When, How, and to What Extent Are Individuals with Unresponsive Wakefulness Syndrome Able to Progress? Functional Independence

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Data Analysis
3. Results
3.1. Participants
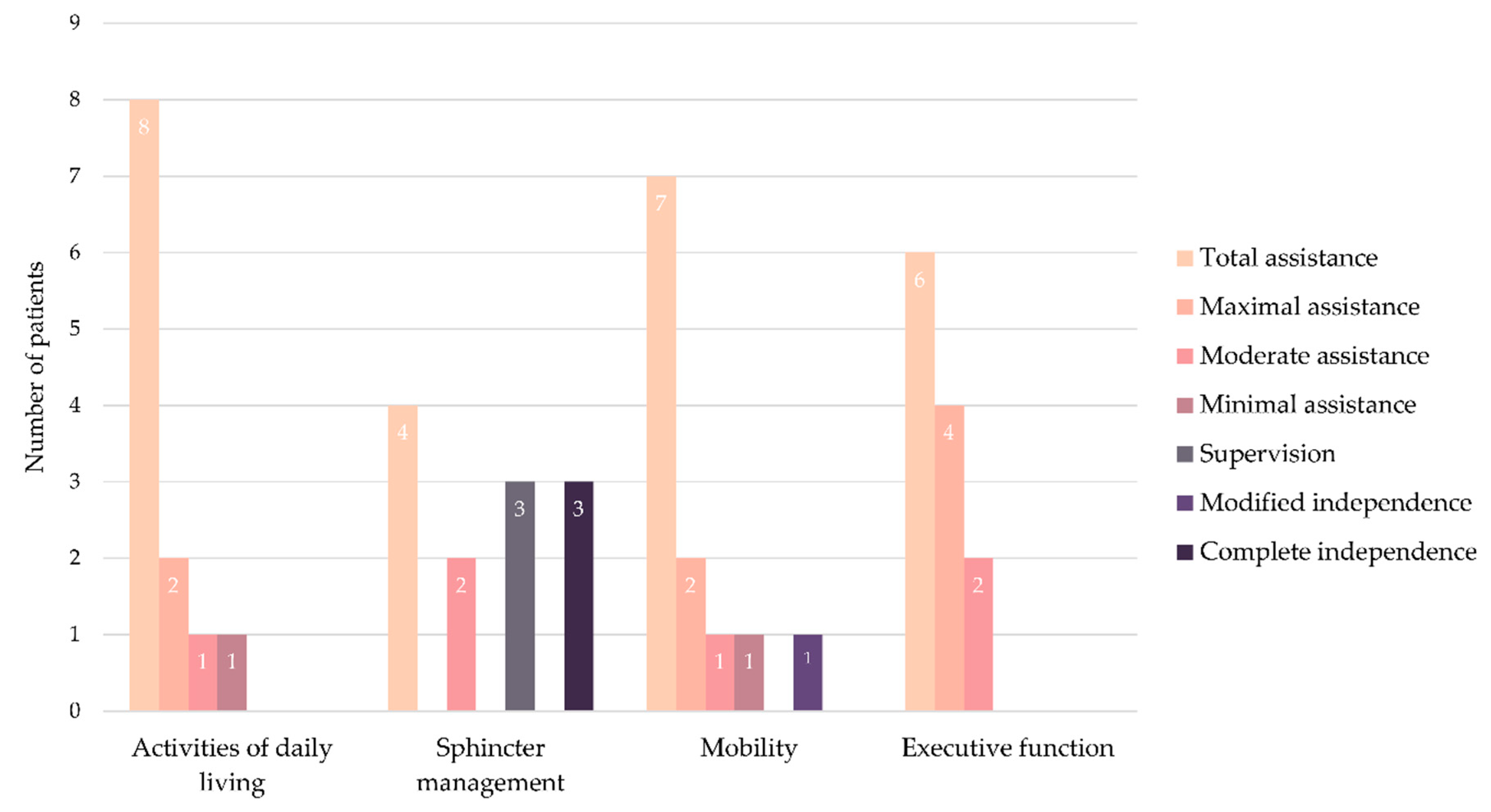
3.2. Functional Independence
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Jennett, B.; Plum, F. Persistent vegetative state after brain damage. RN 1972, 35, 734–737. [Google Scholar] [CrossRef]
- Casarett, D.; Fishman, J.M.; MacMoran, H.J.; Pickard, A.; Asch, D.A. Epidemiology and prognosis of coma in daytime television dramas. Br. Med. J. 2005, 331, 1537–1539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Septien, S.; Rubin, M.A. Disorders of Consciousness: Ethical Issues of Diagnosis, Treatment, and Prognostication. Semin. Neurol. 2018, 38, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Aspen Consensus Conference Workgroup on the Vegetative and Minimally Conscious States Draft Consensus Statement; Aspen: Hoboken, NJ, USA, 1996.
