
Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Assessment
2.3. Treatment
2.4. Statistical Analysis
3. Results
3.1. Baseline Assessment
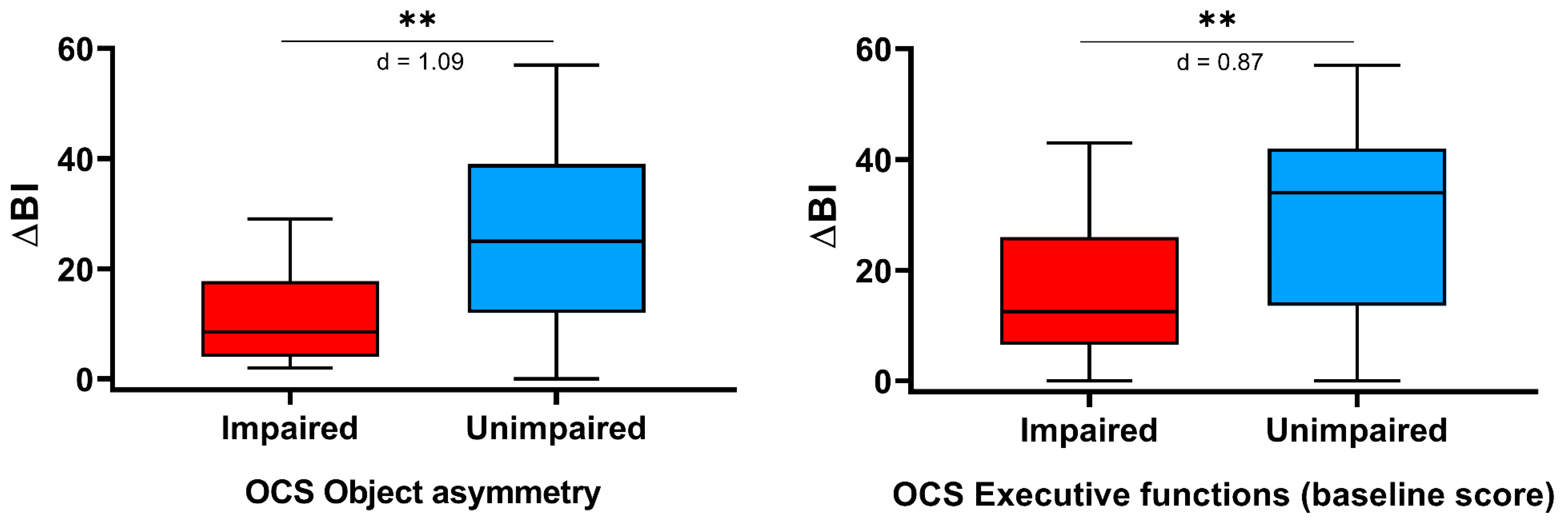
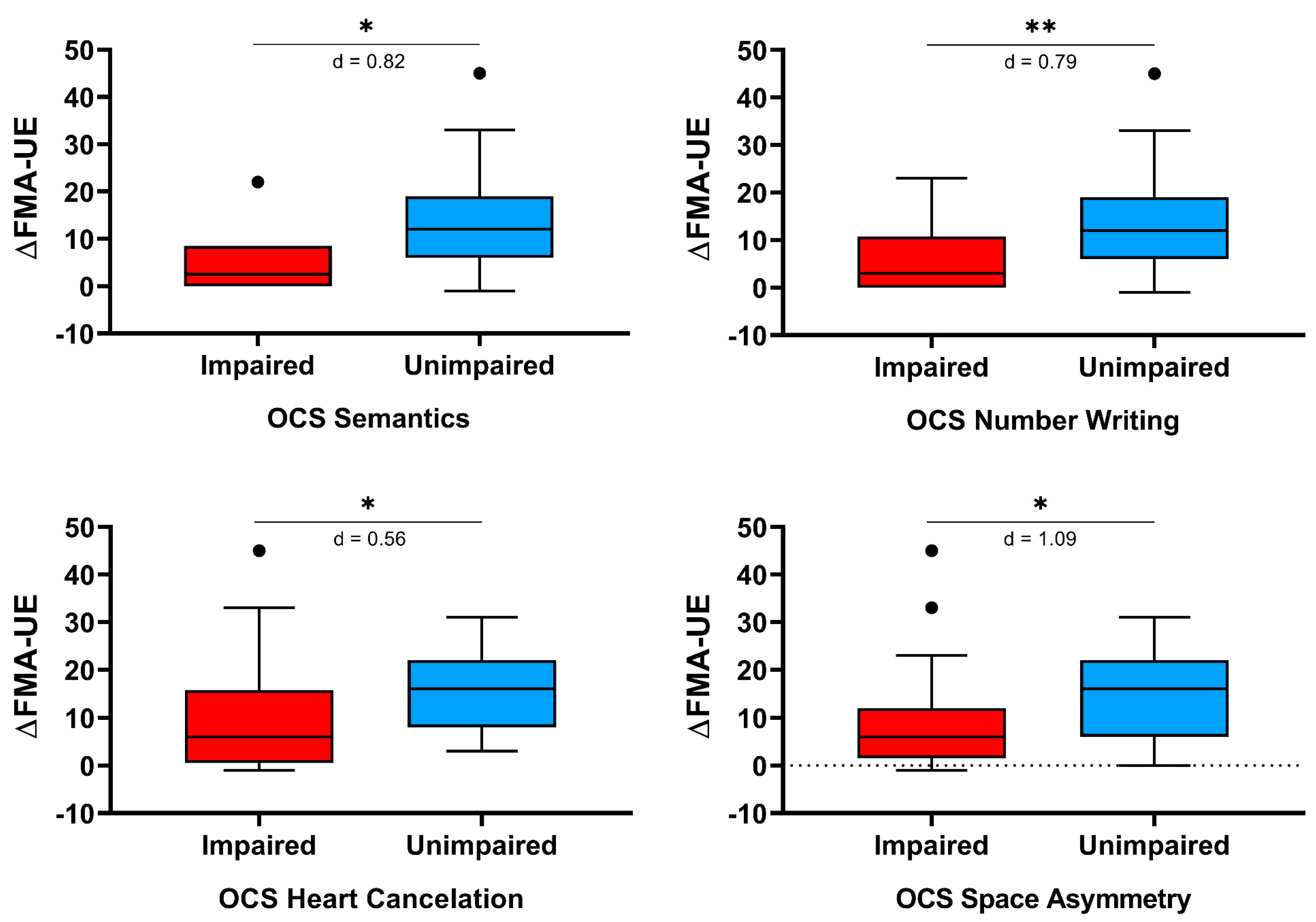
3.2. Rehabilitation Outcomes
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gassert, R.; Dietz, V. Rehabilitation robots for the treatment of sensorimotor deficits: A neurophysiological perspective. J. Neuroeng. Rehabil. 2018, 15, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 9, CD006876. [Google Scholar] [CrossRef]
- Rodgers, H.; Bosomworth, H.; Krebs, H.I.; van Wijck, F.; Howel, D.; Wilson, N.; Aird, L.; Alvarado, N.; Andole, S.; Cohen, D.L.; et al. Robot assisted training for the upper limb after stroke (RATULS): A multicentre randomised controlled trial. Lancet 2019, 394, 51–62. [Google Scholar] [CrossRef] [Green Version]
- Aprile, I.; Germanotta, M.; Cruciani, A.; Loreti, S.; Pecchioli, C.; Cecchi, F.; Montesano, A.; Galeri, S.; Diverio, M.; Falsini, C.; et al. Upper Limb Robotic Rehabilitation after Stroke: A Multicenter, Randomized Clinical Trial. J. Neurol. Phys. Ther. 2020, 44, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Nys, G.M.S.; Van Zandvoort, M.J.E.; De Kort, P.L.M.; Van Der Worp, H.B.; Jansen, B.P.W.; Algra, A.; De Haan, E.H.F.; Kappelle, L.J. The prognostic value of domain-specific cognitive abilities in acute first-ever stroke. Neurology 2005, 64, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Leśniak, M.; Bak, T.; Czepiel, W.; Seniów, J.; Członkowska, A. Frequency and prognostic value of cognitive disorders in stroke patients. Dement. Geriatr. Cogn. Disord. 2008, 26, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Gottesman, R.F.; Hillis, A.E. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol. 2010, 9, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Pendlebury, S.T.; Rothwell, P.M. Prevalence, incidence, and factors associated with pre-stroke and post-stroke dementia: A systematic review and meta-analysis. Lancet Neurol. 2009, 8, 1006–1018. [Google Scholar] [CrossRef]
- Pollock, A.; Farmer, S.E.; Brady, M.C.; Langhorne, P.; Mead, G.E.; Mehrholz, J.; van Wijck, F. Interventions for improving upper limb function after stroke. Cochrane Database Syst. Rev. 2014, 2014, CD010820. [Google Scholar] [CrossRef] [PubMed]
