
Persistence of the Effects of the COVID-19 Lockdown on Sleep: A Longitudinal Study

 , , , , ,
, , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
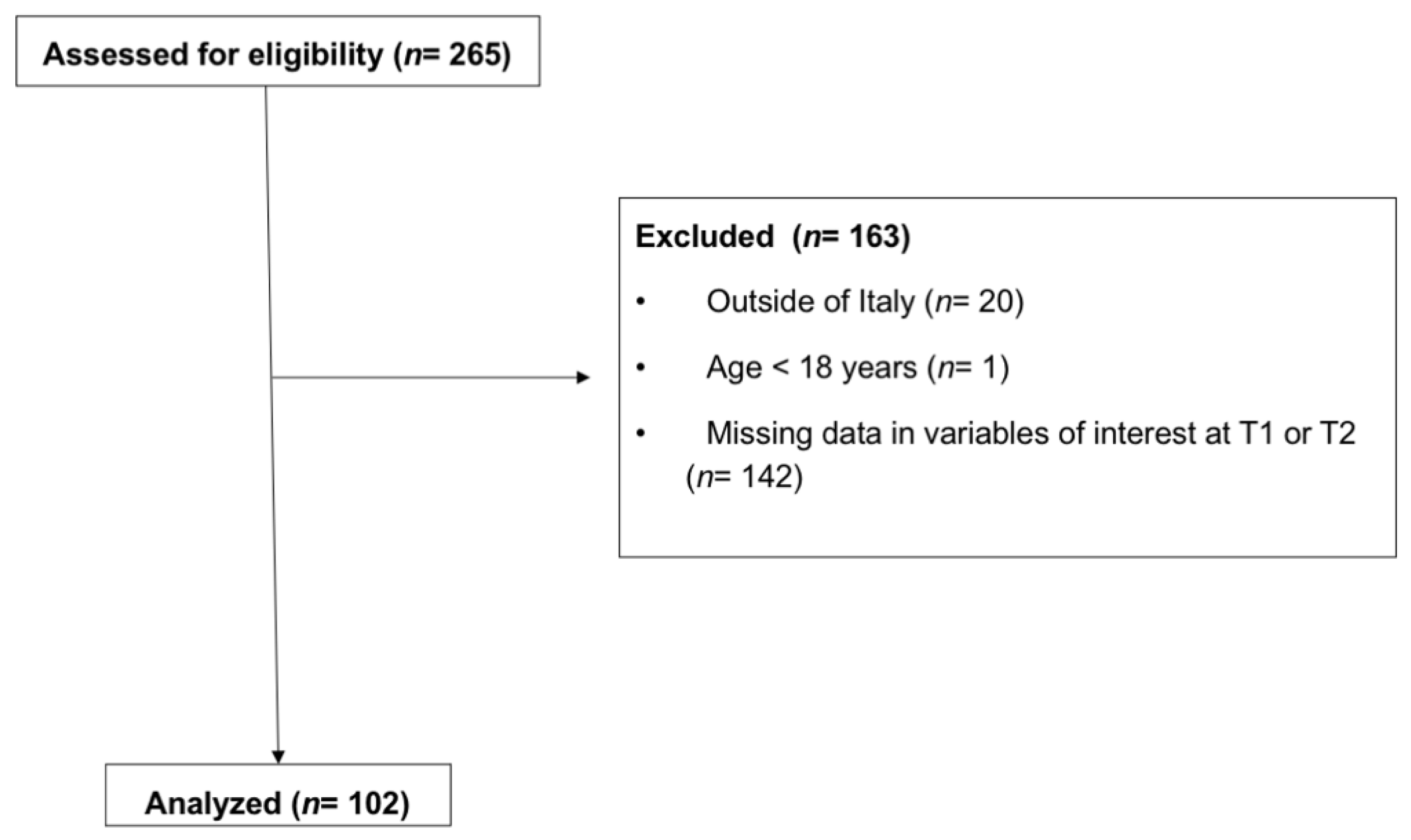
2.1. Design and Participants
2.2. Materials
2.3. Statistics
3. Results
3.1. Sociodemographic, Sleep, and Clinical Characteristics of the Sample
3.2. Post-Lockdown Changes in Clinical and Sleep Measures
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Torales, J.; O’Higgins, M.; Castaldelli-Maia, J.M.; Ventriglio, A. The outbreak of COVID-19 coronavirus and its impact on global mental health. Int. J. Soc. Psychiatry 2020, 66, 317–320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahrami, H.; BaHammam, A.S.; Bragazzi, N.L.; Saif, Z.; Faris, M.; Vitiello, M.V. Sleep problems during the COVID-19 pandemic by population: A systematic review and meta-analysis. J. Clin. Sleep Med. 2021, 17, 299–313. [Google Scholar] [CrossRef] [PubMed]
- Casagrande, M.; Favieri, F.; Tambelli, R. The enemy who sealed the world: Effects quarantine due to the COVID-19 on sleep quality, anxiety, and psychological distress in the Italian population. Sleep Med. 2020, 75, 12–20. [Google Scholar] [CrossRef]
- Cellini, N.; Canale, N.; Mioni, G.; Costa, S. Changes in sleep pattern, sense of time and digital media use during COVID-19 lockdown in Italy. J. Sleep Res. 2020, 29, e13074. [Google Scholar] [CrossRef] [PubMed]
- Franceschini, C.; Musetti, A.; Zenesini, C.; Palagini, L.; Scarpelli, S.; Quattropani, M.C.; Lenzo, V.; Freda, M.F.; Lemmo, D.; Vegni, E.; et al. Poor Sleep Quality and Its Consequences on Mental Health during the COVID-19 Lockdown in Italy. Front. Psychol. 2020, 11, 574475. [Google Scholar] [CrossRef] [PubMed]
- Kocevska, D.; Blanken, T.F.; Van Someren, E.J.W.; Rösler, L. Sleep quality during the COVID-19 pandemic: Not one size fits all. Sleep Med. 2020, 76, 86–88. [Google Scholar] [CrossRef]
- Holzinger, B.; Mayer, L.; Nierwetberg, F.; Klösch, G. COVID-19 lockdown—Are Austrians finally able to compensate their sleep debt? Sleep Med. X 2021, 3, 100032. [Google Scholar] [CrossRef]
- Alfonsi, V.; Gorgoni, M.; Scarpelli, S.; Zivi, P.; Sdoia, S.; Mari, E.; Fraschetti, A.; Ferlazzo, F.; Giannini, A.M.; De Gennaro, L. COVID-19 lockdown and poor sleep quality: Not the whole story. J. Sleep Res. 2021, 30, e13368. [Google Scholar] [CrossRef]
