
External Validation and Calibration of the DecaPreT Prediction Model for Decannulation in Patients with Acquired Brain Injury

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Prediction Model and Statistical Analysis
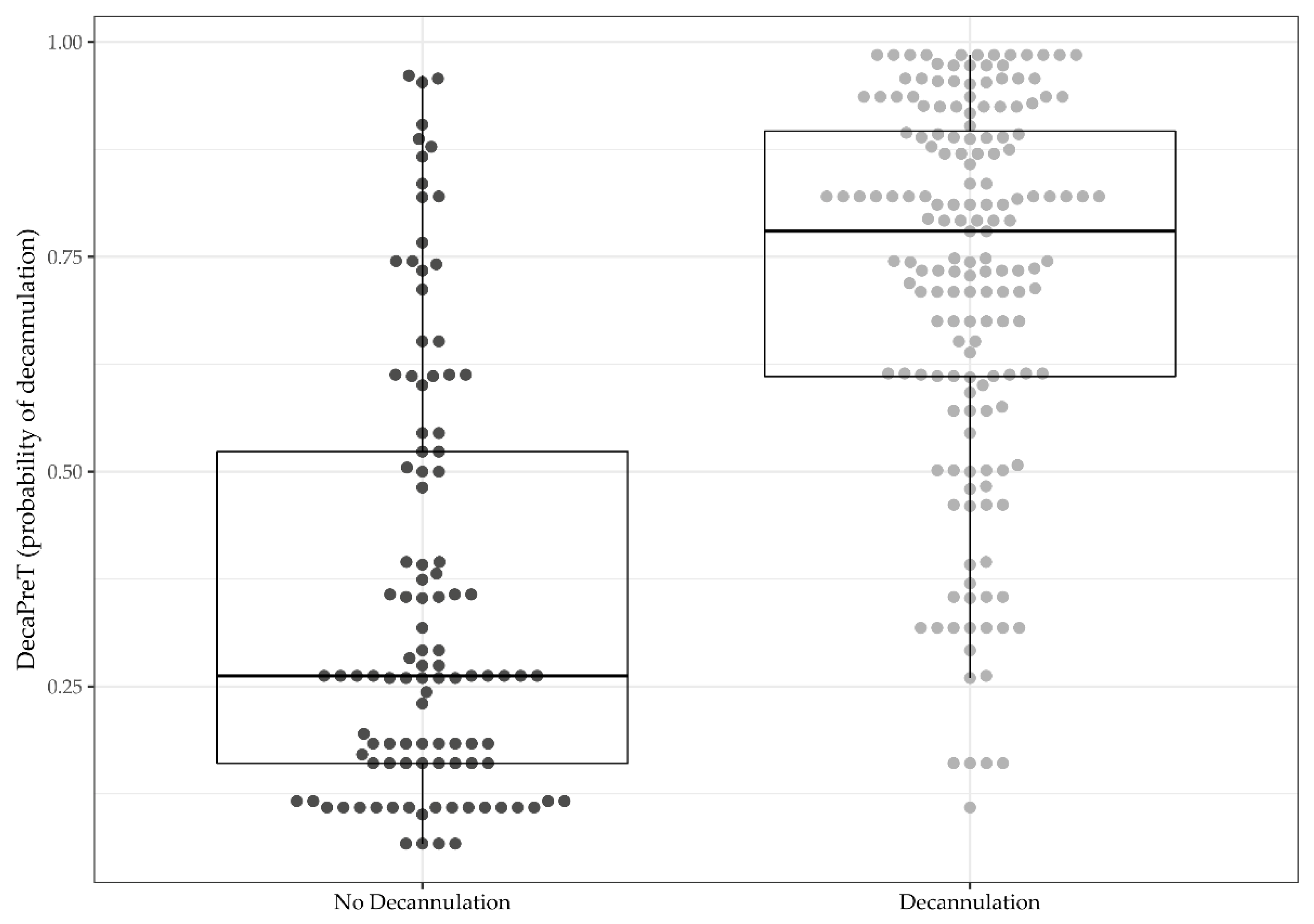
3. Results
3.1. Clinical Characteristics at Admission and Discharge
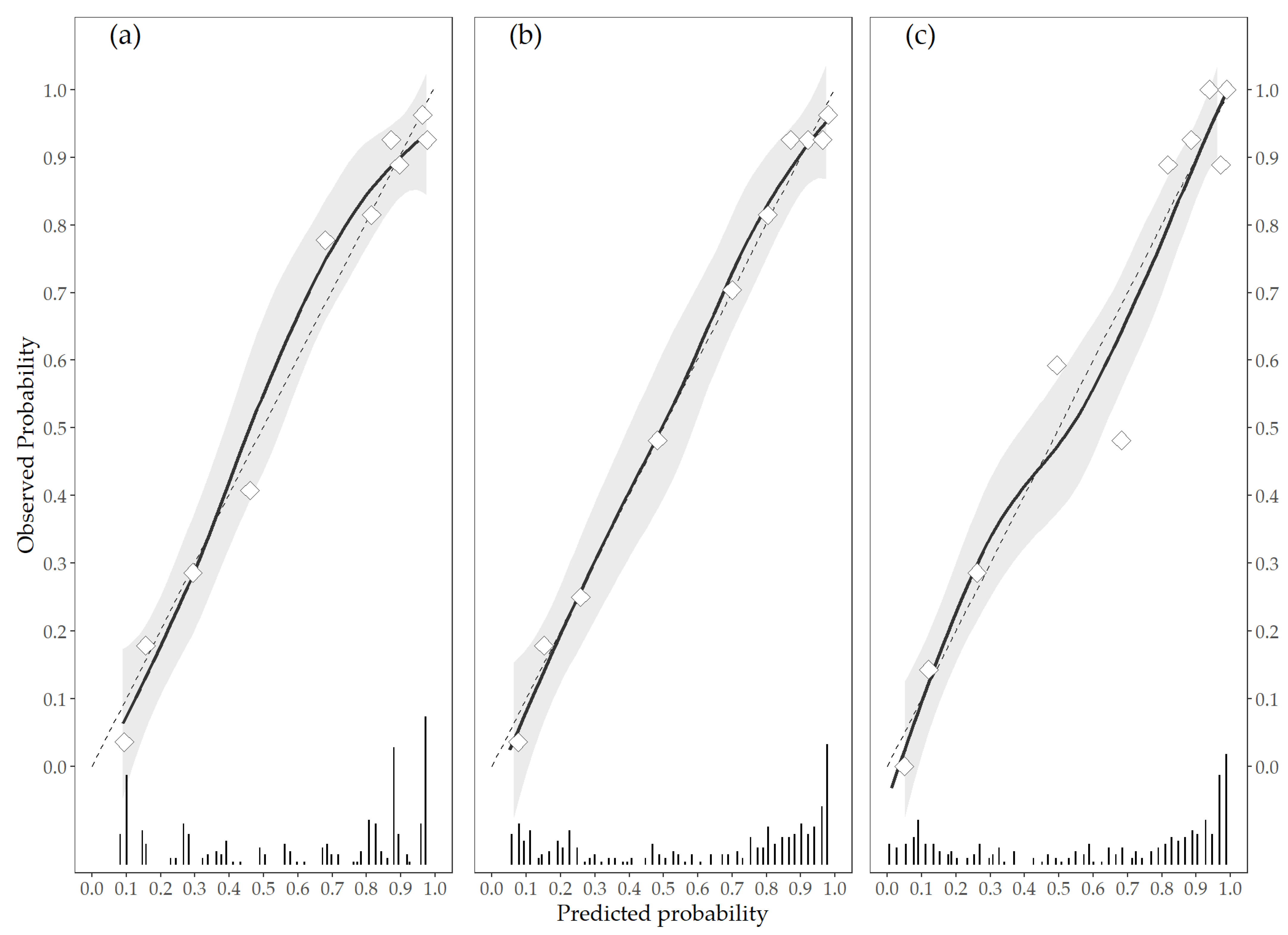
3.2. Update of the DecaPreT Model
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Estimate | SE | p-Value | |
|---|---|---|---|
| Revision model | |||
| Intercept | −2.452 | 0.43 | <0.0001 |
| Age score | 0.056 | 0.222 | 0.8 |
| Saliva score | 0.137 | 0.458 | 0.766 |
| VS score | 1.718 | 0.392 | <0.0001 |
| Coughing score | 1.212 | 0.174 | <0.0001 |
| Pathogenesis score | 0.23 | 0.164 | 0.161 |
| Continuous model | |||
| Intercept | −2.613 | 0.868 | 0.003 |
| Age (years) | −0.01 | 0.011 | 0.393 |
| Saliva score | 0.154 | 0.47 | 0.743 |
| CRS-r | 0.129 | 0.025 | <0.0001 |
| Coughing score | 1.123 | 0.173 | <0.0001 |
| Pathogenesis score | 0.18 | 0.173 | 0.297 |
| Complete model | |||
| Intercept | −0.822 | 0.976 | 0.4 |
| Age (years) | −0.018 | 0.012 | 0.135 |
| Saliva score | 0.161 | 0.478 | 0.737 |
| CRS-r | 0.13 | 0.026 | <0.0001 |
| Coughing score | 1.146 | 0.181 | <0.0001 |
| Pathogenesis score | 0.151 | 0.179 | 0.399 |
| Length of stay in ICU (days) | 0.13 | 0.026 | <0.0001 |
References
- Taylor, G.J.; Bagby, M.R.; Parker, J.D.A. The Alexithymia Construct: A Potential Paradigm for Psychosomatic Medicine. Psychosomatics 1991, 32, 153–164. [Google Scholar] [CrossRef]
- Durbin, C.G., Jr. Tracheostomy: Why, when, and how? Respir. Care 2010, 55, 1056–1068. [Google Scholar] [PubMed]
- Morrism, P.E.; Griffin, L.; Berry, M.; Thompson, C.; Hite, R.D.; Winkelman, C.; Hopkins, R.O.; Ross, A.; Dixon, L.; Leach, S. Receiving early mobility during an intensive care unit admission is a predictor of improved outcomes in acute respiratory failure. Am. J. Med. Sci. 2011, 341, 373–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christopher, K.L. Tracheostomy decannulation. Respir. Care 2005, 50, 538–541. [Google Scholar] [PubMed]
