
A CNN-Based Autoencoder and Machine Learning Model for Identifying Betel-Quid Chewers Using Functional MRI Features


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. MRI Data Acquisition
2.3. Functional MRI Preprocessing
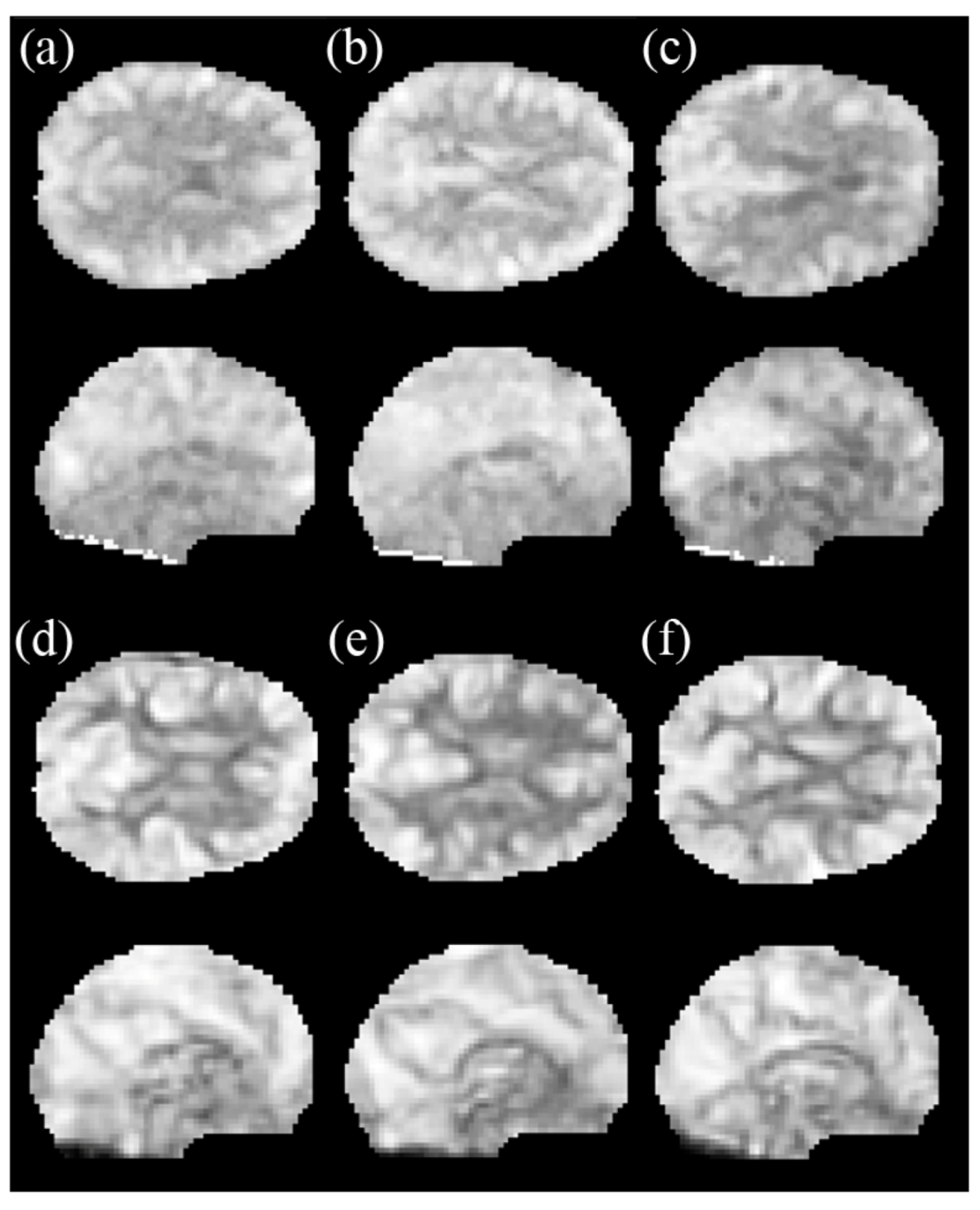
2.4. Amplitude of the Low-Frequency Fluctuations (ALFF)
2.5. Regional Homogeneity (ReHo)
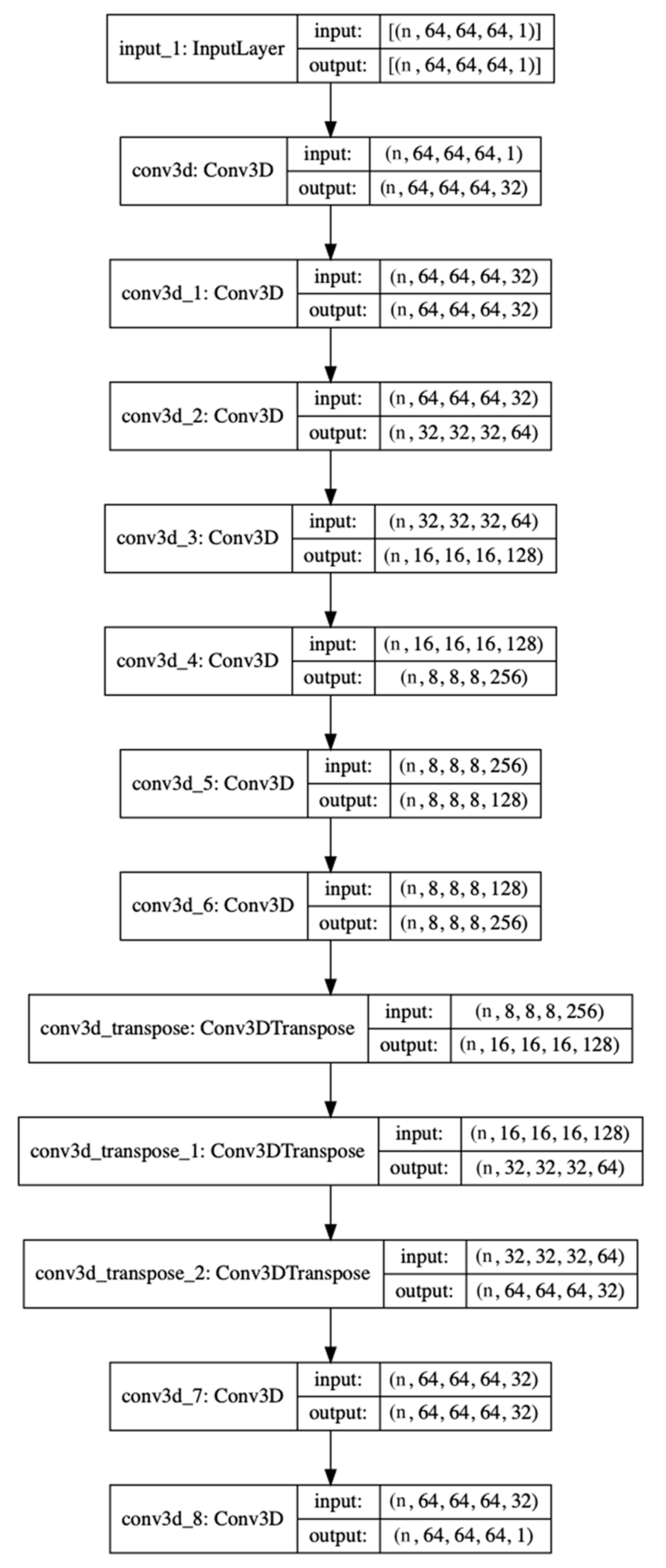
2.6. Autoencoder and Supervised Machine-Learning Algorithm
3. Results
3.1. Participants
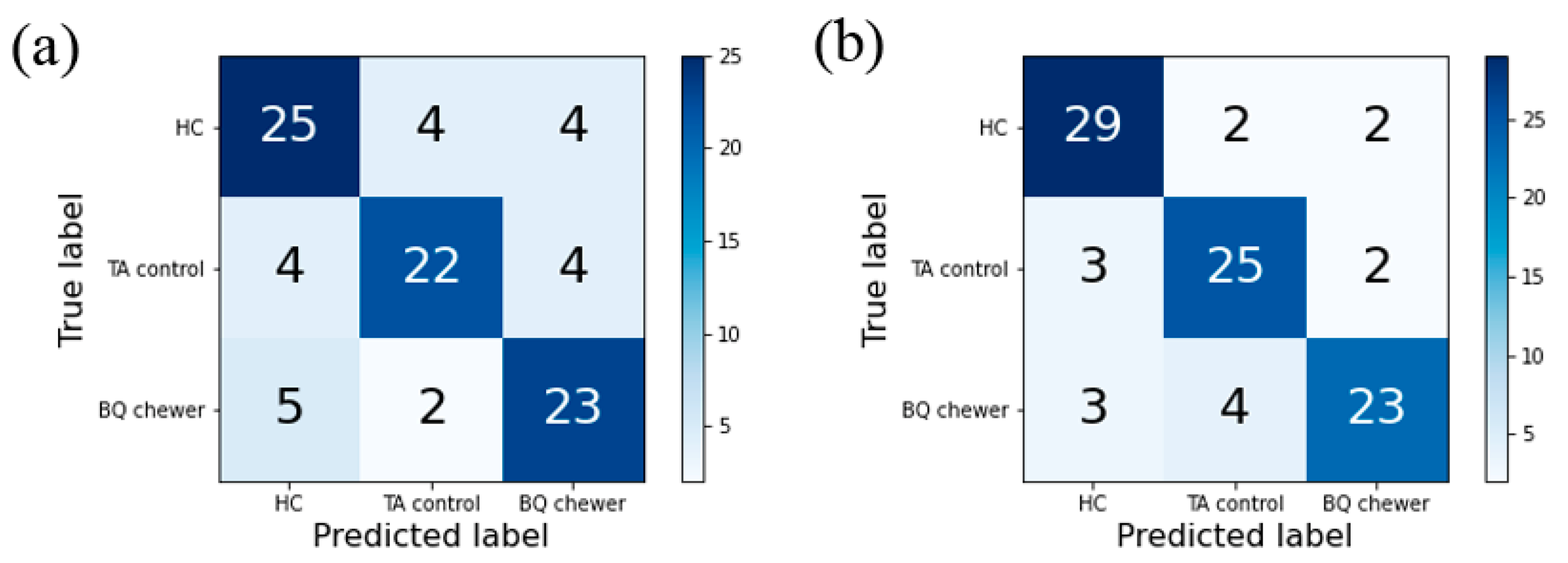
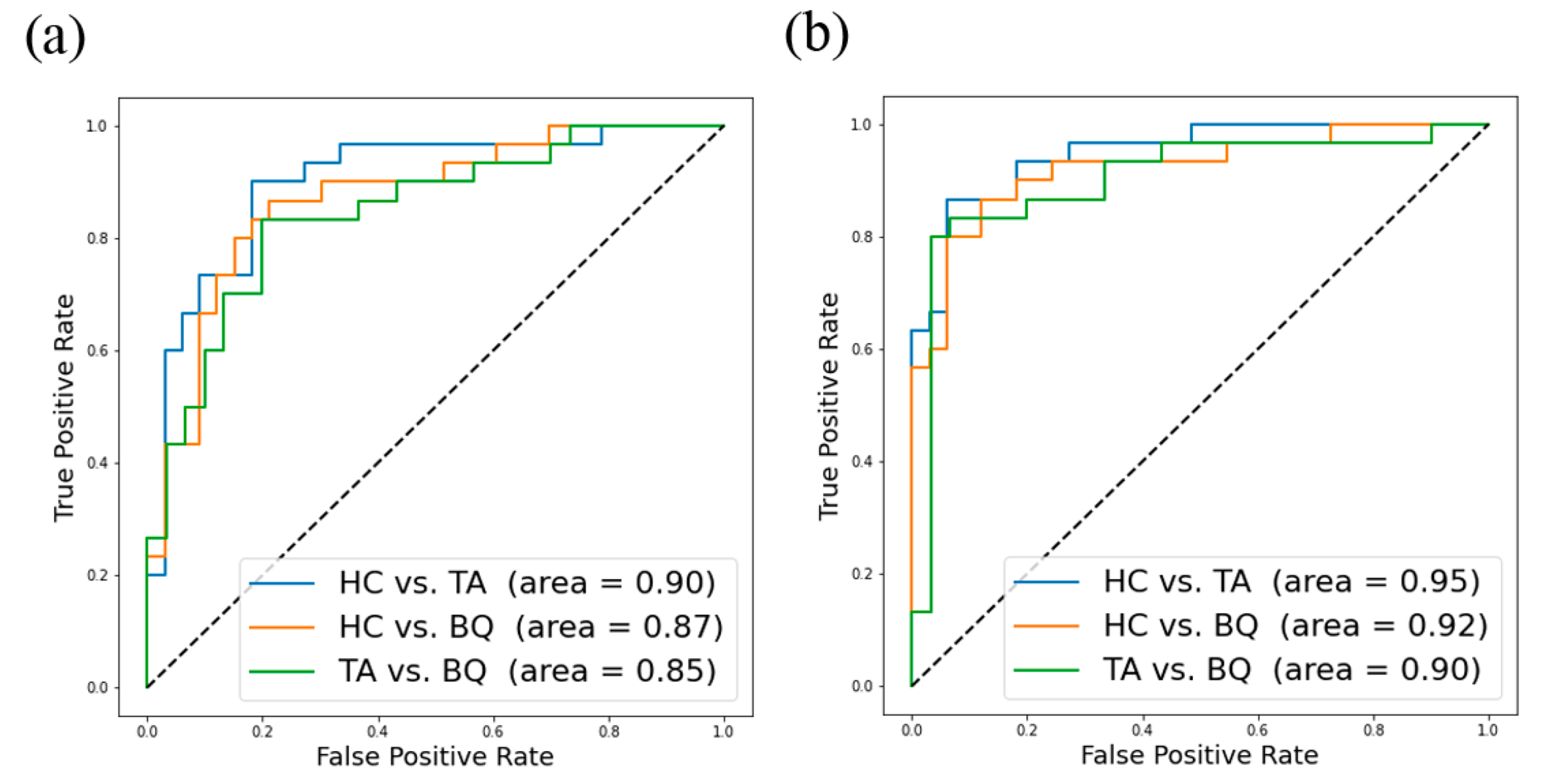
3.2. The Autoencoder and Supervised Machine-Learning Algorithm
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| ALFF | amplitude of low-frequency fluctuations |
| AP | anterior–posterior |
| AUC | area under the curve |
| AUDIT | Alcohol Use Disorders Identification Test |
| BNDS | Betel Nut Dependency Scale |
| BQ | betel quid |
| CART | decision tree classifier |
| CNN | convolutional neural network |
| DL | deep learning |
| DSM | The Diagnostic and Statistical Manual of Mental Disorders |
| EPI | echo-planar image |
| FTND | Fagerstrom Test for Nicotine Dependence |
| FOV | field of view |
| FWHM | full-width at half-maximum |
| HC | healthy controls |
| ICD | The International Statistical Classification of Diseases and Related Health Problems |
| KCC | Kendall’s coefficient of concordance |
| KNN | k-nearest neighbors’ classifier |
| LDA | linear discriminant analysis |
| LOOCV | leave-one-out-cross-validation |
| LR | logistic regression |
| MLP | multilayer perceptron |
| MNI | Montreal Neurological Institute |
| NB | Gaussian naive Bayes |
| OvO | one-vs.-one |
| ReHo | regional homogeneity |
| REST | Resting-State Data Analysis tool kit |
| RF | random forest |
| RL | right-left |
| rs-fMRI | resting-state functional magnetic resonance imaging |
| SPECT | single photon emission computerized tomography |
