
Investigating Brain Microstructural Alterations in Type 1 and Type 2 Diabetes Using Diffusion Tensor Imaging: A Systematic Review

 ,
,  , , and
, , and
Abstract
:1. Introduction
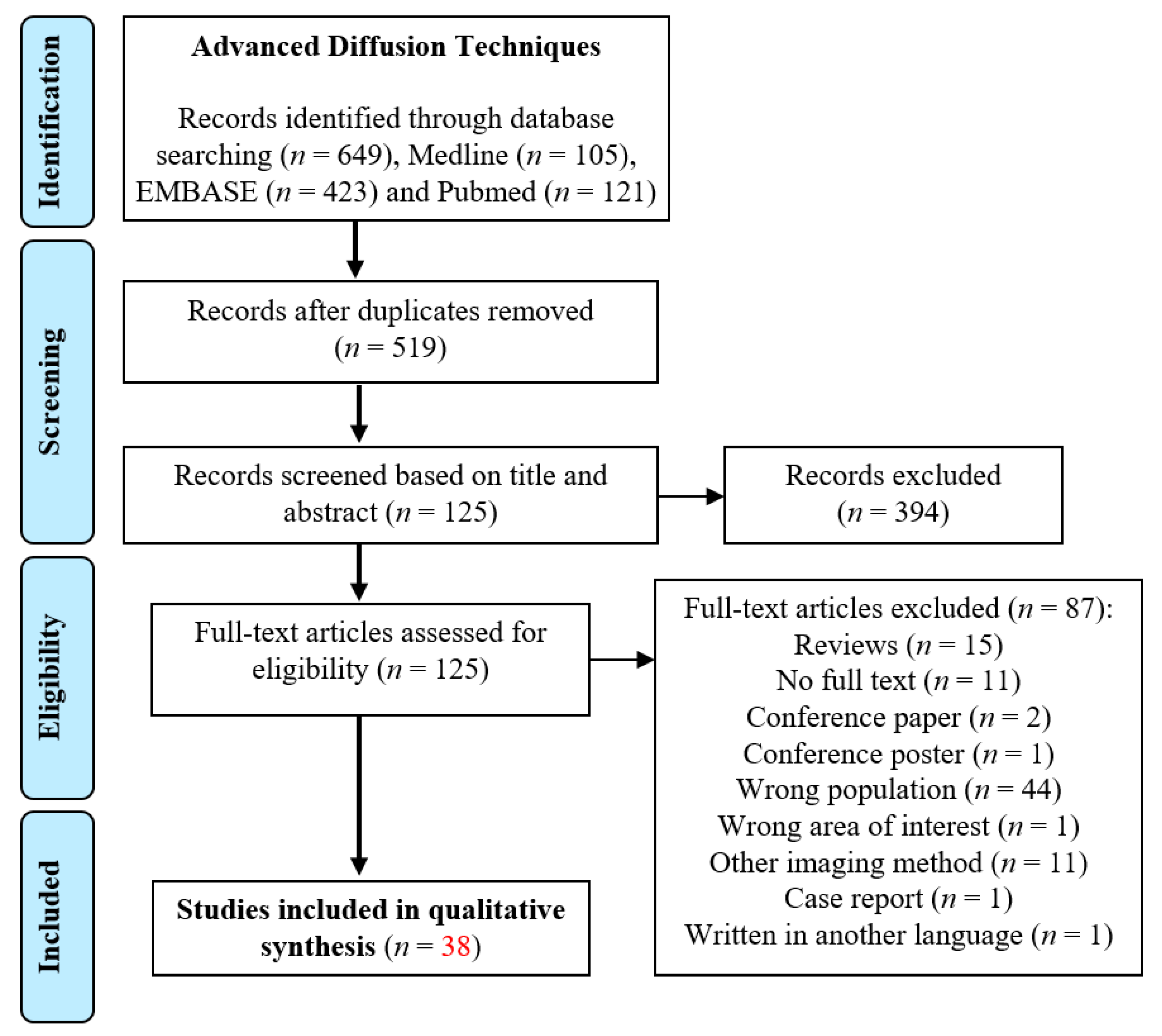
2. Materials and Methods
2.1. Data Sources and Search Strategy
2.2. Study Selection and Inclusion Criteria
2.3. Data Extraction and Management
3. Results
3.1. Overview of Reviewed DTI-T1DM Studies
3.1.1. Between-Group Differences: Microstructural Alterations in T1DM
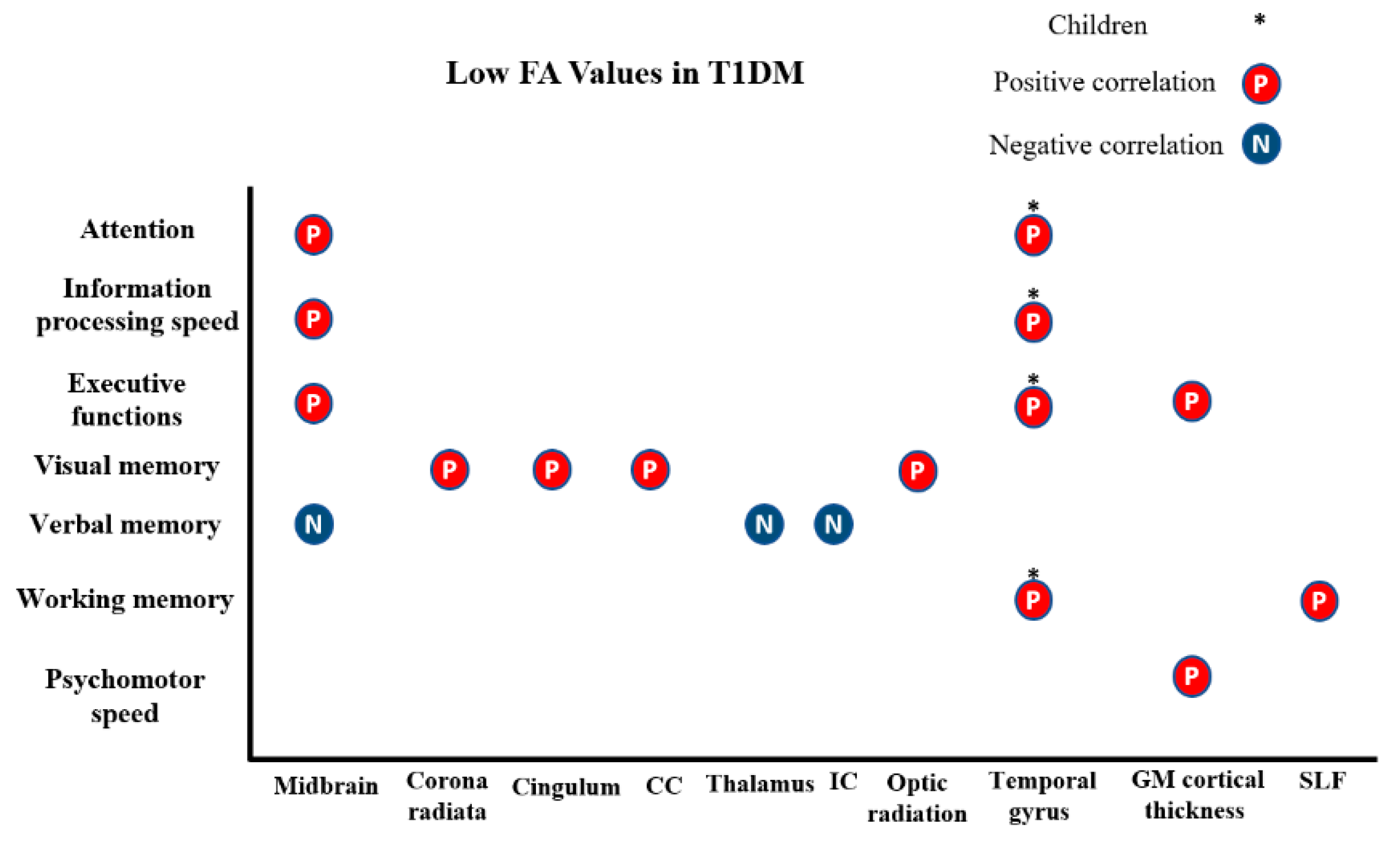
3.1.2. Microstructural and Cognitive Abnormalities in T1DM
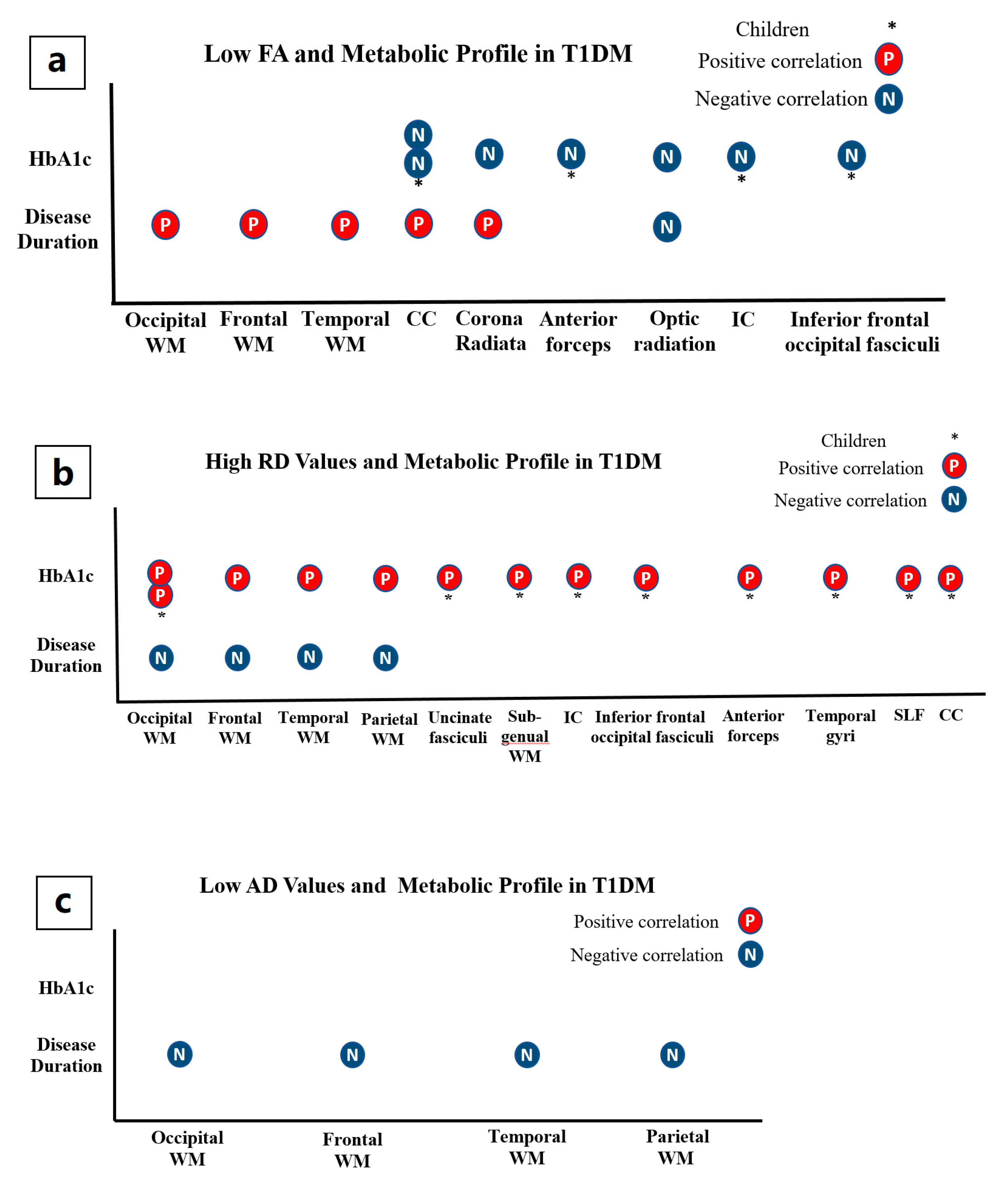
3.1.3. Microstructural Alterations and Metabolic Profile in T1DM
3.2. Overview of Reviewed DTI-T2DM Studies
3.2.1. Between-Group Differences: Microstructural Alterations in T2DM
3.2.2. Microstructural and Cognitive Abnormalities in T2DM
3.2.3. Microstructural Alterations and Metabolic Profile in T2DM
4. Discussion
4.1. T1DM Patients versus Healthy Controls
4.2. T2DM Patients versus Healthy Controls
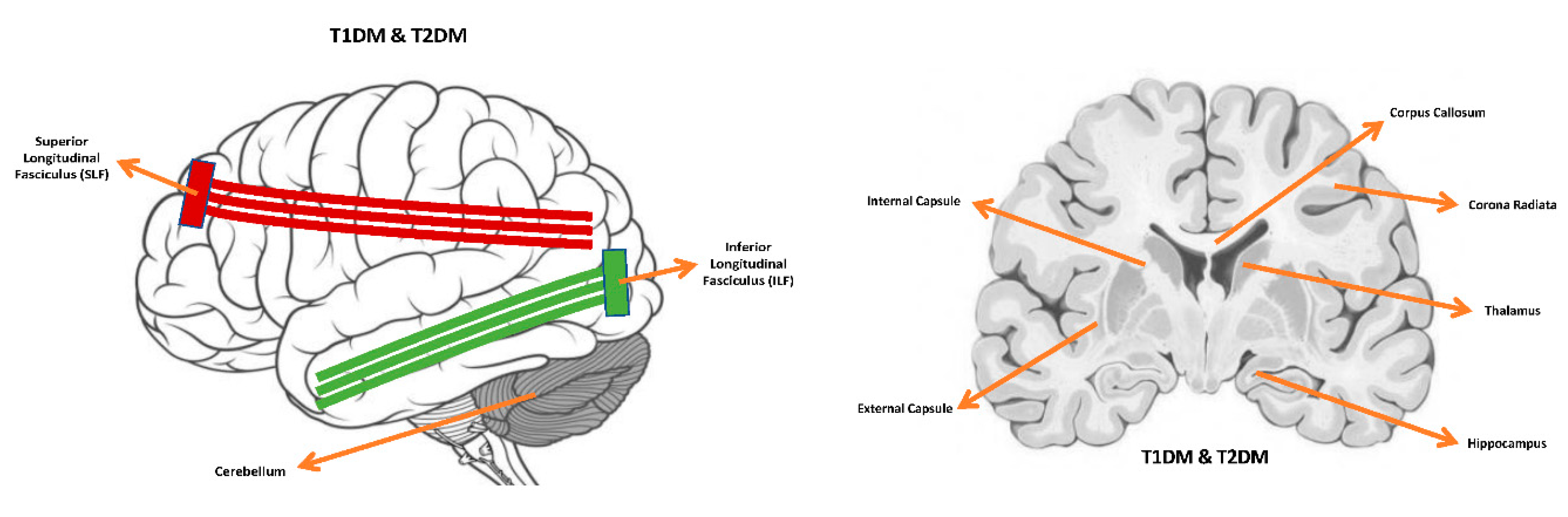
4.3. Common Microstructural Alterations, Cognitive Deficits and Comorbidities
4.4. Multi-Shell Diffusion Imaging Models
4.5. Limitations
4.6. Future Directions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ozougwu, O. The pathogenesis and pathophysiology of type 1 and type 2 diabetes mellitus. J. Physiol. Pathophysiol. 2013, 4, 46–57. [Google Scholar] [CrossRef] [Green Version]
- Kodl, C.T.; Franc, D.T.; Rao, J.P.; Anderson, F.S.; Thomas, W.; Mueller, B.A. Diffusion tensor imaging identifies deficits in white matter microstructure in subjects with type 1 diabetes that correlate with reduced neurocognitive function. Diabetes 2008, 57, 3083–3089. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biessels, G.J.; Deary, I.J.; Ryan, C.M. Cognition and diabetes: A lifespan perspective. Lancet Neurol. 2008, 7, 184–190. [Google Scholar] [CrossRef]