- Morin, C.M.; Bjorvatn, B.; Chung, F.; Holzinger, B.; Partinen, M.; Penzel, T.; Ivers, H.; Wing, Y.K.; Chan, N.Y.; Merikanto, I.; et al. Insomnia, anxiety, and depression during the COVID-19 pandemic: An international collaborative study. Sleep Med. 2021, 87, 38–45. [Google Scholar] [CrossRef]
- Altena, E.; Baglioni, C.; Espie, C.A.; Ellis, J.; Gavriloff, D.; Holzinger, B.; Schlarb, A.; Frase, L.; Jernelöv, S.; Riemann, D. Dealing with sleep problems during home confinement due to the COVID-19 outbreak: Practical recommendations from a task force of the European CBT-I Academy. J. Sleep Res. 2020, 29, e13052. [Google Scholar] [CrossRef]
- Salfi, F.; Lauriola, M.; Amicucci, G.; Corigliano, D.; Viselli, L.; Tempesta, D.; Ferrara, M. Gender-related time course of sleep disturbances and psychological symptoms during the COVID-19 lockdown: A longitudinal study on the Italian population. Neurobiol. Stress 2020, 13, 100259. [Google Scholar] [CrossRef]
- Salfi, F.; Amicucci, G.; Corigliano, D.; D’Atri, A.; Viselli, L.; Tempesta, D.; Ferrara, M. Changes of evening exposure to electronic devices during the COVID-19 lockdown affect the time course of sleep disturbances. Sleep 2021, 44, zsab080. [Google Scholar] [CrossRef]
- Gorgoni, M.; Scarpelli, S.; Alfonsi, V.; Annarumma, L.; Cordone, S.; Stravolo, S.; De Gennaro, L. Pandemic dreams: Quantitative and qualitative features of the oneiric activity during the lockdown due to COVID-19 in Italy. Sleep Med. 2021, 81, 20–32. [Google Scholar] [CrossRef] [PubMed]
- Salfi, F.; D’Atri, A.; Tempesta, D.; Ferrara, M. Sleeping under the waves: A longitudinal study across the contagion peaks of the COVID-19 pandemic in Italy. J. Sleep Res. 2021, 30, e13313. [Google Scholar] [CrossRef]
- Pieh, C.; Budimir, S.; Humer, E.; Probst, T. Comparing Mental Health during the COVID-19 Lockdown and 6 Months after the Lockdown in Austria: A Longitudinal Study. Front. Psychiatry 2021, 12, 625973. [Google Scholar] [CrossRef] [PubMed]
- Beck, F.; Leger, D.; Cortaredona, S.; Verger, P.; Peretti-Watel, P.; COCONEL Group. Would we recover better sleep at the end of COVID-19? A relative improvement observed at the population level with the end of the lockdown in France. Sleep Med. 2021, 78, 115–119. [Google Scholar] [CrossRef]
- Pakerson, G.R.; Broadhead, W.E.; Tse, C.K. Development of the 17-item Duke health profile. Fam. Pract. 1991, 8, 396–401. [Google Scholar] [CrossRef]
