Hong, D. An update on clinical significance of use of THSD7A in diagnosing idiopathic membranous nephropathy: A systematic review and meta-analysis of THSD7A in IMN. Ren. Fail. 2018, 40, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Guerry, M.J.; Vanhille, P.; Ronco, P. Serum anti-PLA2R antibodies may be present before clinical manifestations of membranous nephropathy. Kidney Int. 2016, 89, 1399. [Google Scholar] [CrossRef]
- Stanescu, H.C.; Arcos-Burgos, M.; Medlar, A.; Bockenhauer, D.; Kottgen, A.; Ragomirescu, L. Risk HLA-DQA1 and PLA2R1 alleles in idiopathic membranous nephropathy. N. Engl. J. Med. 2011, 364, 616–626. [Google Scholar] [CrossRef]
- Hladunewich, M.A.; Troyanov, S.; Calafati, J. The natural history of the non-nephrotic membranous nephropathy patient. Clin. J. Am. Soc. Nephrol. 2009, 4, 1417–1422. [Google Scholar] [CrossRef]
- Stehlé, T.; Joly, D.; Vanhille, P.; Boffa, J.J.; Rémy, P.; Mesnard, L.; Hoffmann, M.; Grimbert, P.; Choukroun, G.; Vrtovsnik, F.; et al. Clinicopathological study of glomerular diseases associated with sarcoidosis: A multicenter study. Orphanet. J. Rare. Dis. 2013, 8, 65. [Google Scholar] [CrossRef]
- Stehlé, T.; Audard, V.; Ronco, P.; Debiec, H. Phospholipase A2 receptor and sarcoidosis-associated membranous nephropathy. Nephrol. Dial. Transplant. 2015, 30, 1047–1050. [Google Scholar] [CrossRef] [Green Version]
- Iannuzzi, M.C.; Rybicki, B.A. Sarcoidosis. N. Engl. J. Med. 2007, 357, 2153–2165. [Google Scholar] [CrossRef]
- Debiec, H.; Ronco, P. Immunopathogenesis of membranous nephropathy: An update. Semin. Immunopathol. 2014, 36, 381–397. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.; Li, Y.; Xue, J.; Xiong, Z.; Wang, L.; Sun, Z.; Ren, Y.; Zhu, X.; Hao, C.M. Renal Phospholipase A2 Receptor in Hepatitis B Virus-Associated Membranous Nephropathy. Am. J. Nephrol. 2015, 41, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, Y.; Nagai, Y.; Mikami, T.; Akasaka, Y.; Shibuya, K.; Urita, Y. Anti-phospholipase A2 receptor antibody positive hepatitis B virus-associated membranous nephropathy remitted with entecavir after relapse with lamivudine. J. Nephropathol. 2018, 7, 93–97. [Google Scholar] [CrossRef]
- Xu, X.; Zhu, X.; Yuan, S.; Jiang, W.; Xia, Y.; Liu, H.; Li, J.; Sun, L.; Peng, Y.; Liu, F. Role of M-Type phospholipase A2 receptor and its antibody in hepatitis B virus-Associated membranous nephropathy. J. Cent. South. Univ. Med. Sci. 2016, 41, 1064–1068. [Google Scholar]
- Tomas, N.M. Autoantibodies against thrombospondin type 1 domain–containing 7A induce membranous nephropathy. J. Clin. Investig. 2016, 126, 2519–2532. [Google Scholar] [CrossRef]
- Hoxha, E.; Wiech, T.; Stahl, P.R. A mechanism for cancer-associated membranous nephropathy. N. Engl. J. Med. 2016, 374, 1995–1996. [Google Scholar] [CrossRef]
- Hoxha, E.; Beck, L.H.; Wiech, T. An indirect immunofluorescence method facilitates detection of thrombospondin type 1 domain-containing 7A-specific antibodies in membranous nephropathy. J. Am. Soc. Nephrol. 2016, 28, 520–531. [Google Scholar] [CrossRef]