| SPM | statistical parametric mapping |
| SVM | support vector machine |
| TA | tobacco- and alcohol-user controls |
| XGB | extreme gradient boost |
References
- Winstock, A. Areca nut-abuse liability, dependence and public health. Addict. Biol. 2002, 7, 133–138. [Google Scholar] [CrossRef]
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Betel-quid and areca-nut chewing and some areca-nut-derived nitrosamines. IARC Monogr. Eval. Carcinog. Risks Hum. 2004, 85, 1–334. [Google Scholar]
- Benegal, V.; Rajkumar, R.P.; Muralidharan, K. Does areca nut use lead to dependence? Drug Alcohol Depend. 2008, 97, 114–121. [Google Scholar] [CrossRef]
- Lee, C.-H.; Chiang, S.-L.; Ko, A.M.-S.; Hua, C.-H.; Tsai, M.-H.; Warnakulasuriya, S.; Ibrahim, S.O.; Sunarjo, S.; Zain, R.B.; Ling, T.-Y.; et al. Betel-quid dependence domains and Syndrome associated with betel-quid ingredients among chewers: An Asian multi-country evidence. Addiction 2014, 109, 1194–1204. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.-H.; Ko, A.M.-S.; Yang, F.M.; Hung, C.-C.; Warnakulasuriya, S.; Ibrahim, S.O.; Zain, R.B.; Ko, Y.-C. Association of dsm-5 betel-quid use disorder with oral potentially malignant disorder in 6 betel-quid endemic asian populations. JAMA Psychiatry 2018, 75, 261–269. [Google Scholar] [CrossRef] [Green Version]
- Sariah, A.; Zhening, L.; Pu, W.; Liu, H.; Xue, Z.; Huang, X. Structural and functional alterations in Betel-Quid chewers: A systematic review of neuroimaging findings. Front. Psychiatry 2019, 10, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weng, J.-C.; Chou, Y.-S.; Huang, G.-J.; Tyan, Y.-S.; Ho, M.-C. Mapping brain functional alterations in betel-quid chewers using resting-state fMRI and network analysis. Psychopharmacology 2018, 235, 1257–1271. [Google Scholar] [CrossRef]