- Garuti, G.; Reverberi, C.; Briganti, A.; Massobrio, M.; Lombardi, F.; Lusuardi, M. Swallowing disorders in tracheotomised patients: A multidisciplinary/multiprofessional approach in decannulation protocol. Multidiscip. Respir. Med. 2014, 9, 2–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Checklin, M.; Etty-Leal, M.; Iseli, T.A.; Potter, N.; Fisher, S.; Chapman, L. Saliva management options for difficult-to-wean people with tracheostomy following severe acquired brain injury (ABI): A review of the literature. Brain Inj. 2015, 29, 1–10. [Google Scholar] [CrossRef]
- Reverberi, C.; Lombardi, F.; Lusuardi, M.; Pratesi, A.; Di Bari, M. Development of the Decannulation Prediction Tool in Patients with Dysphagia after Acquired Brain Injury. J. Am. Med. Dir. Assoc. 2019, 20, 470–475. [Google Scholar] [CrossRef]
- Ceriana, P.; Carlucci, A.; Navalesi, P.; Rampulla, C.; Delmastro, M.; Piaggi, G.; De Mattia, E.; Nava, S. Weaning from tracheotomy in long-term mechanically ventilated patients: Feasibility of a decisional flowchart and clinical outcome. Intensive Care Med. 2003, 29, 845–848. [Google Scholar] [CrossRef]
- Hernández, G.; Ortiz, R.; Pedrosa, A.; Cuena, R.; Vaquero Collado, C.; González Arenas, P.; García Plaza, S.; Canabal Berlanga, A.; Fernández, R. The indication of tracheotomy conditions the predictors of time to decannulation in critical patients. Med. Intensiva 2012, 36, 531–539. [Google Scholar] [CrossRef]
- Enrichi, C.; Battel, I.; Zanetti, C.; Koch, I.; Ventura, L.; Palmer, K.; Meneghello, F.; Piccione, F.; Rossi, S.; Lazzeri, M.; et al. Clinical Criteria for Tracheostomy Decannulation in Subjects with Acquired Brain Injury. Respir. Care. 2017, 62, 1255–1263. [Google Scholar] [CrossRef] [Green Version]
- Mortensen, J.; Kjeldsen, S.S.; Honoré, H.; Pedersen, A.R. Using Routinely Gathered Clinical Data to Develop a Prognostic Online Tool for Decannulation in Subjects With Acquired Brain Injury. Respir. Care. 2020, 65, 1678–1686. [Google Scholar] [CrossRef]
