Influence of Static Magnetic Field Stimulation on the Accuracy of Tachystoscopically Presented Line Bisection

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Experimental Procedure
2.2.1. Intervention Experiment
2.2.2. Preliminary Experiment
2.3. Transcranial Static Magnetic Stimulation (tSMS)
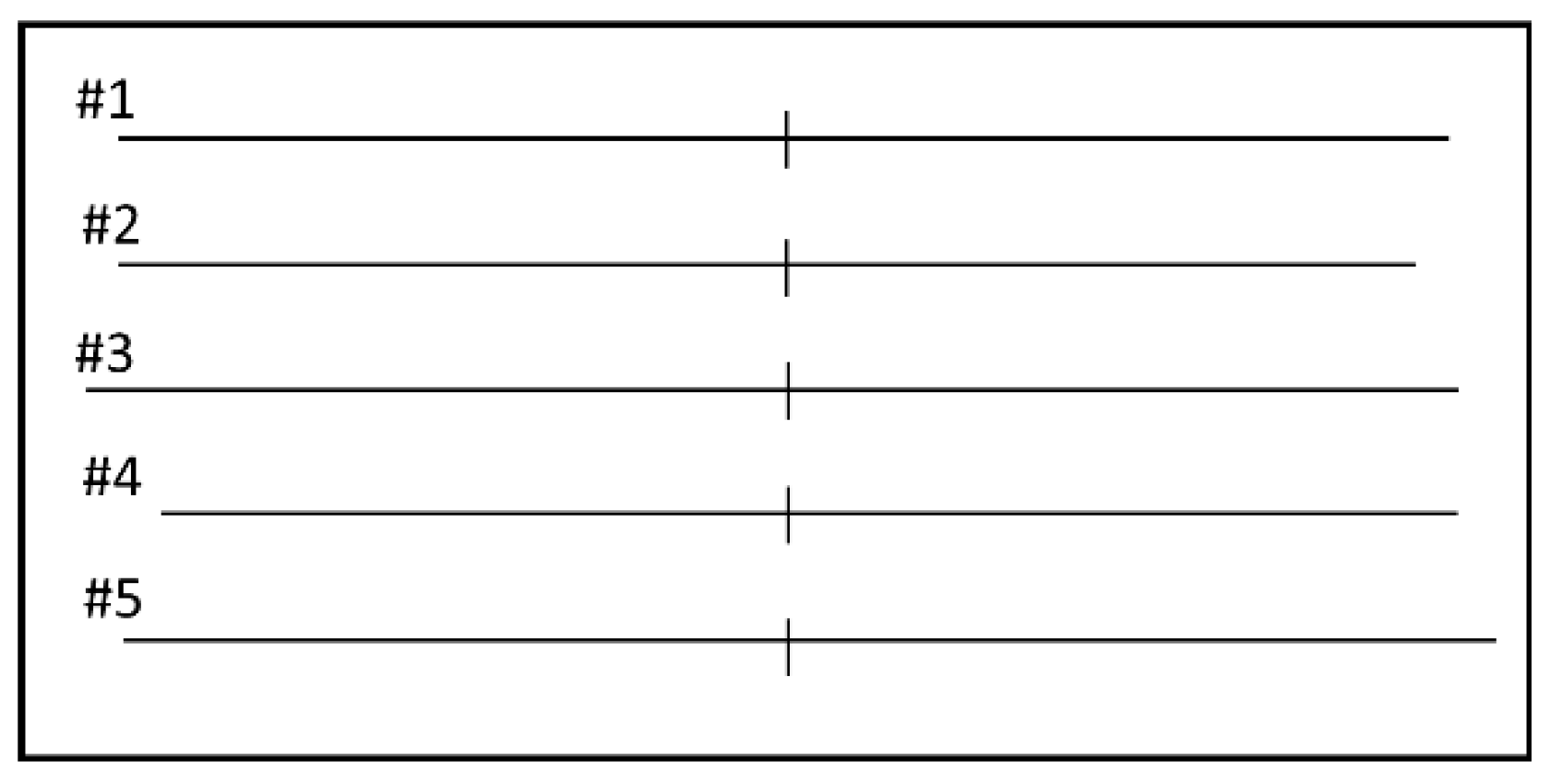
2.4. Line Length Judgement Task
2.5. Data and Statical Analyses
2.5.1. Scoring of Task Performance
2.5.2. Preliminary Experiment
2.5.3. Intervention Experiment
3. Results
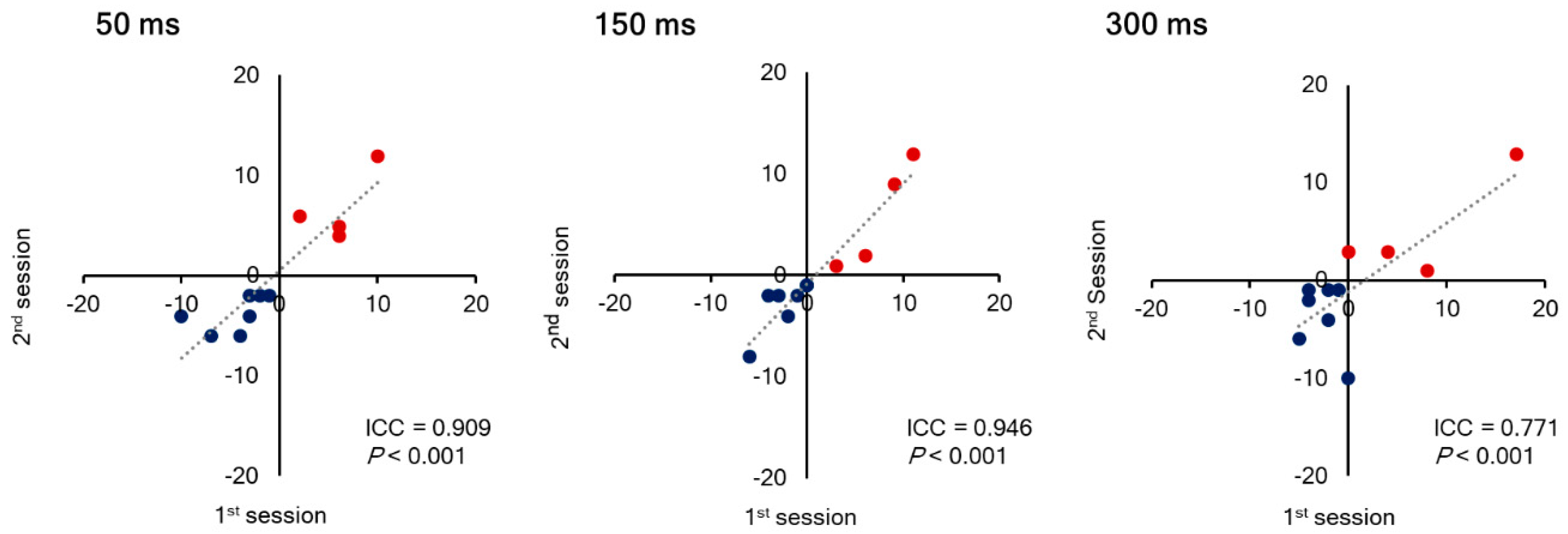
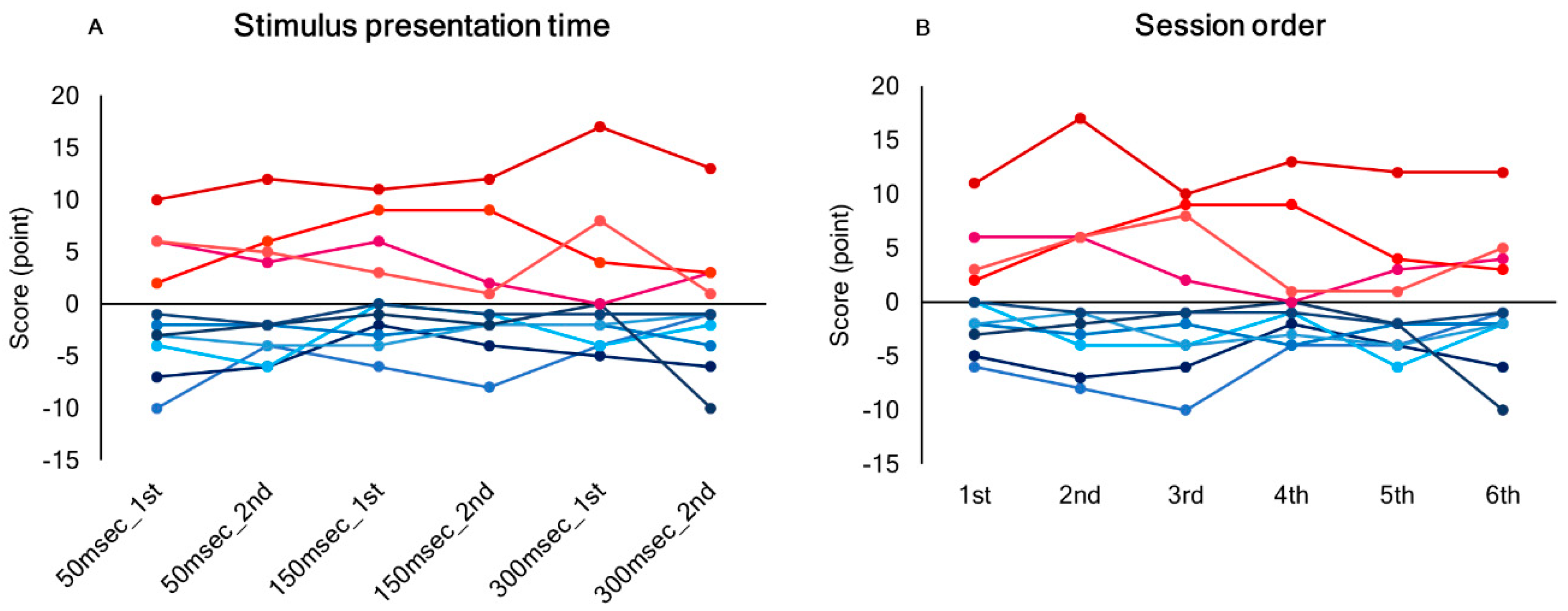
3.1. Inter-Trial Reproducibility of the Score in Line Length Judgement Task
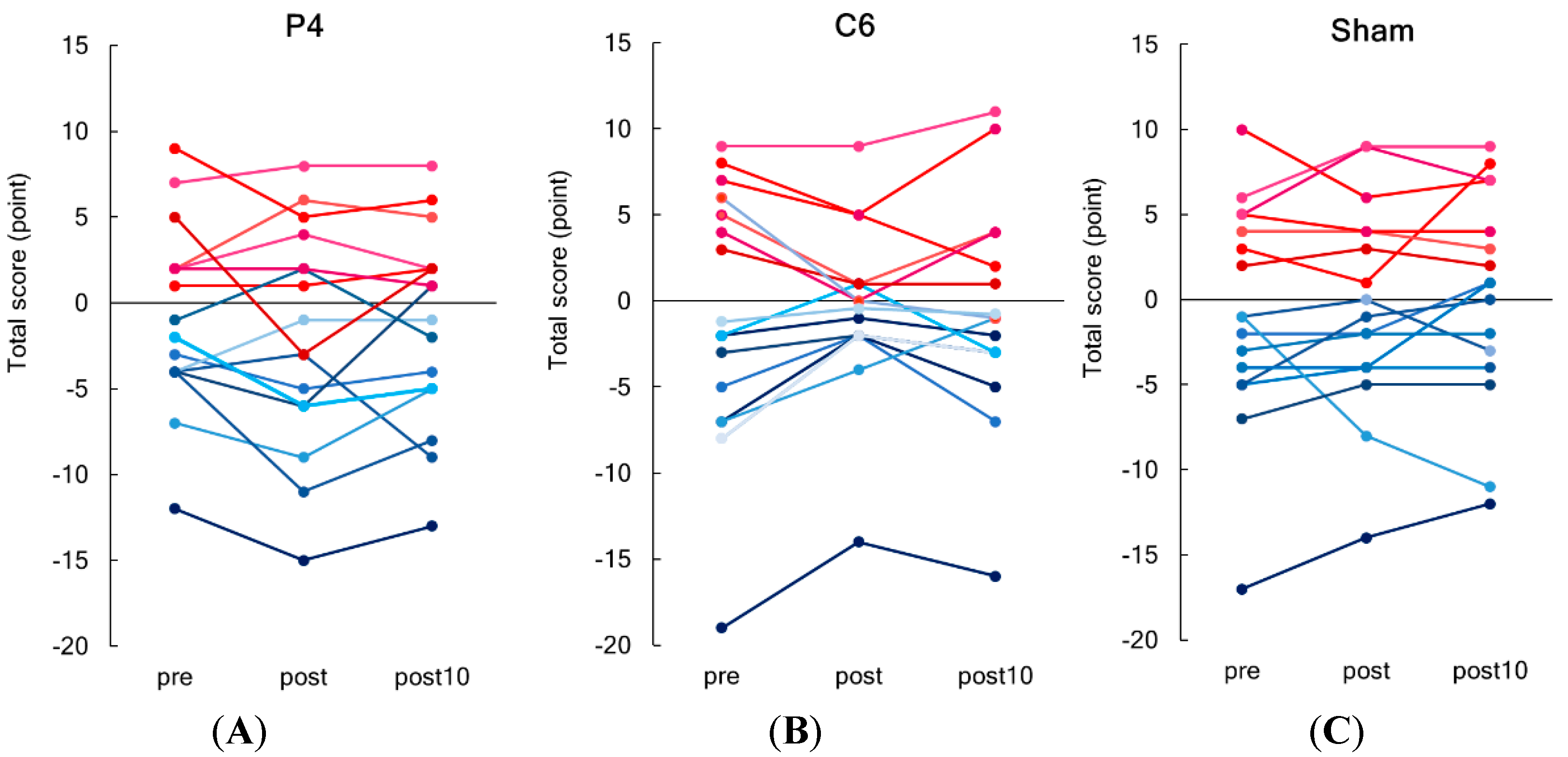
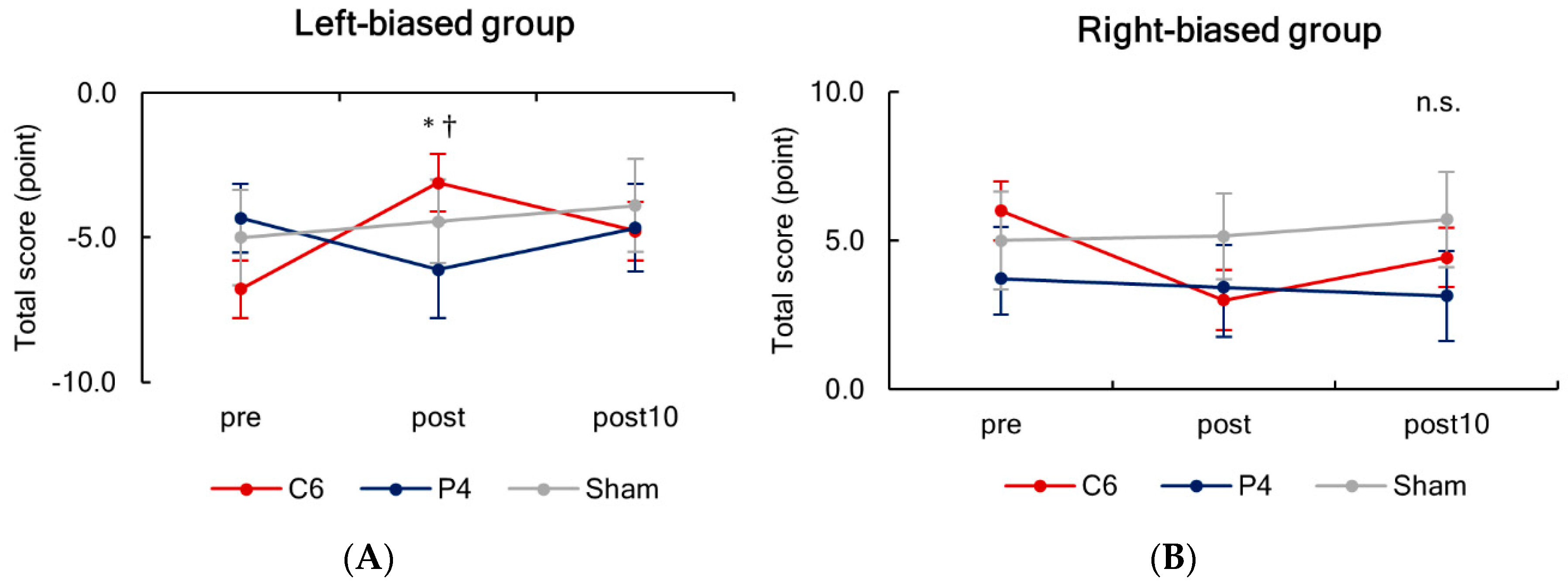
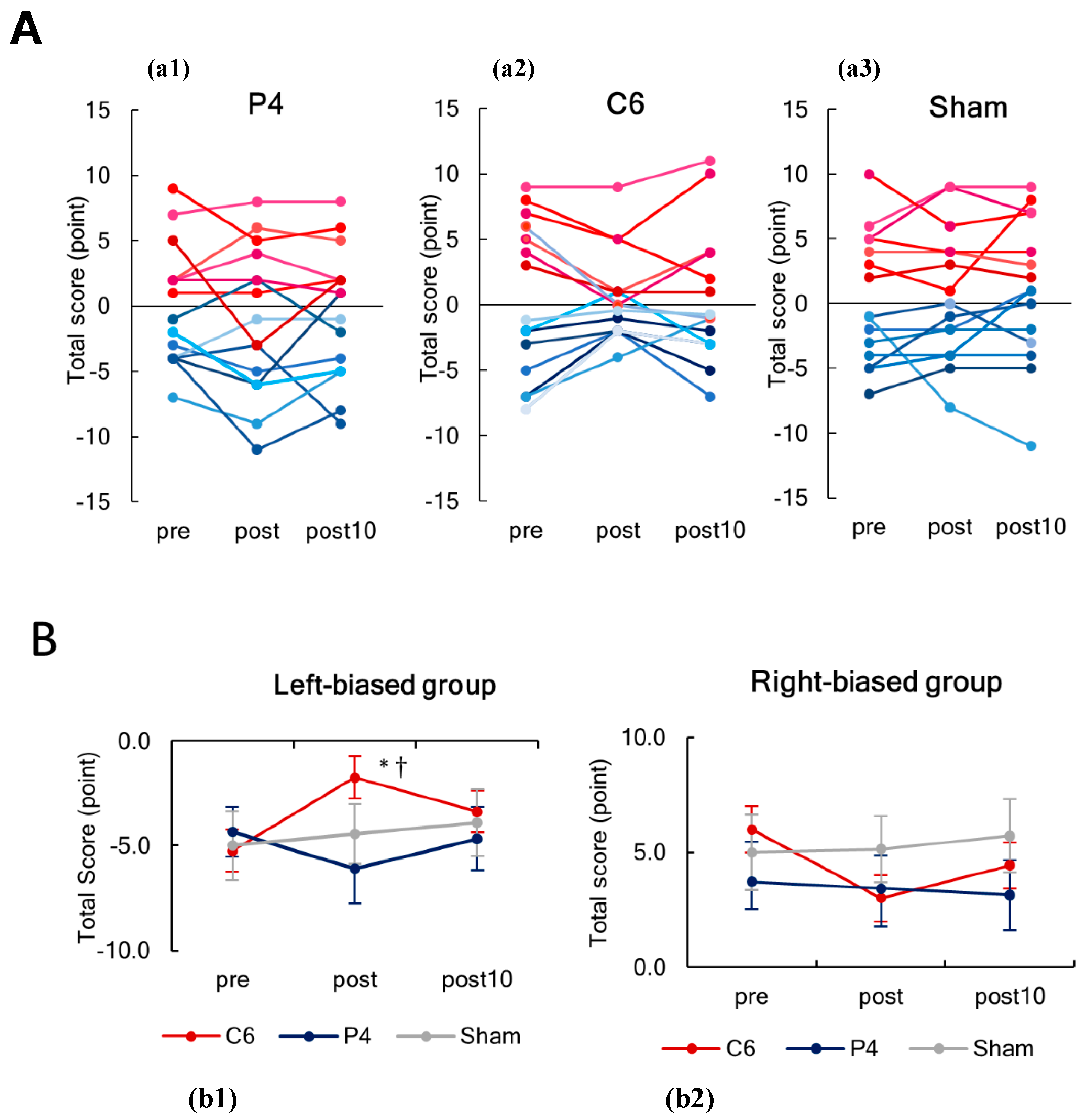
3.2. Effects of tSMS on the Scores of Line Length Judgement Task
4. Discussion
4.1. Leftward and Rightward Biases in Healthy Individuals
4.2. Putative Mechanisms Underlying Change in the Score of Line Length Judgement Task by tSMS Over C6
4.3. Clinical Application
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

References
- Oliviero, A.; Mordillo-Mateos, L.; Arias, P.; Panyavin, I.; Foffani, G.; Aguilar, J. Transcranial static magnetic field stimulation of the human motor cortex. J. Physiol. 2011, 589, 4949–4958. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aguila, J.; Cudeiro, J.; Rivadulla, C. Effects of Static Magnetic Fields on the Visual Cortex: Reversible Visual Deficits and Reduction of Neuronal Activity. Cereb. Cortex 2016, 26, 628–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rivadulla, C.; Aguilar, J.; Coletti, M.; Aguila, J.; Prieto, S.; Cudeiro, J. Static magnetic fields reduce epileptiform activity in anesthetized rat and monkey. Sci. Rep. 2018, 8, 15985. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Classen, J.; Gerloff, C.; Celnik, P.; Wassermann, E.M.; Hallett, M.; Cohen, L.G. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology 1997, 48, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Huang, Y.Z.; Edwards, M.J.; Rounis, E.; Bhatia, K.P.; Rothwell, J.C. Theta burst stimulation of the human motor cortex. Neuron 2005, 45, 201–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nitsche, M.A.; Paulus, W. Excitability changes induced in the human motor cortex by weak transcranial direct current stimulation. J. Physiol. 2000, 527, 633–639. [Google Scholar] [CrossRef]
- Nojima, I.; Koganemaru, S.; Fukuyama, H.; Mima, T. Static magnetic field can transiently alter the human intracortical inhibitory system. Clin. Neurophysiol. 2015, 126, 2314–2319. [Google Scholar] [CrossRef]
