Expression of Circulating MicroRNAs Linked to Bone Metabolism in Chronic Kidney Disease-Mineral and Bone Disorder

 ,
,  ,
,  , , and
, , and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Medical Records
2.2. BMD Measurements
2.3. Blood Sampling and Isolation of MicroRNAs from the Serum
2.4. Reverse Transcription and PCR Analysis
Quality Control
2.5. MicroRNA Primer Assays
2.6. Biochemical Assays
2.7. Statistical Analysis
3. Results
3.1. Study Population
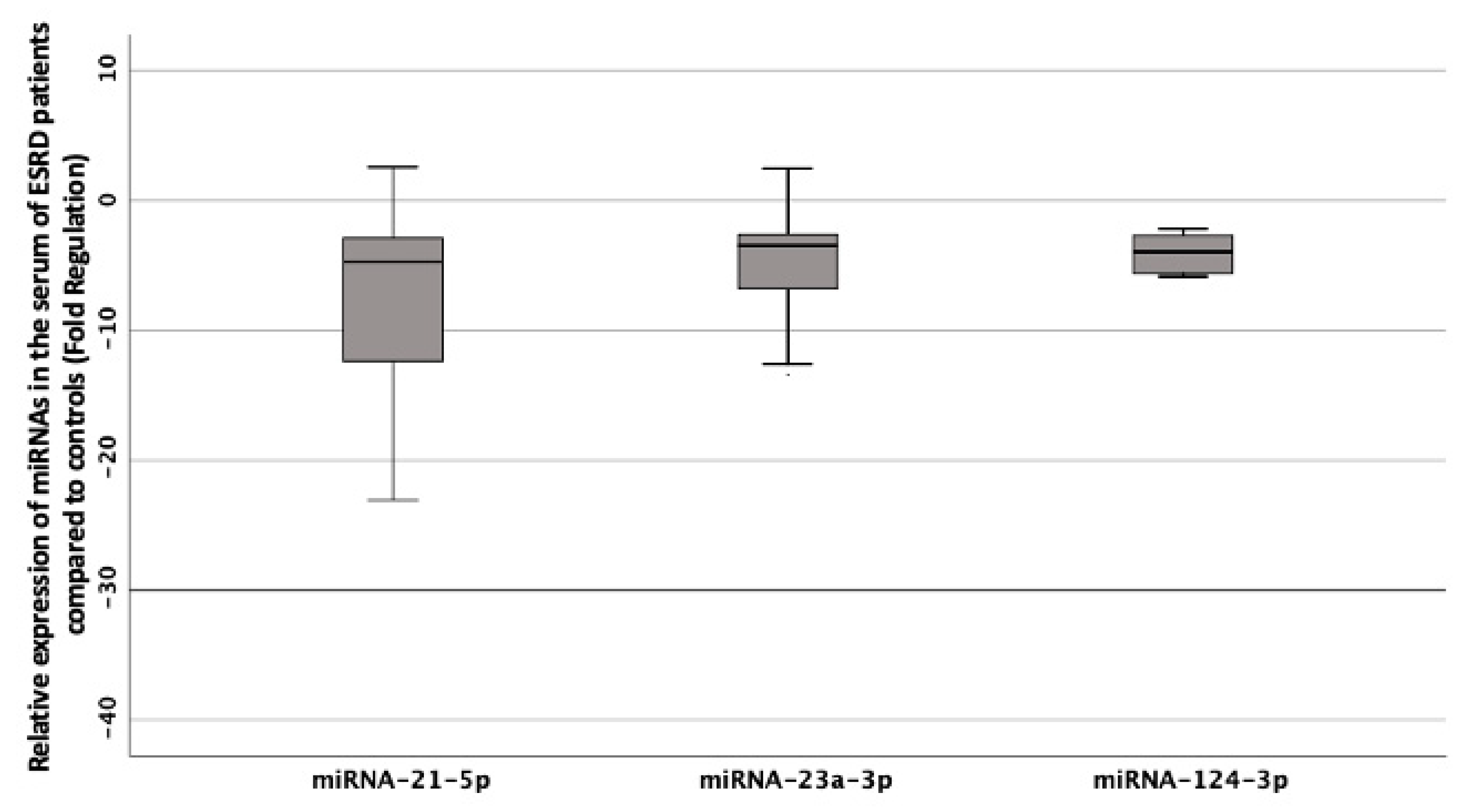
3.2. Differential Expression of the Selected Panel of MiRNAs Linked to Bone Metabolism in the Serum of Patients with CKD on HD Compared to Controls
4. Discussion
Author Contributions
Funding
Conflicts of Interest
Abbreviations
| miRNA | microRNAs |
| CKD-MBD | Chronic kidney disease-mineral and bone disorder |
| HD | Hemodialysis |
| KDIGO | Kidney Disease Improving Global Outcomes |
| DXA | Dual energy X-ray absorptiometry |
| TBS | Trabecular bone score |
| PMO | Postmenopausal osteoporosis |
| ESRD | End Stage Renal Disease |
| BMI | Body Mass Index |
| GDPR | General data protection regulation |
| BMD | Bone mineral density |
| LS | Lumbar spine |
| FN | Femoral neck |
| TH | Total hip |
| PTH | Parathyroid hormone |
| CVA | coefficient of variation for analytical imprecision |
| Β-CTX | C-terminal cross-linking telopeptide of type I collagen |
| P1NP | Procollagen type 1 N-terminal propeptide |
| SD | Standard deviation |
| RANKL | Receptor activator of nuclear factor kappa-B ligand |
| NFATc1 | Nuclear factor of activated T-cells |
| LN | Lupus nephritis |
| IL | Interleukins |
| TNF-α | Tumor necrosis factor-alpha |
| TRAF6 | TNF receptor associated factor-6 |
| RUNX2 | Runt |
| AKI | Acute kidney injury |
| AMI | Acute myocardial infarction |
| TGF-β | Transforming growth factor beta |
| AIDS | Acquired immune deficiency syndrome |
References
- Kidney Disease: Improving Global Outcomes (KDIGO) CKD-MBD Work Group. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD). Kidney Int. Suppl. 2009, 113, S1–S130. [Google Scholar]
- Ketteler, M.; Block, G.A.; Evenepoel, P.; Fukagawa, M.; Herzog, C.A.; McCann, L.; Moe, S.M.; Shroff, R.; Tonelli, M.A.; Toussaint, N.D.; et al. Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Guideline Update: What’s changed and why it matters. Kidney Int. 2017, 92, 26–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alem, A.M.; Sherrard, D.J.; Gillen, D.L.; Weiss, N.S.; Beresford, S.A.; Heckbert, S.R.; Wong, C.; Stehman-Breen, C. Increased risk of hip fracture among patients with end-stage renal disease. Kidney Int. 2000, 58, 396–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fusaro, M.; Tripepi, G.; Noale, M.; Vajente, N.; Plebani, M.; Zaninotto, M.; Guglielmi, G.; Miotto, D.; Dalle Carbonare, L.; D’Angelo, A.; et al. High prevalence of vertebral fractures assessed by quantitative morphometry in hemodialysis patients, strongly associated with vascular calcifications. Calcif. Tissue Int. 2013, 93, 39–47. [Google Scholar] [CrossRef]
