Changes in Coordination and Its Variability with an Increase in Functional Performance of the Lower Extremities

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
Participants
3. Gait Assessment
4. IMU-Derived Variables
5. Statistical Analysis
6. Results

{kind=link}
{kind=link}
{kind=link}
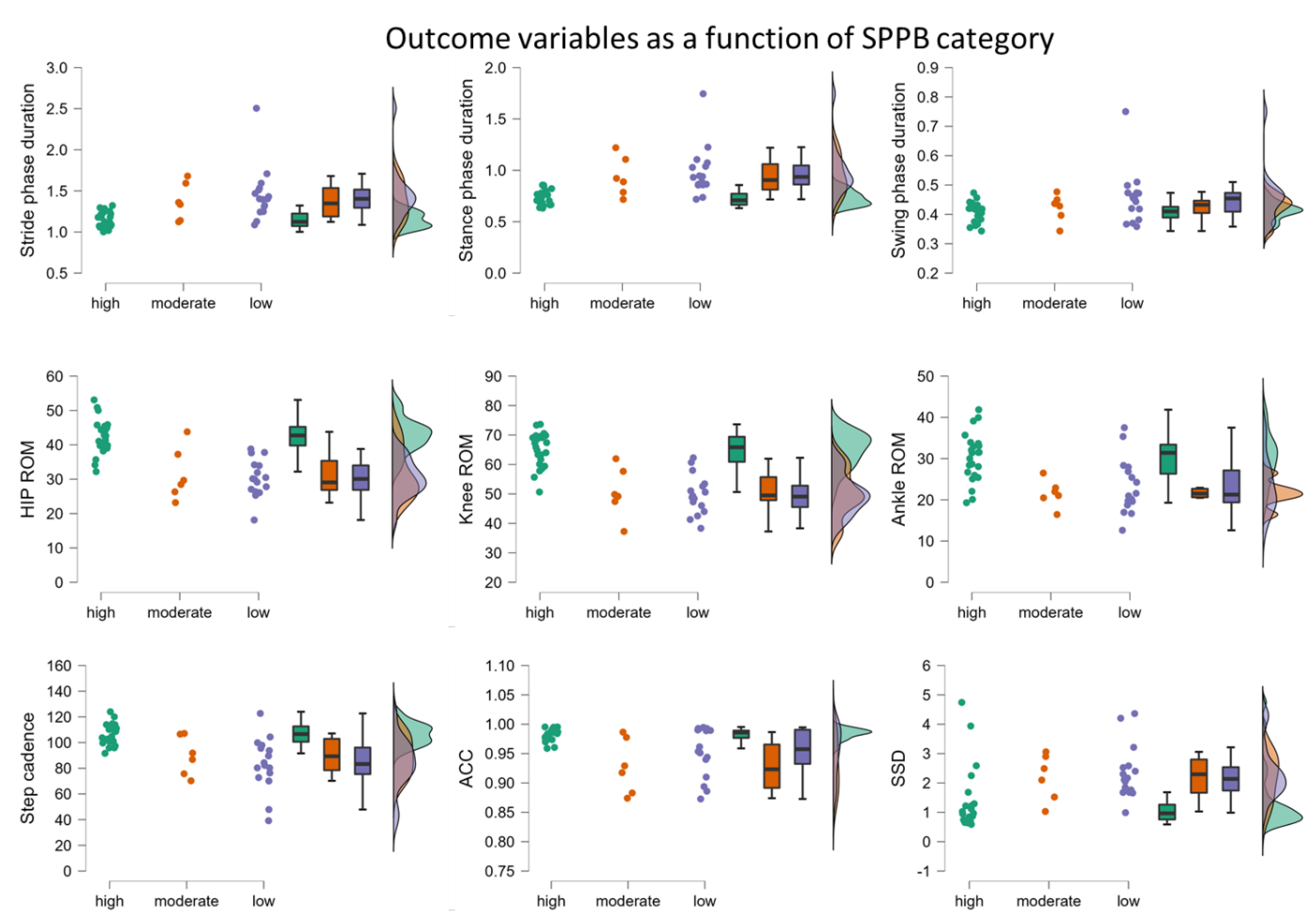
| IMU-Derived Parameter | Correlation with SPPB Total Score | Sub-Group Comparison | ||
|---|---|---|---|---|
| ρ | p | H(2) | p | |
| Stride duration | −0.690 | <0.001 * | 19.805 | <0.001 * |
| Stance duration | −0.754 | <0.001 * | 24.071 | <0.001 * |
| Swing duration | −0.362 | 0.015 | 5.761 | 0.056 |
| Hip ROM | 0.717 | <0.001 * | 25.918 | <0.001 * |
| Knee ROM | 0.741 | <0.001 * | 26.125 | <0.001 * |
| Ankle ROM | 0.537 | 0.001 * | 13.591 | <0.001 * |
| Cadence | 0.678 | <0.001 * | 17.506 | <0.001 * |
| SSD | −0.552 | <0.001 * | 14.057 | <0.001 * |
| ACC | 0.300 | 0.045 | 7.469 | 0.024 |
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Afilalo, J.; Lauck, S.; Kim, D.H.; Lefèvre, T.; Piazza, N.; Lachapelle, K.; Martucci, G.; Lamy, A.; Labinaz, M.; Peterson, M.D.; et al. Frailty in older adults undergoing aortic valve replacement: The FRAILTY-AVR study. J. Am. Coll. Cardiol. 2017, 70, 689–700. [Google Scholar] [CrossRef] [PubMed]
- Ashikaga, K.; Saji, M.; Takanashi, S.; Nagayama, M.; Akashi, Y.J.; Isobe, M. Physical performance as a predictor of midterm outcome after mitral valve surgery. Heart Vessel. 2019, 34, 1665–1673. [Google Scholar] [CrossRef] [PubMed]
- Awai, L.; Curt, A. Intralimb coordination as a sensitive indicator of motor-control impairment after spinal cord injury. Front. Hum. Neurosci. 2014, 8, 148. [Google Scholar] [CrossRef] [PubMed]
- Bellettiere, J.; Lamonte, M.J.; Unkart, J.; Liles, S.; Laddu-Patel, D.; Manson, J.E.; Banack, H.; Seguin-Fowler, R.; Chavez, P.; Tinker, L.F.; et al. Short Physical Performance Battery and Incident Cardiovascular Events Among Older Women. JAHA 2020, 9, e016845. [Google Scholar] [CrossRef]
- Bergland, A.; Strand, B.H. Norwegian reference values for the Short Physical Performance Battery (SPPB): The Tromsø Study. BMC Geriatr. 2019, 19, 216. [Google Scholar] [CrossRef] [Green Version]
- Berner, K.; Cockcroft, J.; Louw, Q. Kinematics and temporospatial parameters during gait from inertial motion capture in adults with and without HIV: A validity and reliability study. BioMed. Eng. OnLine 2020, 19, 57. [Google Scholar] [CrossRef]
- Berner, K.; Cockcroft, J.; Morris, L.D.; Louw, Q. Concurrent validity and within-session reliability of gait kinematics measured using an inertial motion capture system with repeated calibration. J. Bodyw. Mov. Ther. 2020, 24, 251–260. [Google Scholar] [CrossRef]
- Bernstein, N. The Coordination and Regulation of Movements; Pergamon Press: London, UK, 1967. [Google Scholar]
- Cirstea, M.C.; Mitnitski, A.B.; Feldman, A.G.; Levin, M.F. Interjoint coordination dynamics during reaching in stroke. Exp. Brain Res. 2003, 151, 289–300. [Google Scholar] [CrossRef]
