Targeting Stereotactic Body Radiotherapy on Metabolic PET- and Immuno-PET-Positive Vertebral Metastases

 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Population
2.1.1. Breast Cancer Cohort
2.1.2. Medullary Thyroid Cancer Cohort
2.2. PET/CT and MRI Imaging
2.2.1. PET/CT Imaging
2.2.2. iPET-CT Imaging
2.2.3. MRI Acquisition
2.3. Analysis of CTVs Determined by MRI and PET and Determination of Sensitivity
2.4. Statistical Methods
3. Results
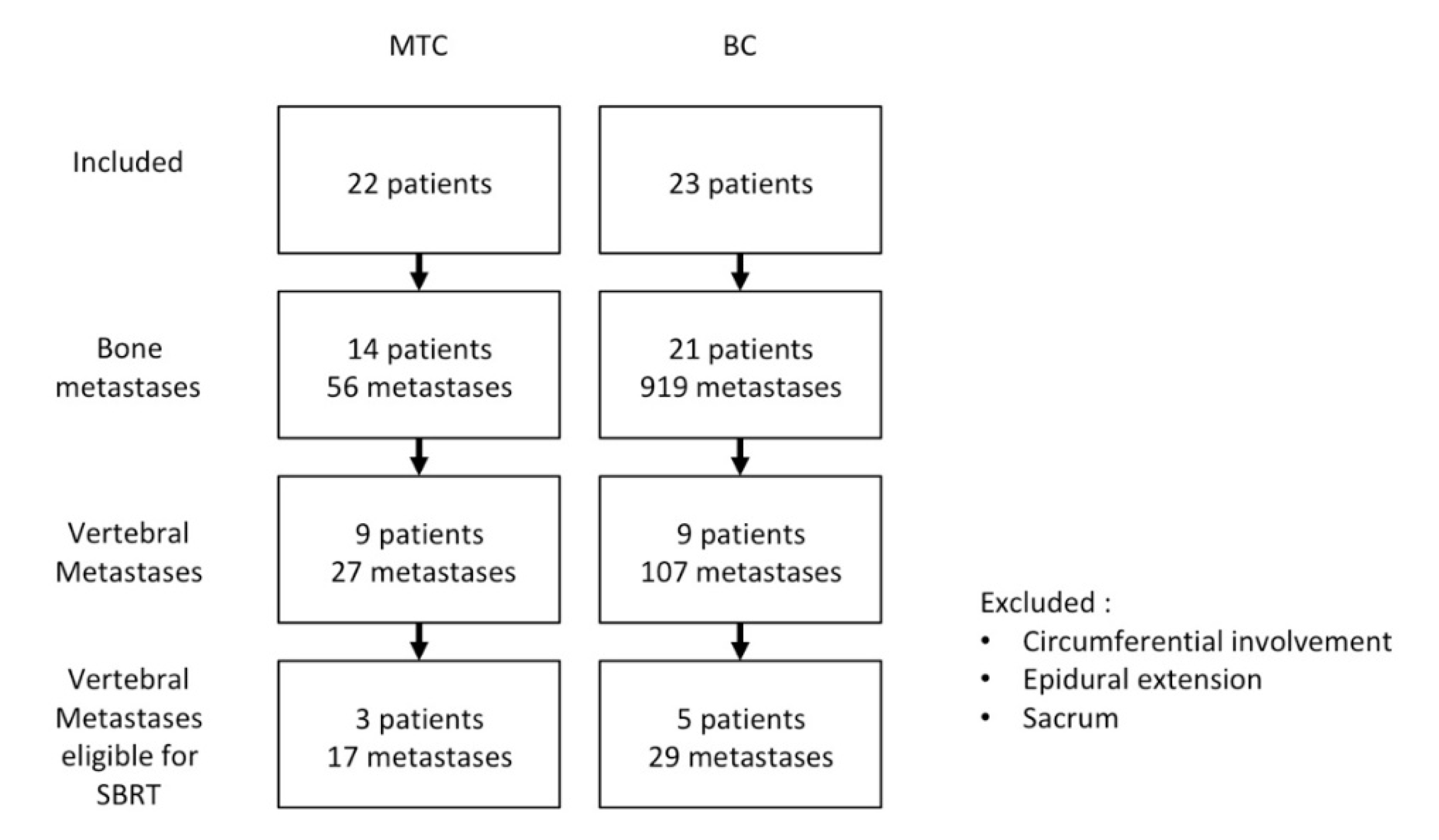
3.1. Patient Population and Number of Vertebrae
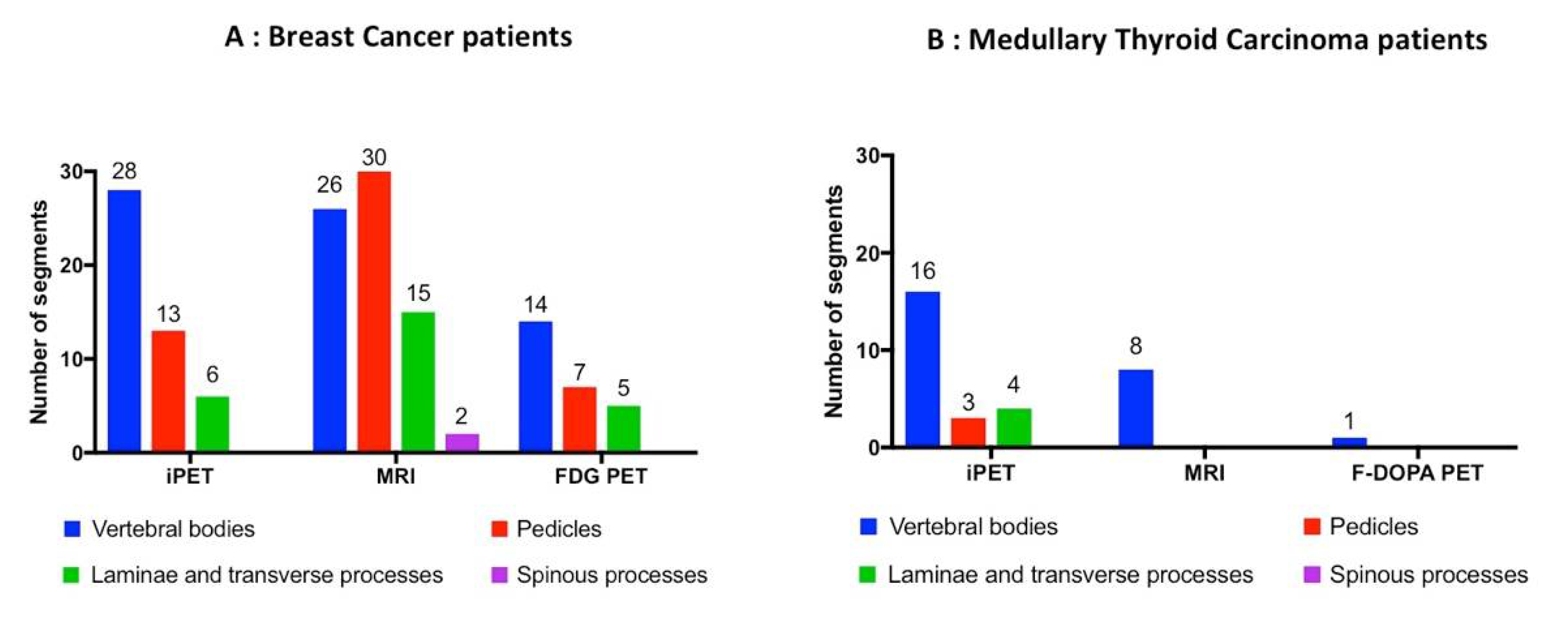
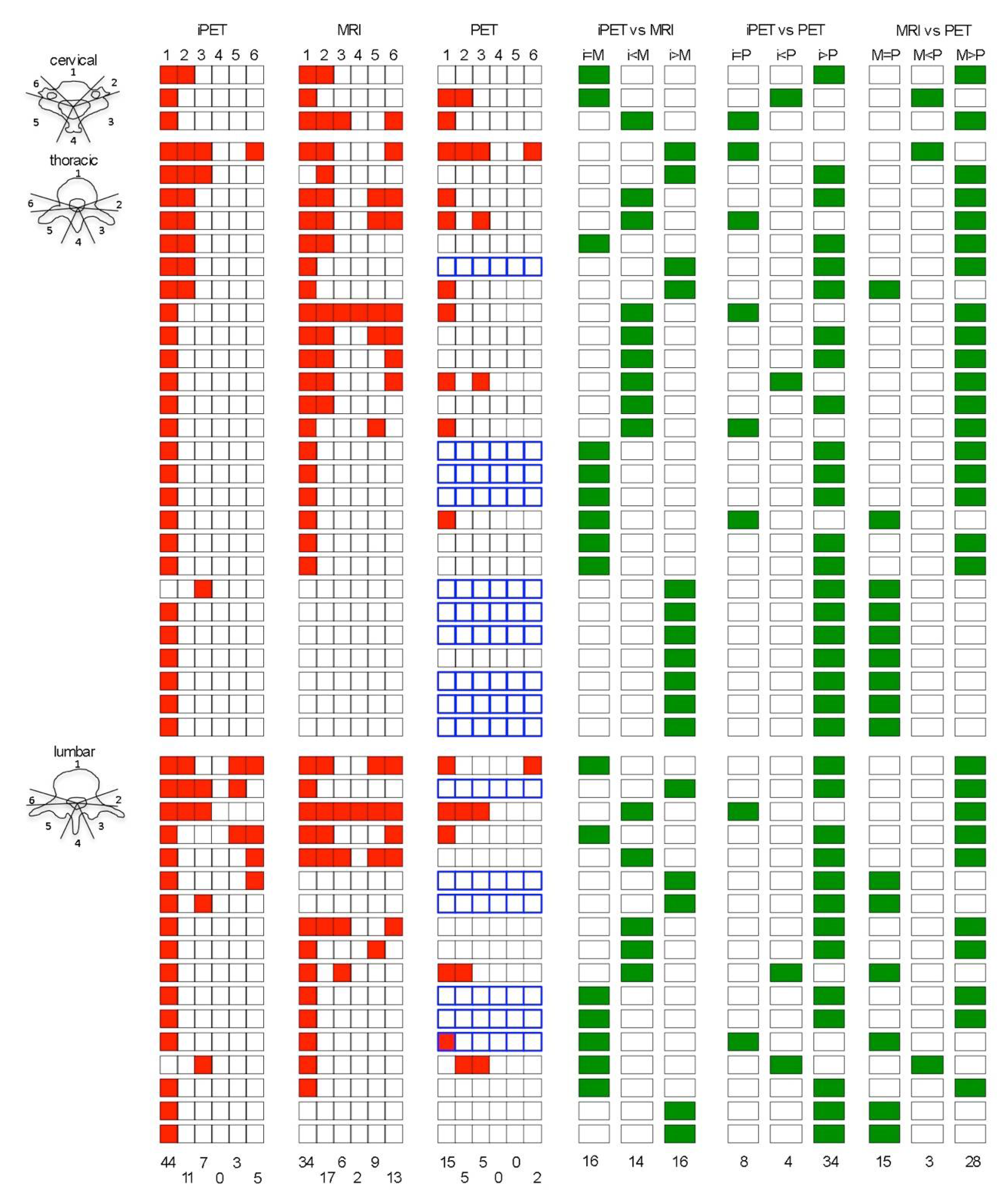
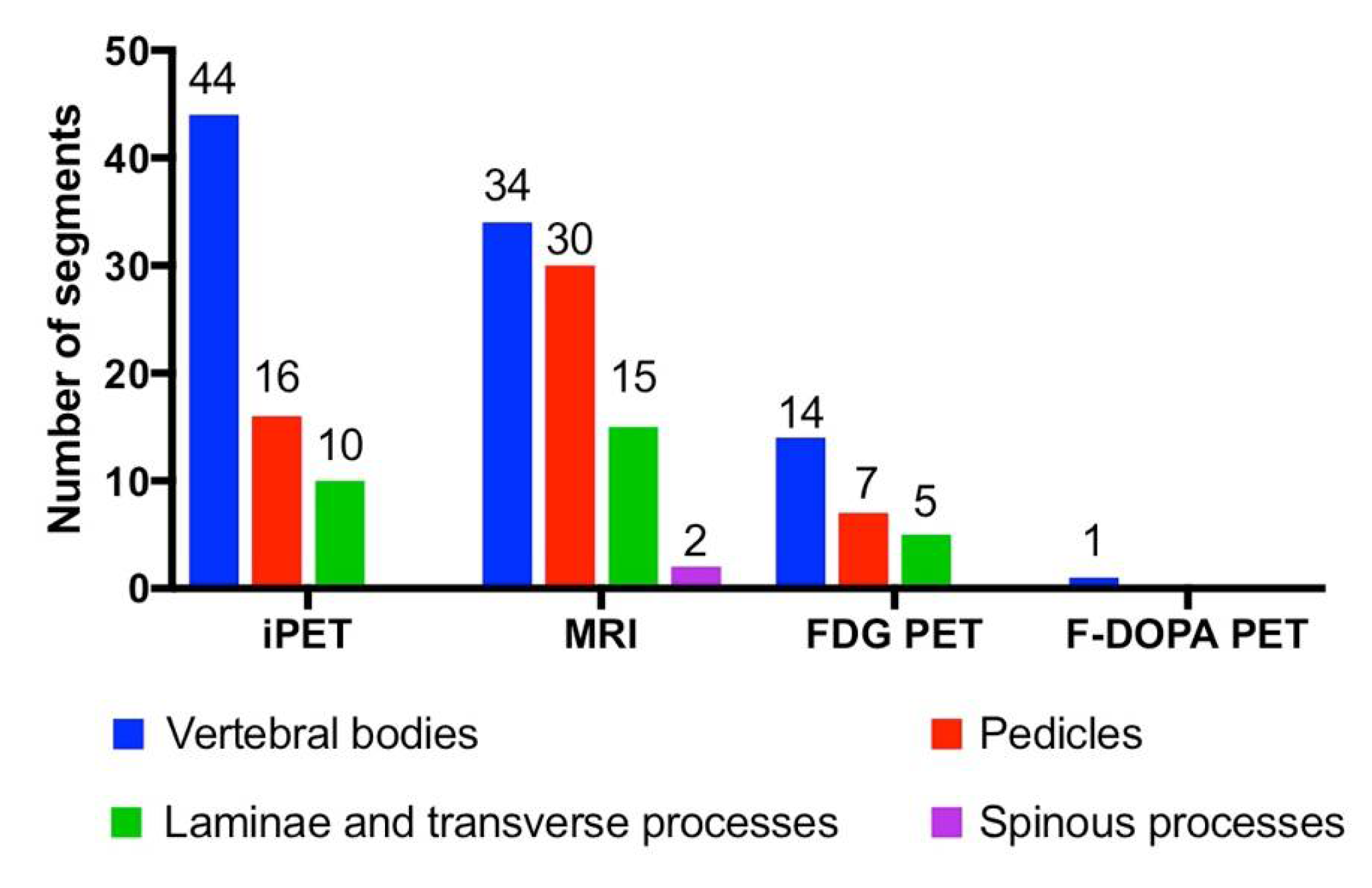
3.2. Vertebral Segments Analysis
3.3. CTV Delineation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| SABR | stereotactic ablative radiotherapy |
| SBRT | stereotactic body radiation therapy |
| VM | vertebral metastasis |
| CTV | clinical target volume |
| CEA | carcino embryonic antigen |
| iPET | immuno positron emission tomography |
| PET-CT | positron emission tomography-computed tomography |
| BC | breast cancer |
| MTC | medullary thyroid carcinoma |
| MRI | magnetic resonance imaging |
| F-DOPA | l-3,4-dihydroxy-6-[18f]fluorophenylalanine |
| FDG | fluoro desoxy glucose |
| HAMA | human antimouse antibody |
| HAHA | human antihuman antibody |
| IQR | interquartile range |
| ISRC | International Spine Radiosurgery Consortium |
References
