Impact of Aquatic Exercise on Respiratory Outcomes and Functional Activities in Children with Neuromuscular Disorders: Findings from an Open-Label and Prospective Preliminary Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
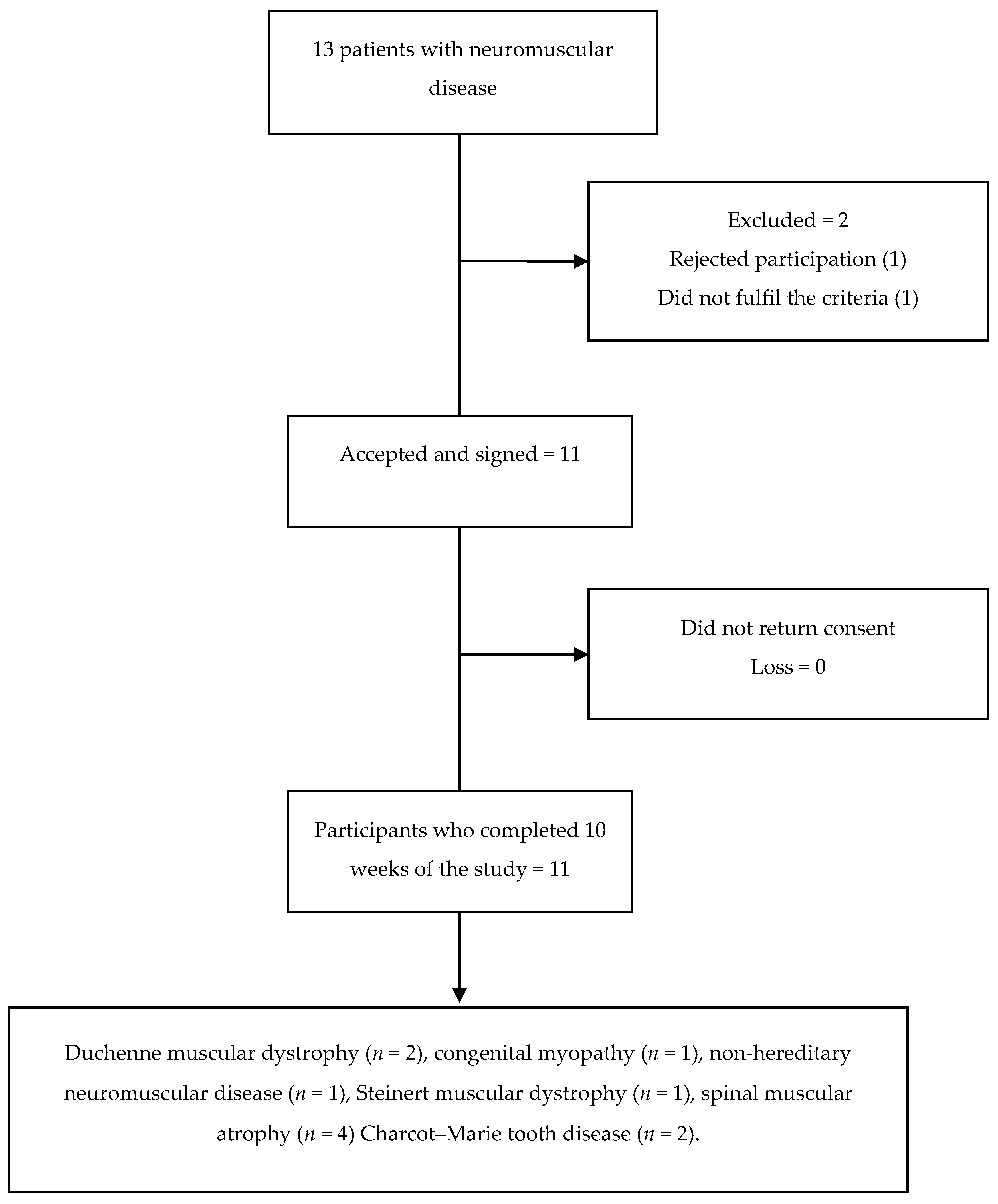
2.1. Participants
2.2. Data Collection
Outcome Measures
2.3. Procedure
2.4. Statistical Analysis
2.5. Ethical Considerations
3. Results
Descriptive Characteristics of the Sample
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dowling, J.J.; Gonorazky, H.D.; Cohn, R.D.; Campbell, C. Treating pediatric neuromuscular disorders: The future is now. Am. J. Med. Genet. 2018, 176, 804–841. [Google Scholar] [CrossRef] [Green Version]
- Gilbreath, H.R. Common neuromuscular disorders in Pediatrics. Physician Assist. Clin. 2016, 1, 583–597. [Google Scholar] [CrossRef]
- Kaplan, J.C.; Hamroun, D. The 2015 version of the gene table of monogenic neuromuscular disorders (nuclear genome). Neuromuscul. Disord. 2014, 24, 1123–1153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bushby, K.; Finkel, R.; Birnkrant, D.J.; Case, L.E.; Clemens, P.R.; Cripe, L.; Kaul, A.; Kinnett, K.; McDonald, C.; Pandya, S.; et al. DMD care considerations working group. Diagnosis and management of Duchenne muscular dystrophy, part 1: Diagnosis, and pharmacological and psychosocial management. Lancet Neurol. 2010, 9, 77–93. [Google Scholar] [PubMed]
- Bushby, K.; Finkel, R.; Birnkrant, D.J.; Case, L.E.; Clemens, P.R.; Cripe, L.; Kaul, A.; Kinnett, K.; McDonald, C.; Pandya, S.; et al. DMD care considerations working group. Diagnosis and management of Duchenne muscular dystrophy, part 2: Implementation of multidisciplinary care. Lancet Neurol. 2010, 9, 177–189. [Google Scholar]
- Pareyson, D.; Marchesi, C. Diagnosis, natural history, and management of Charcot-Marie-Tooth disease. Lancet Neurol. 2009, 8, 654–667. [Google Scholar] [CrossRef]
- Martini, J.; Hukuda, M.E.; Caromano, F.A.; Favero, F.M.; Fu, C.; Voos, M.C. The clinical relevance of timed motor performance in children with Duchenne muscular dystrophy. Physiother. Theory Pract. 2015, 31, 1–9. [Google Scholar] [CrossRef]
