Drug-Induced Gingival Overgrowth: The Effect of Cyclosporin A and Mycophenolate Mophetil on Human Gingival Fibroblasts

 , , and
, , and
Abstract
:1. Introduction
1.1. Role of Cyclosporine A and Mycophenolate Mophetil on Gingival Hyperplasia
1.2. Objective
2. Experimental Section
2.1. Primary Human Fibroblast Cells Culture
2.2. Cell Viability Test
2.3. Cell Treatment and RNA Isolation
2.4. Reverse Transcription and Quantitative Real-Time RT-PCR
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Gawron, K.; Łazarz-Bartyzel, K.; Potempa, J.; Chomyszyn-Gajewska, M. Gingival fibromatosis: Clinical, molecular and therapeutic issues. Orphanet J. Rare Dis. 2016, 11, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nanda, T.; Singh, B.; Sharma, P.; Arora, K.S. Cyclosporine A and amlodipine induced gingival overgrowth in a kidney transplant recipient: Case presentation with literature review. BMJ Case Rep. 2019, 12, e229587. [Google Scholar] [CrossRef]
- Crăiţoiu, Ş.; Bobic, A.G.; Manolea, H.O.; Mehedinţi, M.C.; Pascu, R.M.; Florescu, A.M.; Petcu, I.C.; Osman, A.; Fărcaş-Berechet, C.M.; Iacov-Crăiţoiu, M.M. Immunohistochemical study of experimentally drug-induced gingival overgrowth. Rom. J. Morphol. Embryol. 2019, 60, 95–102. [Google Scholar]
- Tungare, S.; Paranjpe, A.G. Drug Induced Gingival Overgrowth (DIGO); StatPearls Publishing: Treasure Island, FL, USA, 2019. [Google Scholar]
- Lauritano, D.; Martinelli, M.; Baj, A.; Beltramini, G.; Candotto, V.; Ruggiero, F.; Palmieri, A. Drug-induced gingival hyperplasia: An in vitro study using amlodipine and human gingival fibroblasts. Int. J. Immunopathol. Pharm. 2019, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Madi, M.; Shetty, S.R.; Babu, S.; Achalli, S. Amlodipine-induced Gingival Hyperplasia—A case report and review. West Indian Med. J. 2016, 64, 279–282. [Google Scholar] [CrossRef] [Green Version]
- Jose, J.; Santhosh, Y.L.; Naveen, M.R.; Vijay, K. Case report of amlodipine induced gingival hyperplasia—Late onset at a low use. Asian J. Pharm. Clin. Res. 2011, 4, 65–66. [Google Scholar]
- Aimetti, M.; Romano, F.; Debernardi, C. Effectiveness of periodontal therapy on the severity of cyclosporin A-induced gingival overgrowth. J. Clin. Periodontol. 2005, 32, 846–850. [Google Scholar] [CrossRef]
- Hatahira, H.; Abe, J.; Hane, Y.; Matsui, T.; Sasaoka, S.; Motooka, Y.; Hasegawa, S.; Fukuda, A.; Naganuma, M.; Ohmori, T.; et al. Drug-induced gingival hyperplasia: A retrospective study using spontaneous reporting system databases. J. Pharm. Health Care Sci. 2017, 3, 1–11. [Google Scholar] [CrossRef]
- Dongari-Bagtzoglou, A. Informational paper: Drug-associated gingival enlargement. J. Periodontol. 2004, 75, 1424–1431. [Google Scholar] [CrossRef]
- Hallmon, W.W.; Rossmann, J.A. The role of drugs in the pathogenesis of gingival overgrowth. A collective review of current concepts. Periodontology 2000 1999, 21, 176–196. [Google Scholar] [CrossRef]