- Husain, Z.A.; Sahgal, A.; De Salles, A.; Funaro, M.; Glover, J.; Hayashi, M.; Hiraoka, M.; Levivier, M.; Ma, L.; Martinez-Alvarez, R.; et al. Stereotactic body radiotherapy for de novo spinal metastases: Systematic review. J. Neurosurg. Spine 2017, 27, 295–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossa-Basha, M.; Gerszten, P.C.; Myrehaug, S.; Mayr, N.A.; Yuh, W.T.; Jabehdar Maralani, P.; Sahgal, A.; Lo, S.S. Spinal metastasis: Diagnosis, management and follow-up. Br. J. Radiol. 2019, 92, 20190211. [Google Scholar] [CrossRef] [PubMed]
- Pichon, B.; Campion, L.; Delpon, G.; Thillays, F.; Carrie, C.; Cellier, P.; Pommier, P.; Laude, C.; Mervoyer, A.; Hamidou, H.; et al. High-Dose Hypofractionated Radiation Therapy for Noncompressive Vertebral Metastases in Combination With Zoledronate: A Phase 1 Study. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, 840–847. [Google Scholar] [CrossRef] [PubMed]
- Glicksman, R.M.; Tjong, M.C.; Neves-Junior, W.F.P.; Spratt, D.E.; Chua, K.L.M.; Mansouri, A.; Chua, M.L.K.; Berlin, A.; Winter, J.D.; Dahele, M.; et al. Stereotactic Ablative Radiotherapy for the Management of Spinal Metastases: A Review. JAMA Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Cox, B.W.; Spratt, D.E.; Lovelock, M.; Bilsky, M.H.; Lis, E.; Ryu, S.; Sheehan, J.; Gerszten, P.C.; Chang, E.; Gibbs, I.; et al. International Spine Radiosurgery Consortium consensus guidelines for target volume definition in spinal stereotactic radiosurgery. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e597–e605. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.L.; Liu, T.; Wang, X.M.; Xu, Y.; Deng, S.M. Diagnosis of bone metastases: A meta-analysis comparing (1)(8)FDG PET, CT, MRI and bone scintigraphy. Eur. Radiol. 2011, 21, 2604–2617. [Google Scholar] [CrossRef] [PubMed]
- Qu, X.; Huang, X.; Yan, W.; Wu, L.; Dai, K. A meta-analysis of (1)(8)FDG-PET-CT, (1)(8)FDG-PET, MRI and bone scintigraphy for diagnosis of bone metastases in patients with lung cancer. Eur. J. Radiol. 2012, 81, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Bailly, C.; Clery, P.F.; Faivre-Chauvet, A.; Bourgeois, M.; Guerard, F.; Haddad, F.; Barbet, J.; Cherel, M.; Kraeber-Bodere, F.; Carlier, T.; et al. Immuno-PET for Clinical Theranostic Approaches. Int. J. Mol. Sci. 2016, 18, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rousseau, C.; Goldenberg, D.M.; Colombie, M.; Sebille, J.C.; Meingan, P.; Ferrer, L.; Baumgartner, P.; Cerato, E.; Masson, D.; Campone, M.; et al. Initial Clinical Results of a Novel Immuno-PET Theranostic Probe in HER2-negative Breast Cancer. J. Nucl. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Bodet-Milin, C.; Faivre-Chauvet, A.; Carlier, T.; Rauscher, A.; Bourgeois, M.; Cerato, E.; Rohmer, V.; Couturier, O.; Drui, D.; Goldenberg, D.M.; et al. Immuno-PET Using Anticarcinoembryonic Antigen Bispecific Antibody and 68Ga-Labeled Peptide in Metastatic Medullary Thyroid Carcinoma: Clinical Optimization of the Pretargeting Parameters in a First-in-Human Trial. J. Nucl. Med. 2016, 57, 