- Artilheiro, M.C.; Sá, C.; Favero, F.M.; Caromano, F.A.; Voos, M.C. Patients with Duchenne and Becker muscular dystrophies are not more asymmetrical than healthy controls on timed performance of upper limb tasks. Braz. J. Med. Biol. Res. 2017, 50, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Voos, M.C.; Albuquerque-Goya, P.S.; Leal de-Freitas, B.; Teixeira-Pires, A.M.; Meire-Favero, F.; Aparecida-Caromano, F. Timed immersion expiration measures in patients with muscular dystrophies. Arch. Physiother. 2020, 10, 4. [Google Scholar] [CrossRef] [Green Version]
- Lo Mauro, A.; Aliverti, A. Physiology of respiratory disturbances in muscular dystrophies. Breathe (Sheff) 2016, 12, 318–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buu, M.C. Respiratory complications, management and treatments for neuromuscular disease in children. Curr. Opin. Pediatr. 2017, 29, 326–333. [Google Scholar] [CrossRef] [PubMed]
- Gayraud, J.; Ramonatxo, M.; Rivier, F.; Humberclaude, V.; Petrof, B.; Matecki, S. Ventilatory parameters and maximal respiratory pressure changes with age in Duchenne muscular dystrophy patients. Pediatr. Pulmonol. 2010, 45, 552–559. [Google Scholar] [CrossRef] [PubMed]
- Takken, T.; Groen, W.G.; Hulzebos, E.H.; Ernsting, C.G.; van Hasselt, P.M.; Prinsen, B.H.; Helders, P.J.; Visser, G. Exercise Stress Testing in Children with Metabolic or Neuromuscular Disorders. Int. J. Pediatr. 2010. [Google Scholar] [CrossRef] [Green Version]
- Morse, C.I.; Bostock, E.L.; Twiss, H.M.; Kapp, L.H.; Orme, P.; Jacques, M.F. The cardiorespiratory response and physiological determinants of the assisted 6-minute handbike cycle test in adult males with muscular dystrophy. Muscle Nerve 2018, 58, 427–433. [Google Scholar] [CrossRef] [Green Version]
- Kamen, G.; Knight, C.A. Training-related adaptations in motor unit discharge rate in young and older adults. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 59, 1334–1338. [Google Scholar] [CrossRef] [Green Version]
- Siddique, U.; Rahman, S.; Frazer, A.K.; Pearce, A.J.; Howatson, G.; Kidgel, D.J. Determining the Sites of Neural Adaptations to Resistance Training: A Systematic Review and Meta-analysis. Sports. Med. 2020, 50, 1107–1128. [Google Scholar] [CrossRef]
- Quinn, L.; Morgan, D. From Disease to Health: Physical Therapy Health Promotion Practices for Secondary Prevention in Adult and Pediatric Neurologic Populations. J. Neurol. Phys. Ther. 2017, 41, 46–54. [Google Scholar] [CrossRef]
- Becker, B.E. Aquatic therapy: Scientific foundations and clinical rehabilitation applications. Am. Acad. Phys. Med. Rehab. 2009, 1, 859–872. [Google Scholar] [CrossRef] [PubMed]