- Nojima, I.; Koganemaru, S.; Mima, T. Combination of Static Magnetic Fields and Peripheral Nerve Stimulation Can Alter Focal Cortical Excitability. Front. Hum. Neurosci. 2016, 10, 598. [Google Scholar] [CrossRef] [Green Version]
- Nojima, I.; Watanabe, T.; Gyoda, T.; Sugata, H.; Ikeda, T.; Mima, T. Transcranial static magnetic stimulation over the primary motor cortex alters sequential implicit motor learning. Neurosci. Lett. 2019, 696, 33–37. [Google Scholar] [CrossRef]
- Shibata, S.; Watanabe, T.; Yukawa, Y.; Minakuchi, M.; Shimomura, R.; Mima, T. Effect of transcranial static magnetic stimulation on intracortical excitability in the contralateral primary motor cortex. Neurosci. Lett. 2020, 723, 134871. [Google Scholar] [CrossRef]
- Davila-Perez, P.; Pascual-Leone, A.; Cudeiro, J. Effects of Transcranial Static Magnetic Stimulation on Motor Cortex Evaluated by Different TMS Waveforms and Current Directions. Neuroscience 2019, 413, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Dileone, M.; Mordillo-Mateos, L.; Oliviero, A.; Foffani, G. Long-lasting effects of transcranial static magnetic field stimulation on motor cortex excitability. Brain Stimul. 2018, 11, 676–688. [Google Scholar] [CrossRef] [PubMed]
- Kirimoto, H.; Asao, A.; Tamaki, H.; Onishi, H. Non-invasive modulation of somatosensory evoked potentials by the application of static magnetic fields over the primary and supplementary motor cortices. Sci. Rep. 2016, 6, 34509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirimoto, H.; Tamaki, H.; Matsumoto, T.; Sugawara, K.; Suzuki, M.; Oyama, M.; Onishi, H. Effect of transcranial static magnetic field stimulation over the sensorimotor cortex on somatosensory evoked potentials in humans. Brain Stimul. 2014, 7, 836–840. [Google Scholar] [CrossRef] [PubMed]
- Kirimoto, H.; Tamaki, H.; Otsuru, N.; Yamashiro, K.; Onishi, H.; Nojima, I.; Oliviero, A. Transcranial Static Magnetic Field Stimulation over the Primary Motor Cortex Induces Plastic Changes in Cortical Nociceptive Processing. Front. Hum. Neurosci. 2018, 12, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pineda-Pardo, J.A.; Obeso, I.; Guida, P.; Dileone, M.; Strange, B.A.; Obeso, J.A.; Oliviero, A.; Foffani, G. Static magnetic field stimulation of the supplementary motor area modulates resting-state activity and motor behavior. Commun. Biol. 2019, 2, 397. [Google Scholar] [CrossRef]
- Tsuru, D.; Watanabe, T.; Chen, X.; Kubo, N.; Sunagawa, T.; Mima, T.; Kirimoto, H. The effects of transcranial static magnetic fields stimulation over the supplementary motor area on anticipatory postural adjustments. Neurosci. Lett. 2020, 723, 134863. [Google Scholar] [CrossRef]