- Crawley, M.J. Statistics: An Introduction Using R., 1st ed.; Wiley: Hoboken, NJ, USA, 2005. [Google Scholar] [CrossRef]
- Del Din, S.; Elshehabi, M.; Galna, B.; Hobert, M.A.; Warmerdam, E.; Suenkel, U.; Brockmann, K.; Metzger, F.; Hansen, C.; Berg, D.; et al. Gait analysis with wearables predicts conversion to parkinson disease. Ann. Neurol. 2019, 86, 357–367. [Google Scholar] [CrossRef]
- Desai, G.A.; Gruber, A.H. Segment coordination and variability among prospectively injured and uninjured runners. J. Sport. Sci. 2021, 39, 38–47. [Google Scholar] [CrossRef]
- Dewolf, A.H.; Mesquita, R.M.; Willems, P.A. Intra-limb and muscular coordination during walking on slopes. Eur. J. Appl. Physiol. 2020, 120, 1841–1854. [Google Scholar] [CrossRef] [PubMed]
- Field-Fote, E.C.; Tepavac, D. Improved intralimb coordination in people with incomplete spinal cord injury following training with body weight support and electrical stimulation. Phys. Ther. 2002, 82, 707–715. [Google Scholar] [CrossRef] [PubMed]
- Geritz, J.; Maetzold, S.; Steffen, M.; Pilotto, A.; Corrà, M.F.; Moscovich, M.; Rizzetti, M.C.; Borroni, B.; Padovani, A.; Alpes, A.; et al. Motor, cognitive and mobility deficits in 1000 geriatric patients: Protocol of a quantitative observational study before and after routine clinical geriatric treatment—The ComOn-study. BMC Geriatr. 2020, 20, 45. [Google Scholar] [CrossRef] [PubMed]
- Ghahramani, M.; Mason, B.; Pearsall, P.; Spratford, W. An Analysis of Lower Limb Coordination Variability in Unilateral Tasks in Healthy Adults: A Possible Prognostic Tool. Front. Bioeng. Biotechnol. 2022, 10, 885329. [Google Scholar] [CrossRef]
- Gommans, L.N.M.; Smid, A.T.; Scheltinga, M.R.M.; Cancrinus, E.; Brooijmans, F.A.M.; Meijer, K.; Teijink, J.A. Prolonged stance phase during walking in intermittent claudication. J. Vasc. Surg. 2017, 66, 515–522. [Google Scholar] [CrossRef]
- Hafer, J.F.; Peacock, J.; Zernicke, R.F.; Agresta, C.E. Segment Coordination Variability Differs by Years of Running Experience. Med. Sci. Sport. Exerc. 2019, 51, 1438–1443. [Google Scholar] [CrossRef]
- Hafer, J.F.; Silvernail, J.F.; Hillstrom, H.J.; Boyer, K.A. Changes in coordination and its variability with an increase in running cadence. J. Sport. Sci. 2016, 34, 1388–1395. [Google Scholar] [CrossRef]
- Hamill, J.; Palmer, C.; Van Emmerik, R.E.A. Coordinative variability and overuse injury. Sport. Med. Arthrosc. Rehabil. Ther. Technol. 2012, 4, 45. [Google Scholar] [CrossRef] [Green Version]
- Hollands, K.L.; van Vliet, P.; Zietz, D.; Wing, A.; Wright, C.; Hollands, M.A. Stroke-related differences in axial body segment coordination during preplanned and reactive changes in walking direction. Exp. Brain Res. 2010, 202, 591–604. [Google Scholar] [CrossRef]
- Ihlen, E.A.F. Age-related changes in inter-joint coordination during walking. J. Appl. Physiol. 2014, 117, 189–198. [Google Scholar] [CrossRef] [Green Version]