- Roostaei, M.; Baharlouei, H.; Azadi, H.; Fragala-Pinkham, M.A. Effects of Aquatic Intervention on Gross Motor Skills in Children with Cerebral Palsy: A Systematic Review. Phys. Occup. Ther. Pediatr. 2017, 37, 496–515. [Google Scholar] [CrossRef]
- Salem, Y.; Gropack, S.J. Aquatic Therapy for a Child with Type III Spinal Muscular Atrophy: A Case Report. Phys. Occup. Ther. Pediatr. 2010, 30, 313–324. [Google Scholar] [CrossRef]
- Cuhna, M.B.; Oliviera, A.S.B.; Labrocini, R.H.D.D.; Gabbai, A.A. Spinar muscular atrophy Type III (intermediary) and III (Kugelberg-Welander): Evolution of 50 patients with physiotherapy and hydrotherapy in a swimming pool. Arq. Neuropsiquiatr. 1996, 54, 402–406. [Google Scholar]
- Figuers, C. Aquatic therapy intervention for a child diagnosed with spinal muscular atrophy. Phys. Ther. Case. Rep. 1999, 2, 109–112. [Google Scholar]
- Hind, D.; Parkin, J.; Whitwoth, V.; Rex, S.; Young, T.; Hampson, L.; Sheehan, J.; Maguire, C.; Cantrill, H.; Scott, E.; et al. Aquatic therapy for boys with Duchenne muscular dystrophy (DMD): An external pilot randomized controlled trial. Pilot. Feasibility Stud. 2017, 3, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Finder, J.D.; Birnkrant, D.; Carl, J.; Farber, H.J.; Gozal, D.; Iannaccone, S.T.; Kovesi, T.; Kravitz, R.M.; Panitch, H.; Schramm, C.; et al. Respiratory care of the patient with Duchenne muscular dystrophy: ATS consensus statement. Am. J. Respir. Crit. Care Med. 2004, 70, 456–465. [Google Scholar]
- Chatwin, M.; Toussaint, M.; Gonçalves, M.R.; Sheers, N.; Mellies, U.; Gonzales-Bermejo, J.; Sancho, J.; Fauroux, B.; Andersen, T.; Hov, B.; et al. Airway clearance techniques in neuromuscular disorders: A state of the art review. Respir. Med. 2018, 136, 98–110. [Google Scholar] [CrossRef] [Green Version]
- Dohna-Schawke, C.; Ragette, R.; Teschler, H.; Voit, T.; Mellies, U. Predictors of severe chest infections in pediatric neuromuscular disorders. Neuromuscul. Disord. 2006, 16, 325–328. [Google Scholar] [CrossRef]
- Chiang, J.; Mehta, K.K.; Amin, R. Respiratory Diagnostic Tools in Neuromuscular Disease. Children (Basel) 2018, 5, 78. [Google Scholar] [CrossRef] [Green Version]
- Represas-Represas, C.; Botana-Rial, M.; Leiro-Fernández, V.; González-Silva, A.I.; Del Campo-Pérez, V.; Fernández-Villa, A. Assessment of the Portable COPD-6 Device for Detecting Obstructive Airway Diseases. Arch. Bronchoneumol. 2010, 46, 426–432. [Google Scholar] [CrossRef]