- Landeros-Weisenberger, A.; Mantovani, A.; Motlagh, M.G.; de Alvarenga, P.G.; Katsovich, L.; Leckman, J.F.; Lisanby, S.H. Randomized Sham Controlled Double-blind Trial of Repetitive Transcranial Magnetic Stimulation for Adults with Severe Tourette Syndrome. Brain Stimul. 2015, 8, 574–581. [Google Scholar] [CrossRef] [Green Version]
- Shirota, Y.; Hamada, M.; Terao, Y.; Ohminami, S.; Tsutsumi, R.; Ugawa, Y.; Hanajima, R. Increased primary motor cortical excitability by a single-pulse transcranial magnetic stimulation over the supplementary motor area. Exp. Brain Res. 2012, 219, 339–349. [Google Scholar] [CrossRef]
- Shirota, Y.; Hanajima, R.; Ohminami, S.; Tsutsumi, R.; Ugawa, Y.; Terao, Y. Supplementary motor area plays a causal role in automatic inhibition of motor responses. Brain Stimul. 2019, 12, 1020–1026. [Google Scholar] [CrossRef]
- Vanier, M.; Gauthffir, L.; Lambert, J.; Pepin, E.P.; Robillard, A.; Dubouloz, C.J.; Gagnon, R.; Joannette, Y. Evaluation of Left Visuospatial Neglect: Norms and Discrimination Power of Two Tests. Neuropsychology 1990, 4, 87–96. [Google Scholar] [CrossRef]
- Mort, D.J.; Malhotra, P.; Mannan, S.K.; Rorden, C.; Pambakian, A.; Kennard, C.; Husain, M. The anatomy of visual neglect. Brain 2003, 126, 1986–1997. [Google Scholar] [CrossRef] [PubMed]
- Mort, D.J.; Kennard, C. Visual search and its disorders. Curr. Opin. Neurol. 2003, 16, 51–57. [Google Scholar] [CrossRef]
- Karnath, H.O.; Fruhmann Berger, M.; Kuker, W.; Rorden, C. The anatomy of spatial neglect based on voxelwise statistical analysis: A study of 140 patients. Cereb. Cortex 2004, 14, 1164–1172. [Google Scholar] [CrossRef] [PubMed]
- Husain, M.; Rorden, C. Non-spatially lateralized mechanisms in hemispatial neglect. Nat. Rev. Neurosci. 2003, 4, 26–36. [Google Scholar] [CrossRef] [PubMed]
- Yordanova, J.; Kolev, V.; Verleger, R.; Heide, W.; Grumbt, M.; Schurmann, M. Synchronization of fronto-parietal beta and theta networks as a signature of visual awareness in neglect. NeuroImage 2017, 146, 341–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.R.; Chun, M.H.; Kim, D.Y.; Lee, S.J. Effect of high- and low-frequency repetitive transcranial magnetic stimulation on visuospatial neglect in patients with acute stroke: A double-blind, sham-controlled trial. Arch. Phys. Med. Rehabil. 2013, 94, 803–807. [Google Scholar] [CrossRef]
- Oliveri, M. Brain stimulation procedures for treatment of contralesional spatial neglect. Restor. Neurol. Neurosci. 2011, 29, 421–425. [Google Scholar] [CrossRef]
- Salazar, A.P.S.; Vaz, P.G.; Marchese, R.R.; Stein, C.; Pinto, C.; Pagnussat, A.S. Noninvasive Brain Stimulation Improves Hemispatial Neglect After Stroke: A Systematic Review and Meta-Analysis. Arch. Phys. Med. Rehabil. 2018, 99, 355–366. [Google Scholar] [CrossRef]