- Kwon, S.; Perera, S.; Pahor, M.; Katula, J.A.; King, A.C.; Groessl, E.J.; Studenski, S.A. What is a meaningful change in physical performance? Findings from a clinical trial in older adults (the LIFE-P study). J. Nutr. Health Aging 2009, 13, 538–544. [Google Scholar] [CrossRef] [PubMed]
- Latash, M.L. Progress in Motor Control; Latash Human Kinetics: Harrogate, UK, 1998. [Google Scholar]
- Lauretani, F.; Ticinesi, A.; Gionti, L.; Prati, B.; Nouvenne, A.; Tana, C.; Meschi, T.; Maggio, M. Short-Physical Performance Battery (SPPB) score is associated with falls in older outpatients. Aging Clin. Exp. Res. 2019, 31, 1435–1442. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-C.; Wagenaar, R.C. The impact of walking speed on interlimb coordination in individuals with Parkinson’s disease. J. Phys. Ther. Sci. 2018, 30, 658–662. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Longworth, J.A.; Chlosta, S.; Foucher, K.C. Inter-joint coordination of kinematics and kinetics before and after total hip arthroplasty compared to asymptomatic subjects. J. Biomech. 2018, 72, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.E.; Cantwell, C.; Vowels, L.; Dodd, K. Changes in gait and fatigue from morning to afternoon in people with multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2002, 72, 361–365. [Google Scholar] [CrossRef] [Green Version]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Nez, A.; Fradet, L.; Marin, F.; Monnet, T.; Lacouture, P. Identification of noise covariance matrices to improve orientation estimation by kalman filter. Sensors 2018, 18, 3490. [Google Scholar] [CrossRef] [Green Version]
- Nikolaus, T. Gang, gleichgewicht und stürze—Ursachen und konsequenzen. Dtsch. Med. Wochenschr. 2005, 130, 958–960. [Google Scholar] [CrossRef] [Green Version]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Phan, G.-H.; Hansen, C.; Tommasino, P.; Hussain, A.; Formica, D.; Campolo, D. A complementary filter design on se(3) to identify micro-motions during 3d motion tracking. Sensors 2020, 20, 5864. [Google Scholar] [CrossRef]
- Ramírez-Vélez, R.; Pérez-Sousa, M.A.; Venegas-Sanabria, L.C.; Cano-Gutierrez, C.A.; Hernández-Quiñonez, P.A.; Rincón-Pabón, D.; García-Hermoso, A.; Zambom-Ferraresi, F.; de Asteasu, M.S.; Izquierdo, M. Normative Values for the Short Physical Performance Battery (SPPB) and Their Association With Anthropometric Variables in Older Colombian Adults. The SABE Study, 2015. Front. Med. 2020, 7, 52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rizun, P.R. On the Estimation of Angular Orientation with Microelectromechanical Systems. Unpublished. Ph.D. Thesis, University of Calgary, Calgary, AB, Canada, 2010. [Google Scholar] [CrossRef]
- Sathananthan, J.; Lauck, S.; Piazza, N.; Martucci, G.; Kim, D.H.; Popma, J.J.; Asgar, A.W.; Perrault, L.P.; Lefèvre, T.; Labinaz, M.; et al. Habitual Physical Activity in Older Adults Undergoing TAVR: Insights From the FRAILTY-AVR Study. JACC Cardiovasc. Interv. 2019, 12, 781–789. [Google Scholar] [CrossRef] [PubMed]