- Van Duinkerken, E.; Schoonheim, M.M.; Ijzerman, R.G.; Klein, M.; Ryan, C.M.; Moll, A.C. Diffusion tensor imaging in type 1 diabetes: Decreased white matter integrity relates to cognitive functions. Diabetologia 2012, 55, 1218–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brands, A.M.A.; Biessels, G.J.; De Haan, E.H.F.; Kappelle, L.J.; Kessels, R.P.C. The effects of type 1 diabetes on cognitive performance: A meta-analysis. Diabetes Care 2005, 28, 726–735. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biessels, G.J.; Reijmer, Y.D. Brain changes underlying cognitive dysfunction in diabetes: What can we learn from MRI? Diabetes 2014, 63, 2244–2252. [Google Scholar] [CrossRef] [Green Version]
- Reijmer, Y.D.; Brundel, M.; de Bresser, J.; Kappelle, L.J.; Leemans, A.; Biessels, G.J. Microstructural white matter abnormalities and cognitive functioning in type 2 diabetes: A diffusion tensor imaging study. Diabetes Care 2013, 36, 137–144. [Google Scholar] [CrossRef] [Green Version]
- Yau, P.L.; Javier, D.C.; Ryan, C.M.; Tsui, W.H.; Ardekani, B.A.; Ten, S. Preliminary evidence for brain complications in obese adolescents with type 2 diabetes mellitus. Diabetologia 2010, 53, 2298–2306. [Google Scholar] [CrossRef] [Green Version]
- Groeneveld, O.; Reijmer, Y.; Heinen, R.; Kuijf, H.; Koekkoek, P.; Janssen, J. Brain imaging correlates of mild cognitive impairment and early dementia in patients with type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1253–1260. [Google Scholar] [CrossRef]
- Basser, P.J.; Mattiello, J.; LeBihan, D. MR diffusion tensor spectroscopy and imaging. Biophys. J. 1994, 66, 259–267. [Google Scholar] [CrossRef] [Green Version]
- Pierpaoli, C.; Jezzard, P.; Basser, P.J.; Barnett, A.; Di Chiro, G. Diffusion tensor MR imaging of the human brain. Radiology 1996, 201, 637–648. [Google Scholar] [CrossRef] [PubMed]