- Scarpelli, S.; Gorgoni, M.; Alfonsi, V.; Annarumma, L.; Di Natale, V.; Pezza, E.; De Gennaro, L. The impact of the end of COVID confinement on pandemic dreams, as assessed by a weekly sleep diary: A longitudinal investigation in Italy. J. Sleep Res. 2021, e13429. [Google Scholar] [CrossRef] [PubMed]
- Scarpelli, S.; Alfonsi, V.; Mangiaruga, A.; Musetti, A.; Quattropani, M.C.; Lenzo, V.; Freda, M.F.; Lemmo, D.; Vegni, E.; Borghi, L.; et al. Pandemic nightmares: Effects on dream activity of the COVID-19 lockdown in Italy. J. Sleep Res. 2021, 30, e13300. [Google Scholar] [CrossRef]
- Scarpelli, S.; Alfonsi, V.; D’Anselmo, A.; Gorgoni, M.; Musetti, A.; Plazzi, G.; De Gennaro, L.; Franceschini, C. Dream Activity in Narcoleptic Patients During the COVID-19 Lockdown in Italy. Front. Psychol. 2021, 12, 681569. [Google Scholar] [CrossRef]
- Pietrantonio, F.; De Gennaro, L.; Di Paolo, M.C.; Solano, L. The Impact of Event Scale: Validation of an Italian version. J. Psychosom. Res. 2003, 55, 389–393. [Google Scholar] [CrossRef]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A measure of subjective stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Curcio, G.; Tempesta, D.; Scarlata, S.; Marzano, C.; Moroni, F.; Rossini, P.M.; Ferrara, M.; De Gennaro, L. Validity of the Italian Version of the Pittsburgh Sleep Quality Index (PSQI). Neurol. Sci. 2013, 34, 511–519. [Google Scholar] [CrossRef] [PubMed]
- Palagini, L.; Manni, R. Misurare il Sonno; Minerva Medica: Torino, Italy, 2016. [Google Scholar]
- Nicassio, P.M.; Mendlowitz, D.R.; Fussell, J.J.; Petras, L. The phenomenology of the pre-sleep state: The development of the pre-sleep arousal scale. Behav. Res. Ther. 1985, 23, 263–271. [Google Scholar] [CrossRef]
- Puzino, K.; Amatrudo, G.; Sullivan, A.; Vgontzas, A.N.; Fernandez-Mendoza, J. Clinical Significance and Cut-Off Scores for the Pre-Sleep Arousal Scale in Chronic Insomnia Disorder: A Replication in a Clinical Sample. Behav. Sleep Med. 2020, 18, 705–718. [Google Scholar] [CrossRef]
- Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Pre-sleep arousal and sleep quality during the COVID-19 lockdown in Italy. Sleep Med. 2021, 88, 46–57. [Google Scholar] [CrossRef] [PubMed]
- Natale, V. Validazione di una scala ridotta di mattutinità (r-MEQ). Boll. Psicol. Appl. 1999, 229, 19–26. [Google Scholar]