- Santus, P.; Gramegna, A.; Radovanovic, D.; Raccanelli, R.; Valenti, V.; Rabbiosi, D.; Vitacca, M.; Nava, S. A systematic review on tracheostomy decannulation: A proposal of a quantitative semiquantitative clinical score. BMC Pulm. Med. 2014, 14, 201. [Google Scholar] [CrossRef] [Green Version]
- Heidler, M.D.; Salzwedel, A.; Jöbges, M.; Lück, O.; Dohle, C.; Seifert, M.; von Helden, A.; Hollweg, W.; Völler, H. Decannulation of tracheotomized patients after long-term mechanical ventilation—results of a prospective multicentric study in German neurological early rehabilitation hospitals. BMC Anesthesiol. 2018, 18, 65. [Google Scholar] [CrossRef] [Green Version]
- Battel, I.; Calvo, I.; Walshe, M. Cross-Cultural Validation of the Italian Version of the Functional Oral Intake Scale. Folia Phoniatr. Logop. 2018, 70, 117–123. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org/ (accessed on 26 May 2021).
- Vergouwe, Y.; Royston, P.; Moons, K.G.; Altman, D.G. Development and validation of a prediction model with missing predictor data: A practical approach. J. Clin. Epidemiol. 2010, 63, 205–214. [Google Scholar] [CrossRef] [PubMed]
- Evaluating a Logistic Regression Based Prediction Tool in R. Available online: https://archive.is/czWxN (accessed on 26 May 2021).
- Harrell, F.E., Jr. Regression Modeling Strategies: With Applications to Linear Models, Logistic Regression, and Survival Analysis; Springer: New York, NY, USA, 2001. [Google Scholar]
- Austin, P.C.; Steyerberg, E.W. The Integrated Calibration Index (ICI) and related metrics for quantifying the calibration of logistic regression models. Stat. Med. 2019, 38, 4051–4065. [Google Scholar] [CrossRef] [Green Version]
- Crary, M.A.; Carnaby Mann, G.D.; Groher, M.E. Initial psychometric assessment of a functional oral intake scale for dysphagia in stroke patients. Arch. Phys. Med. Rehabil. 2005, 86, 1516–1520. [Google Scholar] [CrossRef] [PubMed]