- Koch, G.; Bonni, S.; Giacobbe, V.; Bucchi, G.; Basile, B.; Lupo, F.; Versace, V.; Bozzali, M.; Caltagirone, C. theta-burst stimulation of the left hemisphere accelerates recovery of hemispatial neglect. Neurology 2012, 78, 24–30. [Google Scholar] [CrossRef]
- Fan, J.; Li, Y.; Yang, Y.; Qu, Y.; Li, S. Efficacy of Noninvasive Brain Stimulation on Unilateral Neglect After Stroke: A Systematic Review and Meta-analysis. Am. J. Phys. Med. Rehabil. 2018, 97, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Kashiwada, Y.; Omichi, Y.; Kurimoto, S.; Shibata, H.; Miyake, Y.; Kirimoto, T.; Takaishi, Y. Conjugates of a secoiridoid glucoside with a phenolic glucoside from the flower buds of Lonicera japonica Thunb. Phytochemistry 2013, 96, 423–429. [Google Scholar] [CrossRef]
- Oliveri, M.; Bisiach, E.; Brighina, F.; Piazza, A.; La Bua, V.; Buffa, D.; Fierro, B. rTMS of the unaffected hemisphere transiently reduces contralesional visuospatial hemineglect. Neurology 2001, 57, 1338–1340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fierro, B.; Brighina, F.; Oliveri, M.; Piazza, A.; La Bua, V.; Buffa, D.; Bisiach, E. Contralateral neglect induced by right posterior parietal rTMS in healthy subjects. Neuroreport 2000, 11, 1519–1521. [Google Scholar] [CrossRef] [PubMed]
- Oldfield, R.C. The assessment and analysis of handedness: The Edinburgh inventory. Neuropsychologia 1971, 9, 97–113. [Google Scholar] [CrossRef]
- Moseley, P.; Mitrenga, K.J.; Ellison, A.; Fernyhough, C. Investigating the roles of medial prefrontal and superior temporal cortex in source monitoring. Neuropsychologia 2018, 120, 113–123. [Google Scholar] [CrossRef]
- You, D.S.; Kim, D.Y.; Chun, M.H.; Jung, S.E.; Park, S.J. Cathodal transcranial direct current stimulation of the right Wernicke’s area improves comprehension in subacute stroke patients. Brain Lang 2011, 119, 1–5. [Google Scholar] [CrossRef]
- Peirce, J.; Gray, J.R.; Simpson, S.; MacAskill, M.; Hochenberger, R.; Sogo, H.; Kastman, E.; Lindelov, J.K. PsychoPy2: Experiments in behavior made easy. Behav. Res. Methods 2019, 51, 195–203. [Google Scholar] [CrossRef] [Green Version]
- Bowers, D.; Heilman, K.M. Pseudoneglect: Effects of hemispace on a tactile line bisection task. Neuropsychologia 1980, 18, 491–498. [Google Scholar] [CrossRef]
- Friedrich, T.E.; Hunter, P.V.; Elias, L.J. The Trajectory of Pseudoneglect in Adults: A Systematic Review. Neuropsychol. Rev. 2018, 28, 436–452. [Google Scholar] [CrossRef] [Green Version]
- Jewell, G.; McCourt, M.E. Pseudoneglect: A review and meta-analysis of performance factors in line bisection tasks. Neuropsychologia 2000, 38, 93–110. [Google Scholar] [CrossRef]
