
A Mobile App for Measuring Real Time Fatigue in Patients with Multiple Sclerosis: Introducing the Fimo Health App

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Measuring Fatigue
2.1. Patient-Reported Outcome Measures
2.2. Performance-Based Measures for Fatigue
2.3. Measuring Influencing Factors
3. Transtheoretical Model of Health Behavior Change
- Precontemplation: people are not ready and do not intend to take action;
- Contemplation: people are beginning to realize that their behavior is problematic;
- Preparation: people are ready to take action in the immediate future;
- Action: people take action and modify their health behaviors;
- Maintenance: people sustain their actions over a longer period;
- Termination: people do not have the temptation to switch back to old behaviors.
Other Behavior Change Techniques
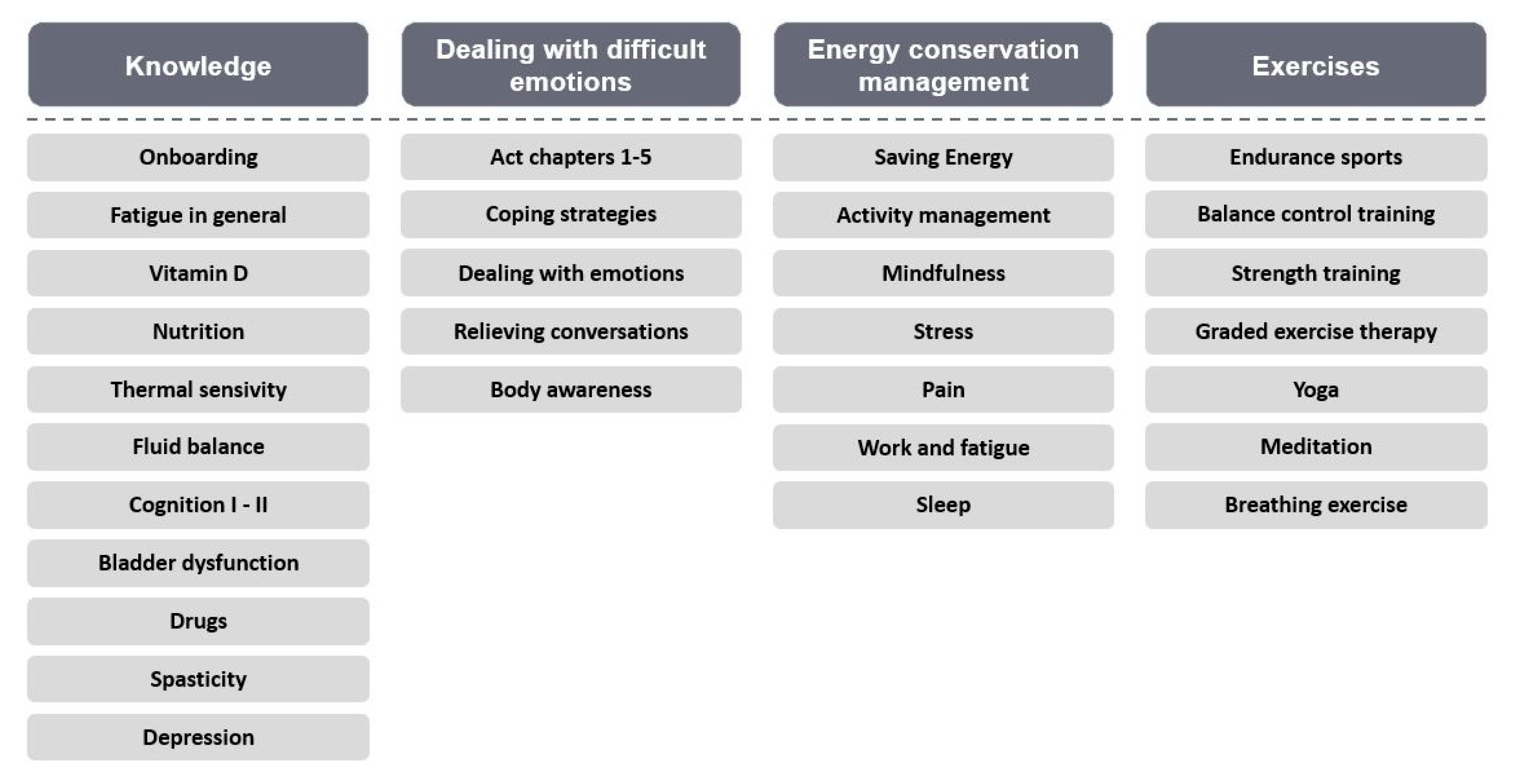
4. Overview of the Fatigue Course
Ten Processes of Change within the Fatigue Course
- Step 1: Consciousness raising:
- Step 2: Dramatic relief:
- Step 3: Self-reevaluation:
- Step 4: Environmental reevaluation:
- Step 5: Self-liberation:
- Step 6: Social liberation:
- Step 7: Counterconditioning:
- Step 8: Stimulus control:
- Step 9: Contingency management:
- Step 10: Helping relationships:
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- National MS Society. What Is Multiple Sclerosis? 2021. Available online: https://www.nationalmssociety.org/What-is-MS/MS-FAQ-s (accessed on 28 July 2021).