- Coresh, J.; Longenecker, J.C.; Miller, E.R., 3rd; Young, H.J.; Klag, M.J. Epidemiology of cardiovascular risk factors in chronic renal disease. J. Am. Soc. Nephrol. 1998, 9 (Suppl. 12), S24–S30. [Google Scholar]
- Dounousi, E.; Leivaditis, K.; Eleftheriadis, T.; Liakopoulos, V. Osteoporosis after renal transplantation. Int. Urol. Nephrol. 2015, 47, 503–511. [Google Scholar] [CrossRef]
- Jamal, S.A.; Chase, C.; Goh, Y.I.; Richardson, R.; Hawker, G.A. Bone density and heel ultrasound testing do not identify patients with dialysis-dependent renal failure who have had fractures. Am. J. Kidney Dis. 2002, 39, 843–849. [Google Scholar] [CrossRef]
- Negri, A.L.; Barone, R.; Quiroga, M.A.; Bravo, M.; Marino, A.; Fradinger, E.; Bogado, C.E.; Zanchetta, J.R. Bone mineral density: Serum markers of bone turnover and their relationships in peritoneal dialysis. Perit. Dial. Int. 2004, 24, 163–168. [Google Scholar] [CrossRef]
- Pimentel, A.; Urena-Torres, P.; Zillikens, M.C.; Bover, J.; Cohen-Solal, M. Fractures in patients with CKD-diagnosis, treatment, and prevention: A review by members of the European Calcified Tissue Society and the European Renal Association of Nephrology Dialysis and Transplantation. Kidney Int. 2017, 92, 1343–1355. [Google Scholar] [CrossRef] [Green Version]
- Martineau, P.; Leslie, W.D. Trabecular bone score (TBS): Method and applications. Bone 2017, 104, 66–72. [Google Scholar] [CrossRef]
- Dusceac, R.; Niculescu, D.A.; Dobre, R.; Dragne, M.C.; Tacu, C.; Peride, I.; David, C.; Checherita, I.; Poiana, C. Chronic hemodialysis is associated with lower trabecular bone score, independent of bone mineral density: A case-control study. Arch. Osteoporos 2018, 13, 125. [Google Scholar] [CrossRef] [PubMed]
- Yavropoulou, M.P.; Vaios, V.; Pikilidou, M.; Chryssogonidis, I.; Sachinidou, M.; Tournis, S.; Makris, K.; Kotsa, K.; Daniilidis, M.; Haritanti, A.; et al. Bone Quality Assessment as Measured by Trabecular Bone Score in Patients With End-Stage Renal Disease on Dialysis. J. Clin. Densitom. 2017, 20, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.E.; Kim, Y.; Shin, S.J.; Hong, Y.S.; Kang, K.Y. Factors associated with low trabecular bone scores in patients with end-stage kidney disease. J. Bone Miner Metab. 2019, 37, 475–483. [Google Scholar] [CrossRef] [PubMed]
- Metzinger-Le Meuth, V.; Burtey, S.; Maitrias, P.; Massy, Z.A.; Metzinger, L. microRNAs in the pathophysiology of CKD-MBD: Biomarkers and innovative drugs. Biochim. Biophys. Acta Mol. Basis Dis. 2017, 1863, 337–345. [Google Scholar] [CrossRef]