- Lamb, F.; Anderson, J.; Saling, M.; Dewey, H. Predictors of subjective cognitive complaint in postacute older adult stroke patients. Arch. Phys. Med. Rehabil. 2013, 94, 1747–1752. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Leys, D.; Esquenazi, A. The interaction between neuropsychological and motor deficits in patients after stroke. Neurology 2013, 80, S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Everard, G.J.; Ajana, K.; Dehem, S.B.; Stoquart, G.G.; Edwards, M.G.; Lejeune, T.M. Is cognition considered in post-stroke upper limb robot-assisted therapy trials? A brief systematic review. Int. J. Rehabil. Res. 2020, 43, 195–198. [Google Scholar] [CrossRef] [PubMed]
- Leem, M.J.; Kim, G.S.; Kim, K.H.; Yi, T.I.; Moon, H.I. Predictors of functional and motor outcomes following upper limb robot-assisted therapy after stroke. Int. J. Rehabil. Res. 2019, 42, 223–228. [Google Scholar] [CrossRef] [PubMed]
- Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Mastrorosa, A.; Castelli, L.; Monteleone, S.; Redolfi, A.; Galeri, S.; Germanotta, M. Robotic Rehabilitation: An Opportunity to Improve Cognitive Functions in Subjects With Stroke. An Explorative Study. Front. Neurol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Demeyere, N.; Riddoch, M.J.; Slavkova, E.D.; Bickerton, W.L.; Humphreys, G.W. The Oxford Cognitive Screen (OCS): Validation of a stroke-specific short cognitive screening tool. Psychol. Assess. 2015, 27, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Mancuso, M.; Varalta, V.; Sardella, L.; Capitani, D.; Zoccolotti, P.; Antonucci, G.; The Italian OCS Group; Abbruzzese, L.; Fonte, C.; La Monica, G.V.; et al. Italian normative data for a stroke specific cognitive screening tool: The Oxford Cognitive Screen (OCS). Neurol. Sci. 2016, 37, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar] [PubMed]
- W Bohannon, R. Motricity Index Scores are Valid Indicators of Paretic Upper Extremity Strength Following Stroke. J. Phys. Ther. Sci. 1999, 11, 59–61. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Jakob, I.; Kollreider, A.; Germanotta, M.; Benetti, F.; Cruciani, A.; Padua, L.; Aprile, I. Robotic and Sensor Technology for Upper Limb Rehabilitation. PMR 2018, 10, S189–S197. [Google Scholar] [CrossRef] [Green Version]