- Liu, T.; Li, J.-j.; Zhao, Z.-y.; Yang, G.-s.; Pan, M.-j.; Li, C.-q.; Pan, S.-y.; Chen, F. Altered spontaneous brain activity in betel quid dependence: A resting-state functional magnetic resonance imaging study. Medicine 2016, 95, e2638. [Google Scholar] [CrossRef]
- Huang, X.; Liu, Z.; Mwansisya, T.E.; Pu, W.; Zhou, L.; Liu, C.; Chen, X.; Rohrbaugh, R.; Marienfeld, C.; Xue, Z. Betel quid chewing alters functional connectivity in frontal and default networks: A resting-state fMRI study. J. Magn. Reson. Imaging 2017, 45, 157–166. [Google Scholar] [CrossRef]
- Liu, T.; Li, J.; Zhang, Z.; Xu, Q.; Lu, G.; Huang, S.; Pan, M.; Chen, F. Altered long-and short-range functional connectivity in patients with betel quid dependence: A resting-state functional MRI study. Cell. Physiol. Biochem. 2016, 40, 1626–1636. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Zhu, Q.; Jiang, C.; Shen, H.; Wang, F.; Liao, W.; Yuan, F. Disrupted resting-state default mode network in betel quid-dependent individuals. Front. Psychol. 2017, 8, 84. [Google Scholar] [CrossRef] [Green Version]
- Liu, T.; Li, J.; Zhao, Z.; Zhong, Y.; Zhang, Z.; Xu, Q.; Yang, G.; Lu, G.; Pan, S.; Chen, F. Betel quid dependence is associated with functional connectivity changes of the anterior cingulate cortex: A resting-state fMRI study. J. Transl. Med. 2016, 14, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, X.; Pu, W.; Liu, H.; Li, X.; Greenshaw, A.J.; Dursun, S.M.; Xue, Z.; Liu, Z. Altered brain functional connectivity in betel quid-dependent chewers. Front. Psychiatry 2017, 8, 239. [Google Scholar] [CrossRef] [Green Version]
- Lundervold, A.S.; Lundervold, A. An overview of deep learning in medical imaging focusing on MRI. Z. Med. Phys. 2019, 29, 102–127. [Google Scholar] [CrossRef]