1505–1511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touchefeu, Y.; Bailly, C.; Frampas, E.; Eugène, T.; Rousseau, C.; Bourgeois, M.; Bossard, C.; Faivre-Chauvet, A.; Rauscher, A.; Masson, D.; et al. Promising clinical performance of pretargeted immuno-PET with anti-CEA bispecific antibody and gallium-68-labelled IMP-288 peptide for imaging colorectal cancer metastases: A pilot study. Eur. J. Nucl. Med. Mol. Imaging 2020. [Google Scholar] [CrossRef] [PubMed]
- Hrinivich, W.T.; Phillips, R.; Da Silva, A.J.; Radwan, N.; Gorin, M.A.; Rowe, S.P.; Pienta, K.J.; Pomper, M.G.; Wong, J.; Tran, P.T.; et al. Online Prostate-Specific Membrane Antigen and Positron Emission Tomography-Guided Radiation Therapy for Oligometastatic Prostate Cancer. Adv. Radiat. Oncol. 2020, 5, 260–268. [Google Scholar] [CrossRef] [PubMed]
- Jabehdar Maralani, P.; Lo, S.S.; Redmond, K.; Soliman, H.; Myrehaug, S.; Husain, Z.A.; Heyn, C.; Kapadia, A.; Chan, A.; Sahgal, A. Spinal metastases: Multimodality imaging in diagnosis and stereotactic body radiation therapy planning. Future Oncol. 2017, 13, 77–91. [Google Scholar] [CrossRef] [PubMed]
- Metser, U.; Lerman, H.; Blank, A.; Lievshitz, G.; Bokstein, F.; Even-Sapir, E. Malignant involvement of the spine: Assessment by 18F-FDG PET/CT. J. Nucl. Med. 2004, 45, 279–284. [Google Scholar] [PubMed]
- Gwak, H.S.; Youn, S.M.; Chang, U.; Lee, D.H.; Cheon, G.J.; Rhee, C.H.; Kim, K.; Kim, H.J. Usefulness of (18)F-fluorodeoxyglucose PET for radiosurgery planning and response monitoring in patients with recurrent spinal metastasis. Minim. Invasive Neurosurg. 2006, 49, 127–134. [Google Scholar] [CrossRef] [PubMed]
