
Which Target Temperature for Post-Anoxic Brain Injury? A Systematic Review from “Real Life” Studies

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
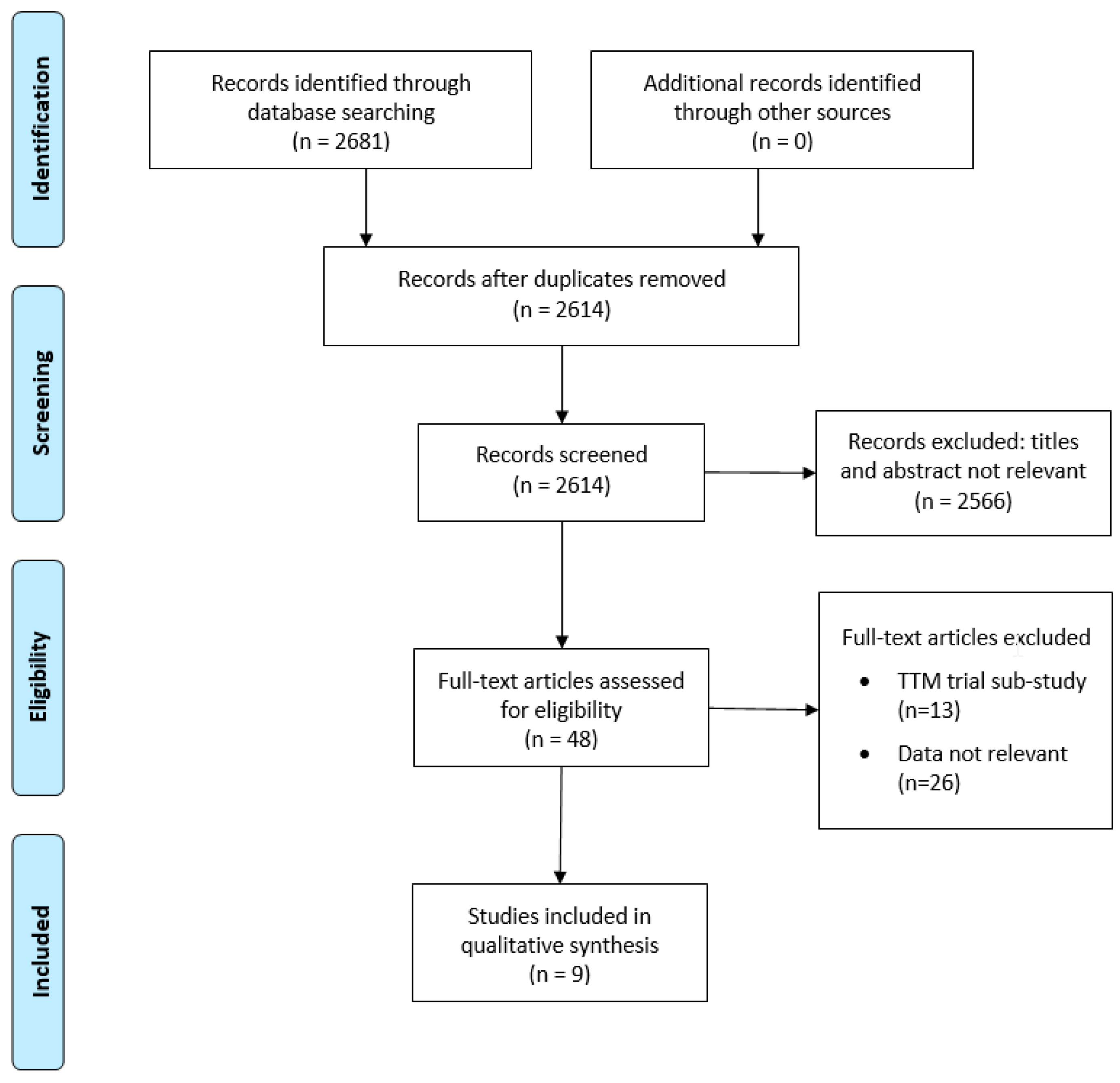
2.1. Search Strategy and Study Selection
2.2. Data Sources and Search Strategies
2.3. Study Screening and Selection
2.4. Appraisal of Study Quality
2.5. Statistical Analyses
3. Results
Unfavorable Neurological Outcome and Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Nolan, J.P.; Berg, R.A.; Andersen, L.W.; Bhanji, F.; Chan, P.S.; Donnino, M.W.; Lim, S.H.; Ma, M.H.-M.; Nadkarni, V.M.; Starks, M.A.; et al. Cardiac Arrest and Cardiopulmonary Resuscitation Outcome Reports: Update of the Utstein Resuscitation Registry Template for In-Hospital Cardiac Arrest: A Consensus Report From a Task Force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian and New Zealand Council on Resuscitation, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Southern Africa, Resuscitation Council of Asia). Resuscitation 2019, 144, 166–177. [Google Scholar]
- Sandroni, C.; D’Arrigo, S.; Cacciola, S.; Hoedemaekers, C.W.E.; Kamps, M.J.A.; Oddo, M.; Taccone, F.S.; Di Rocco, A.; Meijer, F.J.A.; Westhall, E.; et al. Prediction of poor neurological outcome in comatose survivors of cardiac arrest: A systematic review. Intensiv. Care Med. 2020, 46, 1803–1851. [Google Scholar] [CrossRef] [PubMed]
- Lilja, G.; Nielsen, N.; Friberg, H.; Horn, J.; Kjaergaard, J.; Nilsson, L.A.F.; Pellis, T.; Wetterslev, J.; Wise, M.P.; Bosch, F.; et al. Cognitive Function in Survivors of Out-of-Hospital Cardiac Arrest After Target Temperature Management at 33 °C Versus 36 °C. Circulation 2015, 131, 1340–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taccone, F.S.; Crippa, I.A.; Scolletta, S.; Dell’Anna, A.M. Neuroprotective strategies and neuroprognostication after cardiac arrest. Best Pract. Res. Clin. Anaesthesiol. 2015, 29, 451–464. [Google Scholar] [CrossRef] [PubMed]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of Comatose Survivors of Out-of-Hospital Cardiac Arrest with Induced Hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef] [PubMed]
- HACA Investigatoris. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Lascarrou, J.B.; Merdji, H.; Le Gouge, A.; Colin, G.; Grillet, G.; Girardie, P.; Coupez, E.; Dequin, P.F.; Cariou, A.; Boulain, T.; et al. Targeted Temperature Management for Cardiac Arrest with Nonshockable Rhythm. N. Engl. J. Med. 2019, 381, 2327–2337. [Google Scholar] [CrossRef]
- Panchal, A.R.; Bartos, J.A.; Cabañas, J.G.; Donnino, M.W.; Drennan, I.R.; Hirsch, K.G.; Kudenchuk, P.J.; Kurz, M.C.; Lavonas, E.J.; Morley, P.T.; et al. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2020, 142 (Suppl. 2), S366–S468. [Google Scholar] [CrossRef]