- Fox, L.A.; Hershey, T.; Mauras, N.; Arbeláez, A.M.; Tamborlane, W.V.; Buckingham, B. Persistence of abnormalities in white matter in children with type 1 diabetes. Diabetologia 2018, 61, 1538–1547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walhovd, K.B.; Johansen-Berg, H.; Káradóttir, R.T. Unraveling the secrets of white matter—Bridging the gap between cellular, animal and human imaging studies. Neuroscience 2014, 276, 2–13. [Google Scholar] [CrossRef] [Green Version]
- Sanjari Moghaddam, H.; Ghazi Sherbaf, F.; Aarabi, M.H. Brain microstructural abnormalities in type 2 diabetes mellitus: A systematic review of diffusion tensor imaging studies. Front. Neuroendocrinol. 2019, 55, 100782. [Google Scholar] [CrossRef] [PubMed]
- Beaulieu, C. The basis of anisotropic water diffusion in the nervous system—A technical review. NMR Biomed. 2002, 15, 435–455. [Google Scholar] [CrossRef] [PubMed]
- Jelescu, I.O.; Zurek, M.; Winters, K.V.; Veraart, J.; Rajaratnam, A.; Kim, N.S. In vivo quantification of demyelination and recovery using compartment-specific diffusion MRI metrics validated by electron microscopy. NeuroImage 2016, 132, 104–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.K.; Sun, S.W.; Ramsbottom, M.J.; Chang, C.; Russell, J.; Cross, A.H. Dysmyelination revealed through MRI as increased radial (but unchanged axial) diffusion of water. Neuroimage 2002, 17, 1429–1436. [Google Scholar] [CrossRef] [PubMed]
- Wheeler-Kingshott, C.A.M.; Cercignani, M. About “axial” and “radial” diffusivities. Magn. Reson. Med. 2009, 61, 1255–1260. [Google Scholar] [CrossRef]
- Jeurissen, B.; Leemans, A.; Tournier, J.D.; Jones, D.K.; Sijbers, J. Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum. Brain Mapp. 2013, 34, 2747–2766. [Google Scholar] [CrossRef]