- Moffitt, M.L.; Bencivenni, D.; Cohen, R.E. Drug-induced gingival enlargement: An overview. Compend. Contin. Educ. Dent. 2013, 34, 330–336. [Google Scholar] [PubMed]
- Van Gelder, T.; Hesselink, D.A. Mycophenolate revisited. Transpl. Int. 2015, 28, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Maripuri, S.; Kasiske, B.L. The role of mycophenolate mofetil in kidney transplantation revisited. Transpl. Rev. 2014, 28, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Suthanthiran, M.; Morris, R.E.; Strom, T.B. Immunosuppressants: Cellular and molecular mechanisms of action. Am. J. Kidney Dis. 1996, 28, 159–172. [Google Scholar] [CrossRef]
- Kataoka, M.; Kido, J.-I.; Shinohara, Y.; Nagata, T. Drug-induced gingival overgrowth—A Review. Boil. Pharm. Bull. 2005, 28, 1817–1821. [Google Scholar] [CrossRef] [Green Version]
- Trandafir, D.; Trandafir, V.; Gogalniceanu, D. Gingival overgrowth induced by immunossupressive treatment with cyclosporine a and Mycofenolate mofetil in a patient with kidney transplant—A case report and a literature preview. Int. J. Med. Dent. 2013, 3, 183–187. [Google Scholar]
- Ghafari, A.; Poorabbas, R.; Anvieh Takieh, J.; Sepehrvand, N.; Kargar, C.; Hatami, S. Gingival enlargement and its risk factors in kidney transplant patients rceiving Cyclosporine A. Iran. J. Kidney Dis. 2010, 4, 66–70. [Google Scholar]
- de la Rosa García, E.; Mondragón Padilla, A. The effect of mycophenolate mophetil and azathioprine on gingival overgrowth associated with cyclosporin a use in kidney transplant patients. Nefrología 2009, 29, 474–478. [Google Scholar]
- Ramírez-Rámiz, A.; Brunet-Llobet, L.; Lahor-Soler, E.; Miranda, J. On the cellular and molecular mechanisms of drug-induced gingival overgrowth. Open Dent. J. 2017, 11, 420–435. [Google Scholar] [CrossRef] [Green Version]
- Malek, R.; El Houari, B.; Kissa, J. Periodontal management of Cyclosporin A—Induced gingival overgrowth: A nonsurgical approach. Case Rep. Dent. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Trackman, P.C.; Kantarci, A. Molecular and clinical aspects of drug-induced gingival overgrowth. J. Dent. Res. 2015, 94, 540–546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rapone, B.; Ferrara, E.; Santacroce, L.; Cesarano, F.; Arazzi, M.; Di Liberato, L.; Scacco, S.; Grassi, R.; Grassi, F.R.; Gnoni, A.; et al. Periodontal microbiological status influences the occurrence of Cyclosporine-A and Tacrolimus-induced gingival overgrowth. Antibiotics 2019, 8, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalobos, I.M.; Redondo-De Oro, K.; Díaz Caballero, A. Case report: Gingival overgrowth induced by sirolimus in a patient with kidney transplant. Sch. J. Dent. Sci. 2015, 2, 181–183. [Google Scholar]