- Giacino, J.T.; Kalmar, K. The vegetative and minimally conscious states: A comparison of clinical features and functional outcome. J. Head Trauma Rehabil. 1997, 12, 36–51. [Google Scholar] [CrossRef]
- Burke, W.J. The minimally conscious state: Definition and diagnostic criteria. Neurology 2002, 59, 1473–1474. [Google Scholar] [CrossRef] [PubMed]
- Farisco, M.; Laureys, S.; Evers, K. The intrinsic activity of the brain and its relation to levels and disorders of consciousness. Mind Matter 2017, 15, 197–219. [Google Scholar]
- Laureys, S.; Celesia, G.G.; Cohadon, F.; Lavrijsen, J.; León-Carrión, J.; Sannita, W.G.; Sazbon, L.; Schmutzhard, E.; von Wild, K.R.; Zeman, A.; et al. Unresponsive wakefulness syndrome: A new name for the vegetative state or apallic syndrome. BMC Med. 2010, 8, 68. [Google Scholar] [CrossRef] [Green Version]
- Sarà, M.; Sacco, S.; Cipolla, F.; Onorati, P.; Scoppetta, C.; Albertini, G.; Carolei, A. An unexpected recovery from permanent vegetative state. Brain Inj. 2007, 21, 101–103. [Google Scholar] [CrossRef]
- Dhamapurkar, S.K.; Rose, A.; Florschutz, G.; Wilson, B.A. The natural history of continuing improvement in an individual after a long period of impaired consciousness: The story of I.J. Brain Inj. 2016, 30, 230–236. [Google Scholar] [CrossRef]
- Faran, S.; Vatine, J.J.; Lazary, A.; Ohry, A.; Birbaumer, N.; Kotchoubey, B. Late recovery from permanent traumatic vegetative state heralded by event-related potentials. J. Neurol. Neurosurg. Psychiatry 2006, 77, 998–1000. [Google Scholar] [CrossRef] [Green Version]
- Childs, N.L.; Mercer, W.N. Brief report: Late improvement in consciousness after post-traumatic vegetative state. N. Engl. J. Med. 1996, 334, 24–25. [Google Scholar] [CrossRef] [PubMed]
- McMillan, T.M.; Herbert, C.M. Further recovery in a potential treatment withdrawal case 10 years after brain injury. Brain Inj. 2004, 18, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Sancisi, E.; Battistini, A.; Di Stefano, C.; Simoncini, L.; Simoncini, L.; Montagna, P.; Piperno, R. Late recovery from post-traumatic vegetative state. Brain Inj. 2009, 23, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Illman, N.A.; Crawford, S. Late-recovery from “permanent” vegetative state in the context of severe traumatic brain injury: A case report exploring objective and subjective aspects of recovery and rehabilitation. Neuropsychol. Rehabil. 2018, 28, 1360–1374. [Google Scholar] [CrossRef]
- De Tanti, A.; Saviola, D.; Basagni, B.; Cavatorta, S.; Chiari, M.; Casalino, S.; De Bernardi, D.; Galvani, R. Recovery of consciousness after 7 years in vegetative state of non-traumatic origin: A single case study. Brain Inj. 2016, 30, 1029–1034. [Google Scholar] [CrossRef]