- Aye, T.; Barnea-Goraly, N.; Ambler, C.; Hoang, S.; Schleifer, K.; Park, Y. White matter structural differences in young children with type 1 diabetes: A diffusion tensor imaging study. Diabetes Care 2012, 35, 2167–2173. [Google Scholar] [CrossRef] [Green Version]
- Barnea-Goraly, N.; Raman, M.; Mazaika, P.; Marzelli, M.; Hershey, T.; Weinzimer, S.A. Alterations in white matter structure in young children with type 1 diabetes. Diabetes Care 2014, 37, 332–340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Toprak, H.; Yetis, H.; Alkan, A.; Filiz, M.; Kurtcan, S.; Aralasmak, A. Relationships of DTI findings with neurocognitive dysfunction in children with Type 1 diabetes mellitus. Br. J. Radiol. 2016, 89, 20150680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmed, H.H.; Azzam, H.M.E.; Farid, S.M.; Abdelmaksoud, A.A.; Rassem, I.M.M. Neurocognitive profile and diffusion tensor imaging in pediatric patients with type 1 diabetes mellitus. Middle East Curr. Psychiatry 2014, 21, 205–211. [Google Scholar] [CrossRef]
- Franc, D.T.; Kod, C.T.; Mueller, B.A.; Muetze, R.L.; Lim, K.O.; Seaquist, E.R. High connectivity between reduced cortical thickness and disrupted white matter tracts in long-standing type 1 diabetes. Diabetes 2011, 60, 315–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, S.; Kim, J.; Musen, G.; Renshaw, P.F.; Hwang, J.; Bolo, N.R. Prefronto-Temporal White Matter Microstructural Alterations 20 years after the Diagnosis of Type 1 Diabetes Mellitus HHS Public Access. Pediatr. Diabetes 2018, 19, 478–485. [Google Scholar] [CrossRef]
- Antenor-Dorsey, J.A.V.; Meyer, E.; Rutlin, J.; Perantie, D.C.; White, N.H.; Arbelaez, A.M. White matter microstructural integrity in youth with type 1 diabetes. Diabetes 2013, 62, 581–589. [Google Scholar] [CrossRef] [Green Version]
- Atlas of Anatomy|Telencephalon. Available online: https://www.winkingskull.com/Image/Toc/16/54002 (accessed on 14 January 2021).