- Olai, H.; Thornéus, G.; Watson, H.; MacLeod, M.; Rhodes, J.; Friberg, H.; Nielsen, N.; Cronberg, T.; Deierborg, T. Meta-analysis of targeted temperature management in animal models of cardiac arrest. Intensiv. Care Med. Exp. 2020, 8, 3–16. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted Temperature Management at 33°C versus 36°C after Cardiac Arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, N. The Target Temperature for Post Cardiac Arrest Patients Should Be 36 °C. Crit. Care Med. 2017, 45, 1552–1554. [Google Scholar] [CrossRef] [PubMed]
- Abazi, L.; Awad, A.; Nordberg, P.; Jonsson, M.; Taccone, F.S.; Wickerts, C.J.; Svensson, L.; Hollenberg, J.; Ringh, M.; Forsberg, S. Long-term survival in out-of-hospital cardiac arrest patients treated with targeted temperature control at 33 °C or 36 °C: A national registry study. Resuscitation 2019, 143, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Bray, J.E.; Stub, D.; Bloom, J.E.; Segan, L.; Mitra, B.; Smith, K.; Finn, J.; Bernard, S. Changing target temperature from 33 °C to 36 °C in the ICU management of out-of-hospital cardiac arrest: A before and after study. Resuscitation 2017, 113, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Bradley, S.M.; Liu, W.; McNally, B.; Vellano, K.; Henry, T.D.; Mooney, M.R.; Burke, M.N.; Brilakis, E.S.; Grunwald, G.K.; Adhaduk, M.; et al. Temporal Trends in the Use of Therapeutic Hypothermia for Out-of-Hospital Cardiac Arrest. JAMA Netw. Open 2018, 1, e184511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lopez-De-Sa, E.; Juarez, M.; Armada, E.; Sanchez-Salado, J.C.; Sanchez, P.L.; Loma-Osorio, P.; Sionis, A.; Monedero, M.C.; Martinez-Sellés, M.; Martín-Benitez, J.C.; et al. A multicentre randomized pilot trial on the effectiveness of different levels of cooling in comatose survivors of out-of-hospital cardiac arrest: The FROST-I trial. Intensiv. Care Med. 2018, 44, 1807–1815. [Google Scholar] [CrossRef]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomized studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Casamento, A.; Minson, A.; Radford, S.; Mårtensson, J.; Ridgeon, E.; Young, P.J.; Bellomo, R. A comparison of therapeutic hypothermia and strict therapeutic normothermia after cardiac arrest. Resuscitation 2016, 106, 83–88. [Google Scholar] [CrossRef]
- Callaway, C.W.; Coppler, P.J.; Faro, J.; Puyana, J.S.; Solanki, P.; Dezfulian, C.; Doshi, A.A.; Elmer, J.; Frisch, A.; Guyette, F.X.; et al. Association of Initial Illness Severity and Outcomes After Cardiac Arrest With Targeted Temperature Management at 36 °C or 33 °C. JAMA Netw. Open 2020, 3, e208215. [Google Scholar] [CrossRef]
- Cragun, B.N.; Philp, F.H.; O’Neill, J.; Noorbakhsh, M.R.; Tindall, R.P.; Philp, A.S.; Ditillo, M.F. Therapeutic Hypothermia and Targeted Temperature Management for Traumatic Arrest and Surgical Patients. Ther. Hypothermia Temp. Manag. 2019, 9, 156–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Düggelin, R.; Maggiorini, M.; Voigtsberger, S.; Schwarz, U.; Hilty, M.P. Increased protocol adherence and safety during controlled normothermia as compared to hypothermia after cardiac arrest. J. Crit. Care 2020. Epub ahead of Print. [Google Scholar] [CrossRef]