- Harris, L.; Fritsche, H.; Mennel, R.; Norton, L.; Ravdin, P.; Taube, S.; Somerfield, M.R.; Hayes, D.F.; Bast, R.C., Jr. American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J. Clin. Oncol. 2007, 25, 5287–5312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oudoux, A.; Salaun, P.Y.; Bournaud, C.; Campion, L.; Ansquer, C.; Rousseau, C.; Bardet, S.; Borson-Chazot, F.; Vuillez, J.P.; Murat, A.; et al. Sensitivity and prognostic value of positron emission tomography with F-18-fluorodeoxyglucose and sensitivity of immunoscintigraphy in patients with medullary thyroid carcinoma treated with anticarcinoembryonic antigen-targeted radioimmunotherapy. J. Clin. Endocrinol. Metab. 2007, 92, 4590–4597. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| iPET | MRI | FDG-PET | F-DOPA PET | ||
|---|---|---|---|---|---|
| BC | Cervical | 3 | 3 | 2 | NA |
| Thoracic | 16 | 15 | 8 | NA | |
| Lumbar | 10 | 9 | 5 | NA | |
| MTC | Cervical | 0 | 0 | NA | 0 |
| Thoracic | 10 | 4 | NA | 0 | |
| Lumbar | 7 | 4 | NA | 1 | |
| Total | 46 | 35 | 15 | 1 |
| Location | iPET | MRI | FDG-PET | F-DOPA PET | Number of Individual Vertebrae Segments | |
|---|---|---|---|---|---|---|
| BC | Total | 47 | 73 | 26 | NA | 86 |
| Cervical | 4 | 7 | 3 | NA | 8 | |
| Thoracic | 25 | 38 | 13 | NA | 45 | |
| Lumbar | 18 | 28 | 10 | NA | 33 | |