- Mak, K.K.; Lee, K.; Park, C. Applications of machine learning in addiction studies: A systematic review. Psychiatry Res. 2019, 275, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Whelan, R.; Watts, R.; Orr, C.A.; Althoff, R.R.; Artiges, E.; Banaschewski, T.; Barker, G.J.; Bokde, A.L.; Büchel, C.; Carvalho, F.M. Neuropsychosocial profiles of current and future adolescent alcohol misusers. Nature 2014, 512, 185–189. [Google Scholar] [CrossRef]
- Mete, M.; Sakoglu, U.; Spence, J.S.; Devous, M.D.; Harris, T.S.; Adinoff, B. Successful classification of cocaine dependence using brain imaging: A generalizable machine learning approach. BMC Bioinform. 2016, 17, 49–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ding, X.; Yang, Y.; Stein, E.A.; Ross, T.J. Combining multiple resting-state fMRI features during classification: Optimized frameworks and their application to nicotine addiction. Front. Hum. Neurosci. 2017, 11, 362. [Google Scholar] [CrossRef]
- Abraham, A.; Pedregosa, F.; Eickenberg, M.; Gervais, P.; Mueller, A.; Kossaifi, J.; Gramfort, A.; Thirion, B.; Varoquaux, G. Machine learning for neuroimaging with scikit-learn. Front. Neuroinform. 2014, 8, 14. [Google Scholar] [CrossRef] [Green Version]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V. Scikit-learn: Machine learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Li, R.H.; Ho, M.C.; Tang, T.C.; Chang, C.F. Development of the betel nut dependency scale (BNDS). Chin. J. Psychol. 2012, 54, 331–348. [Google Scholar] [CrossRef]
- Huang, C.-L.; Lin, H.-H.; Wang, H.-H. The psychometric properties of the Chinese version of the fagerstrom test for nicotine dependence. Addict. Behav. 2006, 31, 2324–2327. [Google Scholar] [CrossRef] [PubMed]
- Fagerström, K.-O. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict. Behav. 1978, 3, 235–241. [Google Scholar] [CrossRef]