- Gao, C.; Scullin, M.K. Sleep health early in the coronavirus disease 2019 (COVID-19) outbreak in the United States: Integrating longitudinal, cross-sectional, and retrospective recall data. Sleep Med. 2020, 73, 1–10. [Google Scholar] [CrossRef]
- Marelli, S.; Castelnuovo, A.; Somma, A.; Castronovo, V.; Mombelli, S.; Bottoni, D.; Leitner, C.; Fossati, A.; Ferini-Strambi, L. Impact of COVID-19 lockdown on sleep quality in university students and administration staff. J. Neurol. 2020, 268, 8–15. [Google Scholar] [CrossRef]
- Leone, M.J.; Sigman, M.; Golombek, D.A. Effects of lockdown on human sleep and chronotype during the COVID-19 pandemic. Curr. Biol. 2020, 30, R930–R931. [Google Scholar] [CrossRef]
- Korman, M.; Tkachev, V.; Reis, C.; Komada, Y.; Kitamura, S.; Gubin, D.; Kumar, V.; Roenneberg, T. COVID-19-mandated social restrictions unveil the impact of social time pressure on sleep and body clock. Sci. Rep. 2020, 10, 22225. [Google Scholar] [CrossRef] [PubMed]
- Bacaro, V.; Chiabudini, M.; Buonanno, C.; De Bartolo, P.; Riemann, D.; Mancini, F.; Baglioni, C. Insomnia in the Italian Population during Covid-19 Outbreak: A Snapshot on One Major Risk Factor for Depression and Anxiety. Front. Psychiatry 2020, 11, 579107. [Google Scholar] [CrossRef]
- Alfonsi, V.; Gorgoni, M.; Scarpelli, S.; Zivi, P.; Sdoia, S.; Mari, E.; Quaglieri, A.; Ferlazzo, F.; Giannini, A.M.; De Gennaro, L. Changes in slep pattern and dream activity across and after the COVID-19 lockdown in Italy: A longitudinal observational study. J. Sleep Res. 2021, e13500. [Google Scholar] [CrossRef]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: A review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Li, H.Y.; Cao, H.; Leung, D.Y.P.; Mak, Y.W. The psychological impacts of a COVID-19 outbreak on college students in China: A longitudinal study. Int. J. Environ. Res. Pub. Health 2020, 17, 3933. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; McIntyre, R.S.; Choo, F.N.; Tran, B.; Ho, R.; Sharma, V.; et al. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. 2020, 87, 40–48. [Google Scholar] [CrossRef] [PubMed]
- Daly, M.; Robinson, E. Psychological distress and adaptation to the COVID-19 crisis in the United States. J. Psychiatr. Res. 2021, 136, 603–609. [Google Scholar] [CrossRef]