- Yoshida, T.; Nagata, J.; Yamane, A. Growth factors and proliferation of cultured rat gingival cells in response to Cyclosporin A. J. Periodontal Res. 2005, 40, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Vahabi, S.; Salman, B.N.; Rezazadeh, F.; Namdari, M. Effects of cyclosporine and phenytoin on biomarker expressions in gingival fibroblasts of children and adults: An in vitro study. J. Basic Clin. Physiol. Pharm. 2014, 25, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Ponnaiyan, D.; Jegadeesan, V. Cyclosporine A: Novel concepts in its role in drug-induced gingival overgrowth. Dent. Res. J. 2016, 12, 499–506. [Google Scholar] [CrossRef]
- Chae, H.-J.; Ha, M.-S.; Yun, D.-H.; Pae, H.-O.; Chung, H.-T.; Chae, S.-W.; Jung, Y.-K.; Kim, H.-R. Mechanism of Cyclosporine-induced overgrowth in gingiva. J. Dent. Res. 2006, 85, 515–519. [Google Scholar] [CrossRef]
- Ganesh, P.R. Immunoexpression of interleukin-6 in drug-induced gingival overgrowth patients. Contemp. Clin. Dent. 2016, 7, 140–145. [Google Scholar] [CrossRef]
- Cotrim, P.; Martelli-Júnior, H.; Graner, E.; Sauk, J.; Coletta, R. Cyclosporin A Induces proliferation in human gingival fibroblasts via induction of transforming growth factor-β1. J. Periodontol. 2003, 74, 1625–1633. [Google Scholar] [CrossRef]
- Yamaguchi, M.; Naruishi, K.; Yamada-Naruishi, H.; Omori, K.; Nishimura, F.; Takashiba, S. Long-term cyclosporin A exposure suppresses cathepsin-B and -L activity in gingival fibroblasts. J. Periodontal Res. 2004, 39, 320–326. [Google Scholar] [CrossRef]
- Gong, Y.; Lu, J.; Ding, X.; Yu, Y. Effect of adjunctive roxithromycin therapy on interleukin-1β, transforming growth factor-β1 and vascular endothelial growth factor in gingival crevicular fluid of cyclosporine A-treated patients with gingival overgrowth. J. Periodontal Res. 2013, 49, 448–457. [Google Scholar] [CrossRef]
- Wu, K.-J.; Huang, G.-F.; Chen, C.-H.; Chang, H.-H.; Deng, Y. Cyclosporine A induces connective tissue growth factor expression in human gingival fibroblasts: Suppression by epigallocatechin-3-gallate. J. Med. Assoc. 2014, 113, 828–832. [Google Scholar] [CrossRef] [PubMed]
- Lauritano, D.; Palmieri, A.; Lucchese, A.; Di Stasio, D.; Moreo, G.; Carinci, F. Role of Cyclosporine in gingival hyperplasia: An in vitro study on gingival fibroblasts. Int. J. Mol. Sci. 2020, 21, 595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmittgen, T.D.; Livak, K.J. Analyzing real-time PCR data by the comparative CT method. Nat. Protoc. 2008, 3, 1101–1108. [Google Scholar] [CrossRef] [PubMed]
- McAnulty, R. Fibroblasts and myofibroblasts: Their source, function and role in disease. Int. J. Biochem. Cell Boil. 2007, 39, 666–671. [Google Scholar] [CrossRef] [PubMed]
- Van Linthout, S.; Miteva, K.; Tschöpe, C. Crosstalk between fibroblasts and inflammatory cells. Cardiovasc. Res. 2014, 102, 258–269. [Google Scholar] [CrossRef] [Green Version]