- Beckerman, H.; Blikman, L.J.; Heine, M.; Malekzadeh, A.; Teunissen, C.E.; Bussmann, J.B.; Kwakkel, G.; Van Meeteren, J.; de Groot, V. The effectiveness of aerobic training, cognitive behavioural therapy, and energy conservation management in treating MS-related fatigue: The design of the TREFAMS-ACE programme. Trials 2013, 14, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Multiple Sclerosis Council for Clinical Practice Guidelines, Fatigue Guidelines Development Panel of the Multiple Sclerosis Council for Clinical Practice Guidelines. Fatigue and Multiple Sclerosis. In Evidence—Based Management Strategies for Fatigue in Multiple Sclerosis; Paralyzed Veterans of America: Washington, DC, USA, 1998. [Google Scholar]
- Van den Akker, L.E.; Beckerman, H.; Collette, E.H.; Twisk, J.W.; Bleijenberg, G.; Dekker, J.; Knoop, H.; de Groot, V. Cognitive behavioral therapy positively affects fatigue in patients with multiple sclerosis: Results of a randomized controlled trial. Mult. Scler. 2017, 23, 1542–1553. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.M.; Arnett, P.A. Factors related to employment status changes in individuals with multiple sclerosis. Mult. Scler. J. 2005, 11, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Palotai, M.; Wallack, M.; Kujbus, G.; Dalnoki, A.; Guttmann, C. Usability of a Mobile App for Real-Time Assessment of Fatigue and Related Symptoms in Patients With Multiple Sclerosis: Observational Study. JMIR mHealth uHealth 2021, 9, e19564. [Google Scholar] [CrossRef]
- Langeskov-Christensen, M.; Bisson, E.J.; Finlayson, M.L.; Dalgas, U. Potential pathophysiological pathways that can explain the positive effects of exercise on fatigue in multiple sclerosis: A scoping review. J. Neurol. Sci. 2017, 373, 307–320. [Google Scholar] [CrossRef] [PubMed]
- National MS Society. Fatigue. 2021. Available online: https://www.nationalmssociety.org/For-Professionals/Clinical-Care/Managing-MS/Symptom-Management/Fatigue (accessed on 27 July 2021).
- Svenningsson, A.; Falk, E.; Celius, E.G.; Fuchs, S.; Schreiber, K.; Berkö, S.; Sun, J.; Penner, I.K.; Tynergy Trial Investigators. Results from the TYNERGY Trial; A Study in the Real Life Setting. PLoS ONE 2013, 8, e58643. [Google Scholar] [CrossRef]
- Asano, M.; Finlayson, M.L. Meta-Analysis of Three Different Types of Fatigue Management Interventions for People with Multiple Sclerosis: Exercise, Education, and Medication. Mult. Scler. Int. 2014, 2014, 798285. [Google Scholar] [CrossRef]
- Rooney, S.; Moffat, F.; Wood, L.; Paul, L. Effectiveness of fatigue management interventions in reducing severity and impact of fatigue in people with progressive multiple sclerosis: A systematic review. Int. J. MS Care 2019, 21, 35–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmadi, A.; Arastoo, A.A.; Nikbakht, M.; Zahednejad, S.; Rajabpour, M. Comparison of the Effect of 8 weeks Aerobic and Yoga Training on Ambulatory Function, Fatigue and Mood Status in MS Patients. Iran. Red. Crescent. Med. J. 2013, 15, 449–454. [Google Scholar] [CrossRef] [Green Version]
- Razazian, N.; Yavari, Z.; Farnia, V.; Azizi, A.; Kordavani, L.; Bahmani, D.S.; Holsboer-Trachsler, E.; Brand, S. Exercising Impacts on Fatigue, Depression, and Paresthesia in Female Patients with Multiple Sclerosis. Med. Sci. Sports Exerc. 2016, 48, 796–803. [Google Scholar] [CrossRef]
- Krupp, L.B. Fatigue in multiple sclerosis. CNS Drugs 2003, 17, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Fadaeizadeh, L.; Emami, H.; Samiei, K. Comparison of visual analogue scale and faces rating scale in measuring acute postoperative pain. Arch. Iran. Med. 2009, 12, 73–75. [Google Scholar]
- Kos, D.; Nagels, G.; D’Hooghe, M.B.; Duportail, M.; Kerckhofs, E. A rapid screening tool for fatigue impact in multiple sclerosis. BMC Neurol. 2006, 6, 27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale: Application to patients with multiple sclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Schwid, S.R.; Covington, M.; Segal, B.M.; Goodman, A.D. Fatigue in multiple sclerosis: Current understanding and future directions. J. Rehabil. Res. Dev. 2002, 39, 211–224. [Google Scholar]