- Faroux, B.; Quijano-Roy, S.; Desguerre, I.; Khirani, S. The value of Respiratory Muscle Testing in Children with Neuromuscular Disease. Chest 2015, 147, 552–559. [Google Scholar] [CrossRef]
- Schoser, B.; Fong, E.; Geberhiwot, T.; Hughes, D.; Kissel, J.T.; Madathil, S.C.; Orlikowski, D.; Polkey, M.I.; Roberts, M.; Tiddens, A.W.M.; et al. Maximun inspiratory pressure as a clinically meaningful trial endpoint for neuromuscular diseases: A comprehensive review of the literature. Orphanet J. Rare Dis. 2017, 12, 52. [Google Scholar] [CrossRef] [Green Version]
- Tyrosh, R.; Katz-Leurer, M.; Getz, M.D. Halliwick-Based Aquatic Assesments: Reliability and Validity. Int. J. Aquat. Res. Educ. 2008, 2, 224–236. [Google Scholar]
- Haley, S.M.; Coster, W.J.; Ludlow, L.H.; Haltiwanger, J.T.; Andrellos, P.A. Pediatric Evaluation of Disability Inventory (PEDI). Development, Standarization and Administration Manual; Trustees of Boston University: Boston, MA, USA, 1992. [Google Scholar]
- Girabent-Farrés, M.; Fagoaga, J.; Amor-Barbosa, M.; Bagur-Calafat, C. Spanish Translation and Validation of the Neuromuscular Module of the Pediatric Quality of Life Inventory (PedsQL): Evaluation of the Quality of Life Perceived by 8–18 Years Old Children with Neuromuscular Diseases and by Their Parents. Rev. Neurol. 2018, 67, 425–435. [Google Scholar]
- Girabent-Farreés, M.; Monneé-Guasch, L.; Bagur-Calafat, C.; Fagoaga, J. Spanish Translation and Validation of the Neuromuscular Module of the Pediatric Quality of Life Inventory (PedsQL): Evaluation of the Quality of Life Perceived by the Parents of 2–4-year-old Children with Neuromuscular Diseases. Rev. Neurol. 2018, 66, 81–88. [Google Scholar] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeren, M.; Cakir, E.; Gurses, H.N. Effects of inspiratory muscle training on postural stability, pulmonary function and functional capacity in children with cystic fibrosis: A randomised controlled trial. Respir. Med. 2019, 148, 24–30. [Google Scholar] [CrossRef]
- Montes, J.; Garber, C.E.; Kramer, S.S.; Montgomery, M.J.; Dunaway, S.; Kamil-Rosenberg, S.; Carr, B.; Cruz, R.; Strauss, N.E.; Sproule, D.; et al. Single-blind, randomized, controlled clinical trial of exercise in ambulatory spinal muscular atrophy: Why are the results negative? J. Neuromuscul. Dis. 2015, 2, 463–470. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Participant Code | Diagnosis of the Child | Age (Years) | Sex | Height (cm) | Weight (kg) | Time Since Began Aquatic Therapy (Months) | Vignos Scale | Mechanical Ventilation |