- Aprile, I.; Cruciani, A.; Germanotta, M.; Gower, V.; Pecchioli, C.; Cattaneo, D.; Vannetti, F.; Padua, L.; Gramatica, F. Upper Limb Robotics in Rehabilitation: An Approach to Select the Devices, Based on Rehabilitation Aims, and Their Evaluation in a Feasibility Study. Appl. Sci. 2019, 9, 3920. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, J.; Hayward, K.S.; Dancause, N.; Lannin, N.A.; Ward, N.S.; Nudo, R.J.; Farrin, A.; Churilov, L.; Boyd, L.A.; Jones, T.A.; et al. A stroke recovery trial development framework: Consensus-based core recommendations from the Second Stroke Recovery and Rehabilitation Roundtable. Int. J. Stroke 2019, 14, 792–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Loetscher, T.; Potter, K.J.; Wong, D.; das Nair, R. Cognitive rehabilitation for attention deficits following stroke. Cochrane Database Syst. Rev. 2019, 2019, CD002842. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.W.; Wu, C.Y.; Lin, K.C.; Yao, G.; Wu, K.Y.; Chang, Y.J. Dose-response relationship of robot-assisted stroke motor rehabilitation: The impact of initial motor status. Stroke 2012, 43, 2729–2734. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Entry Characteristics | Mean (SD) or N (%) |
|---|---|
| Age | 68.4 (12.4) |
| Sex (men/women) | 29 (56.9%)/22 (43.1%) |
| Dominant side (Right/Left) | 47 (92.2%)/4 (7.8%) |
| Education years | 10.2 (3.8) |
| Stroke type (Ischemic/Hemorrhagic) | 36 (70.6%)/15 (29.4%) |
| Affected side (Right/Left) | 23 (45.1%)/28 (54.9%) |
| Days from index stroke to enrollment | 74.6 (41.3) |
| Language impairment | 11 (21.6%) |
| Neglect syndrome | 10 (19.6%) |
| Fugl-Meyer Assessment for Upper Extremity | 21.5 (18.1) |
| Motricity Index | 37.3 (27.9) |
| Modified Barthel Index | 40.3 (18.3) |
| Domain | Task | Whole Group | Right Hemiparesis | Left Hemiparesis | p | |||
|---|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | |||
| Language | Picture naming | 20 | 39.2% | 12 | 52.2% | 8 | 28.6% | 0.149 |
| Semantics | 6 | 11.8% | 4 | 17.4% | 2 | 7.1% | 0.390 | |
| Sentence reading | 24 | 47.1% | 15 | 65.2% | 9 | 32.1% | 0.026 | |