- Chen, C.H.; Chen, W.J.; Cheng, A.T. New approach to the validity of the alcohol use disorders identification test: Stratum-specific likelihood ratios analysis. Alcohol Clin. Exp. Res. 2005, 29, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, J.B.; Aasland, O.G.; Babor, T.F.; Grant, M. Development of the alcohol use disorders identification test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption-II. Addiction 1993, 88, 791–804. [Google Scholar] [CrossRef]
- Ersche, K.D.; Williams, G.B.; Robbins, T.W.; Bullmore, E.T. Meta-analysis of structural brain abnormalities associated with stimulant drug dependence and neuroimaging of addiction vulnerability and resilience. Curr. Opin. Neurobiol. 2013, 23, 615–624. [Google Scholar] [CrossRef] [Green Version]
- Ersche, K.D.; Jones, P.S.; Williams, G.B.; Turton, A.J.; Robbins, T.W.; Bullmore, E.T. Abnormal brain structure implicated in stimulant drug addiction. Science 2012, 335, 601–604. [Google Scholar] [CrossRef] [Green Version]
- Yue, Y.; Jia, X.; Hou, Z.; Zang, Y.; Yuan, Y. Frequency-dependent amplitude alterations of resting-state spontaneous fluctuations in late-onset depression. BioMed. Res. Int. 2015, 2015, 505479. [Google Scholar] [CrossRef] [PubMed]
- Zou, Q.H.; Zhu, C.Z.; Yang, Y.; Zuo, X.N.; Long, X.Y.; Cao, Q.J.; Wang, Y.F.; Zang, Y.F. An improved approach to detection of amplitude of low-frequency fluctuation (ALFF) for resting-state fMRI: Fractional ALFF. J. Neurosci. Methods 2008, 172, 137–141. [Google Scholar] [CrossRef] [Green Version]
- Zang, Y.; Jiang, T.; Lu, Y.; He, Y.; Tian, L. Regional homogeneity approach to fMRI data analysis. Neuroimage 2004, 22, 394–400. [Google Scholar] [CrossRef]
- Ben-David, A. Comparison of classification accuracy using Cohen’s Weighted Kappa. Expert Syst. Appl. 2008, 34, 825–832. [Google Scholar] [CrossRef]
- Chen, V.C.; Lin, T.Y.; Yeh, D.C.; Chai, J.W.; Weng, J.C. Predicting chemo-brain in breast cancer survivors using multiple MRI features and machine-learning. Magn. Reson. Med. 2019, 81, 3304–3313. [Google Scholar] [CrossRef] [PubMed]