|---|---|---|---|---|---|---|---|---|
| S1 | DMD | 18 | M | 157 | 61 | 48 | 7 | Does not require |
| S2 | Congenital myopathy | 7 | M | 129 | 23 | 18 | 2 | Does not require |
| S3 | NMD non hereditary | 10 | M | 142 | 32 | 18 | 1 | Does not require |
| S4 | SMA type II | 5 | M | 115 | 17 | 24 | 9 | Nocturnal BiPAP |
| S5 | SMA type II | 4 | M | 100 | 15.6 | 15 | 9 | Nocturnal BiPAP |
| S6 | SMA type III | 5 | F | 107 | 15 | 20 | 2 | Does not require |
| S7 | DMD | 11 | M | 146 | 63 | 21 | 9 | Does not require |
| S8 | SMA type II | 4 | F | 98 | 12 | 18 | 8 | Does not require |
| S9 | CMT | 5 | F | 119 | 20 | 24 | 3 | Does not require |
| S10 | CMT | 12 | F | 150 | 45 | 24 | 7 | Does not require |
| S11 | Steinert myotonic dystrophy | 11 | F | 152 | 40 | 6 | 1 | Does not require |
| Measurement Moments | 1st Session of Aquatic Therapy | 5th Session of AT | 10th Session of AT | p-Value | |||
|---|---|---|---|---|---|---|---|
| Mean/CI Outcome Measures | PRE: Baseline | POST | PRE | POST | PRE | POST: Final | |
| FEV1 Mean CI | 1.3 ± 0.61 0.4–2.14 | 1.14 ± 0.52 0.4–1.99 | 1.12 ± 0.48 0.5–2.16 | 1.23 ± 0.53 0.52–2.02 | 1.04 ± 0.58 0.38–2.09 | 1.22 ± 0.59 0.45–2.13 | >0.05 |
| PCF Mean CI | 156.36 ± 63.45 60–250 | 160.91 ± 61.23 70–250 | 164.55 ± 75.28 70–270 | 166.36 ± 73.39 70–260 | 169.09 ± 78.54 70–270 | 174.55 ± 76.07 70–270 | >0.05 |
| MEP Mean CI | 33.91 ± 17.64 8–57 | 33.18 ± 20.05 7–66 | 33.36 ± 17.41 6–54 | 33.09 ± 15.68 11–53 | 35.45 ± 18.09 11–56 | 37.82 ± 19.66 12–63 | >0.05 |
| MIP Mean CI | −27.18 ±16.28 −50–−4 | −30.36 ± 18.51 −57–−1 | −31.64 ± 14.62 −48–−7 | -34.27 ± 19.08 −59–−9 | −34.64 ± 14.3 −52–−9 | −35.82 ± 19.67 −59–−12 | >0.05 |
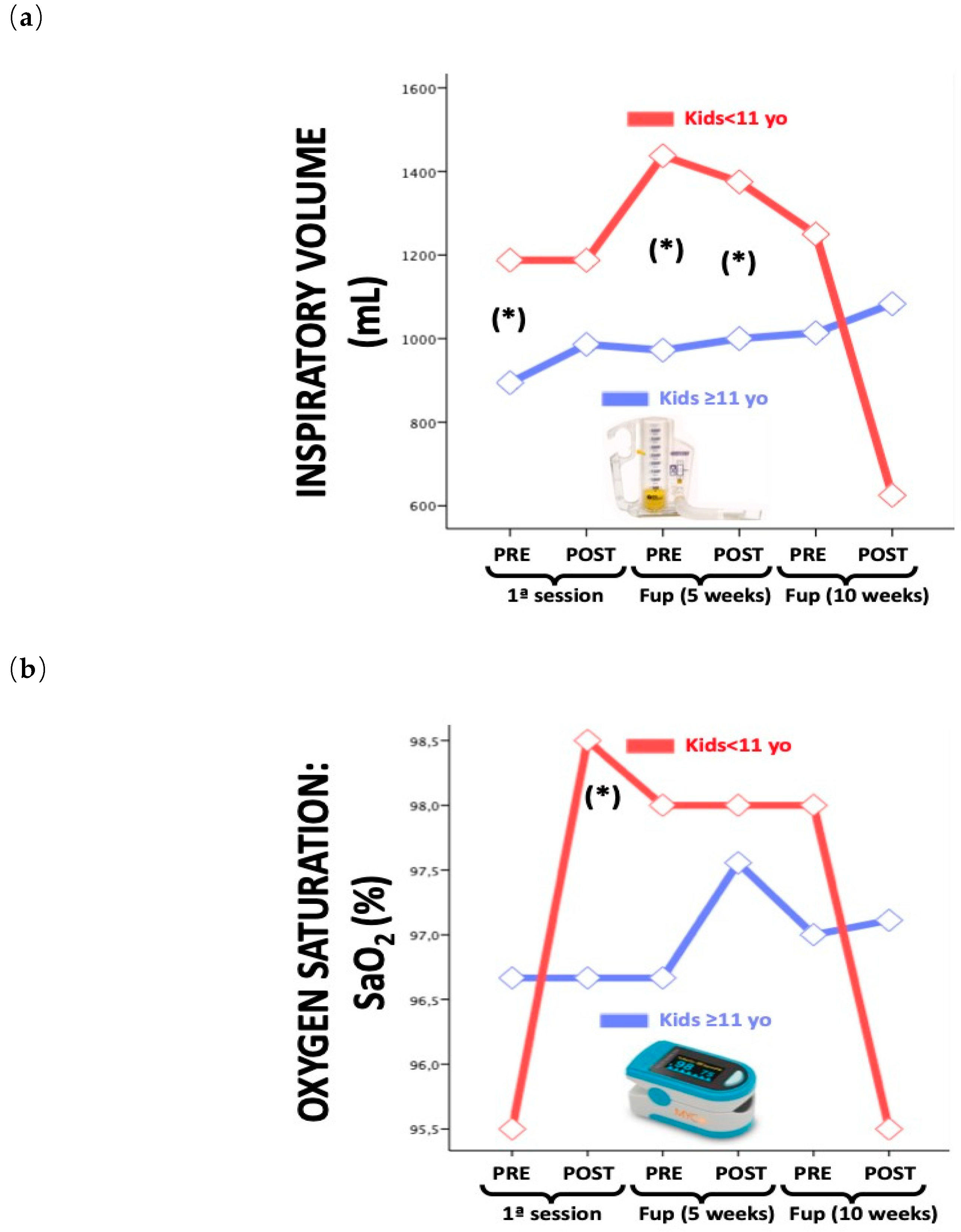
| Inspired VOL Mean CI | 947.73 ± 469.5 200–1.750 | 1.022.73 ± 446.58 250–2.000 | 1.056.82 ± 441.46 375–1.750 | 1.137.50 ± 505.01 250–2.000 | 1.056.82 ± 560.03 250–2.125 | 1.000.00 ± 594.24 125–2.375 | 0.002 |
| O2 SAT Mean CI | 96.45 ± 1.44 94–98 | 97 ± 1.55 94–99 | 96.91 ± 1.3 95–98 | 97.64 ± 0.67 97–99 | 97.18 ± 0.75 96–98 | 96.82 ± 1.17 95–99 | 0.029 |