- Rofey, D.L.; Arslanian, S.A.; El Nokali, N.E.; Verstynen, T.; Watt, J.C.; Black, J.J. Brain volume and white matter in youth with type 2 diabetes compared to obese and normal weight, non-diabetic peers: A pilot study. Int. J. Dev. Neurosci. 2015, 46, 88–91. [Google Scholar] [CrossRef]
- Nouwen, A.; Chambers, A.; Chechlacz, M.; Higgs, S.; Blissett, J.; Barrett, T.G. Microstructural abnormalities in white and gray matter in obese adolescents with and without type 2 diabetes. Neuroimage Clin. 2017, 16, 43–51. [Google Scholar] [CrossRef]
- Yau, P.L.; Javier, D.; Tsui, W.; Sweat, V.; Bruehl, H.; Borod, J.C. Emotional and neutral declarative memory impairments and associated white matter microstructural abnormalities in adults with type 2 diabetes. Psychiatry Res. 2009, 174, 223–230. [Google Scholar] [CrossRef] [Green Version]
- Zhang, A.; Ajilore, O.; Zhan, L.; Gadelkarim, J.; Korthauer, L.; Yang, S. White matter tract integrity of anterior limb of internal capsule in major depression and type 2 diabetes. Neuropsychopharmacology 2013, 38, 1451–1459. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Wang, Y.; Wang, J.; Zhou, X.; Shu, N.; Wang, Y. White matter integrity disruptions associated with cognitive impairments in type 2 diabetic patients. Diabetes 2014, 63, 3596–3605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, X.; Jiaerken, Y.; Xu, X.; Jackson, A.; Huang, P.; Yang, L. Abnormal corpus callosum induced by diabetes impairs sensorimotor connectivity in patients after acute stroke. Eur. Radiol. 2019, 29, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Tan, X.; Fang, P.; An, J.; Lin, H.; Liang, Y.; Shen, W. Micro-structural white matter abnormalities in type 2 diabetic patients: A DTI study using TBSS analysis. Neuroradiology 2016, 58, 1209–1216. [Google Scholar] [CrossRef] [PubMed]
- van Bloemendaal, L.; Ijzerman, R.G.; Ten Kulve, J.S.; Barkhof, F.; Diamant, M.; Veltman, D.J. Alterations in white matter volume and integrity in obesity and type 2 diabetes. Metab. Brain Dis. 2016, 31, 621–629. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.J.; Yu, J.H.; Shin, M.S.; Shin, Y.W.; Kim, M.S. Hyperglycemia Reduces Efficiency of Brain Networks in Subjects with Type 2 Diabetes. PLoS ONE 2016, 11, e0157268. [Google Scholar] [CrossRef] [Green Version]
- Reijmer, Y.D.; Leemans, A.; Brundel, M.; Kappelle, L.J.; Biessels, G.J.; Utrecht Vascular Cognitive Impairment Study Group. Disruption of the cerebral white matter network is related to slowing of information processing speed in patients with type 2 diabetes. Diabetes 2013, 62, 2112–2115. [Google Scholar] [CrossRef] [Green Version]
- Zhang, J.; Liu, Z.; Li, Z.; Wang, Y.; Chen, Y.; Li, X. Disrupted White Matter Network and Cognitive Decline in Type 2 Diabetes Patients. J. Alzheimer’s Dis. 2016, 53, 185–195. [Google Scholar] [CrossRef]
- Yau, P.L.; Hempel, R.; Tirsi, A.; Convit, A. Cerebral white matter and retinal arterial health in hypertension and type 2 diabetes mellitus. Int. J. Hypertens. 2013, 2013, 329602. [Google Scholar] [CrossRef]
- Xiong, Y.; Sui, Y.; Xu, Z.; Zhang, Q.; Karaman, M.M.; Cai, K. A Diffusion Tensor Imaging Study on White Matter Abnormalities in Patients with Type 2 Diabetes Using Tract-Based Spatial Statistics. AJNR Am. J. Neuroradiol. 2016, 37, 1462–1469. [Google Scholar] [CrossRef] [Green Version]
- Hsu, J.L.; Chen, Y.L.; Leu, J.G.; Jaw, F.S.; Lee, C.H.; Tsai, Y.F. Microstructural white matter abnormalities in type 2 diabetes mellitus: A diffusion tensor imaging study. Neuroimage 2012, 59, 1098–1105. [Google Scholar] [CrossRef]
- Zhang, Y.; Cao, Y.; Xie, Y.; Liu, L.; Qin, W.; Lu, S. Altered brain structural topological properties in type 2 diabetes mellitus patients without complications. J. Diabetes 2019, 11, 129–138. [Google Scholar] [CrossRef] [PubMed]
- Falvey, C.M.; Rosano, C.; Simonsick, E.M.; Harris, T.; Strotmeyer, E.S.; Satterfield, S. Macro-andmicrostructural magnetic resonance imaging indices associated with diabetes among community-dwelling older adults. Diabetes Care 2013, 36, 677–682. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, Y.; Zhang, Y.; Qin, W.; Lu, S.; Ni, C.; Zhang, Q. White Matter Microstructural Abnormalities in Type 2 Diabetes Mellitus: A Diffusional Kurtosis Imaging Analysis. AJNR Am. J. Neuroradiol. 2017, 38, 617–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yau, P.L.; Kluger, A.; Borod, J.C.; Convit, A. Neural substrates of verbal memory impairments in adults with type 2 diabetes mellitus. J. Clin. Exp. Neuropsychol. Off. J. Int. Neuropsychol. Soc. 2014, 36, 74–87. [Google Scholar] [CrossRef] [Green Version]