- Gürkan, A.; Becerik, S.; Öztürk, V.Ö; Atmaca, H.; Atilla, G.; Emingil, G. Interleukin-6 family of Cytokines in crevicular fluid of renal transplant recipients with and without Cyclosporine A—Induced gingival overgrowth. J. Periodontol. 2015, 86, 1069–1077. [Google Scholar] [CrossRef]
- Brown, R.S.; Arany, P.R. Mechanism of drug-induced gingival overgrowth revisited: A unifying hypothesis. Oral Dis. 2014, 21, e51–e61. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Khalil, R.A. Matrix metalloproteinases, vascular remodeling, and vascular disease. Adv. Pharmacol. 2018, 81, 241–330. [Google Scholar] [CrossRef]
- Van Lint, P.; Libert, C. Matrix metalloproteinase-8: Cleavage can be decisive. Cytokine Growth Factor Rev. 2006, 17, 217–223. [Google Scholar] [CrossRef]
- Decock, J.; Hendrickx, W.; Thirkettle, S.; Gutiérrez-Fernández, A.; Robinson, S.D.; Edwards, D.R. Pleiotropic functions of the tumor- and metastasis-suppressing matrix metalloproteinase-8 in mammary cancer in MMTV-PyMT transgenic mice. Breast Cancer Res. 2015, 17, 38. [Google Scholar] [CrossRef] [Green Version]
- Matziari, M.; Dive, V.; Yiotakis, A. Matrix metalloproteinase 11 (MMP-11; stromelysin-3) and synthetic inhibitors. Med. Res. Rev. 2007, 27, 528–552. [Google Scholar] [CrossRef] [PubMed]
- Pecina-Slaus, N. Tumor suppressor gene E-cadherin and its role in normal and malignant cells. Cancer Cell Int. 2003, 3, 17. [Google Scholar] [CrossRef] [Green Version]
- Tu, H.-P.; Chen, Y.-T.; Shieh, Y.-S.; Chin, Y.-T.; Huang, R.-Y.; Yang, S.-F.; Gau, C.-H.; Fu, E. Cyclosporin-induced downregulation of the expression of E-Cadherin during proliferation of edentulous Gingival Epithelium in rats. J. Periodontol. 2006, 77, 832–839. [Google Scholar] [CrossRef]
- Sume, S.S.; Kantarci, A.; Lee, A.; Hasturk, H.; Trackman, P.C. Epithelial to mesenchymal transition in gingival overgrowth. Am. J. Pathol. 2010, 177, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Lu, J.; Yu, Y.; Gong, Y. Epithelial to mesenchymal transition in Cyclosporine A—Induced rat gingival overgrowth. Arch. Oral Boil. 2017, 81, 48–55. [Google Scholar] [CrossRef]
- Lamouille, S.; Subramanyam, D.; Blelloch, R.; Derynck, R. Regulation of epithelial-mesenchymal and mesenchymal-epithelial transitions by microRNAs. Curr. Opin. Cell Boil. 2013, 25, 200–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Pauw, M.T.; Bos, T.V.D.; Everts, V.; Beertsen, W. Phagocytosis of fibronectin and collagens type i, iii, and v by human gingival and periodontal ligament fibroblasts in vitro. J. Periodontol. 2001, 72, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Ríos, M.H.; Sorsa, T.; Obregón, F.; Tervahartiala, T.; Valenzuela, M.A.; Pozo, P.; Dutzan, N.; Lesaffre, E.; Molas, M.; Gamonal, J. Proteolytic roles of matrix metalloproteinase (MMP)-13 during progression of chronic periodontitis: Initial evidence for MMP-13/MMP-9 activation cascade. J. Clin. Periodontol. 2009, 36, 1011–1017. [Google Scholar] [CrossRef]