| Memory | Orientation | 13 | 25.5% | 7 | 30.4% | 6 | 21.4% | 0.529 |
| Recall and recognition | 21 | 41.2% | 14 | 60.9% | 7 | 25.0% | 0.012 | |
| Episodic memory | 28 | 54.9% | 14 | 60.9% | 14 | 50.0% | 0.573 | |
| Number | Number writing | 14 | 27.5% | 10 | 43.5% | 4 | 14.3% | 0.029 |
| Calculation | 36 | 70.6% | 19 | 82.6% | 17 | 60.7% | 0.125 | |
| Perception | Visual Field | 1 | 2.0% | 0 | 0.0% | 1 | 3.6% | >0.999 |
| Spatial attention | Hearts cancelation | 32 | 62.7% | 14 | 60.9% | 18 | 64.3% | >0.999 |
| Space asymmetry | 22 | 43.1% | 8 | 34.8% | 14 | 50.0% | 0.395 | |
| Object asymmetry | 10 | 19.6% | 1 | 4.3% | 9 | 32.1% | 0.015 | |
| Praxis | Imitation | 13 | 25.5% | 7 | 30.4% | 6 | 21.4% | 0.529 |
| Executive function | Baseline score | 26 | 51.0% | 11 | 47.8% | 15 | 53.6% | 0.781 |
| Shifting score | 14 | 27.5% | 6 | 26.1% | 8 | 28.6% | >0.999 | |
| Domain | ΔBI | ΔMI | ΔFMA-UE | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | p | Mean (SD) | p | Mean (SD) | p | |||
| Language | Picture Naming | impaired | 21.3 (15.1) | 0.678 | 12.5 (11.6) | 0.112 | 8.5 (7.5) | 0.053 |
| unimpaired | 23.5 (15.9) | 18.5 (13.3) | 14.2 (11.0) | |||||
| Semantics | impaired | 15.3 (8.1) | 0.268 | 13.3 (8.6) | 0.875 | 5.2 (8.4) | 0.037 | |
| unimpaired | 23.6 (16.0) | 16.5 (13.4) | 12.8 (10.0) | |||||
| Sentence Reading | impaired | 22.0 (14.5) | 0.872 | 14.0 (13.1) | 0.201 | 9.5 (9.4) | 0.074 | |
| unimpaired | 23.1 (16.6) | 18.1 (12.6) | 14.1 (10.3) | |||||
| Memory | Orientation | impaired | 21.2 (14.3) | 0.863 | 14.1 (13.1) | 0.428 | 8.2 (8.4) | 0.14 |
| unimpaired | 23.1 (16.0) | 16.9 (12.9) | 13.2 (10.4) | |||||
| Recall and Recognition | impaired | 24.7 (13.5) | 0.329 | 15.5 (12.8) | 0.81 | 11.0 (8.8) | 0.715 | |
| unimpaired | 21.1 (16.8) | 16.6 (13.2) | 12.6 (11.0) | |||||
| Episodic Memory | impaired | 21.3 (14.1) | 0.576 | 17.5 (14.1) | 0.615 | 11.7 (10.8) | 0.655 | |
| unimpaired | 24.2 (17.2) | 14.5 (11.3) | 12.2 (9.5) | |||||
| Number processing | Number Writing | impaired | 19.4 (11.8) | 0.428 | 11.6 (11.1) | 0.133 | 6.6 (8.8) | 0.007 |
| unimpaired | 23.8 (16.6) | 17.9 (13.2) | 14.0 (9.9) | |||||
| Calculation | impaired | 21.4 (14.3) | 0.521 | 14.6 (12.9) | 0.198 | 11.1 (10.9) | 0.158 | |