- Xian, L.; Dong, D.; Luo, J.; Zhuo, L.; Li, K.; Zhang, P.; Wang, W.; Xu, Y.; Xu, G.; Wang, L.; et al. Expression of THSD7A in neoplasm tissues and its relationship with proteinuria. BMC Nephrol. 2019, 20, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Quintana, L.F.; Miguel, B.; Miguel, S.; Perez, N.S.; Lopez-Hoyos, M.; Patricia, V.; Emillio, R.; Odette, V.; Guadalupe, E.; Fritz, D.; et al. Antiphospholipase A2 antibody predict the risk of post transplantation recurrence of membranous nephropathy. Transplantation 2015, 99, 1709–1714. [Google Scholar] [CrossRef]
- Gupta, G.; Fattah, H.; Ayalon, R.; Kidd, J.; Gehr, T.; Quintana, L.F. Pretransplant phospholipase A2 receptor autoantibody concentration is associated with clinically significant recurrence of membranous nephropathy post-kidney transplantation. Clin. Transpl. 2016, 30, 461–469. [Google Scholar] [CrossRef]
- Leon, J.; Pérez-Sáez, M.J.; Batal, I.; Beck, L.H.; Rennke, H.G.; Canaud, G.; Legendre, C.; Pascual, J.; Riella, L.V. Membranous Nephropathy Post-Transplantation. Transplantation 2019, 103, 1. [Google Scholar]
- Debiec, H.; Lefeu, F.; Kemper, M.J.; Niaudet, P.; Deschênes, G.; Remuzzi, G.; Ulinski, T.; Ronco, P. Early-childhood membranous nephropathy due to cationic bovine serum albumin. N. Engl. J. Med. 2011, 364, 2101–2110. [Google Scholar] [CrossRef] [PubMed]
- Tomas, N.M.; Beck, L.H.; Meyer-Schwesinger, C.; Seitz-Polski, B.; Ma, H.; Zahner, G.; Dolla, G.; Hoxha, E.; Helmchen, U.; Dabert-Gay, A.-S.; et al. Thrombospondin Type-1 Domain-Containing 7A in Idiopathic Membranous Nephropathy. N. Engl. J. Med. 2014, 371, 2277–2287. [Google Scholar] [CrossRef] [Green Version]
- Wai, H.; Lim, M.S.G.W. Recurrent and de novo glomerulonephritis after kidney transplantation. Core Concepts Ren. Transplant. 2019, 10, 211–231. [Google Scholar]
- Peter, D.B.; Beck Jr, L.H.; Waldman, M. Detection and Monitoring PLA2R Autoantibodies by LIPS in Membranous Nephropathy. J. Immunol. Methods 2017, 20, 48–55. [Google Scholar]
- Beck Jr, L.H.; Bonegio, R.G.; Lambeau, G.; Beck, D.M.; Powell, D.W.; Cummins, T.D.; Klein, J.B. M-type Phospholipase A2 receptor as target antigen in idiopathic membranous nephropathy. N. Engl. J. Med. 2009, 361, 11–21. [Google Scholar] [CrossRef]
- Mahmood, T.; Yang, P.C. Western blot: Technique, Theory and Trouble shooting. N. Am. J. Med. Sci. 2012, 4, 429–434. [Google Scholar]
- Qin, W.; Beck Jr, L.H.; Zeng, C.; Chen, Z.; Li, S.; Zuo, K.; Salant, D.J. Anti-phospholipase A2 receptor antibody in membranous nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1137–1143. [Google Scholar] [CrossRef]
- Dahnrich, C.; Komowski, L.; Probst, C.; Seitz-Polski, B.; Esnault, V.; Wetzels, J.F.; Hofstra, J.M.; Hoxha, E.; Stahl, R.A.; Lambeau, G.; et al. Development of standarzed ELISA for the determination of autoantibodies against human M-type phospholipase A2 receptor in primary membranous nephropathy. Clin. Chim. Acta 2013, 421, 213–218. [Google Scholar] [CrossRef]
- Hoxha, E.; Blöcker, I.M.; Probst, C. Detection of PLA2R specific autoantibodies in patients with idiopathic membranous nephropathy using PLA2R producing HEK293 cells. In Proceedings of the 7th Congress on Autoimmunity, Ljubljana, Slovenia, 5–9 May 2010. [Google Scholar]