- Brodie, E.E.; Pettigrew, L.E.L. Is left always right? Directional deviations in visual line bisection as a function of hand and initial scanning direction. Neuropsychologia 1996, 34, 467–470. [Google Scholar] [CrossRef]
- Dellatolas, G.; Vanluchene, J.; Coutin, T. Visual and motor components in simple line bisection: An investigation in normal adults. Cogn. Brain Res. 1996, 4, 49–56. [Google Scholar] [CrossRef]
- McCourt, M.E.; Mark, V.W.; Radonovich, K.J.; Willison, S.K.; Freeman, P. The effects of gender, menstrual phase and practice on the perceived location of the midsagittal plane. Neuropsychologia 1997, 35, 717–724. [Google Scholar] [CrossRef]
- McCourt, M.E.; Olafson, C. Cognitive and perceptual influences on visual line bisection: Psychophysical and chronometric analyses of pseudoneglect. Neuropsychologia 1997, 35, 369–380. [Google Scholar] [CrossRef]
- Manning, L.; Halligan, P.W.; Marshall, J.C. Individual Variation in Line Bisection—A Study of Normal Subjects with Application to the Interpretation of Visual Neglect. Neuropsychologia 1990, 28, 647–655. [Google Scholar] [CrossRef]
- Albuquerque, W.W.; Costa, R.M.; Fernandes Tde, S.; Porto, A.L. Evidences of the static magnetic field influence on cellular systems. Prog. Biophys. Mol. Biol. 2016, 121, 16–28. [Google Scholar] [CrossRef]
- Lu, X.W.; Du, L.; Kou, L.; Song, N.; Zhang, Y.J.; Wu, M.K.; Shen, J.F. Effects of moderate static magnetic fields on the voltage-gated sodium and calcium channel currents in trigeminal ganglion neurons. Electromagn. Biol. Med. 2015, 34, 285–292. [Google Scholar] [CrossRef]
- Rosen, A.D. Mechanism of action of moderate-intensity static magnetic fields on biological systems. Cell Biochem. Biophys. 2003, 39, 163–173. [Google Scholar] [CrossRef]
- Rosen, A.D. Inhibition of calcium channel activation in GH3 cells by static magnetic fields. Biochim. Biophys. Acta (BBA)-Biomembr. 1996, 1282, 149–155. [Google Scholar] [CrossRef] [Green Version]
- Hernando, A.; Galvez, F.; Garcia, M.A.; Soto-Leon, V.; Alonso-Bonilla, C.; Aguilar, J.; Oliviero, A. Effects of Moderate Static Magnetic Field on Neural Systems Is a Non-invasive Mechanical Stimulation of the Brain Possible Theoretically? Front. Neurosci. 2020, 14, 419. [Google Scholar] [CrossRef] [PubMed]
- Carrasco-Lopez, C.; Soto-Leon, V.; Cespedes, V.; Profice, P.; Strange, B.A.; Foffani, G.; Oliviero, A. Static Magnetic Field Stimulation over Parietal Cortex Enhances Somatosensory Detection in Humans. J. Neurosci. 2017, 37, 3840–3847. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Rosa, J.J.; Soto-Leon, V.; Real, P.; Carrasco-Lopez, C.; Foffani, G.; Strange, B.A.; Oliviero, A. Static Magnetic Field Stimulation over the Visual Cortex Increases Alpha Oscillations and Slows Visual Search in Humans. J. Neurosci. 