| Measurement Moments | Baseline: 1st Session of Aquatic Therapy | Follow-up: 5th Session of AP | Follow-up: 10th Session of AP | p | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Outcome Measures | MEAN 1 | DS 1 | MIN 1 | MAX 1 | MEAN 2 | DS 2 | MIN 2 | MAX 2 | MEAN 3 | DS 3 | MIN 3 | MAX 3 | |
| WOTA 1 | 42.36 | 8.2 | 28 | 50 | 43.09 | 7.45 | 30 | 50 | 45.73 | 5.55 | 34 | 51 | >0.05 |
| PEDI | |||||||||||||
| Selfcare | 51.36 | 11.52 | 35 | 68 | 52.36 | 11.47 | 38 | 69 | 54.73 | 10.36 | 41 | 70 | >0.05 |
| Mobility | 28.55 | 18.37 | 8 | 54 | 30.55 | 19.05 | 9 | 53 | 31.55 | 18.34 | 10 | 52 | >0.05 |
| Social function | 58.64 | 4.2 | 53 | 65 | 59.45 | 3.98 | 53 | 65 | 60.09 | 4.11 | 54 | 65 | >0.05 |
| PEDSQL | |||||||||||||
| D (p) | 70.26 | 13.39 | 54.41 | 94.11 | 71.68 | 10.31 | 55.89 | 90 | 71.25 | 7.54 | 58.8 | 82.35 | >0.05 |
| C (p) | 64.77 | 38.34 | 25.1 | 100 | 63.63 | 33.6 | 27.99 | 100 | 68.94 | 30.75 | 16.67 | 100 | >0.05 |
| FF (p) | 66.5 | 14.92 | 45 | 90 | 67.73 | 20.17 | 35 | 90 | 63.64 | 18.99 | 25 | 95 | >0.05 |
| TOTAL p | 70.73 | 12.92 | 51 | 98 | 69.55 | 11.94 | 50 | 88.04 | 66.6 | 6.01 | 56 | 74 | >0.05 |
| TOTAL c | 79.52 | 9.4 | 65 | 94.71 | 75.68 | 6.99 | 61 | 82.35 | 73.65 | 8.39 | 58 | 87 | >0.05 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huguet-Rodríguez, M.; Arias-Buría, J.L.; Huguet-Rodríguez, B.; Blanco-Barrero, R.; Braña-Sirgo, D.; Güeita-Rodríguez, J. Impact of Aquatic Exercise on Respiratory Outcomes and Functional Activities in Children with Neuromuscular Disorders: Findings from an Open-Label and Prospective Preliminary Pilot Study. Brain Sci. 2020, 10, 458. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070458
Huguet-Rodríguez M, Arias-Buría JL, Huguet-Rodríguez B, Blanco-Barrero R, Braña-Sirgo D, Güeita-Rodríguez J. Impact of Aquatic Exercise on Respiratory Outcomes and Functional Activities in Children with Neuromuscular Disorders: Findings from an Open-Label and Prospective Preliminary Pilot Study. Brain Sciences. 2020; 10(7):458. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070458
Chicago/Turabian StyleHuguet-Rodríguez, Marta, José Luis Arias-Buría, Belén Huguet-Rodríguez, Rocío Blanco-Barrero, Daniel Braña-Sirgo, and Javier Güeita-Rodríguez. 2020. "Impact of Aquatic Exercise on Respiratory Outcomes and Functional Activities in Children with Neuromuscular Disorders: Findings from an Open-Label and Prospective Preliminary Pilot Study" Brain Sciences 10, no. 7: 458. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10070458