- Hakiki, B.; Pancani, S.; Draghi, F.; Portaccio, E.; Tofani, A.; Binazzi, B.; Anna Maria, R.; Scarpino, M.; Macchi, C.; Cecchi, F. Decannulation and improvement of responsiveness in patients with disorders of consciousness. Neuropsychol. Rehabil. 2020. [Google Scholar] [CrossRef] [PubMed]
- Zivi, I.; Valsecchi, R.; Maestri, R.; Maffia, S.; Zarucchi, A.; Molatore, K.; Vellati, E.; Saltuari, L.; Frazzitta, G. Early Rehabilitation Reduces Time to Decannulation in Patients With Severe Acquired Brain Injury: A Retrospective Study. Front. Neurol. 2018, 9, 559. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quiñones-Ossa, G.A.; Durango-Espinosa, Y.A.; Padilla-Zambrano, H.; Ruiz, J.; Moscote-Salazar, L.R.; Galwankar, S.; Gerber, J.; Hollandx, R.; Ghosh, A.; Pal, R.; et al. Current Status of Indications, Timing, Management, Complications, and Outcomes of Tracheostomy in Traumatic Brain Injury Patients. J Neurosci. Rural Pract. 2020, 11, 222–229. [Google Scholar]
- Chen, H.; Cohen, P.; Chen, S. Biased odds ratios from dichotomization of age. Stat. Med. 2007, 26, 3487–3497. [Google Scholar] [CrossRef] [PubMed]
- Van Walraven, C.; Hart, R.G. Leave ’em alone—why continuous variables should be analyzed as such. Neuroepidemiology 2008, 30, 138–139. [Google Scholar] [CrossRef] [PubMed]


| ABI (n = 273) | |
|---|---|
| Age at injury (years) | 53.01 ± 17.75 |
| Female | 93 (34.07) |
| Length of stay ICU (days) | 36.00 (28.00–49.00) |
| CRS-r at admission | 11.00 (5.00–21.00) |
| Feeding at admission | |
| Oral | 12 (4.40) |
| NG tube | 158 (57.88) |
| PEG | 103 (37.73) |
| Brainstem injury (%) | 43 (15.75) |
| Age DecaPreT score | |
| <47 | 98 (35.90) |
| 47–61 | 86 (31.50) |
| >61 | 89 (32.60) |
| Saliva Aspiration DecaPreT score | |
| No | 191 (69.96) |
| Yes | 82 (30.04) |
| Vegetative status DecaPreT score | |
| No | 168 (61.54) |
| Yes | 105 (38.46) |
| Coughing Score DecaPreT score | |
| Voluntary and reflex | 111 (40.66) |
| Reflex only | 46 (16.85) |
| Voluntary only | 50 (18.32) |
| Neither | 66 (24.18) |
| Pathogenesis of brain lesion DecaPreT score | |
| Trauma | 96 (35.16) |
| Other | 15 (5.49) |
| Stroke | 140 (51.28) |