- Daly, M.; Sutin, A.; Robinson, E. Longitudinal changes in mental health and the COVID-19 pandemic: Evidence from the UK Household Longitudinal Study. Psychol. Med. 2020, 1–10. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall Sample (n = 102) | ||
|---|---|---|
| N | % | |
| Demographic features | ||
| Gender | ||
| Male | 17 | 16.67 |
| Female | 85 | 83.33 |
| Age (Mean ± SE: 36.69 ± 1.50 years) | ||
| 18–25 | 35 | 34.31 |
| 26–30 | 15 | 14.71 |
| 31–40 | 15 | 14.71 |
| 41–50 | 13 | 12.74 |
| >50 | 24 | 23.53 |
| Education | ||
| Middle school | 1 | 0.98 |
| High school | 36 | 35.29 |
| Undergraduate/Graduate | 62 | 60.78 |
| Post-graduate | 3 | 2.94 |
| Italian area | ||
| North | 43 | 42.15 |
| Center | 46 | 45.09 |
| South | 13 | 12.75 |
| Having a partner | ||
| No | 41 | 40.20 |
| Yes | 61 | 59.80 |
| Having children | ||
| No | 78 | 76.47 |
| Yes | 24 | 23.53 |
| Home size (Mean ± SE: 111.00 ± 6.27 sq. m.) | ||
| Lockdown (T1) a | Post-lockdown (T2) b | p | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| COVID-19-related features | |||||
| Work | 0.27 | ||||
| No | 47 | 46.08 | 52 | 50.98 | |
| Yes | 55 | 53.92 | 50 | 49.02 | |
| Cohabitation | 0.37 | ||||
| No | 23 | 22.55 | 20 | 19.61 | |
| Yes | 79 | 77.45 | 82 | 80.39 | |
| Knowing a relative/friend infected by COVID-19 | 0.08 | ||||
| No | 54 | 52.94 | 45 | 44.12 | |
| Yes | 48 | 47.06 | 57 | 55.88 | |
| Sleep and clinical features | |||||
| rMEQ | 0.27 | ||||
| Evening type | 24 | 23.53 | 30 | 29.41 | |
| Neutral type | 51 | 50.00 | 46 | 45.10 | |
| Morning type | 27 | 26.47 | 26 | 25.49 | |
| PSQI Global | 0.85 | ||||
| PSQI ≤ 5 | 39 | 38.24 | 41 | 40.20 | |
| PSQI > 5 | 63 | 61.76 | 61 | 59.80 | |
| PSAS-Cognitive | 0.54 | ||||
| PSAS-C ≤ 19 | 52 | 50.98 | 56 | 54.90 | |
| PSAS-C > 19 | 50 | 49.02 | 46 | 45.10 | |
| PSAS-Somatic | 1.00 | ||||
| PSAS-S ≤ 13 | 61 | 59.80 | 60 | 58.82 | |
| PSAS-S > 13 | 41 | 40.20 | 42 | 41.18 | |
| BDI | 0.24 | ||||
| BDI ≤ 13 | 71 | 69.61 | 65 | 63.73 | |
| BDI > 13 | 31 | 30.39 | 37 | 36.27 | |
| IES | * 0.001 | ||||
| IES ≤ 25 | 27 | 26.47 | 45 | 44.12 | |
| IES > 25 | 75 | 73.53 | 57 | 55.88 | |
| Current intake of medication | 0.45 | ||||
| No | 52 | 50.98 | 55 | 53.92 | |
| Yes | 50 | 49.02 | 47 | 46.08 | |
| Positive Predictive Value | Negative Predictive Value | |
|---|---|---|
| IES | 68% | 77.8% |
| BDI | 80.6% | 83.1% |
| PSQI | 76.2% | 66.7% |
| PSAS-C | 72% | 80.8% |
| PSAS-S | 68.3% | 77% |