- Hofstra, J.M.; Debiec, H.; Short, C.D. Antiphospholipase A2 receptor antibody titer and subclass in idiopathic membranous nephropathy. J. Am. Soc. Nephrol. 2012, 23, 1735–1743. [Google Scholar] [CrossRef]
- Debiec, H. Nephrotic syndrome: A new specific test for idiopathic mem- branous nephropathy. Nat. Rev. Nephrol. 2011, 7, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Wandinger, K.P.; Saschenbrecker, S.; Stoecker, W. Anti-NMDA-receptor en- cephalitis: A severe, multistage, treatable disorder presenting with psychosis. J. Neuroimmunol. 2011, 231, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Waters, P.J.; McKeon, A.; Leite, M.I. Serologic diagnosis of NMO: A multicenter comparison of aquaporin-4-IgG assays. Neurology 2012, 78, 665–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komorowski, L.; Teegen, B.; Probst, C. Autoantibodies against exocrine pancreas in Crohn’s disease are directed against two antigens: The glycoproteins CUZD1 and GP2. J. Crohns Colitis 2013, 7, 780–790. [Google Scholar] [CrossRef] [PubMed]
- Hemmilä, I.; Dakubu, S.; Mukkala, V.M.; Siitari, H.; Lövgren, T. Europium as a label in time-resolved immunofluorometric assays. Anal. Biochem. 1984, 137, 335–343. [Google Scholar] [CrossRef]
- Soini, E.; Hemmila, I. Flouroimmunoassay: Present status and key problems. Clin. Chem. 1979, 353–362. [Google Scholar]
- Zhang, Q.; Huang, B.; Liu, X.; Liu, B.; Zhang, Y.; Zhang, Z.; Hua, J.; Fan, Y.; Hu, L.; Meng, M.; et al. Ultrasensitive Quantitation of Anti-Phospholipase A2 Receptor Antibody as A Diagnostic and Prognostic Indicator of Idiopathic Membranous Nephropathy. Sci. Rep. 2017, 7, 1–7. [Google Scholar] [CrossRef]
- Behnert, A.; Fritzler, M.J.; Teng, B.; Zhang, M.; Bollig, F.; Haller, H.; Skoberne, A.; Mahler, M.; Schiffer, M. An Anti-Phospholipase A2Receptor Quantitative Immunoassay and Epitope Analysis in Membranous Nephropathy Reveals Different Antigenic Domains of the Receptor. PLoS ONE 2013, 8, e61669. [Google Scholar] [CrossRef]
- Behnert, A.; Schiffer, M.; Müller-Deile, J.; Beck, L.H.; Mahler, M.; Fritzler, M.J. Antiphospholipase A2receptor autoantibodies: A comparison of three different immunoassays for the diagnosis of idiopathic membranous nephropathy. J. Immunol. Res. 2014, 2014, 143274. [Google Scholar] [CrossRef]
- Burbelo, P.D.; Lebovitz, E.E.; Notkins, A.L. Luciferase immunoprecipitation systems for measuring antibodies in autoimmune and infectious diseases. Transl. Res. 2015, 165, 325–335. [Google Scholar] [CrossRef]
- Ayalon, R.; Beck, L.H., Jr.; Schlumberger, W. Evaluation of Anti-PLA2R1 as Measured by a Novel ELISA in Patients with Idiopathic Membranous Nephropathy a Cohort Study. Am. J. Clin. Pathol. 2014, 142, 29–34. [Google Scholar]
- Dai, H.; Zhang, H.; He, Y. Diagnostic accuracy of PLA2R autoantibodies and glomerular staining for the differentiation of idiopathic and secondary membranous nephropathy: An updated meta-analysis. Sci. Rep. 2015, 5, 8803. [Google Scholar] [CrossRef] [PubMed]