- Rietberg, M.; van Wegen, E.E.H.; Kwakkel, G. Measuring fatigue in patients with multiple sclerosis: Reproducibility, responsiveness and concurrent validity of three Dutch self-report questionnaires. Disabil. Rehabil. 2010, 32, 1870–1876. [Google Scholar] [CrossRef]
- Chilcot, J.; Norton, S.; Kelly, M.E.; Moss-Morris, R. The Chalder Fatigue Questionnaire is a valid and reliable measure of perceived fatigue severity in multiple sclerosis. Mult. Scler. J. 2016, 22, 677–684. [Google Scholar] [CrossRef]
- Braley, T.J.; Chervin, R.D. Fatigue in multiple sclerosis: Mechanisms, evaluation, and treatment. Sleep 2010, 33, 1061–1067. [Google Scholar] [CrossRef]
- Andreasen, A.K.; Spliid, P.E.; Andersen, H.; Jakobsen, J. Fatigue and processing speed are related in multiple sclerosis. Eur. J. Neurol. 2010, 17, 212–218. [Google Scholar] [CrossRef]
- Benedict, R.H.B.; DeLuca, J.; Phillips, G.; LaRocca, N.; Hudson, L.D.; Rudick, R. Validity of the Symbol Digit Modalities Test as a cognition performance outcome measure for multiple sclerosis. Mult. Scler. J. 2017, 23, 721–733. [Google Scholar] [CrossRef] [PubMed]
- Van Oirschot, P.; Heerings, M.; Wendrich, K.; den Teuling, B.; Martens, M.B.; Jongen, P.J. Symbol digit modalities test variant in a smartphone app for persons with multiple sclerosis: Validation study. JMIR mHealth uHealth 2020, 8, e18160. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Velicer, W.F. The transtheoretical model of health behavior change. Am. J. Health Promot. 1997, 12, 38–48. [Google Scholar] [CrossRef]
- Liu, K.T.; Kueh, Y.C.; Arifin, W.N.; Kim, Y.; Kuan, G. Application of Transtheoretical Model on Behavioral Changes, and Amount of Physical Activity Among University’s Students. Front. Psychol. 2018, 9, 2402. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. In Health Behavior: Theory, Research, and Practice; John Wiley & Sons: Hoboken, NJ, USA, 2015; Volume 97. [Google Scholar]
- Matuska, K.; Mathiowetz, V.; Finlayson, M. Use and perceived effectiveness of energy conservation strategies for managing multiple sclerosis fatigue. Am. J. Occup. Ther. 2007, 61, 62–69. [Google Scholar] [CrossRef] [Green Version]
- Schüler, J.; Wolff, W.; Dettmers, C. Exercise in Multiple Sclerosis: Knowing is Not Enough—The Crucial Role of Intention Formation and Intention Realization. Neurol. Ther. 2019, 8, 5–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abraham, C.; Michie, S. A taxonomy of behavior change techniques used in interventions. Heal. Psychol. 2008, 27, 379. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Korte, E.; Wiezer, N.; Roozeboom, M.B.; Vink, P.; Kraaij, W. Behavior change techniques in mhealth apps for the mental and physical health of employees: Systematic assessment. JMIR mHealth uHealth 2018, 6, e167. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berthele, A.; Hemmer, B. S2k-Leitlinie: Diagnose und Therapie der Multiplen Sklerose, Neuromyelitis-optica-Spektrum-Erkrankungen und MOG-IgG-assoziierten Erkrankungen. DGNeurologie 2021, 4, 251–275. [Google Scholar] [CrossRef]
- Grossman, P.; Kappos, L.; Gensicke, H.; D’Souza, M.; Mohr, D.; Penner, I.-K.; Steiner, C. MS quality of life, depression, and fatigue improve after mindfulness training: A randomized trial. Neurology 2010, 75, 1141–1149. [Google Scholar] [CrossRef] [Green Version]
- Heine, M.; Verschuren, O.; Hoogervorst, E.L.; van Munster, E.; Hacking, H.G.; Visser-Meily, A.; Twisk, J.W.; Beckerman, H.; de Groot, V.; Kwakkel, G.; et al. Does aerobic training alleviate fatigue and improve societal participation in patients with multiple sclerosis? A randomized controlled trial. Mult. Scler. 2017, 23, 1517–1526. [Google Scholar] [CrossRef] [Green Version]