| unimpaired | 25.3 (18.2) | 20.0 (12.6) | 13.9 (7.8) | |||||
| Perception | Visual Field | impaired | 26.0 (0.0) | 0.784 | 9.0 (0.0) | 0.588 | 3.0 (0.0) | 0.431 |
| unimpaired | 22.5 (15.6) | 16.3 (13.0) | 12.1 (10.1) | |||||
| Spatial attention | Hearts Cancelation | impaired | 19.0 (14.0) | 0.054 | 15.1 (12.9) | 0.423 | 10.0 (10.9) | 0.015 |
| unimpaired | 28.6 (16.2) | 18.0 (13.0) | 15.2 (7.7) | |||||
| Object Asymmetry | impaired | 11.4 (9.3) | 0.01 | 12.5 (15.4) | 0.263 | 9.7 (13.5) | 0.171 | |
| unimpaired | 25.3 (15.5) | 17.0 (12.3) | 12.5 (9.2) | |||||
| Space Asymmetry | impaired | 21.8 (14.3) | 0.909 | 15.8 (13.5) | 0.886 | 9.0 (11.4) | 0.011 | |
| unimpaired | 23.2 (16.5) | 16.4 (12.7) | 14.2 (8.5) | |||||
| Praxis | Imitation | impaired | 18.2 (14.6) | 0.289 | 15.7 (13.8) | 0.828 | 11.5 (12.5) | 0.573 |
| unimpaired | 24.1 (15.6) | 16.3 (12.7) | 12.1 (9.3) | |||||
| Executive function | Baseline Score | impaired | 16.5 (12.5) | 0.006 | 15.6 (13.0) | 0.872 | 10.7 (11.4) | 0.135 |
| unimpaired | 28.9 (15.9) | 16.7 (13.0) | 13.3 (8.6) | |||||
| Shifting Score | impaired | 27.9 (12.5) | 0.078 | 17.8 (14.0) | 0.567 | 14.2 (9.4) | 0.200 | |
| unimpaired | 20.6 (16.1) | 15.5 (12.6) | 11.1 (10.3) | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Monteleone, S.; Redolfi, A.; Garattini, R.; Sacella, G.; Noro, F.; Galeri, S.; et al. Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation. Brain Sci. 2021, 11, 587. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050587
Aprile I, Guardati G, Cipollini V, Papadopoulou D, Monteleone S, Redolfi A, Garattini R, Sacella G, Noro F, Galeri S, et al. Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation. Brain Sciences. 2021; 11(5):587. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050587
Chicago/Turabian StyleAprile, Irene, Giulia Guardati, Valeria Cipollini, Dionysia Papadopoulou, Serena Monteleone, Alessandra Redolfi, Romina Garattini, Gianluigi Sacella, Fulvia Noro, Silvia Galeri, and et al. 2021. "Influence of Cognitive Impairment on the Recovery of Subjects with Subacute Stroke Undergoing Upper Limb Robotic Rehabilitation" Brain Sciences 11, no. 5: 587. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11050587