- Li, W.Y. Diagnostic test accuracy of Serum anti-PLa2R autoantibodies and Glomerular PLa2R antigen for diagnosing idiopathic membranous Nephropathy: An Updated meta-analysis. Front. Med. 2018, 5, 101. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Li, X.; Ma, C.; Wang, P.; Liu, J.; Su, H.; Zhuo, H.; Kong, X.; Xu, D.; Xu, D. Serum anti-PLA2R antibody as a diagnostic biomarker of idiopathic membranous nephropathy: The optimal cut-off value for Chinese patients. Clin. Chim. Acta 2018, 476, 9–14. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.H.; Su, P.T.; Du, X.Y.; Kuo, M.W.; Lin, C.Y.; Yang, C.C.; Chan, H.S.; Chang, S.J.; Kuo, C.; Seo, K.; et al. Thrombospondin type I domain containing 7A (THSD7A) mediates endothelial cell migration and tube formation. J. Cell. Physiol. 2010, 222, 685–694. [Google Scholar] [CrossRef]
- Sharma, S.G. Tissue staining for THSD7A in glomeruli correlates with serum antibodies in primary membranous nephropathy: A clinicopathological study. Mod. Pathol. 2018, 31, 616. [Google Scholar] [CrossRef]
- Iwakura, T.; Ohashi, N.; Kato, A. Prevalence of enhanced granular expression of thrombospondin type-1 domain-containing 7A in the glomeruli of Japanese patients with idiopathic membranous nephr-opathy. PLoS ONE 2015, 10, e0138841. [Google Scholar] [CrossRef]
- Wang, Y.; He, Y.X.; Diao, T.T.; Wei, S.Y.; Qi, W.R.; Wang, C.C.; Song, S.M.; Bi, M.; Li, C.M.; Zhang, C.X.; et al. Urine anti-PLA2R antibody is a novel biomarker of idiopathic membranous nephropathy. Oncotarget 2018, 9, 67–74. [Google Scholar] [CrossRef]
- Pourcine, F.; Dahan, K.; Mihout, F.; Cachanado, M.; Brocheriou, I.; Debiec, H.; Ronco, P. Prognostic value of PLA2R autoimmunity detected by measurement of anti-PLA2R antibodies combined with detection of PLA2R antigen in membranous nephropathy: A single-centre study over 14 years. PLoS ONE 2017, 12, e0173201. [Google Scholar] [CrossRef]
- De Vriese, A.S.; Glassock, R.J.; Nath, K.A.; Sethi, S.; Fervenza, F.C. A Proposal for a Serology-Based Approach to Membranous Nephropathy. J. Am. Soc. Nephrol. 2017, 28, 421–430. [Google Scholar] [CrossRef]
- Francis, J.M.; Beck LHJr, S.D. Membranous nephropathy: A journey from bench to bedside. Am. J. Kidney Dis. 2011, 616–626. [Google Scholar] [CrossRef] [PubMed]
- Debiec, H. Immune response against autoantigen PLA2R is not gambling: Implications for pathophysiology, prognosis and therapy. J. Am. Soc. Nephrol. 2016, 1275–1277. [Google Scholar] [CrossRef] [PubMed]
- Qu, Z.; Zhang, M.F.; Cui, Z.; Wang, J.; Wang, M.; Zhang, Y.M.; Wang, F.; Wang, X.; Meng, L.Q.; Cheng, X.Y.; et al. Antibodies against M-type phospholipase A2 receptor may predict treatment response and outcome in membranous nephropathy. Am. J. Nephrol. 2018, 48, 438–446. [Google Scholar] [CrossRef] [PubMed]
- Tampoia, M. Definition of a new cut-off for the anti-phospholipase A2 receptor (PLA2R) autoantibody immunoassay in patients affected by idiopathic membranous nephropathy. J. Nephrol. 2018, 31, 899–905. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Liu, L.; Guo, Y.; Yang, L. Clinical value of a serum anti-PLA2R antibody in the diagnosis and monitoring of primary membranous nephropathy in adults. Int. J. Nephrol. Renovasc. Dis. 2018, 11, 241–247. [Google Scholar] [CrossRef]
- Bobart, S.A.; De Vriese, A.S.; Pawar, A.S.; Zand, L.; Sethi, S.; Giesen, C.; Lieske, J.C.; Fervenza, F.C. Noninvasive diagnosis of primary membranous nephropathy using phospholipase A2 receptor antibodies. Kidney Int. 2019, 95, 429–438. [Google Scholar] [CrossRef] [Green Version]