- Neal, C.S.; Michael, M.Z.; Pimlott, L.K.; Yong, T.Y.; Li, J.Y.; Gleadle, J.M. Circulating microRNA expression is reduced in chronic kidney disease. Nephrol. Dial. Transpl. 2011, 26, 3794–3802. [Google Scholar] [CrossRef] [Green Version]
- Brigant, B.; Metzinger-Le Meuth, V.; Massy, Z.A.; McKay, N.; Liabeuf, S.; Pelletier, M.; Sallee, M.; M’Baya-Moutoula, E.; Paul, P.; Drueke, T.B.; et al. Serum microRNAs are altered in various stages of chronic kidney disease: A preliminary study. Clin. Kidney J. 2017, 10, 30–37. [Google Scholar] [CrossRef]
- Chen, N.X.; Kiattisunthorn, K.; O’Neill, K.D.; Chen, X.; Moorthi, R.N.; Gattone, V.H., 2nd; Allen, M.R.; Moe, S.M. Decreased microRNA is involved in the vascular remodeling abnormalities in chronic kidney disease (CKD). PLoS ONE 2013, 8, e64558. [Google Scholar] [CrossRef] [Green Version]
- Anastasilakis, A.D.; Makras, P.; Pikilidou, M.; Tournis, S.; Makris, K.; Bisbinas, I.; Tsave, O.; Yovos, J.G.; Yavropoulou, M.P. Changes of Circulating MicroRNAs in Response to Treatment With Teriparatide or Denosumab in Postmenopausal Osteoporosis. J. Clin. Endocrinol. Metab. 2018, 103, 1206–1213. [Google Scholar] [CrossRef]
- Yavropoulou, M.P.; Anastasilakis, A.D.; Makras, P.; Papatheodorou, A.; Rauner, M.; Hofbauer, L.C.; Tsourdi, E. Serum Profile of microRNAs Linked to Bone Metabolism During Sequential Treatment for Postmenopausal Osteoporosis. J. Clin. Endocrinol. Metab. 2020, 105, e2885–e2894. [Google Scholar] [CrossRef]
- Yavropoulou, M.P.; Anastasilakis, A.D.; Makras, P.; Tsalikakis, D.G.; Grammatiki, M.; Yovos, J.G. Expression of microRNAs that regulate bone turnover in the serum of postmenopausal women with low bone mass and vertebral fractures. Eur. J. Endocrinol. 2017, 176, 169–176. [Google Scholar] [CrossRef]
- Kanis, J.A. Assessment of fracture risk and its application to screening for postmenopausal osteoporosis: Synopsis of a WHO report. Osteoporos Int. 1994, 4, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Kanis, J.A.; Melton, L.J., 3rd; Christiansen, C.; Johnston, C.C.; Khaltaev, N. The diagnosis of osteoporosis. J. Bone Miner Res. 1994, 9, 1137–1141. [Google Scholar] [CrossRef] [PubMed]
- Kozomara, A.; Griffiths-Jones, S. miRBase: Annotating high confidence microRNAs using deep sequencing data. Nucleic Acids Res. 2014, 42, D68–D73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paraskevopoulou, M.D.; Georgakilas, G.; Kostoulas, N.; Vlachos, I.S.; Vergoulis, T.; Reczko, M.; Filippidis, C.; Dalamagas, T.; Hatzigeorgiou, A.G. DIANA-microT web server v5.0: Service integration into miRNA functional analysis workflows. Nucleic Acids Res. 2013, 41, W169–W173. [Google Scholar] [CrossRef] [Green Version]
- Reczko, M.; Maragkakis, M.; Alexiou, P.; Grosse, I.; Hatzigeorgiou, A.G. Functional microRNA targets in protein coding sequences. Bioinformatics 2012, 28, 771–776. [Google Scholar] [CrossRef]