- Yoon, S.; Cho, H.; Kim, J.; Lee, D.W.; Kim, G.H.; Hong, Y.S. Brain changes in overweight/obese and normal-weight adults with type 2 diabetes mellitus. Diabetologia 2017, 60, 1207–1217. [Google Scholar] [CrossRef] [Green Version]
- van Bussel, F.C.; Backes, W.H.; Hofman, P.A.; van Boxtel, M.P.; Schram, M.T.; Stehouwer, C.D. Altered Hippocampal White Matter Connectivity in Type 2 Diabetes Mellitus and Memory Decrements. J. Neuroendocrinol. 2016, 28, 12366. [Google Scholar] [CrossRef]
- Xiong, Y.; Sui, Y.; Zhang, S.; Zhou, X.J.; Yang, S.; Fan, Y. Brain microstructural alterations in type 2 diabetes: Diffusion kurtosis imaging provides added value to diffusion tensor imaging. Eur. Radiol. 2019, 29, 1997–2008. [Google Scholar] [CrossRef]
- Xiong, Y.; Zhang, S.; Shi, J.; Fan, Y.; Zhang, Q.; Zhu, W. Application of neurite orientation dispersion and density imaging to characterize brain microstructural abnormalities in type-2 diabetics with mild cognitive impairment. J. Magn. Reson. Imaging 2019, 50, 889–898. [Google Scholar] [CrossRef]
- Fang, P.; An, J.; Tan, X.; Zeng, L.L.; Shen, H.; Qiu, S. Changes in the cerebellar and cerebro-cerebellar circuit in type 2 diabetes. Brain Res. Bull. 2017, 130, 95–100. [Google Scholar] [CrossRef]
- Hoogenboom, W.S.; Marder, T.J.; Flores, V.L.; Huisman, S.; Eaton, H.P.; Schneiderman, J.S. Cerebral white matter integrity and resting-state functional connectivity in middle-aged patients with type 2 diabetes. Diabetes 2014, 63, 728–738. [Google Scholar] [CrossRef] [Green Version]
- Raffield, L.M.; Brenes, G.A.; Cox, A.J.; Freedman, B.I.; Hugenschmidt, C.E.; Hsu, F.C. Associations between anxiety and depression symptoms and cognitive testing and neuroimaging in type 2 diabetes. J. Diabetes Its Complicat. 2016, 30, 143–149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- López Fernández, M.L.; Barrio Castellanos, R.; Portellano Pérez, J.A.; Martínez Arias, R. Executive functions in children with type 1 diabetes using the neuropsychology test. An. Pediatr. 2013, 78, 88–93. [Google Scholar] [CrossRef] [PubMed]
- Northam, E.A.; Rankins, D.; Lin, A.; Wellard, R.M.; Pell, G.S.; Finch, S.J. Central nervous system function in youth with type 1 diabetes 12 years after disease onset. Diabetes Care 2009, 32, 445–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Northam, E.A.; Anderson, P.J.; Jacobs, R.; Hughes, M.; Warne, G.L.; Werther, G.A. Neuropsychological profiles of children with type 1 diabetes 6 years after disease onset. Diabetes Care 2001, 24, 1541–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geijselaers, S.L.C.; Sep, S.J.S.; Stehouwer, C.D.A.; Biessels, G.J. Glucose regulation, cognition, and brain MRI in type 2 diabetes: A systematic review. Lancet Diabetes Endocrinol. 2015, 3, 75–89. [Google Scholar] [CrossRef]
- Feinkohl, I.; Price, J.F.; Strachan, M.W.J.; Frier, B.M. The impact of diabetes on cognitive decline: Potential vascular, metabolic, and psychosocial risk factors. Alzheimer’s Res. Ther. 2015, 7, 46. [Google Scholar] [CrossRef] [Green Version]
- McCrimmon, R.J.; Ryan, C.M.; Frier, B.M. Diabetes and cognitive dysfunction. Lancet 2012, 379, 2291–2299. [Google Scholar] [CrossRef]
- Bruehl, H.; Sweat, V.; Tirsi, A.; Shah, B.; Convit, A. Obese Adolescents with Type 2 Diabetes Mellitus Have Hippocampal and Frontal Lobe Volume Reductions. Neurosci. Med. 2011, 2, 34. [Google Scholar] [CrossRef] [Green Version]
- Yang, S.; Ajilore, O.; Wu, M.; Lamar, M.; Kumar, A. Impaired macromolecular protein pools in fronto-striato-thalamic circuits in type 2 diabetes revealed by magnetization transfer imaging. Diabetes 2015, 64, 183–192. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Schneider, T.; Wheeler-Kingshott, C.A.; Alexander, D.C. NODDI: Practical in vivo neurite orientation dispersion and density imaging of the human brain. Neuroimage 2012, 61, 1000–1016. [Google Scholar] [CrossRef]
- Tournier, J.D.; Mori, S.; Leemans, A. Diffusion tensor imaging and beyond. Magn. Reson. Med. 2011, 65, 1532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basser, P.J.; Jones, D.K. Diffusion-tensor MRI: Theory, experimental design and data analysis—A technical review. NMR Biomed. 2002, 15, 456–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Selection and Inclusion Criteria (a) | |