- Gürkan, A.; Emingil, G.; Afacan, B.; Berdeli, A.; Atilla, G. Alpha 2 integrin gene (ITGA2) polymorphism in renal transplant recipients with and without drug induced gingival overgrowth. Arch. Oral Boil. 2014, 59, 283–288. [Google Scholar] [CrossRef]
- Liu, C.; Tao, T.; Zhao, L.; Ding, Y. Decreased Alpha 2 integrin gene expression in non-familial gingival fibromatosis: A report of two cases. Int. J. Clin. Exp. Pathol. 2017, 10, 7492–7497. [Google Scholar] [PubMed]



{kind=link}
{kind=link}
| Gene | Fold Change | Gene Function |
|---|---|---|
| CD44 | 1.56 | Cell-Cell Adhesion (MIM:107269) |
| CDH1 | 4.62 | Cell-Cell Adhesion (MIM:192090) |
| COL1A2 | 2.20 | Collagens and Extracellular Matrix Structural constituent (MIM:192090) |
| COL2A1 | 1.71 | Collagens and Extracellular Matrix Structural constituent (MIM:120140) |
| COL3A1 | 1.71 | Collagens and Extracellular Matrix Structural constituent (MIM:120180) |
| COL4A1 | 3.43 | Collagens and Extracellular Matrix Structural constituent (MIM:120130) |
| COL5A1 | 1.31 | Collagens and Extracellular Matrix Structural constituent (MIM:120215) |
| COL6A1 | 1.69 | Collagens and Extracellular Matrix Structural constituent (MIM:120220) |
| COL7A1 | 0.74 | Collagens and Extracellular Matrix Structural constituent (MIM:120120) |
| COL8A1 | 2.54 | Collagens and Extracellular Matrix Structural constituent (MIM:120251) |
| COL9A1 | 1.42 | Collagens and Extracellular Matrix Structural constituent (MIM:120210) |
| COL10A1 | 2.10 | Collagens and Extracellular Matrix Structural constituent (MIM:120110) |
| COL11A1 | 1.95 | Collagens and Extracellular Matrix Structural constituent (MIM:120280) |
| CTNNA1 | 2.19 | Cell Adhesion Molecule (MIM:116805) |
| CTNNB1 | 2.36 | Cell Adhesion Molecule (MIM:116806) |
| CTNND2 | 0.95 | Cell Adhesion Molecule (MIM:604275) |
| FN1 | 1.03 | Cell Adhesion Molecule (MIM:135600) |
| HAS1 | 1.86 | Transmembrane Receptor (MIM:601463) |
| ILF3 | 1.73 | Transmembrane Receptor (MIM:603182) |
| ITGA1 | 3.72 | Transmembrane Receptor (MIM:192968) |
| ITGA2 | 5.30 | Transmembrane Receptor (MIM:192974) |
| ITGA3 | 3.04 | Transmembrane Receptor (MIM:605025) |
| ITGA4 | 1.71 | Transmembrane Receptor (MIM:192975) |
| ITGA5 | 2.82 | Transmembrane Receptor (MIM:135620) |
| ITGA6 | 1.84 | Transmembrane Receptor (MIM:147556) |
| ITGA7 | 4.81 | Transmembrane Receptor (MIM:600536) |
| ITGA8 | 1.82 | Transmembrane Receptor (MIM:604063) |
| ITGB1 | 2.22 | Transmembrane Receptor (MIM:135630) |
| ITGB2 | 0.91 | Transmembrane Receptor (MIM:600065) |
| ITGB4 | 0.59 | Transmembrane Receptor (MIM:147557) |
| ITGB5 | 1.46 | Transmembrane Receptor (MIM:147561) |
| LAMA1 | 1.30 | Basement Membrane Constituent (MIM:150320) |
| LAMA2 | 0.12 | Basement Membrane Constituent (MIM:156225) |
| LAMA3 | 1.63 | Basement Membrane Constituent (MIM:600805) |
