1. Introduction
Adverse childhood experiences (ACEs) are potentially traumatic events that can have negative, lasting effects on health and well-being [
1]. ACEs range from physical, emotional, or sexual abuse and neglect to the incarceration of a parent or parental divorce [
1]. There is evidence indicating ACEs as a risk for the development of BD and of worse outcomes for bipolar disorder (BD) [
2]. A study conducted two decades ago reported a higher number of ACEs in patients with BD than in normal controls [
3]. Furthermore, adverse experiences, including childhood abuse and neglect, have been reported in more than half of the patients with BD [
4]. Subsequent studies have also indicated a relationship between ACEs and BD [
2]. Additionally, there is a reported association between ACEs and the clinical outcomes of BD, including early age at onset (AAO), psychotic features, rapid cycling, a higher mood episode number, and suicidality [
4,
5,
6,
7].
However, the validity of these findings is uncertain considering the limitations of the aforementioned studies [
8]. For example, more than 40% of the studies did not use structured clinical interviews for BD diagnosis; furthermore, they did not use scales for ACEs evaluation, including the Childhood Trauma Questionnaires (CTQ) and Childhood Life Events Scale (CLES) [
3,
9]. These aforementioned limitations contribute to the inconsistent results and their reduced reliability. Furthermore, there are scarce large-scale studies on the ACE types affecting the clinical outcomes, the effect of post-childhood abuse or adverse experiences on clinical outcomes, and the influence of the number of ACEs on clinical outcomes. We hypothesized that specific ACEs type or multiple ACEs interact with the vulnerability to BD, and that this interaction would induce earlier AAO and worse clinical outcomes of BD. We also hypothesized that post-childhood adverse experiences had a weaker effect on clinical outcomes than ACEs did.
The aim of this study was to clarify the relationship between ACEs and the clinical outcomes of BD. Thus, we investigated the effects of various ACEs, including the number, type, and timing, on the clinical outcomes of BD.
4. Discussion
We aimed to clarify the relationship between ACEs and the clinical outcomes of BD. Moreover, we analyzed the effects of various ACE factors, including the number, type, and timing, on the clinical outcomes of BD.
We found that 63.1% of the patients had a history of exposure to at least one ACE. A previous review reported that 67% of patients with BD across 16 studies had a history of exposure to at least one ACE [
13], which is consistent with our findings; however, the prevalence ranged from 5.3% to 76.5%. This significant discrepancy could be attributed to methodological limitations in some of the studies, including small sample sizes, as well as a lack of the use of scales for ACE evaluation and of structured clinical interviews for BD diagnosis [
8]. In addition, the female group reported greater frequencies of ACEs than the male group. Moreover, the female group with ACEs revealed stronger associations with suicidality than the male group.
Moreover, we observed that several ACE types, including family loss, chronic illness, lengthy hospitalization, permanent injury or disability, adverse life changes, and PA, have robust negative effect on clinical outcomes, including AAO, psychotic episodes, chronicity, suicide attempts, mixed symptoms or episodes, comorbidity of substance misuse, and life functioning.
Furthermore, we observed a significant positive correlation between the number of ACEs and the severity of clinical manifestations (
Table 4 and
Table 5). A previous study reported a more significant effect of abuse than that of neglect [
6]. Contrastingly, we found a positive correlation between the number of ACEs and the severity of the clinical outcomes of BD, which is consistent with a previous study (
Table 4 and
Table 5) [
4]. This indicates that the number and severity of ACEs influence the clinical outcomes of BD. Our results are consistent with those of previous reports of serious clinical outcomes in patients with BD exposed to ACEs; however, the variables with a significant effect on the clinical features, course, and comorbidities have varied across studies [
4,
6,
14,
15,
16,
17,
18,
19,
20].
We found an association between exposure to ACEs and early AAO. Specifically, there was a positive correlation of the number of ACEs and specific ACEs, including PA, with early AAO. This suggests that persistent hypothalamic-pituitary-adrenal axis over-activation leads to an elevated risk for BD during adolescence or adulthood [
21]. Another suggestion could be that ACEs affects the BD onset by interrupting brain network maturation [
22], impairing the limbic-cortical circuits (e.g., the volume reduction of the hippocampus and amygdala) [
23,
24], and interacting with genetic or epigenetic factors [
25].