|---|---|
| Inclusion | Exclusion |
|
|
| |
| |
| Participants Selection and Inclusion Criteria (b) | |
| Inclusion | Exclusion |
|
|
| |
| |
| Microstructural Alterations in Type 1 Diabetes Mellitus (T1DM) Patients | ||||
|---|---|---|---|---|
| Region | ↓ FA (Fractional Anisotropy) | ↓ MD (Mean Diffusivity) | ↑ RD (Radial Diffusivity) | ↓ AD (Axial Diffusivity) |
| Corpus callosum | van Duinkerken et al. 2012 (with/without microangiopathy), Kodl et al. 2008, Yoon et al. 2018 [5,7,8]. | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. | Antenor-Dorsey et al. 2013, van Duinkerken et al. 2012 (with/without microangiopathy), Tandy et al. 2012 [1,4,8]. |
| Corona radiata | van Duinkerken et al. 2012 (without microangiopathy), Kodl et al. 2008, Franc et al. 2011, Toprak et al. 2016 [2,7,8]. | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. | -- |
| Thalamic radiation | van Duinkerken et al. 2012 (with microangiopathy) [8]. | -- | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. |
| Forceps minor and major | van Duinkerken et al. 2012 (with microangiopathy) [8]. | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. |
| Superior longitudinal fasciculi (SLF) | van Duinkerken et al. 2012 (with microangiopathy), Ahmed et al. 2014, Yoon et al. 2018 [5,8,9]. | -- | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8]. |
| Optic radiation | Ahmed et al. 2014, Kodl et al. 2008, Franc et al. 2011 [3,7,9]. | -- | -- | -- |
| Putamen | Toprak et al. 2016 [2] | -- | -- | -- |
| Inferior longitudinal fasciculus (ILF) | Toprak et al. 2016 [2] | -- | -- | -- |
| Thalamus | Toprak et al. 2016 [2] | Antenor-Dorsey et al. 2013 [4] | -- | Antenor-Dorsey et al. 2013, Tandy et al. 2012 [1,4] |
| Hippocampus | Toprak et al. 2016 [2] | -- | -- | -- |
| Inferior frontal-occipital fasciculus | Yoon et al. 2018 [5] | -- | van Duinkerken et al. 2012 (with/without microangiopathy) [8] | -- |
| Superior parietal lobule | Antenor-Dorsey et al. 2013 [4] | -- | Antenor-Dorsey et al. 2013 [4] | Antenor-Dorsey et al. 2013 [4] |
| Cerebellum | -- | -- | Antenor-Dorsey et al. 2013 [4] | Antenor-Dorsey et al. 2013 [4] |
| Internal capsules | -- | -- | -- | Antenor-Dorsey et al. 2013; Tandy et al. 2012 [1,4] |
| External capsules | -- | -- | -- | Antenor-Dorsey et al. 2013 [4] |
| Cerebral peduncle | -- | -- | -- | Antenor-Dorsey et al. 2013 [4] |
| Cingulate gyrus | -- | -- | -- | Tandy et al. 2012 [1] |
| Superior temporal gyrus | -- | -- | -- | Tandy et al. 2012 [1] |
| White matter (widespread changes) | Barnea-Goraly et al. 2014 [6] | -- | Barnea-Goraly et al. 2014 (reduced RD with longer disease duration, and increased RD with younger age at disease onset) [6]. | Barnea-Goraly et al. 2014 [6] |
| Microstructural Alterations in T2DM Patients | ||||
|---|---|---|---|---|
| Region | ↓ FA | ↑ MD | ↑ RD | ↑ AD |
| Corpus callosum | Yau et al. 2013; Zhang et al. 2014; Tan et al. 2016; Zhang et al. 2016; Nouwen et al. 2017; Yoon et al. 2017; Xie et al. 2017; Sun et al. 2018; Yu et al. 2018, Kim et al. 2016 [10,13,17,18,19,23,26,28,29,36]. | Reijmer et al. 2013; Zhang et al. 2014; Xie et al. 2017; Sun et al. 2018; Xiong et al. 2018 [13,18,20,28,38]. | Zhang et al. 2014; Nouwen et al. 2017; Xie et al. 2017; Sun et al. 2018; Yu et al. 2018 [13,18,23,28,29]. | Reijmer et al. 2013; Xie et al. 2017; Sun et al. 2018 [13,20,28]. |
| Corona radiata | Zhang et al. 2014; Yoon et al. 2017; Xiong et al. 2018; Sun et al. 2018 [10,13,18,38]. | Zhang et al. 2014; Xiong et al. 2016; Sun et al. 2018; Xiong et al. 2018 [13,18,23,28,38]. | Zhang et al. 2014; Xiong et al. 2016; Sun et al. 2018; Nouwen et al. 2017 [13,16,18,23]. | Xiong et al. 2016; Sun et al. 2018 [13,16]. |
| Cingulum | Yau et al. 2010; Hoogenboom et al. 2014; Zhang et al. 2014; Tan et al. 2016; Nouwen et al. 2017; Yoon et al. 2017; Sun et al. 2018; Xion et al. 2018; Zhang et al. 2016; Xiong et al. 2016 [10,13,16,18,23,26,30,31,36,38]. | Falvey et al. 2012; Zhang et al. 2014; Sun et al. 2018; Xiong et al. 2018 [13,16,18,34]. | Zhang et al. 2014; Xiong et al. 2016; Nouwen et al. 2017; Sun et al. 2018 [13,16,18,23]. | Tan et al. 2016; Xiong et al. 2016; Sun et al. 2018 [13,16,26]. |