- Wong, N.; Wang, X. miRDB: An online resource for microRNA target prediction and functional annotations. Nucleic Acids Res. 2015, 43, D146–D152. [Google Scholar] [CrossRef]
- Agarwal, V.; Bell, G.W.; Nam, J.W.; Bartel, D.P. Predicting effective microRNA target sites in mammalian mRNAs. Elife 2015, 4, 1–38. [Google Scholar] [CrossRef]
- Cho, S.; Jang, I.; Jun, Y.; Yoon, S.; Ko, M.; Kwon, Y.; Choi, I.; Chang, H.; Ryu, D.; Lee, B.; et al. MiRGator v3.0: A microRNA portal for deep sequencing, expression profiling and mRNA targeting. Nucleic Acids Res. 2013, 41, D252–D257. [Google Scholar] [CrossRef] [Green Version]
- Betel, D.; Koppal, A.; Agius, P.; Sander, C.; Leslie, C. Comprehensive modeling of microRNA targets predicts functional non-conserved and non-canonical sites. Genome Biol. 2010, 11, R90. [Google Scholar] [CrossRef] [Green Version]
- Sugatani, T.; Vacher, J.; Hruska, K.A. A microRNA expression signature of osteoclastogenesis. Blood 2011, 117, 3648–3657. [Google Scholar] [CrossRef]
- Wang, S.; Liu, Z.; Wang, J.; Ji, X.; Yao, Z.; Wang, X. miR21 promotes osteoclastogenesis through activation of PI3K/Akt signaling by targeting Pten in RAW264.7 cells. Mol. Med. Rep. 2020, 21, 1125–1132. [Google Scholar] [PubMed]
- Hu, C.H.; Sui, B.D.; Du, F.Y.; Shuai, Y.; Zheng, C.X.; Zhao, P.; Yu, X.R.; Jin, Y. miR-21 deficiency inhibits osteoclast function and prevents bone loss in mice. Sci. Rep. 2017, 7, 43191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hassan, M.Q.; Gordon, J.A.; Beloti, M.M.; Croce, C.M.; van Wijnen, A.J.; Stein, J.L.; Stein, G.S.; Lian, J.B. A network connecting Runx2, SATB2, and the miR-23a~27a~24-2 cluster regulates the osteoblast differentiation program. Proc. Natl. Acad. Sci. USA 2010, 107, 19879–19884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dai, Y.; Zheng, C.; Li, H. Inhibition of miR-23a-3p promotes osteoblast proliferation and differentiation. J. Cell Biochem. 2019, 29497, 1–12. [Google Scholar] [CrossRef]
- Zhao, W.; Wu, C.; Dong, Y.; Ma, Y.; Jin, Y.; Ji, Y. MicroRNA-24 Regulates Osteogenic Differentiation via Targeting T-Cell Factor-1. Int. J. Mol. Sci. 2015, 16, 11699–11712. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Fan, L.; Hu, J.; Zhang, L.; Liao, L.; Liu, S.; Wu, D.; Yang, P.; Shen, L.; Chen, J.; et al. MiR-26a Rescues Bone Regeneration Deficiency of Mesenchymal Stem Cells Derived From Osteoporotic Mice. Mol. Ther. 2015, 23, 1349–1357. [Google Scholar] [CrossRef] [Green Version]
- Kapinas, K.; Kessler, C.B.; Delany, A.M. miR-29 suppression of osteonectin in osteoblasts: Regulation during differentiation and by canonical Wnt signaling. J. Cell Biochem. 2009, 108, 216–224. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Kim, H.J.; Park, C.K.; Kim, Y.G.; Lee, H.J.; Kim, J.Y.; Kim, H.H. MicroRNA-124 regulates osteoclast differentiation. Bone 2013, 56, 383–389. [Google Scholar] [CrossRef]