| Lockdown (T1) a Mean ± SE | Post-Lockdown (T2) b Mean ± SE | F1,101 | p | |
|---|---|---|---|---|
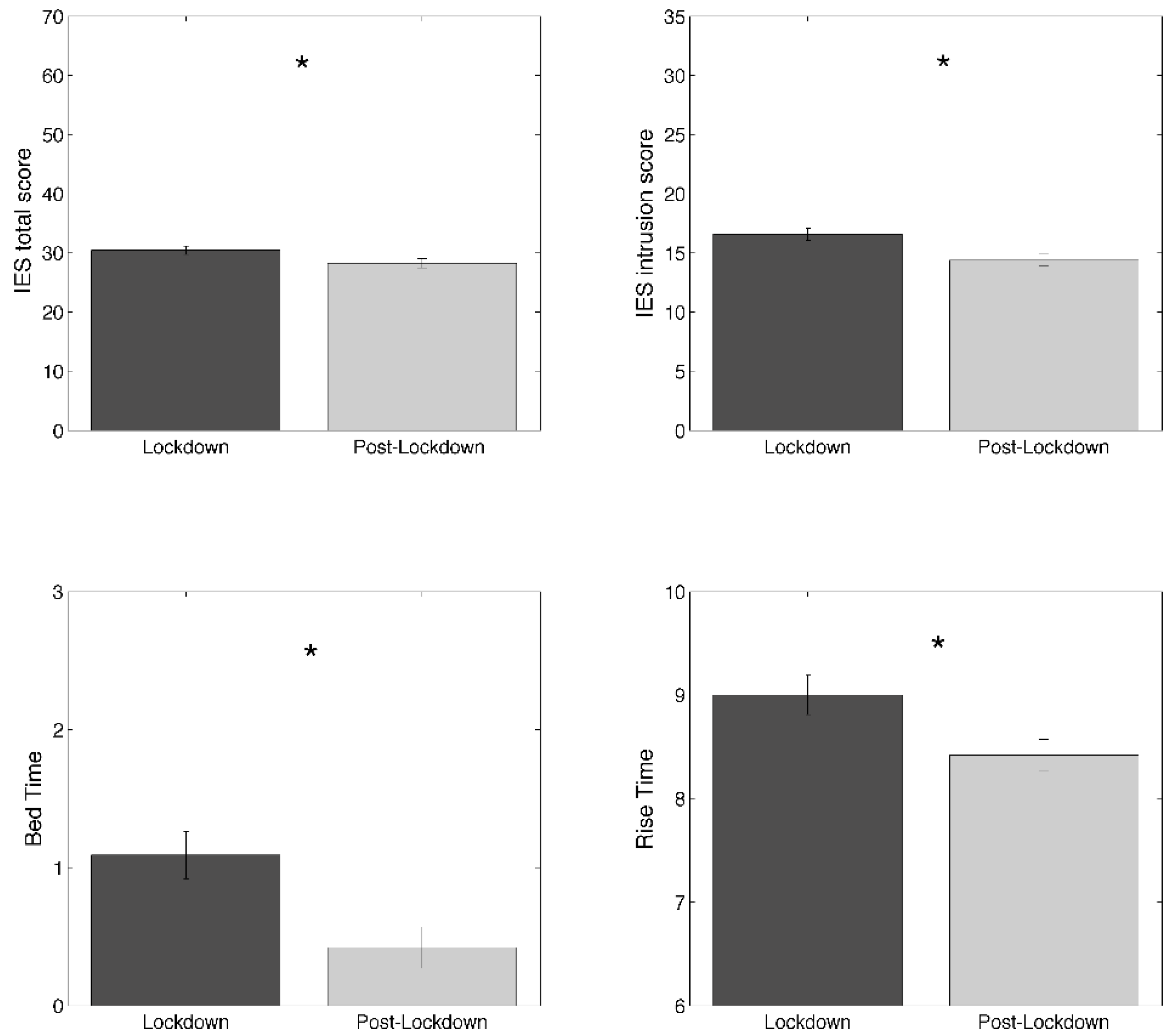
| IES total score | 30.43 ± 0.73 | 28.25 ± 0.80 | 14.34 | * 0.0003 |
| IES Intrusion | 16.57 ± 0.51 | 14.38 ± 0.51 | 31.58 | * <0.00001 |
| IES Avoidance | 13.86 ± 0.38 | 13.87 ± 0.41 | 0.001 | 0.98 |
| BDI | 11.73 ± 0.89 | 12.08 ± 0.90 | 0.24 | 0.62 |
| rMEQ | 14.43 ± 0.39 | 14.18 ± 0.40 | 1.52 | 0.22 |
| PSQI—Global Score | 6.75 ± 0.36 | 6.75 ± 0.34 | 0.00 | 1.00 |
| PSQI C1—Subjective sleep quality | 1.52 ± 0.09 | 1.41 ± 0.08 | 1.88 | 0.17 |
| PSQI C2—Sleep latency | 1.57 ± 0.12 | 1.44 ± 0.11 | 2.35 | 0.13 |
| PSQI C3—Sleep duration | 0.75 ± 0.07 | 0.83 ± 0.07 | 1.53 | 0.22 |
| PSQI C4—Habitual sleep efficiency | 0.33 ± 0.08 | 0.50 ± 0.09 | 2.98 | 0.09 |
| PSQI C5—Sleep disturbance | 1.35 ± 0.05 | 1.23 ± 0.05 | 3.90 | 0.051 |
| PSQI C6—Sleeping medication | 0.42 ± 0.10 | 0.46 ± 0.10 | 0.35 | 0.56 |
| PSQI C7—Daytime dysfunctions | 0.80 ± 0.07 | 0.87 ± 0.07 | 1.09 | 0.30 |
| Total bedtime (min) | 471.75 ± 8.73 | 480.06 ± 8.15 | 0.74 | 0.39 |
| Total sleep time (min) | 424.41 ± 7.93 | 418.14 ± 7.61 | 1.03 | 0.31 |
| Bed time | 01.09 ± 0.17 | 00.42 ± 0.15 | 6.10 | * 0.02 |
| Rise time | 09.00 ± 0.19 | 8.42 ± 0.15 | 5.30 | * 0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gorgoni, M.; Scarpelli, S.; Mangiaruga, A.; Alfonsi, V.; Bonsignore, M.R.; Fanfulla, F.; Ferini-Strambi, L.; Nobili, L.; Plazzi, G.; De Gennaro, L.; et al. Persistence of the Effects of the COVID-19 Lockdown on Sleep: A Longitudinal Study. Brain Sci. 2021, 11, 1520. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111520
Gorgoni M, Scarpelli S, Mangiaruga A, Alfonsi V, Bonsignore MR, Fanfulla F, Ferini-Strambi L, Nobili L, Plazzi G, De Gennaro L, et al. Persistence of the Effects of the COVID-19 Lockdown on Sleep: A Longitudinal Study. Brain Sciences. 2021; 11(11):1520. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111520
Chicago/Turabian StyleGorgoni, Maurizio, Serena Scarpelli, Anastasia Mangiaruga, Valentina Alfonsi, Maria R. Bonsignore, Francesco Fanfulla, Luigi Ferini-Strambi, Lino Nobili, Giuseppe Plazzi, Luigi De Gennaro, and et al. 2021. "Persistence of the Effects of the COVID-19 Lockdown on Sleep: A Longitudinal Study" Brain Sciences 11, no. 11: 1520. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci11111520