| LAMB1 | 0.50 | Basement Membrane Constituent (MIM:150240) |
| LAMB2 | 2.08 | Basement Membrane Constituent (MIM:150325) |
| LAMB3 | 4.86 | Basement Membrane Constituent (MIM:150310) |
| MMP2 | 1.61 | Extracellular Matrix Protease (MIM:120360) |
| MMP3 | 2.90 | Extracellular Matrix Protease (MIM:185250) |
| MMP7 | 2.37 | Extracellular Matrix Protease (MIM:178990) |
| MMP8 | 0.45 | Extracellular Matrix Protease (MIM:120355) |
| MMP9 | 1.43 | Extracellular Matrix Protease (MIM:120361) |
| MMP10 | 4.59 | Extracellular Matrix Protease (MIM:185260) |
| MMP11 | 0.03 | Extracellular Matrix Protease (MIM:185261) |
| MMP12 | 4.26 | Extracellular Matrix Protease (MIM:601046) |
| MMP13 | 3.82 | Extracellular Matrix Protease (MIM:600108) |
| MMP14 | 1.20 | Extracellular Matrix Protease (MIM:600754) |
| MMP15 | 0.06 | Extracellular Matrix Protease (MIM:602261) |
| MMP16 | 0.42 | Extracellular Matrix Protease (MIM:602262) |
| MMP24 | 0.09 | Extracellular Matrix Protease (MIM:604871) |
| MMP26 | 3.43 | Extracellular Matrix Protease (MIM:605470) |
| TGFB1 | 1.51 | TGF-β Signaling (MIM:190180) |
| TGFB2 | 1.25 | TGF-β Signaling (MIM:190220) |
| TGFB3 | 1.05 | TGF-β Signaling (MIM:190230) |
| TIMP1 | 1.09 | Extracellular Matrix Protease Inhibitor (MIM:305370) |
| VCAN | 1.07 | Cell Adhesion Molecule (MIM:118661) |
| RPL13 | 1.00 | Housekeeping gene (MIM:113703) |
| Gene | Fold Change | Gene Function |
|---|---|---|
| CD44 | 0.74 | Cell-Cell Adhesion (MIM:107269) |
| CDH1 | 5.01 | Cell-Cell Adhesion (MIM:192090) |
| COL1A2 | 0.92 | Collagens and Extracellular Matrix Structural constituent (MIM:192090) |
| COL2A1 | 0.62 | Collagens and Extracellular Matrix Structural constituent (MIM:120140) |
| COL3A1 | 0.85 | Collagens and Extracellular Matrix Structural constituent (MIM:120180) |
| COL4A1 | 1.73 | Collagens and Extracellular Matrix Structural constituent (MIM:120130) |
| COL5A1 | 0.62 | Collagens and Extracellular Matrix Structural constituent (MIM:120215) |
| COL6A1 | 0.82 | Collagens and Extracellular Matrix Structural constituent (MIM:120220) |
| COL7A1 | 0.26 | Collagens and Extracellular Matrix Structural constituent (MIM:120120) |
| COL8A1 | 0.85 | Collagens and Extracellular Matrix Structural constituent (MIM:120251) |
| COL9A1 | 0.91 | Collagens and Extracellular Matrix Structural constituent (MIM:120210) |
| COL10A1 | 0.97 | Collagens and Extracellular Matrix Structural constituent (MIM:120110) |
| COL11A1 | 0.85 | Collagens and Extracellular Matrix Structural constituent (MIM:120280) |
| CCTNA1 | 1.25 | Cell Adhesion Molecule (MIM:116805) |
| CTNB | 1.27 | Cell Adhesion Molecule (MIM:116806) |
| CTNND2 | 0.96 | Cell Adhesion Molecule (MIM:604275) |
| FN1 | 0.56 | Cell Adhesion Molecule (MIM:135600) |
| HAS1 | 0.97 | Transmembrane Receptor (MIM:601463) |
| ILF3 | 0.93 | Transmembrane Receptor (MIM:603182) |
| ITGA1 | 1.31 | Transmembrane Receptor (MIM:192968) |