- Li, H.; Xie, H.; Liu, W.; Hu, R.; Huang, B.; Tan, Y.F.; Xu, K.; Sheng, Z.F.; Zhou, H.D.; Wu, X.P.; et al. A novel microRNA targeting HDAC5 regulates osteoblast differentiation in mice and contributes to primary osteoporosis in humans. J. Clin. Invest. 2009, 119, 3666–3677. [Google Scholar] [CrossRef] [Green Version]
- Znorko, B.; Oksztulska-Kolanek, E.; Michalowska, M.; Kaminski, T.; Pawlak, K. Does the OPG/RANKL system contribute to the bone-vascular axis in chronic kidney disease? A systematic review. Adv. Med. Sci. 2017, 62, 52–64. [Google Scholar] [CrossRef]
- Walsh, M.C.; Choi, Y. Biology of the RANKL-RANK-OPG System in Immunity, Bone, and Beyond. Front. Immunol. 2014, 5, 511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gomez, I.G.; Nakagawa, N.; Duffield, J.S. MicroRNAs as novel therapeutic targets to treat kidney injury and fibrosis. Am. J. Physiol. Renal. Physiol. 2016, 310, F931–F944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zununi Vahed, S.; Omidi, Y.; Ardalan, M.; Samadi, N. Dysregulation of urinary miR-21 and miR-200b associated with interstitial fibrosis and tubular atrophy (IFTA) in renal transplant recipients. Clin. Biochem. 2017, 50, 32–39. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Zhang, X.; Si, F. MicroRNA-124 represents a novel diagnostic marker in human lupus nephritis and plays an inhibitory effect on the growth and inflammation of renal mesangial cells by targeting TRAF6. Int. J. Clin. Exp. Pathol. 2019, 12, 1578–1588. [Google Scholar] [PubMed]
- Eleftheriadis, T.; Kartsios, C.; Antoniadi, G.; Kazila, P.; Dimitriadou, M.; Sotiriadou, E.; Koltsida, M.; Golfinopoulos, S.; Liakopoulos, V.; Christopoulou-Apostolaki, M. The impact of chronic inflammation on bone turnover in hemodialysis patients. Ren. Fail 2008, 30, 431–437. [Google Scholar] [CrossRef] [PubMed]
- Kaminski, T.W.; Pawlak, K.; Karbowska, M.; Mysliwiec, M.; Pawlak, D. Indoxyl sulfate-the uremic toxin linking hemostatic system disturbances with the prevalence of cardiovascular disease in patients with chronic kidney disease. BMC Nephrol. 2017, 18, 35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fan, P.C.; Chen, C.C.; Peng, C.C.; Chang, C.H.; Yang, C.H.; Yang, C.; Chu, L.J.; Chen, Y.C.; Yang, C.W.; Chang, Y.S.; et al. A circulating miRNA signature for early diagnosis of acute kidney injury following acute myocardial infarction. J. Transl. Med. 2019, 17, 139. [Google Scholar] [CrossRef] [Green Version]
- Naylor, K.L.; Prior, J.; Garg, A.X.; Berger, C.; Langsetmo, L.; Adachi, J.D.; Goltzman, D.; Kovacs, C.S.; Josse, R.G.; Leslie, W.D. Trabecular Bone Score and Incident Fragility Fracture Risk in Adults with Reduced Kidney Function. Clin. J. Am. Soc. Nephrol. 2016, 11, 2032–2040. [Google Scholar] [CrossRef]