2015, 35, 9182–9193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lozano-Soto, E.; Soto-Leon, V.; Sabbarese, S.; Ruiz-Alvarez, L.; Sanchez-Del-Rio, M.; Aguilar, J.; Strange, B.A.; Foffani, G.; Oliviero, A. Transcranial static magnetic field stimulation (tSMS) of the visual cortex decreases experimental photophobia. Cephalalgia Int. J. Headache 2018, 38, 1493–1497. [Google Scholar] [CrossRef]
- Heimrath, K.; Sproggel, A.; Repplinger, S.; Heinze, H.J.; Zaehle, T. Transcranial Static Magnetic Field Stimulation Over the Temporal Cortex Modulating the Right Ear Advantage in Dichotic Listening. Neuromodul. J. Int. Neuromodul. Soc. 2019. [Google Scholar] [CrossRef]
- Matsugi, A.; Okada, Y. Cerebellar transcranial static magnetic field stimulation transiently reduces cerebellar brain inhibition. Funct. Neurol. 2017, 32, 77–82. [Google Scholar] [CrossRef]
- Corbetta, M.; Shulman, G.L. Spatial neglect and attention networks. Annu. Rev. Neurosci. 2011, 34, 569–599. [Google Scholar] [CrossRef] [Green Version]
- Corbetta, M.; Kincade, M.J.; Lewis, C.; Snyder, A.Z.; Sapir, A. Neural basis and recovery of spatial attention deficits in spatial neglect. Nat. Neurosci. 2005, 8, 1603–1610. [Google Scholar] [CrossRef]
- He, B.J.; Snyder, A.Z.; Vincent, J.L.; Epstein, A.; Shulman, G.L.; Corbetta, M. Breakdown of functional connectivity in frontoparietal networks underlies behavioral deficits in spatial neglect. Neuron 2007, 53, 905–918. [Google Scholar] [CrossRef] [Green Version]
- Lunven, M.; Bartolomeo, P. Attention and spatial cognition: Neural and anatomical substrates of visual neglect. Ann. Phys. Rehabil. Med. 2017, 60, 124–129. [Google Scholar] [CrossRef]
- Rivadulla, C.; Foffani, G.; Oliviero, A. Magnetic field strength and reproducibility of neodymium magnets useful for transcranial static magnetic field stimulation of the human cortex. Neuromodulation Technol. Neural Interface 2014, 17, 438–441; discussion 441–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hashemi, S.; Abdolali, A. Three-dimensional analysis, modeling, and simulation of the effect of static magnetic fields on neurons. Bioelectromagnetics 2017, 38, 128–136. [Google Scholar] [CrossRef] [PubMed]
- Park, J.; Lee, C.; Lee, S.; Im, C.H. Comparison of magnetic field distributions generated by various permanent magnets for transcranial static magnetic stimulation: A simulation study. Comput. Biol. Med. 2019, 114, 103476. [Google Scholar] [CrossRef] [PubMed]
- Tharayil, J.J.; Goetz, S.M.; Bernabei, J.M.; Peterchev, A.V. Field Distribution of Transcranial Static Magnetic Stimulation in Realistic Human Head Model. Neuromodulation Technol. Neural Interface 2018, 21, 340–347. [Google Scholar] [CrossRef]