- Mathiowetz, V.G.; Matuska, K.M.; Finlayson, M.L.; Luo, P.; Chen, H.Y. One-year follow-up to a randomized controlled trial of an energy conservation course for persons with multiple sclerosis. Int. J. Rehabilit. Res. 2007, 30, 305–313. [Google Scholar] [CrossRef]
- Hayes, S.C.; Strosahl, K.; Wilson, K.G. Acceptance and Commitment Therapy: An Experiential Approach to Behaviour Change; Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Sheppard, S.C.; Forsyth, J.P.; Hickling, E.J.; Bianchi, J. A Novel Application of Acceptance and Commitment Therapy for Psychosocial Problems Associated with Multiple Sclerosis. Int. J. MS Care 2010, 12, 200–206. [Google Scholar] [CrossRef]
- Jacobsen, H.B.; Kallestad, H.; Landrø, N.I.; Borchgrevink, P.C.; Stiles, T.C. Processes in acceptance and commitment therapy and the rehabilitation of chronic fatigue. Scand. J. Psychol. 2017, 58, 211–220. [Google Scholar] [CrossRef] [PubMed]
- Hayes, S.C.; Luoma, J.B.; Bond, F.W.; Masuda, A.; Lillis, J. Acceptance and Commitment Therapy: Model, processes and outcomes. Behav. Res. Ther. 2006, 44, 1–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, S.C.; Levin, M.E.; Plumb-Vilardaga, J.; Villatte, J.L.; Pistorello, J. Acceptance and Commitment Therapy and Contextual Behavioral Science: Examining the Progress of a Distinctive Model of Behavioral and Cognitive Therapy. Behav. Ther. 2013, 44, 180–198. [Google Scholar] [CrossRef] [Green Version]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Rincon, D.; Leach, B.; Pollard, J.; Parkinson, S.; Gkousis, E.; Lichten, C.; Sussex, J.; Manville, C. Exploring the Societal Burden of Multiple Sclerosis: A Study into the Non-Clinical Impact of the Disease, Including Changes with Progression; RAND Corporation: Santa Monica, CA, USA, 2019. [Google Scholar]
- Heinonen, T.; Castrén, E.; Luukkaala, T.; Mäkinen, K.; Ruutiainen, J.; Kuusisto, H. The retirement rate due to multiple sclerosis has decreased since 1995–A retrospective study in a Finnish central hospital. Mult. Scler. Relat. Disord. 2020, 45, 102360. [Google Scholar] [CrossRef]
- Nejati, S.; Esfahani, S.R.; Rahmani, S.; Afrookhteh, G.; Hoveida, S. The Effect of Group Mindfulness-based Stress Reduction and Consciousness Yoga Program on Quality of Life and Fatigue Severity in Patients with MS. J. Caring Sci. 2016, 5, 325–335. [Google Scholar] [CrossRef] [Green Version]
- Johansson, S.; Ytterberg, C.; Hillert, J.; Holmqvist, L.W.; von Koch, L. A longitudinal study of variations in and predictors of fatigue in multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2008, 79, 454–457. [Google Scholar] [CrossRef]
- Powell, D.J.H.; Liossi, C.; Schlotz, W.; Moss-Morris, R. Tracking daily fatigue fluctuations in multiple sclerosis: Ecological momentary assessment provides unique insights. J. Behav. Med. 2017, 40, 772–783. [Google Scholar] [CrossRef] [Green Version]
- Scholz, M.; Haase, R.; Schriefer, D.; Voigt, I.; Ziemssen, T. Electronic health interventions in the case of multiple sclerosis: From theory to practice. Brain Sci. 2021, 11, 180. [Google Scholar] [CrossRef] [PubMed]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mäcken, J.; Wiegand, M.; Müller, M.; Krawinkel, A.; Linnebank, M. A Mobile App for Measuring Real Time Fatigue in Patients with Multiple Sclerosis: Introducing the Fimo Health App. Brain Sci. 2021, 11, 1235. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091235
Mäcken J, Wiegand M, Müller M, Krawinkel A, Linnebank M. A Mobile App for Measuring Real Time Fatigue in Patients with Multiple Sclerosis: Introducing the Fimo Health App. Brain Sciences. 2021; 11(9):1235. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091235
Chicago/Turabian StyleMäcken, Jana, Marie Wiegand, Mathias Müller, Alexander Krawinkel, and Michael Linnebank. 2021. "A Mobile App for Measuring Real Time Fatigue in Patients with Multiple Sclerosis: Introducing the Fimo Health App" Brain Sciences 11, no. 9: 1235. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11091235