- Johnson, N.J.; Danielson, K.R.; Counts, C.R.; Ruark, K.; Scruggs, S.; Hough, C.L.; Maynard, C.; Sayre, M.R.; Carlbom, D.J. Targeted Temperature Management at 33 Versus 36 Degrees: A Retrospective Cohort Study. Crit. Care Med. 2020, 48, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Johnsson, J.; Wahlström, J.; Dankiewicz, J.; Annborn, M.; Agarwal, S.; Dupont , A.; Forsberg, S.; Friberg, H.; Hand, R.; Hirsch, K.G.; et al. Functional outcomes associated with varying levels of targeted temperature management after out-of-hospital cardiac arrest - An INTCAR2 registry analysis. Resuscitation 2020, 146, 229–236. [Google Scholar] [CrossRef] [Green Version]
- Okazaki, T.; Hifumi, T.; Kawakita, K.; Kuroda, Y. Targeted temperature management guided by the severity of hyperlactatemia for out-of-hospital cardiac arrest patients: A post hoc analysis of a nationwide, multicenter prospective registry. Ann. Intensiv. Care 2019, 9, 127. [Google Scholar] [CrossRef]
- Deye, N.; Vincent, F.; Michel, P.; Ehrmann, S.; da Silva, D.; Piagnerelli, M.; Kimmoun, A.; Hamzaoui, O.; Lacherade, J.-C.; de Jonghe, B.; et al. Changes in cardiac arrest patients’ temperature management after the 2013 “TTM” trial: Results from an international survey. Ann. Intensiv. Care 2016, 6, 4. [Google Scholar] [CrossRef] [Green Version]
- Storm, C.; Nee, J.; Sunde, K.; Holzer, M.; Hubner, P.; Taccone, F.S.; Friberg, H.; Lopez-De-Sa, E.; Cariou, A.; Schefold, J.C.; et al. A survey on general and temperature management of post cardiac arrest patients in large teaching and university hospitals in 14 European countries—The SPAME trial results. Resuscitation 2017, 116, 84–90. [Google Scholar] [CrossRef]
- Salter, R.; Bailey, M.; Bellomo, R.; Eastwood, G.; Goodwin, A.; Nielsen, N.; Pilcher, D.; Nichol, A.; Saxena, M.; Shehabi, Y.; et al. Changes in Temperature Management of Cardiac Arrest Patients Following Publication of the Target Temperature Management Trial. Crit. Care Med. 2018, 46, 1722–1730. [Google Scholar] [CrossRef]
- Harmon, M.B.; Hodiamont, C.; Dankiewicz, J.; Nielsen, N.; Schultz, M.J.; Horn, J.; Friberg, H.; Juffermans, N.P. Microbiological profile of nosocomial infections following cardiac arrest: Insights from the targeted temperature management (TTM) trial. Resuscitation 2020, 148, 227–233. [Google Scholar] [CrossRef] [Green Version]
- Rundgren, M.; Ullén, S.; Morgan, M.; Glover, G.; Cranshaw, J.; Al-Subaie, N.; Walden, A.P.; Joannidis, M.; Ostermann, M.; Dankiewicz, J.; et al. Renal function after out-of-hospital cardiac arrest; the influence of temperature management and coronary angiography, a post hoc study of the target temperature management trial. Crit. Care 2019, 23, 163. [Google Scholar] [CrossRef] [Green Version]
- Lybeck, A.; Friberg, H.; Aneman, A.; Hassager, C.; Horn, J.; Kjaergaard, J.; Kuiper, M.; Nielsen, N.; Ullén, S.; Wise, M.P.; et al. Prognostic significance of clinical seizures after cardiac arrest and target temperature management. Resuscitation 2017, 114, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Borgquist, O.; Wise, M.P.; Nielsen, N.; Al-Subaie, N.; Cranshaw, J.; Cronberg, T.; Glover, G.; Hassager, C.; Kjaergaard, J.; Kuiper, M.; et al. Dysglycemia, Glycemic Variability, and Outcome After Cardiac Arrest and Temperature Management at 33 °C and 36 °C. Crit. Care Med. 2017, 45, 1337–1343. [Google Scholar] [CrossRef] [PubMed]