- Arene, N.U.; Hillis, A.E. Rehabilitation of unilateral spatial neglect and neuroimaging. Eur. Med. 2007, 43, 255–269. [Google Scholar]
- Ringman, J.M.; Saver, J.L.; Woolson, R.F.; Clarke, W.R.; Adams, H.P. Frequency, risk factors, anatomy, and course of unilateral neglect in an acute stroke cohort. Neurology 2004, 63, 468–474. [Google Scholar] [CrossRef]
- Pedersen, P.M.; Jorgensen, H.S.; Nakayama, H.; Raaschou, H.O.; Olsen, T.S. Hemineglect in acute stroke—Incidence and prognostic implications—The Copenhagen Stroke Study. Am. J. Phys. Med. Rehabil. 1997, 76, 122–127. [Google Scholar] [CrossRef] [PubMed]
- Karnath, H.O.; Rennig, J.; Johannsen, L.; Rorden, C. The anatomy underlying acute versus chronic spatial neglect: A longitudinal study. Brain 2011, 134, 903–912. [Google Scholar] [CrossRef]
- Bowen, A.; Lincoln, N.B.; Dewey, M.E. Spatial neglect: Is rehabilitation effective? Stroke 2002, 33, 2728–2729. [Google Scholar] [CrossRef]
- Kashiwagi, F.T.; El Dib, R.; Gomaa, H.; Gawish, N.; Suzumura, E.A.; da Silva, T.R.; Winckler, F.C.; de Souza, J.T.; Conforto, A.B.; Luvizutto, G.J.; et al. Noninvasive Brain Stimulations for Unilateral Spatial Neglect after Stroke: A Systematic Review and Meta-Analysis of Randomized and Nonrandomized Controlled Trials. Neural Plast 2018, 2018, 1638763. [Google Scholar] [CrossRef] [Green Version]
- Lefaucheur, J.P.; Antal, A.; Ayache, S.S.; Benninger, D.H.; Brunelin, J.; Cogiamanian, F.; Cotelli, M.; De Ridder, D.; Ferrucci, R.; Langguth, B.; et al. Evidence-based guidelines on the therapeutic use of transcranial direct current stimulation (tDCS). Clin. Neurophysiol. 2017, 128, 56–92. [Google Scholar] [CrossRef] [PubMed]
- Lefaucheur, J.P.; Andre-Obadia, N.; Antal, A.; Ayache, S.S.; Baeken, C.; Benninger, D.H.; Cantello, R.M.; Cincotta, M.; de Carvalho, M.; De Ridder, D.; et al. Evidence-based guidelines on the therapeutic use of repetitive transcranial magnetic stimulation (rTMS). Clin. Neurophysiol. 2014, 125, 2150–2206. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Score | Response |
|---|---|
| 0 | Correct response |
| +1 | Right segment of line #1 judged longer, or left and right segments of lines #2 and #3 judged equal (rightward bias) |
| −1 | Left segment of line #1 judged longer, or left and right segments of lines #4 and #5 judged equal (leftward bias) |
| +2 | Right segment of lines #2 and #3 judged longer (rightward bias) |
| −2 | Left segment of lines #4 and #5 judged longer (leftward bias) |
| Stim. Site | P4 | C6 | Sham | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Pre | Post | Post 10 | Pre | Post | Post 10 | Pre | Post | Post 10 |