- Jullien, P.; Polski, B.S.; Maillard, N.; Thibaudin, D.; Laurent, B.; Ollier, E.; Alamartine, E.; Lambeau, G.; Mariat, C. Anti-phospholipase A2 receptor antibody levels at diagnosis predicts spontaneous remission of idiopathic membranous nephropathy. Clin. Kidney J. 2017, 10, 209–214. [Google Scholar] [CrossRef] [Green Version]
- Debiec, H.; Ronco, P. PLA2R autoantibodies and PLA2R glomerular deposits in membranous nephropathy. N. Engl. J. Med. 2011, 364, 689–690. [Google Scholar] [CrossRef]
- Hladunewich, M.A.; Cattran, D.; Beck, L.H.; Odutayo, A.; Sethi, S.; Ayalon, R.; Leung, N.R. A pilot study to determine the dose and effectiveness of adrenocortico- trophic hormone (H.P. Acthar® Gel) in ne- phrotic syndrome due to idiopathic membra- nous nephropathy. Nephrol. Dial. Transpl. 2014, 29, 1570–1577. [Google Scholar] [CrossRef]
- Dahan, K.; Debiec, H.; Plaisier, E.; Cachanado, M.; Rousseau, A.; Wakselman, L.; Michel, P.-A.; Mihout, F.; Dussol, B.; Matignon, M.; et al. Rituximab for Severe Membranous Nephropathy: A 6-Month Trial with Extended Follow-Up. J. Am. Soc. Nephrol. 2017, 28, 348–358. [Google Scholar] [CrossRef]
- Ruggenenti, P.; Debiec, H.; Ruggiero, B.; Chianca, A.; Pelle, T.; Gaspari, F.; Suardi, F.; Gagliardini, E.; Orisio, S.; Benigni, A.; et al. Anti-Phospholipase A2 Receptor Antibody Titer Predicts Post-Rituximab Outcome of Membranous Nephropathy. J. Am. Soc. Nephrol. 2015, 26, 2545–2558. [Google Scholar] [CrossRef] [PubMed]
- Beck, L.H.; Fervenza, F.C.; Beck, D.M.; Bonegio, R.G.B.; Malik, F.A.; Erickson, S.B.; Cosio, F.G.; Cattran, D.C.; Salant, D.J. Rituximab-Induced Depletion of Anti-PLA2R Autoantibodies Predicts Response in Membranous Nephropathy. J. Am. Soc. Nephrol. 2011, 22, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Dahan, K.; Gillion, V.; Johanet, C.; Debiec, H.; Ronco, P. The Role of PLA2R Antibody in Treatment of Membranous Nephropathy. Kidney Int. Rep. 2018, 3, 498–501. [Google Scholar] [CrossRef] [PubMed]
- Stohl, W.; Hiepe, F.; Latinis, K.M. Belimumab reduces autoantibodies normalizes low complement levels, and reduces select B cell populations in patients with systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2328–2337. [Google Scholar] [CrossRef] [PubMed]
- Willcocks, L.; Barrett, C.; Brenchley, P.; Schmidt, T.; Gisbert, S.; Cai, G.; Savage, C. Effect of belimumab on proteinuria and anti-PLA2R autoantibody in idiopathic membranous ne-phropathy—6 months data. Nephrol. Dial. Transpl. 2015, 30, 32–33. [Google Scholar] [CrossRef]
- Lv, J.; Hou, W.; Zhou, X. Interaction between PLA2R1 and HLA-DQA1 variants associates with anti-PLA2R antibodies and membranous nephropathy. J. Am. Soc. Nephrol. 2013, 24, 1323–1329. [Google Scholar] [CrossRef]
- Oh, Y.J.; Yang, S.H.; Kim, D.K.; Kang, S.W. Autoantibodies against phospholipase A2 receptor in Korean patients with membranous nephropathy. PLoS ONE 2013, 8, e62151. [Google Scholar] [CrossRef]
- Bech, A.P.; Hofstra, J.M.; Brenchley, P.E. Association of anti-PLA2R antibodies with outcomes after immunosuppressive therapy in idiopathic membraneous nephropathy. Clin. J. Am. Soc. Nephrol. 2014, 9, 1386–1392. [Google Scholar] [CrossRef]