- Naro, A.; Calabrò, R.S.; Pollicino, P.; Lombardo, C.; Bramanti, P. Unexpected recovery from a vegetative state or misdiagnosis? Lesson learned from a case report. NeuroRehabilitation 2017, 41, 735–738. [Google Scholar] [CrossRef] [Green Version]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. A practical scale. Lancet 1975, 305, 480–484. [Google Scholar] [CrossRef]
- Gouvier, W.D.; Blanton, P.D.; LaPorte, K.K.; Nepomuceno, C. Reliability and validity of the Disability Rating Scale and the Levels of Cognitive Functioning Scale in monitoring recovery from severe head injury. Arch. Phys. Med. Rehabil. 1987, 68, 94–97. [Google Scholar] [CrossRef]
- Katz, D.I.; Polyak, M.; Coughlan, D.; Nichols, M.; Roche, A. Natural history of recovery from brain injury after prolonged disorders of consciousness: Outcome of patients admitted to inpatient rehabilitation with 1–4 year follow-up. Prog. Brain Res. 2009, 177, 73–88. [Google Scholar] [CrossRef]
- Luauté, J.; Maucort-Boulch, D.; Tell, L.; Quelard, F.; Sarraf, T.; Iwaz, J.; Boisson, D.; Fischer, C. Long-term outcomes of chronic minimally conscious and vegetative states. Neurology 2010, 75, 246–252. [Google Scholar] [CrossRef]
- Estraneo, A.; Moretta, P.; Loreto, V.; Lanzillo, B.; Santoro, L.; Trojano, L. Late recovery after traumatic, anoxic, or hemorrhagic long-lasting vegetative state. Neurology 2010, 75, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Moretta, P.; Loreto, V.; Lanzillo, B.; Cozzolino, A.; Saltalamacchia, A.; Lullo, F.; Santoro, L.; Trojano, L. Predictors of recovery of responsiveness in prolonged anoxic vegetative state. Neurology 2013, 80, 464–470. [Google Scholar] [CrossRef]
- Steppacher, I.; Kaps, M.; Kissler, J. Will time heal? A long-term follow-up of severe disorders of consciousness. Ann. Clin. Transl. Neurol. 2014, 1, 401–408. [Google Scholar] [CrossRef] [PubMed]
- Stineman, M.G.; Ross, R.N.; Fiedler, R.; Granger, C.V.; Maislin, G. Staging functional independence validity and applications. Arch. Phys. Med. Rehabil. 2003, 84, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Estraneo, A.; Moretta, P.; Loreto, V.; Santoro, L.; Trojano, L. Clinical and neuropsychological long-term outcomes after late recovery of responsiveness: A case series. Arch. Phys. Med. Rehabil. 2014, 95, 711–716. [Google Scholar] [CrossRef] [PubMed]
- Nakase-Richardson, R.; Whyte, J.; Giacino, J.T.; Pavawalla, S.; Barnett, S.D.; Yablon, S.A.; Sherer, M.; Kalmar, K.; Hammond, F.M.; Greenwald, B.; et al. Longitudinal outcome of patients with disordered consciousness in the NIDRR TBI model systems programs. J. Neurotrauma 2012, 29, 59–65. [Google Scholar] [CrossRef]
- Whyte, J.; Nakase-Richardson, R.; Hammond, F.M.; McNamee, S.; Giacino, J.T.; Kalmar, K.; Greenwald, B.D.; Yablon, S.A.; Horn, L.J. Functional outcomes in traumatic disorders of consciousness: 5-year outcomes from the National Institute on Disability and Rehabilitation Research traumatic brain injury model systems. Arch. Phys. Med. Rehabil. 2013, 94, 1855–1860. [Google Scholar] [CrossRef]