| Total Score | −4.3 ± 1.2 | −6.1 ± 1.7 | −4.7 ± 1.5 | −6.8 ± 1.7 | −3.1 ± 1.4 *† | −4.8 ± 1.5 | −5.0 ± 1.6 | −4.4 ± 1.4 | −3.9 ± 1.6 |
| Total error | 8.3 ± 1.2 | 8.9 ± 1.4 | 7.7 ± 1.4 | 8.7 ± 1.5 | 5.4 ± 1.2 | 8.1 ± 1.2 | 7.6 ± 1.2 | 6.0 ± 1.5 | 6.0 ± 1.1 |
| −1 Error | 8.3 ± 0.8 | 8.9 ± 1.3 | 7.7 ± 1.3 | 7.4 ± 1.4 | 5.4 ± 1.1 | 8.1 ± 1.1 | 7.6 ± 1.2 | 6.0 ± 1.1 | 6.0 ± 1.1 |
| −2 Error | 0.1 ± 0.1 | 0.2 ± 0.1 | 0.0 ± 0.10 | 0.1 ± 0.1 | 0.1 ± 0.1 | 0.2 ± 0.1 | 0.1 ± 0.1 | 0.2 ± 0.1 | 0.1 ± 0.1 |
| +1 Error | 2.2 ± 0.9 | 1.4 ± 0.8 | 1.4 ± 0.8 | 0.8 ± 0.4 | 1.0 ± 0.4 | 1.2 ± 0.5 | 1.2 ± 0.5 | 0.9 ± 0.5 | 1.7 ± 0.5 |
| +2 Error | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.1 ± 0.1 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| Stim. Site | P4 | C6 | Sham | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Time | Pre | Post | Post 10 | Pre | Post | Post 10 | Pre | Post | Post 10 |
| Total Score | 3.7 ± 1.3 | 3.4 ± 1.3 | 3.1 ± 1.3 | 6.0 ± 0.8 | 3.0 ± 1.3 | 4.4 ± 1.7 | 5.0 ± 1.0 | 5.1 ± 1.1 | 5.7 ± 1.0 |
| Total error | 5.9 ± 0.9 | 6.1 ± 1.5 | 6.9 ± 1.4 | 7.9 ± 1.3 | 7.9 ± 1.8 | 6.9 ± 1.5 | 7.6 ± 1.4 | 6.0 ± 1.0 | 6.0 ± 1.1 |
| −1 Error | 1.0 ± 0.6 | 1.4 ± 0.7 | 1.9 ± 0.8 | 0.9 ± 0.3 | 2.4 ± 0.6 | 1.4 ± 0.4 | 1.1 ± 0.5 | 0.9 ± 0.4 | 1.0 ± 0.3 |
| −2 Error | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.0 ± 0.0 |
| +1 Error | 4.6 ± 0.9 | 4.6 ± 1.3 | 4.4 ± 1.3 | 6.6 ± 1.0 | 5.4 ± 1.5 | 5.9 ± 1.6 | 5.9 ± 1.0 | 6.0 ± 1.0 | 6.7 ± 1.0 |
| +2 Error | 0.0 ± 0.0 | 0.1 ± 0.1 | 0.0 ± 0.0 | 0.1 ± 0.1 | 0.0 ± 0.0 | 0.0 ± 0.0 | 0.1 ± 0.1 | 0.0 ± 0.0 | 0.0 ± 0.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kirimoto, H.; Watanabe, T.; Kubo, N.; Date, S.; Sunagawa, T.; Mima, T.; Ogata, K.; Nakazono, H.; Tobimatsu, S.; Oliviero, A. Influence of Static Magnetic Field Stimulation on the Accuracy of Tachystoscopically Presented Line Bisection. Brain Sci. 2020, 10, 1006. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10121006
Kirimoto H, Watanabe T, Kubo N, Date S, Sunagawa T, Mima T, Ogata K, Nakazono H, Tobimatsu S, Oliviero A. Influence of Static Magnetic Field Stimulation on the Accuracy of Tachystoscopically Presented Line Bisection. Brain Sciences. 2020; 10(12):1006. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10121006
Chicago/Turabian StyleKirimoto, Hikari, Tatsunori Watanabe, Nami Kubo, Shota Date, Toru Sunagawa, Tatsuya Mima, Katsuya Ogata, Hisato Nakazono, Shozo Tobimatsu, and Antonio Oliviero. 2020. "Influence of Static Magnetic Field Stimulation on the Accuracy of Tachystoscopically Presented Line Bisection" Brain Sciences 10, no. 12: 1006. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci10121006