- Hoxha, E.; Thiele, I.; Zahner, G.; Panzer, U.; Harendza, S. Phospholipase A2 receptor autoantibodies and clinical outcome in patients with primary membranous nephropathy. J. Am. Soc. Nephrol. 2014, 25, 1357–1366. [Google Scholar] [CrossRef]
- Hoxha, E.; Harendza, S.; Pinnschmidt, H.; Panzer, U. PLA2R antibody level and clinical outcome in patients with membranous nephropathy and non-nephrotic range proteinuria under treatment with inhibitors of the renin-angiotensin system. PLoS ONE 2014, 9, e110681. [Google Scholar] [CrossRef]
- Van den Brand, J.A.; Hofstra, J.M.; We, J. Prognostic value of risk score and urinary markers in idiopathic membranous nephropathy. Clin. J. Am. Soc. Nephrol. 2012, 7, 1242–1248. [Google Scholar] [CrossRef] [PubMed]
- Cattran, D.C.; Kim, E.D.; Reich, H.; Hladunewich, M.; Kim, S.J. Toronto Glomerulonephritis Registry group, and for the T.G.R. Membranous Nephropathy: Quantifying Remission Duration on Outcome. J. Am. Soc. Nephrol. 2017, 28, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Domingos, M.A.M.; Moreira, S.R.; Gomez, L.; Goulart, A.; Lotufo, P.A.; Benseñor, I.; Titan, S. Urinary Retinol-Binding Protein: Relationship to Renal Function and Cardiovascular Risk Factors in Chronic Kidney Disease. PLoS ONE 2016, 11, e0162782. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Ming Wang, W.; Xia Pan, X.; Xu, J.; Ni Gao, C.; Zhang, W.; Ren, H.; Yuan Xie, J.; Yan Shen, P.; Wen Xu, Y.; et al. Biomarkers to detect membranous nephropathy in Chinese patients. Oncotarget 2016, 7, 67868. [Google Scholar] [CrossRef] [PubMed]
- Branten, A.J.; du Buf-Vereijken, P.W.; Klasen, I.S.; Bosch, F.H.; Feith, G.W.; Hollander, D.A. Urinary excretion of beta-2 microglobulin and IgG predict prognosis in idiopathic membranous nephropathy: A validation study. J. Am. Soc. Nephrol. 2005, 16, 169–174. [Google Scholar] [CrossRef] [PubMed]
- Van den Brand, J.A.; van Dijk, P.R.; Hofstra, J.M. Long-term outcomes in idiopathic membranous nephropathy using a restrictive treatment strategy. J. Am. Soc. Nephrol. 2014, 25, 150–158. [Google Scholar] [CrossRef]
- Polanco, N.; Gutiérrez, E.; Covarsí, A. Spontaneous remission of nephrotic syndrome in idiopathic membranous nephropathy. J. Am. Soc. Nephrol. 2010, 21, 697–704. [Google Scholar] [CrossRef]


{kind=link}
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Maifata, S.M.; Hod, R.; Zakaria, F.; Abd Ghani, F. Primary Membranous Glomerulonephritis: The Role of Serum and Urine Biomarkers in Patient Management. Biomedicines 2019, 7, 86. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7040086
Maifata SM, Hod R, Zakaria F, Abd Ghani F. Primary Membranous Glomerulonephritis: The Role of Serum and Urine Biomarkers in Patient Management. Biomedicines. 2019; 7(4):86. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7040086
Chicago/Turabian StyleMaifata, Sadiq Mu’azu, Rafidah Hod, Fadhlina Zakaria, and Fauzah Abd Ghani. 2019. "Primary Membranous Glomerulonephritis: The Role of Serum and Urine Biomarkers in Patient Management" Biomedicines 7, no. 4: 86. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines7040086