| Uncinate Fasciculus | Reijmer et al. 2013; Hoogenboom et al. 2014; Zhang et al. 2014; Tan et al. 2016; Nouwen et al. 2017; Yoon et al. 2017; Xiong et al. 2018 [10,18,23,25,26,30,38]. | Reijmer et al. 2013; Tan et al. 2016; Xiong et al. 2018 [20,26,38]. | Reijmer et al. 2013; Zhang et al. 2014; Nouwen et al. 2017 [16,18,23]. | Reijmer et al. 2013 [20] |
| Superior longitudinal fasciculi (SLF) | Yau et al. 2014; Zhang et al. 2014; Tan et al. 2016; Zhang et al. 2016 [18,22,26,36]. | Reijmer et al. 2013; Zhang et al. 2014 [18,20]. | Reijmer et al. 2013; Zhang et al. 2014 [18,20]. | Reijmer et al. 2013; Bloemendaal et al. 2016 [20,33]. |
| Inferior longitudinal fasciculus (ILF) | Zhang et al. 2014; Kim et al. 2016; Tan et al. 2016; Yoon et al. 2017 [10,17,18,26]. | Reijmer et al. 2013; Tan et al. 2016 [20,26]. | Reijmer et al. 2013 [20] | Reijmer et al. 2013 [20] |
| Thalamus | Zhang et al. 2014; Zhang et al. 2016; Tan et al. 2016; Xiong et al. 2016; Fang et al. 2017; Nouwen et al. 2017; Yoon et al. 2017; Sun et al. 2018 [10,12,13,16,18,23,26,36]. | Zhang et al. 2014; Tan et al. 2016 [18,26] | Zhang et al. 2014; Xiong et al. 2016; Nouwen et al. 2017 [16,18,23]. | Tan et al. 2016; Xiong et al. 2016; Sun et al. 2018 [13,16,26]. |
| Corticospinal tract | Xiong et al. 2016; Sun et al. 2018; Nouwen et al. 2017; Yoon et al. 2017 [10,13,16,23]. | -- | Nouwen et al. 2017 [23] | Bloemendaal et al. 2016 [33] |
| Inferior frontal-occipital fasciculus | Zhang et al. 2014; Zhang et al. 2016; Kim et al. 2016; Nouwen et al. 2017; Yoon et al. 2017 [10,17,18,23,36]. | -- | Nouwen et al. 2017 [23] | Bloemendaal et al. 2016 [33] |
| Cerebellum | Yau et al. 2013; Yoon et al. 2017; Tan et al. 2017; Fang et al. 2017; Xiong et al. 2016 [10,12,16,19,26]. | Yau et al. 2014; Hsu et al. 2012 [14,22]. | Xiong et al. 2016; Hsu et al. 2012 [14,16]. | Xiong et al. 2016; Hsu et al. 2012 [14,16]. |
| Internal capsules | Yau et al. 2013; Zhang et al. 2013; Zhang et al. 2014; Kim et al. 2016; Xiong et al. 2016; Nouwen et al. 2017; Sun et al. 2018 [13,16,17,18,19,23,32]. | Zhang et al. 2014; Xiong et al. 2016; Xiong et al. 2018 [16,18,28,38]. | Zhang et al. 2013; Zhang et al. 2014; Xiong et al. 2016; Nouwen et al. 2017 [16,18,23,32]. | Xiong et al. 2016; Sun et al. 2018 [13,16] |
| External capsules | Yau et al. 2013; Zhang et al. 2014; Kim et al. 2016; Xiong et al. 2016; Nouwen et al. 2017; Yoon et al. 2017; Sun et al. 2018; Xion et al. 2018 [10,13,16,18,19,23,38]. | Zhang et al. 2014; Xiong et al. 2016; Xie et al. 2017; Xiong et al. 2018 [16,18,28,38]. | Xie et al. 2017; Xiong et al. 2016; Nouwen et al. 2017 [16,23,28]. | Xiong et al. 2016; Xie et al. 2017; Sun et al. 2018 [13,16,23,28]. |
| Fornix | Zhang et al. 2014; Zhang et al. 2016; Tan et al. 2016; Xiong et al. 2016; Fang et al. 2017; Nouwen et al. 2017; Yoon et al. 2017; Sun et al. 2018 [10,12,13,16,18,23,26,36]. | Zhang et al. 2014; Tan et al. 2016 [18,26]. | Zhang et al. 2014; Xiong et al. 2016; Nouwen et al. 2017 [16,18,23]. | Tan et al. 2016; Xiong et al. 2016; Sun et al. 2018 [13,16,26] |
| Hippocampus | Van Bussel et al. 2016, Jian-Hui Zhang et al. 2016, Xiong et al. 2016, Xiong et al. 2018, Falvey et al. 2013 [16,34,35,36,38]. | Van Bussel et al. 2016, Xiong et al. 2018, Falvey et al. 2013 [34,35,38]. | -- | -- |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alotaibi, A.; Tench, C.; Stevenson, R.; Felmban, G.; Altokhis, A.; Aldhebaib, A.; Dineen, R.A.; Constantinescu, C.S. Investigating Brain Microstructural Alterations in Type 1 and Type 2 Diabetes Using Diffusion Tensor Imaging: A Systematic Review. Brain Sci. 2021, 11, 140. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020140
Alotaibi A, Tench C, Stevenson R, Felmban G, Altokhis A, Aldhebaib A, Dineen RA, Constantinescu CS. Investigating Brain Microstructural Alterations in Type 1 and Type 2 Diabetes Using Diffusion Tensor Imaging: A Systematic Review. Brain Sciences. 2021; 11(2):140. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020140
Chicago/Turabian StyleAlotaibi, Abdulmajeed, Christopher Tench, Rebecca Stevenson, Ghadah Felmban, Amjad Altokhis, Ali Aldhebaib, Rob A. Dineen, and Cris S. Constantinescu. 2021. "Investigating Brain Microstructural Alterations in Type 1 and Type 2 Diabetes Using Diffusion Tensor Imaging: A Systematic Review" Brain Sciences 11, no. 2: 140. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020140