- Hammond, F.M.; Giacino, J.T.; Nakase Richardson, R.; Sherer, M.; Zafonte, R.D.; Whyte, J.; Arciniegas, D.B.; Tang, X. Disorders of consciousness due to traumatic brain injury: Functional status ten years post-injury. J. Neurotrauma 2019, 36, 1136–1146. [Google Scholar] [CrossRef]
- Giacino, J.T.; Katz, D.I.; Schiff, N.D.; Whyte, J.; Ashman, E.J.; Ashwal, S.; Barbano, R.; Hammond, F.M.; Laureys, S.; Ling, G.S.F.; et al. Practice guideline update recommendations summary: Disorders of consciousness. Neurology 2018, 91, 450–460. [Google Scholar] [CrossRef] [Green Version]
- Kondziella, D.; Bender, A.; Diserens, K.; van Erp, W.; Estraneo, A.; Formisano, R.; Laureys, S.; Naccache, L.; Ozturk, S.; Rohaut, B.; et al. European Academy of Neurology guideline on the diagnosis of coma and other disorders of consciousness. Eur. J. Neurol. 2020, 27, 741–756. [Google Scholar] [CrossRef] [Green Version]
- Noé, E.; Olaya, J.; Navarro, M.D.; Noguera, P.; Colomer, C.; García-Panach, J.; Rivero, S.; Moliner, B.; Ferri, J. Behavioral recovery in disorders of consciousness: A prospective study with the Spanish version of the coma recovery scale-revised. Arch. Phys. Med. Rehabil. 2012, 93, 428–433.e12. [Google Scholar] [CrossRef] [PubMed]
- Ferri, J.; Noé, E.; Lloréns, R. The Spanish version of the coma recovery scale-revised: Events on a correct timeline. Brain Inj. 2015, 29, 1002–1003. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Wright, J. Disability Rating Scale. In Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 862–863. ISBN 978-0-387-79948-3. [Google Scholar]
- Noé, E.; Ferri, J.; Olaya, J.; Navarro, M.D.; O’Valle, M.; Colomer, C.; Moliner, B.; Ippoliti, C.; Maza, A.; Llorens, R. When, how and to what extent are individuals with unresponsive wakefulness syndrome able to progress? Neurobehavioral progress. Brain Sci. 2020. under review. [Google Scholar]
- Greenwald, B.D.; Hammond, F.M.; Harrison-Felix, C.; Nakase-Richardson, R.; Howe, L.L.S.; Kreider, S. Mortality following Traumatic Brain Injury among Individuals Unable to Follow Commands at the Time of Rehabilitation Admission: A National Institute on Disability and Rehabilitation Research Traumatic Brain Injury Model Systems Study. J. Neurotrauma 2015, 32, 1883–1892. [Google Scholar] [CrossRef] [Green Version]
- Estraneo, A.; De Bellis, F.; Masotta, O.; Loreto, V.; Fiorenza, S.; Lo Sapio, M.; Trojano, L. Demographical and clinical indices for long-term evolution of patients in vegetative or in minimally conscious state. Brain Inj. 2019, 33, 1633–1639. [Google Scholar] [CrossRef]
- Pincherle, A.; Rossi, F.; Jöhr, J.; Dunet, V.; Ryvlin, P.; Oddo, M.; Schiff, N.; Diserens, K. Early discrimination of cognitive motor dissociation from disorders of consciousness: Pitfalls and clues. J. Neurol. 2020. [Google Scholar] [CrossRef]