- Dikaios, N.; Alkalbani, J.; Sidhu, H.S.; Fujiwara, T.; Abd-Alazeez, M.; Kirkham, A.; Allen, C.; Ahmed, H.; Emberton, M.; Freeman, A.; et al. Logistic regression model for diagnosis of transition zone prostate cancer on multi-parametric MRI. Eur. Radiol. 2015, 25, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Just, M.A.; Pan, L.; Cherkassky, V.L.; McMakin, D.L.; Cha, C.; Nock, M.K.; Brent, D. Machine learning of neural representations of suicide and emotion concepts identifies suicidal youth. Nat. Hum. Behav. 2017, 1, 911–919. [Google Scholar] [CrossRef] [Green Version]
- Gong, E.; Pauly, J.M.; Wintermark, M.; Zaharchuk, G. Deep learning enables reduced gadolinium dose for contrast-enhanced brain MRI. J. Magn. Reson. Imaging 2018, 48, 330–340. [Google Scholar] [CrossRef] [PubMed]
- Hyun, C.M.; Kim, H.P.; Lee, S.M.; Lee, S.; Seo, J.K. Deep learning for undersampled MRI reconstruction. Phys. Med. Biol. 2018, 63, 135007. [Google Scholar] [CrossRef]
- Tezcan, K.C.; Baumgartner, C.F.; Luechinger, R.; Pruessmann, K.P.; Konukoglu, E. MR Image reconstruction using deep density priors. IEEE Trans. Med. Imaging 2019, 38, 1633–1642. [Google Scholar] [CrossRef]
- Akkus, Z.; Galimzianova, A.; Hoogi, A.; Rubin, D.L.; Erickson, B.J. Deep learning for brain MRI segmentation: State of the art and future directions. J. Digit. Imaging 2017, 30, 449–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ying, X. An overview of overfitting and its solutions. J. Phys. Conf. Ser. 2019, 1168, 022022. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Betel-Quid Chewers (BQ) (n = 16) | Tobacco- and Alcohol-User Controls (TA) (n = 15) | Healthy Controls (HC) (n = 17) | F | p | ||||
|---|---|---|---|---|---|---|---|---|
| Mean | (SD) | Mean | (SD) | Mean | (SD) | |||
| Age | 37.1 | (10.4) | 30.1 | (4.9) | 31.6 | (3.6) | F(2,45) = 4.502 | 0.017 |