- Bro-Jeppesen, J.; Annborn, M.; Hassager, C.; Wise, M.P.; Pelosi, P.; Nielsen, N.; Erlinge, D.; Wanscher, M.; Friberg, H.; Kjaergaard, J.; et al. Hemodynamics and vasopressor support during targeted temperature management at 33 °C Versus 36 °C after out-of-hospital cardiac arrest: A post hoc study of the target temperature management trial. Crit. Care Med. 2015, 43, 318–327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lybeck, A.; Cronberg, T.; Aneman, A.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjærgaard, J.; Kuiper, M.; Wanscher, M.; Stammet, P.; et al. Time to awakening after cardiac arrest and the association with target temperature management. Resuscitation 2018, 126, 166–171. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Friberg, H.; TTM Trial Steering Group. Targeted Temperature Management after Cardiac Arrest. N. Engl. J. Med. 2014, 370, 1360. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author, Year [Ref] | Type of Study | Number | OHCA | IHCA | VF/VT | Mortality Assessment | Definition UO | UO Assessment |
|---|---|---|---|---|---|---|---|---|
| Abazi, 2019 [12] | R | 1038 | YES | NO | 673 | 30-day 6-month | NR | NR |
| Bray, 2017 [13] | R | 76 | YES | NO | 76 | ICU Hospital | CPC 3–5 | Hospital |
| Callaway, 2020 [20] | R | 1319 | YES | YES | 369 | Hospital | CPC 4–5 CPC 3–5 | Hospital |
| Casamento, 2016 [19] | R | 138 | YES | NR | 86 | ICU Hospital | NR | NR |
| Cragun, 2018 [21] | R | 32 | YES * | YES ** | NR | Hospital | Unable to follow commands | Hospital |
| Düggelin, 2020 [22] | R | 133 | YES | YES | 83 | ICU Hospital | CPC 3–5 | Hospital |
| Johnson, 2020 [23] | R | 453 | YES | NO | 173 | Hospital | CPC 3–5 | Hospital |
| Kleissner, 2019 [24] | R | 1710 | YES | NO | 866 | Hospital | CPC 3–5 | Hospital |
| Okazaki, 2019 [25] | R | 435 | YES | NO | 235 | 30-day | CPC 3–5 | 30-day |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minini, A.; Annoni, F.; Peluso, L.; Bogossian, E.G.; Creteur, J.; Taccone, F.S. Which Target Temperature for Post-Anoxic Brain Injury? A Systematic Review from “Real Life” Studies. Brain Sci. 2021, 11, 186. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020186
Minini A, Annoni F, Peluso L, Bogossian EG, Creteur J, Taccone FS. Which Target Temperature for Post-Anoxic Brain Injury? A Systematic Review from “Real Life” Studies. Brain Sciences. 2021; 11(2):186. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020186
Chicago/Turabian StyleMinini, Andrea, Filippo Annoni, Lorenzo Peluso, Elisa Gouvêa Bogossian, Jacques Creteur, and Fabio Silvio Taccone. 2021. "Which Target Temperature for Post-Anoxic Brain Injury? A Systematic Review from “Real Life” Studies" Brain Sciences 11, no. 2: 186. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11020186