| MTC | Total | 23 | 8 | NA | 1 | 23 |
| cervical | 0 | 0 | NA | 0 | 0 | |
| Thoracic | 11 | 4 | NA | 0 | 11 | |
| Lumbar | 12 | 4 | NA | 1 | 12 | |
| BC + MTC | Total | 70 | 81 | 109 | ||
| Cervical | 4 | 7 | 8 | |||
| Thoracic | 36 | 42 | 56 | |||
| Lumbar | 30 | 32 | 45 | |||
| Sensitivity | 64% (70/109) | 74% (81/109) | 30% (26/86) | 4% (1/23) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pichon, B.; Rousseau, C.; Blanc-Lapierre, A.; Delpon, G.; Ferrer, L.; Libois, V.; Le Turnier, M.; Lenoble, C.; Bodet-Milin, C.; Goldenberg, D.M.; et al. Targeting Stereotactic Body Radiotherapy on Metabolic PET- and Immuno-PET-Positive Vertebral Metastases. Biomedicines 2020, 8, 548. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120548
Pichon B, Rousseau C, Blanc-Lapierre A, Delpon G, Ferrer L, Libois V, Le Turnier M, Lenoble C, Bodet-Milin C, Goldenberg DM, et al. Targeting Stereotactic Body Radiotherapy on Metabolic PET- and Immuno-PET-Positive Vertebral Metastases. Biomedicines. 2020; 8(12):548. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120548
Chicago/Turabian StylePichon, Baptiste, Caroline Rousseau, Audrey Blanc-Lapierre, Gregory Delpon, Ludovic Ferrer, Vincent Libois, Matthieu Le Turnier, Cédric Lenoble, Caroline Bodet-Milin, David M. Goldenberg, and et al. 2020. "Targeting Stereotactic Body Radiotherapy on Metabolic PET- and Immuno-PET-Positive Vertebral Metastases" Biomedicines 8, no. 12: 548. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120548