| Anoxia | 22 (8.06) |
| DecaPreT (probability of decannulation) | 0.61 (0.29–0.82) |
| Tested Models | Degrees of Freedom | χ2 | p-Value |
|---|---|---|---|
| Revision vs. Original | 6 | 36.6209 | <0.001 |
| Revision vs. Calibration in the large | 5 | 34.3932 | <0.001 |
| Revision vs. Logistic calibration | 4 | 34.3809 | <0.001 |
| Metric | Revision Model | Continuous Model | Complete Model |
|---|---|---|---|
| Brier score | 0.134 (0.102–0.155) | 0.130 (0.099–0.152) | 0.122 (0.093–0.146) |
| AUC | 0.874 (0.839–0.917) | 0.884 (0.855–0.932) | 0.901 (0.866–0.939) |
| Intercept | 0.021 (−0.001–0.033) | 0.019 (−0.004–0.036) | 0.023 (−0.010–0.044) |
| Slope | 0.943 (0.924–0.958) | 0.935 (0.930–0.965) | 0.933 (0.905–0.944) |
| Emax | 0.016 (0.011–0.022) | 0.018 (0.010–0.020) | 0.019 (0.014–0.028) |
| ICI | 0.041 (0.020–0.071) | 0.023 (0.016–0.063) | 0.018 (0.007–0.053) |
| NRI (>0) * | 0.545 (0.314–0.776) | 0.724 (0.497–0.950) | |
| IDI * | 0.021 (−0.001–0.044) | 0.057 (0.025–0.089) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leto, E.; Lofaro, D.; Lucca, L.F.; Ursino, M.; Rogano, S.; Scola, P.; Tonin, P.; Conforti, D.; Cerasa, A. External Validation and Calibration of the DecaPreT Prediction Model for Decannulation in Patients with Acquired Brain Injury. Brain Sci. 2021, 11, 799. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060799
Leto E, Lofaro D, Lucca LF, Ursino M, Rogano S, Scola P, Tonin P, Conforti D, Cerasa A. External Validation and Calibration of the DecaPreT Prediction Model for Decannulation in Patients with Acquired Brain Injury. Brain Sciences. 2021; 11(6):799. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060799
Chicago/Turabian StyleLeto, Elio, Danilo Lofaro, Lucia Francesca Lucca, Maria Ursino, Stefania Rogano, Paolo Scola, Paolo Tonin, Domenico Conforti, and Antonio Cerasa. 2021. "External Validation and Calibration of the DecaPreT Prediction Model for Decannulation in Patients with Acquired Brain Injury" Brain Sciences 11, no. 6: 799. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060799