- Aleksova, J.; Kurniawan, S.; Elder, G.J. The trabecular bone score is associated with bone mineral density, markers of bone turnover and prevalent fracture in patients with end stage kidney disease. Osteoporos Int. 2018, 29, 1447–1455. [Google Scholar] [CrossRef]
- Yun, H.J.; Ryoo, S.R.; Kim, J.E.; Choi, Y.J.; Park, I.; Shin, G.T.; Kim, H.; Jeong, J.C. Trabecular bone score may indicate chronic kidney disease-mineral and bone disorder (CKD-MBD) phenotypes in hemodialysis patients: A prospective observational study. BMC Nephrol. 2020, 21, 299. [Google Scholar] [CrossRef]
- Yavropoulou, M.; Kolynou, A.; Makras, P.; Skoura, L.; Nanoudis, S.; Pikilidou, M.; Tsave, O.; Metallidis, S.; Chatzidimitriou, D. AEP131 Changes in the relative expression of circulating microRNAs linked to bone metabolism in HIV-infected Individuals with low bone mass. Endocr. Abstr. 2020, 70. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| MiScript Primer Assay | Gene Symbol | Predicted Target-Genes | MicroRNA Sequence | Predicted Mechanism of Action |
|---|---|---|---|---|
| MS00009079 | hsa-miRNA-21-5p | SPRY1; PDCD4; FASLG | 5′UAGCUUAUCAGACUGAUGUUGA | Increases osteoclastogenesis and is up-regulated during RANKL-induced osteoclastogenesis [30,31,32]. |
| MS00031633 | hsa-miRNA-23a-3p | RUNX2; SATB2 | 5′AUCACAUUGCCAGGGAUUUCC | Decreases osteoblastogenesis, through inhibition of RUNX2 translation [33,34]. |
| MS00009205 | hsa-miRNA-24-2-5p | TCF-1; CALB1; SATB2 | 5′UGCCUACUGAGCUGAAACACAG | Decreases osteogenic differentiation through targeting the expression of transcription factor TCF-1 in osteoblastic cells [35]. |
| MS00029239 | hsa-miRNA-26a-5p | ΤΟΒ1; IGF-1 | 5′UUCAAGUAAUCCAGGAUAGGCU | Increases bone formation through repressing TOB1 protein expression, negative regulator of BMP/Smad signaling pathway [36]. |
| MS00003262 | hsa-miRNA-29a-3p | SPARC | 5′UAGCACCAUCUGAAAUCGGUUA | Decreases osteonectin-bone matrix protein-synthesis [37]. |
| MS00006622 | hsa-miRNA-124-3p | NFATC1; NFATC2 | 5′UAAGGCACGCGGUGAAUGCC | Decreases osteoclastogenesis by suppressing NFATc1 [38]. |
| MS00042140 | hsa-miRNA-2861 | HDAC5 | 5′GGGGCCUGGCGGUGGGCGG | Increases osteoblastogenesis through repression of HDAC5 that degrades expression of the RUNX2 gene [39]. |
| MS00019789 | Cel-miRNA-39-3p | Spike in control | 5′UCACCGGGUGUAAAUCAGCUUG |
| Parameters | Patients with CKD on HD (Cases = 30) | Healthy Individuals (Controls, n = 30) | p-Value * |
|---|---|---|---|
| Age (years) | 58.3 ± 12.4 | 54.7 ± 5.5 | 0.256 |
| BMI (kg/m2) | 25.8 ± 3.9 | 25.5 ± 1.5 | 0.821 |
| Males, n (%) | 22 (73%) | 22 (73%) | 0.132 |
| Duration of Hemodialysis (years) | 5.9 ± 4.7 | NA | NA |
| Smoking, n (%) | 4 (13%) | 6 (20%) | 0.156 |
| LS T-score | −1.7 [(−3.7), (+1.7)] | 0.4 [(−1.9), (+0.7)] | 0.001 |
| LS-BMD (gr/cm2) | 0.967 ± 0.21 | 1.177 ± 0.13 | <0.001 |
| TBS | 1.144 ± 0.16 | 1.219 ± 0.15 | 0.004 |