- Schniepp, R.; Möhwald, K.; Wuehr, M. Clinical and automated gait analysis in patients with vestibular, cerebellar, and functional gait disorders: Perspectives and limitations. J. Neurol. 2019, 266, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Vasunilashorn, S.; Coppin, A.K.; Patel, K.V.; Lauretani, F.; Ferrucci, L.; Bandinelli, S.; Guralnik, J.M. Use of the Short Physical Performance Battery Score to predict loss of ability to walk 400 meters: Analysis from the InCHIANTI study. J. Gerontology. Ser. A Biol. Sci. Med. Sci. 2009, 64, 223–229. [Google Scholar] [CrossRef]
- Veronese, N.; Bolzetta, F.; Toffanello, E.D.; Zambon, S.; De Rui, M.; Perissinotto, E.; Coin, A.; Corti, M.-C.; Baggio, G.; Crepaldi, G.; et al. Association between Short Physical Performance Battery and falls in older people: The Progetto Veneto Anziani Study. Rejuvenation Res. 2014, 17, 276–284. [Google Scholar] [CrossRef] [Green Version]
- Volpato, S.; Cavalieri, M.; Sioulis, F.; Guerra, G.; Maraldi, C.; Zuliani, G.; Fellin, R.; Guralnik, J.M. Predictive value of the short physical performance battery following hospitalization in older patients. J. Gerontol. A Biol. Sci. Med. Sci. 2011, 66, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Wennie Huang, W.N.; Perera, S.; Vanswearingen, J.; Studenski, S. Performance Measures Predict Onset of Activity of Daily Living Difficulty in Community-Dwelling Older Adults. J. Am. Geriatr. Soc. 2010, 58, 844–852. [Google Scholar] [CrossRef] [Green Version]
- Williams, D.S.; Martin, A.E. Gait modification when decreasing double support percentage. J. Biomech. 2019, 92, 76–83. [Google Scholar] [CrossRef]
- Yi, L.C.; Sartor, C.D.; Souza, F.T.; Sacco IC, N. Intralimb Coordination Patterns in Absent, Mild, and Severe Stages of Diabetic Neuropathy: Looking Beyond Kinematic Analysis of Gait Cycle. PLoS ONE 2016, 11, e0147300. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hansen, C.; Chebil, B.; Cockroft, J.; Bianchini, E.; Romijnders, R.; Maetzler, W. Changes in Coordination and Its Variability with an Increase in Functional Performance of the Lower Extremities. Biosensors 2023, 13, 156. https://0-doi-org.brum.beds.ac.uk/10.3390/bios13020156
Hansen C, Chebil B, Cockroft J, Bianchini E, Romijnders R, Maetzler W. Changes in Coordination and Its Variability with an Increase in Functional Performance of the Lower Extremities. Biosensors. 2023; 13(2):156. https://0-doi-org.brum.beds.ac.uk/10.3390/bios13020156
Chicago/Turabian StyleHansen, Clint, Baraah Chebil, John Cockroft, Edoardo Bianchini, Robbin Romijnders, and Walter Maetzler. 2023. "Changes in Coordination and Its Variability with an Increase in Functional Performance of the Lower Extremities" Biosensors 13, no. 2: 156. https://0-doi-org.brum.beds.ac.uk/10.3390/bios13020156