| Education Years | 13.6 | (2.1) | 15.5 | (1.9) | 15.8 | (2.3) | F(2,45) = 4.771 | 0.013 |
| BNDS | 28.4 | (3.2) | 11.0 | 11.0 | F(2,44) = 444.311 | <0.001 | ||
| FTND | 4.7 | (2.5) | 4.2 | (2.0) | n/a | F(1,26) = 0.343 | 0.563 | |
| AUDIT | 10.9 | (6.5) | 8.1 | (7.5) | n/a | F(1,26) = 1.168 | 0.290 | |
| Months | 173.5 | (151.9) | n/a | n/a | ||||
| Days | 4.8 | (2.3) | n/a | n/a | ||||
| Number of BQ | 20.8 | (26.1) | n/a | n/a | ||||
| Metric | ACC | CCR (BQ) | CCR (TA) | CCR (HC) | Kappa |
|---|---|---|---|---|---|
| mfALFF | 0.75 | 0.73 | 0.73 | 0.78 | 0.63 |
| mReHo | 0.83 | 0.77 | 0.83 | 0.88 | 0.74 |
| Metric | Accuracy | Precision | Recall | F1-Score | AUC | |
|---|---|---|---|---|---|---|
| mfALFF | HC vs. TA | 0.79 | 0.79 | 0.82 | 0.81 | 0.90 |
| HC vs. BQ | 0.82 | 0.82 | 0.85 | 0.84 | 0.87 | |
| TA vs. BQ | 0.80 | 0.80 | 0.80 | 0.80 | 0.85 | |
| mReHo | HC vs. TA | 0.90 | 0.89 | 0.94 | 0.91 | 0.95 |
| HC vs. BQ | 0.85 | 0.83 | 0.91 | 0.87 | 0.92 | |
| TA vs. BQ | 0.87 | 0.84 | 0.90 | 0.87 | 0.90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ho, M.-C.; Shen, H.-A.; Chang, Y.-P.E.; Weng, J.-C. A CNN-Based Autoencoder and Machine Learning Model for Identifying Betel-Quid Chewers Using Functional MRI Features. Brain Sci. 2021, 11, 809. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060809
Ho M-C, Shen H-A, Chang Y-PE, Weng J-C. A CNN-Based Autoencoder and Machine Learning Model for Identifying Betel-Quid Chewers Using Functional MRI Features. Brain Sciences. 2021; 11(6):809. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060809
Chicago/Turabian StyleHo, Ming-Chou, Hsin-An Shen, Yi-Peng Eve Chang, and Jun-Cheng Weng. 2021. "A CNN-Based Autoencoder and Machine Learning Model for Identifying Betel-Quid Chewers Using Functional MRI Features" Brain Sciences 11, no. 6: 809. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11060809