| LFN T-score | −2.4± 1.1 | −0.87 ± 0.93 | <0.001 |
| LFN BMD (gr/cm2) | 0.740 ± 0.15 | 0.956 ± 0.12 | <0.001 |
| LH T-score | −2.2 ± 1.18 | −0.6 ± 0.81 | <0.001 |
| LH BMD (gr/cm2) | 0.775 ± 0.17 | 1.013 ± 0.11 | <0.001 |
| RFN T-score | −2.47 ± 1.15 | −1.0 ± 0.93 | <0.001 |
| RFN BMD (gr/cm2) | 0.729 ± 0.15 | 0.940 ± 0.12 | <0.001 |
| RH T-score | −2.2 ± 1.15 | −0.68 ± 0.78 | <0.001 |
| RH BMD (gr/cm2) | 0.770 ± 0.16 | 1.003 ± 0.11 | <0.001 |
| Radius T-score | −2.83 ± 2.25 | −0.38 ± 0.93 | <0.001 |
| Radius BMD (gr/cm2) | 0.366 ± 0.11 | 0.96 ± 0.09 | <0.001 |
| TBS | 1.242 ± 0.12 | 1.280 ± 0.12 | 0.098 |
| Serum Calcium # (NR: 8.2–10.6 mg/dl) | 8.8 ± 0.5 | 9.2 ± 0.2 | 0.004 |
| Serum Phosphate (NR: 2.7–4.5 mg/dl) | 4.5 ± 1.6 | 3.2 ± 0.4 | 0.002 |
| Intact PTH (NR: 1.58–6.03 pmol/l) | 32.25 (4.9, 101) | 5 (3.7, 6.0) | <0.001 |
| Serum 25-OH-Vitamin D (nmol/l) | 31.75 (10.0, 99.2) | 55.0 (22.2, 100) | 0.040 |
| Serum ALP (U/lt) | 122.0 (52, 386) | 71 (45, 117) | 0.0013 |
| Serum P1NP (ng/mL) | 53.8 ± 12.4 | 46.9 ± 11.9 | 0.040 |
| Serum β-CTX (ng/l) | 420 ± 120.2 | 330 ± 95.8 | 0.048 |
| Clinical/morphometric Vertebral Fractures | 0 | 0 | NA |
| Other Fractures | 0 | 0 | NA |
| MicroRNAs | Fold Regulation | 95% CI | p-Values |
|---|---|---|---|
| hsa-miRNA-21-5p | −14.7 | (−18.8, −3.9) | p = 0.034 |
| hsa-miRNA-23a-3p | −3.8 | (−8.7, −2.0) | p = 0.005 |
| hsa-miRNA-24-2-5p | 1.14 | (0.80, 2.11) | p = 0.23 |
| hsa-miRNA-26a-5p | 1.02 | (0.05, 4.12) | p = 0.32 |
| hsa-miRNA-29a-3p | 1.31 | (0.01, 2.76) | p = 0.36 |
| hsa-miRNA-124 | −5.9 | (0.97, 9.50) | p = 0.005 |
| hsa-miRNA-2861 | 1.0 | (0.02, 3.79) | p = 0.51 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yavropoulou, M.P.; Vaios, V.; Makras, P.; Georgianos, P.; Batas, A.; Tsalikakis, D.; Tzallas, A.; Ntritsos, G.; Roumeliotis, S.; Eleftheriadis, T.; et al. Expression of Circulating MicroRNAs Linked to Bone Metabolism in Chronic Kidney Disease-Mineral and Bone Disorder. Biomedicines 2020, 8, 601. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120601
Yavropoulou MP, Vaios V, Makras P, Georgianos P, Batas A, Tsalikakis D, Tzallas A, Ntritsos G, Roumeliotis S, Eleftheriadis T, et al. Expression of Circulating MicroRNAs Linked to Bone Metabolism in Chronic Kidney Disease-Mineral and Bone Disorder. Biomedicines. 2020; 8(12):601. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120601
Chicago/Turabian StyleYavropoulou, Maria P., Vasilios Vaios, Polyzois Makras, Panagiotis Georgianos, Anastasios Batas, Dimitrios Tsalikakis, Alexandros Tzallas, Georgios Ntritsos, Stefanos Roumeliotis, Theodoros Eleftheriadis, and et al. 2020. "Expression of Circulating MicroRNAs Linked to Bone Metabolism in Chronic Kidney Disease-Mineral and Bone Disorder" Biomedicines 8, no. 12: 601. https://0-doi-org.brum.beds.ac.uk/10.3390/biomedicines8120601