Regarding psychotic features, 69.4% of our patients had experienced at least one psychotic episode during their lifetime. Interestingly, there was a high odds ratio for patients with more than one ACE to have a history of psychotic episodes compared to patients without a history of ACEs (
Table 5). Furthermore, 99.8% of patients with an experience of more than two ACEs had at least one psychotic episode; contrastingly, the concomitant prevalence in patients with no ACE history was approximately 50% (
Table 4). Therefore, psychotic symptoms were more easily affected by the presence and number of ACEs compared with other clinical outcomes. Psychotic symptoms could be associated with dopaminergic abnormalities induced by HPA axis over-activation [
13]. Previous studies have also reported a significant association of psychotic features in patients with BD with exposure to ACEs [
15,
26]. Contrastingly, other previous studies reported that exposure to ACEs only elevated psychotic symptom occurrence regardless of the psychiatric diagnosis [
5,
14,
20]. Therefore, it remains unclear whether ACEs influences psychotic episode occurrence or psychotic symptoms regardless of the psychiatric diagnosis in patients with BD.
Similarly, we observed a positive correlation between the number of suicide attempts and the number of ACEs. In addition to exposure to ACEs, being female was associated with an increased number of suicide attempts. This could be attributed to the number of ACEs being higher among females. However, a meta-analysis on patients with BD by Schaffer et al. reported an association of being female with suicide attempts and of being male with suicide completion [
27]. Furthermore, being younger had an effect on suicide attempts; however, the odds ratio was only 0.99. However, after adjusting for sex and age, the association of ACEs with suicide attempts remained. Therefore, ACEs, as well as being female and younger, could have an additive effect on suicide attempts in patients with BD, which is similar to the findings of the report by Etain et al [
6].
Additionally, there was an association of mixed symptoms or episodes with ACEs. However, after adjustment for age, sex, AAO, and PA, unlike for other clinical outcomes, there was no relationship between the number of ACEs and mixed symptoms (
Table 8). However, the presence of PA and earlier AAO had an effect on the presence of mixed symptoms/episodes. Therefore, considering the constant odds ratio despite the increased number of ACEs, it is possible that mixed symptoms/episodes are affected by specific ACEs rather than the number of ACEs (
Table 5 and
Table 6).
Moreover, there was a positive association between substance misuse and ACEs, which remained even after adjustment for sex and age. In addition to ACEs, being male was associated with an increased frequency of substance abuse or dependence. Therefore, ACEs, as well as being male, had an effect on substance misuse in patients with BD. Furthermore, there was a positive correlation between the number of ACEs and substance misuse.