- Cruse, D.; Chennu, S.; Chatelle, C.; Bekinschtein, T.A.; Fernández-Espejo, D.; Pickard, J.D.; Laureys, S.; Owen, A.M. Bedside detection of awareness in the vegetative state: A cohort study. Lancet 2011, 378, 2088–2094. [Google Scholar] [CrossRef] [Green Version]
- Monti, M.M.; Vanhaudenhuyse, A.; Coleman, M.R.; Boly, M.; Pickard, J.D.; Tshibanda, L.; Owen, A.M.; Laureys, S. Willful modulation of brain activity in disorders of consciousness. N. Engl. J. Med. 2010, 362, 579–589. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Characteristics | Admission | Progression from UWS to MCS | Emergence from MCS | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Etiology | Age | Time Since Injury | CRS-R | Age | Time Since Injury | Time Since Admission | CRS-R | Signs | Age | Time Since Injury | Time since Admission | CRS-R | Signs | |
| Patient 1 | M | Traumatic | 25 | 86 | 5 | 25 | 110 | 24 | 6 | V | 26 | 271 | 185 | 20 | C |
| Patient 2 | M | Anoxia | 14 | 38 | 7 | 14 | 76 | 38 | 10 | V | 14 | 104 | 66 | 22 | C |
| Patient 3 | M | Traumatic | 26 | 38 | 6 | 26 | 76 | 38 | 18 | M | 26 | 132 | 94 | 23 | C/FU |
| Patient 4 | M | Traumatic | 19 | 240 | 3 | 20 | 486 | 246 | 14 | V/M | 20 | 668 | 428 | 20 | C |
| Patient 5 | W | Traumatic | 31 | 146 | 7 | 31 | 178 | 32 | 8 | V | 32 | 346 | 200 | 19 | C/FU |
| Patient 6 | M | Traumatic | 31 | 62 | 8 | 31 | 89 | 27 | 10 | M | 31 | 172 | 110 | 18 | C/FU |
| Patient 7 | M | Traumatic | 25 | 213 | 8 | 25 | 250 | 37 | 10 | V/M | 25 | 401 | 188 | 16 | C |
| Patient 8 | M | Traumatic | 33 | 45 | 6 | 33 | 91 | 46 | 11 | V/M | 33 | 201 | 156 | 19 | FU |
| Patient 9 | M | Fat embolism | 19 | 45 | 6 | 19 | 86 | 41 | 10 | C | 19 | 99 | 54 | 12 | C |
| Patient 10 | M | Traumatic | 21 | 117 | 8 | 21 | 181 | 64 | 9 | V | 21 | 243 | 126 | 21 | FU |
| Patient 11 | M | Traumatic | 13 | 126 | 8 | 13 | 158 | 32 | 12 | V | 13 | 222 | 96 | 21 | FU |
| Patient 12 | M | Traumatic | 31 | 101 | 7 | 31 | 130 | 29 | 9 | V | 31 | 154 | 53 | 18 | FU |
| Patients | Emergence from MCS | 6-Month Assessment | 12-Month Assessment | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Disability Rating Scale | Barthel Index | Functional Independence Measure | Disability Rating Scale | Barthel Index | Functional Independence Measure | Disability Rating Scale | Barthel Index | Functional Independence Measure | |||||||
| Motor | Cognitive | Total | Motor | Cognitive | Total | Motor | Cognitive | Total | |||||||
| Patient 1 | 17 | 0 | 13 | 6 | 19 | 14 | 21 | 14 | 11 | 25 | 12 | 23 | 20 | 11 | 31 |
| Patient 2 | 14 | 0 | 13 | 7 | 20 | 11 | 26 | 30 | 17 | 47 | 10 | 47 | 36 | 22 | 58 |
| Patient 3 | 17 | 0 | 13 | 6 | 19 | 11 | 25 | 24 | 12 | 36 | 9 | 25 | 26 | 14 | 40 |
| Patient 4 | 20 | 0 | 13 | 5 | 18 | 20 | 0 | 13 | 5 | 18 | 20 | 0 | 13 | 6 | 19 |
| Patient 5 | 19 | 2 | 13 | 5 | 18 | 18 | 2 | 14 | 9 | 23 | 18 | 2 | 14 | 9 | 23 |