| ITGA2 | 2.05 | Transmembrane Receptor (MIM:192974) |
| ITGA3 | 1.47 | Transmembrane Receptor (MIM:605025) |
| ITGA4 | 0.99 | Transmembrane Receptor (MIM:192975) |
| ITGA5 | 1.51 | Transmembrane Receptor (MIM:135620) |
| ITGA6 | 1.08 | Transmembrane Receptor (MIM:147556) |
| ITGA7 | 2.75 | Transmembrane Receptor (MIM:600536) |
| ITGA8 | 0.77 | Transmembrane Receptor (MIM:604063) |
| ITGB1 | 1.03 | Transmembrane Receptor (MIM:135630) |
| ITGB2 | 0.34 | Transmembrane Receptor (MIM:600065) |
| ITGB4 | 0.19 | Transmembrane Receptor (MIM:147557) |
| ITGB5 | 0.63 | Transmembrane Receptor (MIM:147561) |
| LAMA1 | 0.71 | Basement Membrane Constituent (MIM:150320) |
| LAMA2 | 0.15 | Basement Membrane Constituent (MIM:156225) |
| LAMA3 | 0.89 | Basement Membrane Constituent (MIM:600805) |
| LAMB1 | 0.06 | Basement Membrane Constituent (MIM:150240) |
| LAMB2 | 1.08 | Basement Membrane Constituent (MIM:150325) |
| LAMB3 | 2.37 | Basement Membrane Constituent (MIM:150310) |
| MMP2 | 0.77 | Extracellular Matrix Protease (MIM:120360) |
| MMP3 | 1.05 | Extracellular Matrix Protease (MIM:185250) |
| MMP7 | 0.78 | Extracellular Matrix Protease (MIM:178990) |
| MMP8 | 0.05 | Extracellular Matrix Protease (MIM:120355) |
| MMP9 | 0.92 | Extracellular Matrix Protease (MIM:120361) |
| MMP10 | 1.70 | Extracellular Matrix Protease (MIM:185260) |
| MMP11 | 0.03 | Extracellular Matrix Protease (MIM:185261) |
| MMP12 | 2.07 | Extracellular Matrix Protease (MIM:601046) |
| MMP13 | 2.03 | Extracellular Matrix Protease (MIM:600108) |
| MMP14 | 0.98 | Extracellular Matrix Protease (MIM:600754) |
| MMP15 | 0.05 | Extracellular Matrix Protease (MIM:602261) |
| MMP16 | 0.31 | Extracellular Matrix Protease (MIM:602262) |
| MMP24 | 0.04 | Extracellular Matrix Protease (MIM:604871) |
| MMP26 | 0.49 | Extracellular Matrix Protease (MIM:605470) |
| TGFB1 | 1.24 | TGF-β Signaling (MIM:190180) |
| TGFB2 | 0.74 | TGF-β Signaling (MIM:190220) |
| TGFB3 | 0.77 | TGF-β Signaling (MIM:190230) |
| TIMP1 | 0.88 | Extracellular Matrix Protease Inhibitor (MIM:305370) |
| VCAN | 0.88 | Cell Adhesion Molecule (MIM:118661) |
| RPL13 | 1.00 | Housekeeping gene (MIM:113703) |
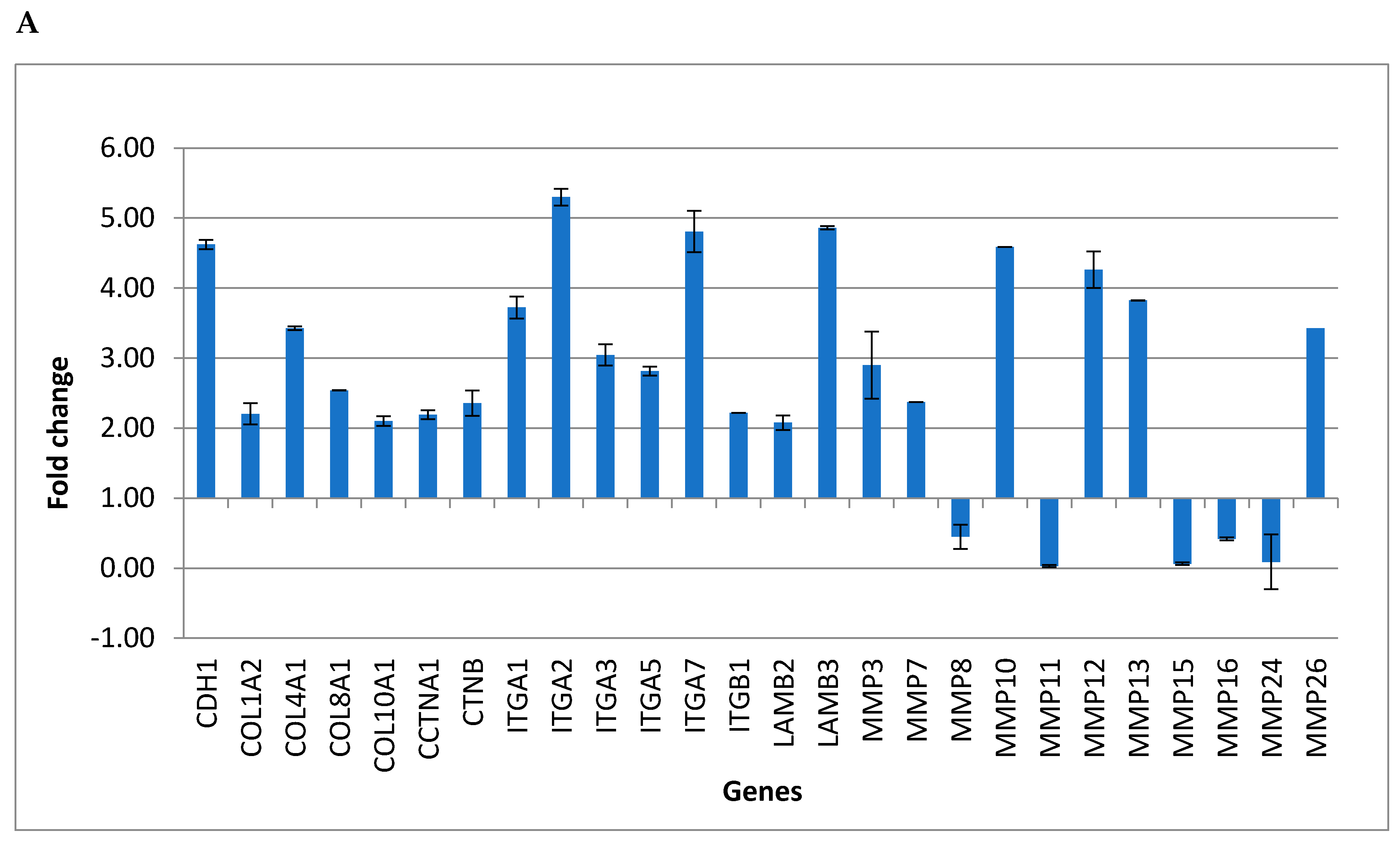
| Gene | Fold Change | SD (+/−) | Gene Function |
|---|---|---|---|
| CDH1 | 4.62 | 0.00 | Cell-Cell Adhesion |
| COL1A2 | 2.20 | 0.07 | Collagens and Extracellular Matrix Structural constituent |
| COL4A1 | 3.43 | 0.15 | Collagens and Extracellular Matrix Structural constituent |
| COL8A1 | 2.54 | 0.02 | Collagens and Extracellular Matrix Structural constituent |
| COL10A1 | 2.10 | 0.00 | Collagens and Extracellular Matrix Structural constituent |
| CCTNA1 | 2.19 | 0.07 | Cell Adhesion Molecule |
| CTNB | 2.36 | 0.06 | Cell Adhesion Molecule |
| ITGA1 | 3.72 | 0.18 | Transmembrane Receptor |
| ITGA2 | 5.30 | 0.16 | Transmembrane Receptor |