There was a significant relationship between ACEs and life functioning; furthermore, patients with more than two ACEs had worse life functioning. In addition to ACEs, being male was associated with worse life functioning. This suggests that ACEs could contribute to worse social and cognitive function, which is consistent with previous findings [
19].
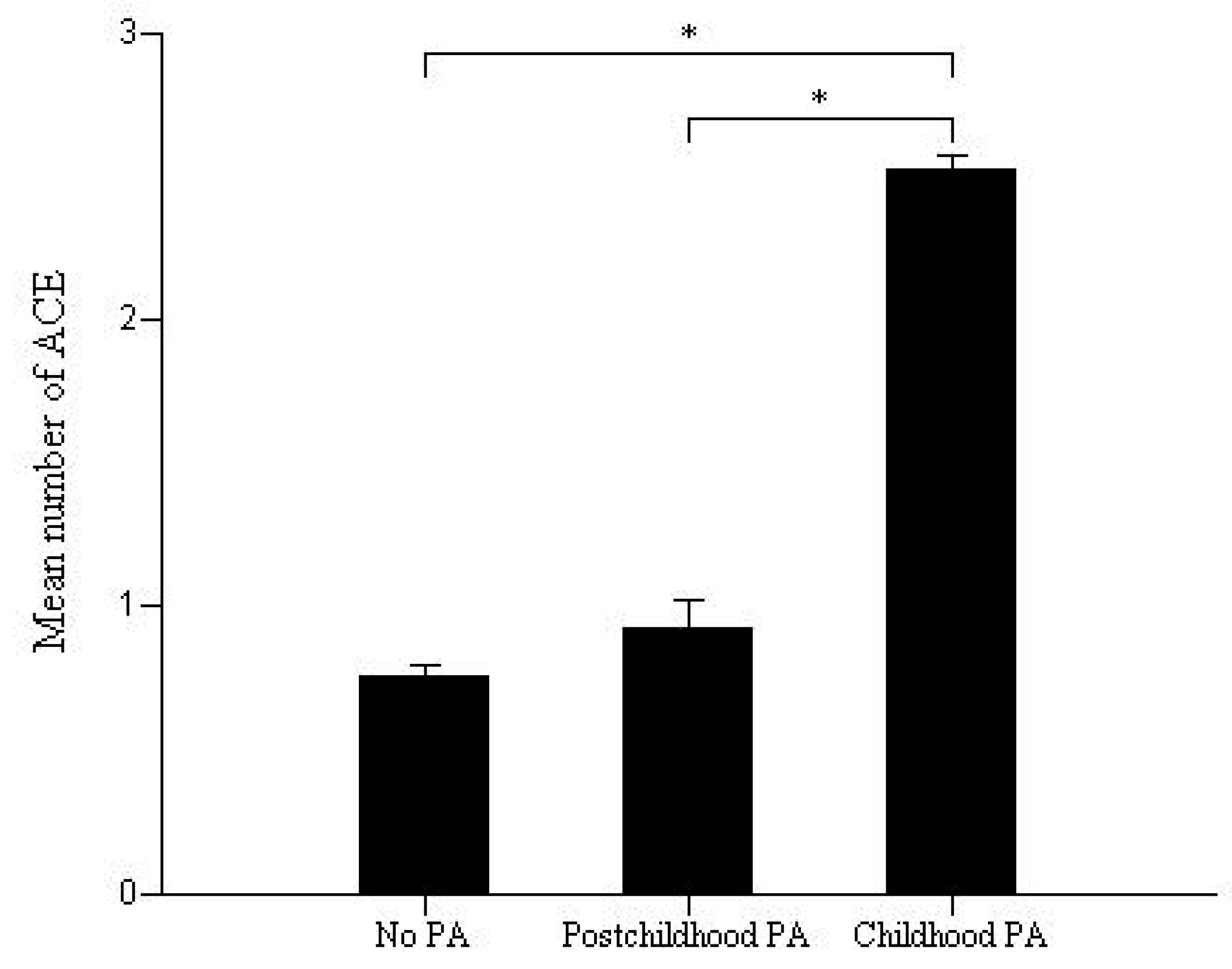
Various types of ACEs, including PA, had an effect on clinical outcomes in patients with BD. However, PA (item 6) and death or injury threat (item 7) were the most potent factors among all types of ACEs since they affected all clinical outcomes (
Table 6). However, multiple regression analysis revealed that the number of ACEs, rather than a specific ACE, such as PA, could be a more potent factor influencing clinical outcomes in patients with BD. However, PA does not represent a single ACE; rather, it represents a complex collective of ACEs since the group with childhood PA had more ACEs than the groups with post-childhood PA or without PA did (
Figure 1). Therefore, future studies should assess whether a specific ACE or the number of ACEs had the most significant effect on clinical outcomes.
This study has several limitations. First, we retrospectively obtained data regarding ACEs using CLES. Studies have used varying ACEs evaluation techniques, such as chart reviews, clinical interviews, CTQ, and CLES, which has resulted in heterogeneity in the definition and measurement of childhood trauma [
8]. For example, CLES focuses on a diverse range of ACEs, such as the loss of parents and siblings, illness, hospitalization, permanent injuries, and PA. Contrastingly, the CTQ reflects a more specific trauma type with the main focus on abuse or neglect. However, despite the methodological differences, a majority of previous studies reported similar results, including earlier AAO and more severe clinical outcomes of BD in patients exposed to ACEs, with recent studies (including the present one) reporting consistent findings. Second, CLES has not been validated to date. In addition, nine adversities are measured and the sum of the number of adversities was presented as a score. Third, the current study included a much larger female sample than male sample. However, gender was included as a covariate in the analyses. Future studies should investigate the frequency and vulnerability to ACEs according to gender differences. Forth, the post-childhood adversities have occurred after the onset of bipolar disorder in some subjects. Lastly, this study was designed without considering a selection bias. Thus, future studies need to be performed with careful consideration of selection bias. Despite these limitations, our study has several strengths, including a large sample size and thorough assessments of the data of patients with BD obtained using structured questionnaires.
In conclusion, we found an association of ACEs with a robust negative effect on clinical outcomes, including AAO, psychotic episodes, suicide attempts, mixed symptoms or episodes, comorbidity of substance misuse, and worse life functioning. These findings indicate the clinical importance for studies on BD to evaluate ACEs. Future prospective case-control studies should attempt to confirm these relationships.




{kind=link}