| Patient 6 | 15 | 4 | 15 | 7 | 22 | 16 | 26 | 29 | 12 | 41 | 16 | 27 | 29 | 12 | 41 |
| Patient 7 | 17 | 0 | 13 | 5 | 18 | 16 | 0 | 13 | 5 | 18 | 16 | 0 | 13 | 6 | 19 |
| Patient 8 | 17 | 0 | 13 | 5 | 18 | 17 | 5 | 24 | 7 | 31 | 17 | 20 | 28 | 8 | 36 |
| Patient 9 | 15 | 2 | 13 | 7 | 20 | 13 | 12 | 21 | 15 | 36 | 9 | 45 | 36 | 17 | 53 |
| Patient 10 | 12 | 12 | 19 | 9 | 28 | 6 | 58 | 62 | 23 | 85 | 6 | 86 | 68 | 24 | 92 |
| Patient 11 | 13 | 8 | 16 | 8 | 24 | 11 | 55 | 52 | 16 | 68 | 7 | 88 | 78 | 19 | 97 |
| Patient 12 | 19 | 0 | 13 | 5 | 18 | 19 | 1 | 13 | 6 | 19 | 19 | 15 | 13 | 6 | 19 |
| Patients | Emergence from MCS | 6-Month Assessment | 12-Month Assessment | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Activities of Daily Living | Sphincter Management | Mobility | Executive Function | Activities of Daily Living | Sphincter Management | Mobility | Executive Function | Activities of Daily Living | Sphincter Management | Mobility | Executive Function | |
| Patient 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 3 | 1 | 1 |
| Patient 2 | 1 | 1 | 1 | 1 | 1 | 7 | 1 | 2 | 1 | 7 | 1 | 3 |
| Patient 3 | 1 | 1 | 1 | 1 | 1 | 4 | 1 | 1 | 1 | 5 | 1 | 2 |
| Patient 4 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 |
| Patient 5 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 1 |
| Patient 6 | 1 | 1 | 1 | 1 | 1 | 3 | 2 | 1 | 1 | 3 | 2 | 1 |
| Patient 7 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Patient 8 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 1 | 2 | 5 | 3 | 1 |
| Patient 9 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 2 | 2 | 5 | 1 | 2 |
| Patient 10 | 1 | 1 | 2 | 1 | 4 | 7 | 4 | 3 | 4 | 7 | 4 | 3 |
| Patient 11 | 1 | 1 | 1 | 1 | 1 | 1 | 6 | 2 | 3 | 7 | 6 | 2 |
| Patient 12 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olaya, J.; Noé, E.; Navarro, M.D.; O’Valle, M.; Colomer, C.; Moliner, B.; Ippoliti, C.; Ferri, J.; Maza, A.; Llorens, R. When, How, and to What Extent Are Individuals with Unresponsive Wakefulness Syndrome Able to Progress? Functional Independence. Brain Sci. 2020, 10, 990. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120990
Olaya J, Noé E, Navarro MD, O’Valle M, Colomer C, Moliner B, Ippoliti C, Ferri J, Maza A, Llorens R. When, How, and to What Extent Are Individuals with Unresponsive Wakefulness Syndrome Able to Progress? Functional Independence. Brain Sciences. 2020; 10(12):990. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120990
Chicago/Turabian StyleOlaya, José, Enrique Noé, María Dolores Navarro, Myrtha O’Valle, Carolina Colomer, Belén Moliner, Camilla Ippoliti, Joan Ferri, Anny Maza, and Roberto Llorens. 2020. "When, How, and to What Extent Are Individuals with Unresponsive Wakefulness Syndrome Able to Progress? Functional Independence" Brain Sciences 10, no. 12: 990. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10120990