| ITGA3 | 3.04 | 0.12 | Transmembrane Receptor |
| ITGA5 | 2.82 | 0.15 | Transmembrane Receptor |
| ITGA7 | 4.81 | 0.06 | Transmembrane Receptor |
| ITGB1 | 2.22 | 0.29 | Transmembrane Receptor |
| LAMB2 | 2.08 | 0.00 | Basement Membrane Constituent |
| LAMB3 | 4.86 | 0.10 | Basement Membrane Constituent |
| MMP3 | 2.90 | 0.02 | Extracellular Matrix Protease |
| MMP7 | 2.37 | 0.48 | Extracellular Matrix Protease |
| MMP8 | 0.45 | 0.00 | Extracellular Matrix Protease |
| MMP10 | 4.59 | 0.17 | Extracellular Matrix Protease |
| MMP11 | 0.03 | 0.00 | Extracellular Matrix Protease |
| MMP12 | 4.26 | 0.02 | Extracellular Matrix Protease |
| MMP13 | 3.82 | 0.26 | Extracellular Matrix Protease |
| MMP15 | 0.06 | 0.00 | Extracellular Matrix Protease |
| MMP16 | 0.42 | 0.02 | Extracellular Matrix Protease |
| MMP24 | 0.09 | 0.02 | Extracellular Matrix Protease |
| MMP26 | 3.43 | 0.39 | Extracellular Matrix Protease |
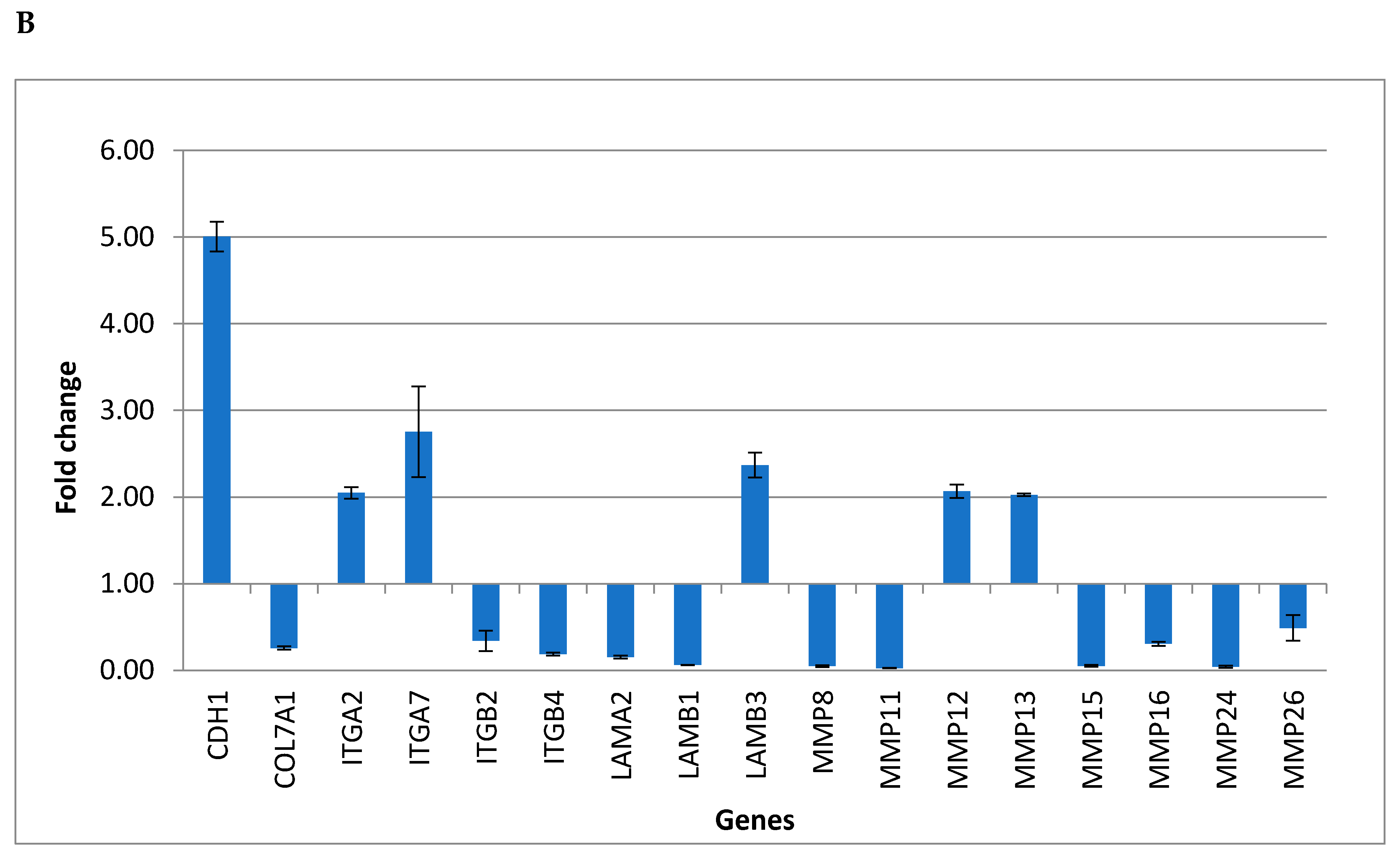
| Gene | Fold Change | SD (+/−) | Gene Function |
|---|---|---|---|
| CDH1 | 5.01 | 0.17 | Cell-Cell Adhesion |
| COL7A1 | 0.26 | 0.02 | Collagens and Extracellular Matrix Structural constituent |
| ITGA2 | 2.05 | 0.07 | Transmembrane Receptor |
| ITGA7 | 2.75 | 0.52 | Transmembrane Receptor |
| ITGB2 | 0.34 | 0.12 | Transmembrane Receptor |
| ITGB4 | 0.19 | 0.02 | Transmembrane Receptor |
| LAMA2 | 0.15 | 0.02 | Basement Membrane Constituent |
| LAMB1 | 0.06 | 0.00 | Basement Membrane Constituent |
| LAMB3 | 2.37 | 0.14 | Basement Membrane Constituent |
| MMP8 | 0.05 | 0.01 | Extracellular Matrix Protease |
| MMP11 | 0.03 | 0.00 | Extracellular Matrix Protease |
| MMP12 | 2.07 | 0.08 | Extracellular Matrix Protease |
| MMP13 | 2.03 | 0.01 | Extracellular Matrix Protease |
| MMP15 | 0.05 | 0.01 | Extracellular Matrix Protease |
| MMP16 | 0.31 | 0.02 | Extracellular Matrix Protease |
| MMP24 | 0.04 | 0.01 | Extracellular Matrix Protease |
| MMP26 | 0.49 | 0.15 | Extracellular Matrix Protease |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lauritano, D.; Moreo, G.; Limongelli, L.; Palmieri, A.; Carinci, F. Drug-Induced Gingival Overgrowth: The Effect of Cyclosporin A and Mycophenolate Mophetil on Human Gingival Fibroblasts. Biomedicines 2020, 8, 221. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8070221
Lauritano D, Moreo G, Limongelli L, Palmieri A, Carinci F. Drug-Induced Gingival Overgrowth: The Effect of Cyclosporin A and Mycophenolate Mophetil on Human Gingival Fibroblasts. Biomedicines. 2020; 8(7):221. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8070221
Chicago/Turabian StyleLauritano, Dorina, Giulia Moreo, Luisa Limongelli, Annalisa Palmieri, and Francesco Carinci. 2020. "Drug-Induced Gingival Overgrowth: The Effect of Cyclosporin A and Mycophenolate Mophetil on Human Gingival Fibroblasts" Biomedicines 8, no. 7: 221. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8070221