

Application of Multi-Dimensional Intelligent Visual Quantitative Assessment System to Evaluate Hand Function Rehabilitation in Stroke Patients
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. General Information
2.2. Methods
- (1)
- MDIVQAS: Based on the pathological motor characteristics of hemiplegic hand and a set of post-stroke hand function rehabilitation evaluation actions corresponding to the Brunnstrom scale, Fugl-Meyer Rating Scale and range of motion measurement, it is a computer-aided technology-based assessment tool. Using the comprehensive quantitative evaluation method of healthy hand modeling and comparison evaluation of the affected hand, the 3D spatial position and motion vector information of various joints of the phalanx, metacarpal and wrist were acquired in real time with the help of video equipment, and then various motion parameters of the hand joint were analyzed as the system parameters of the hand function evaluation standard. In order to prevent the ambiguity and subjectivity in the guidance process of the standard movement demonstration, At the bottom left of the screen, there is a 3D animation of the action being evaluated to achieve a consistent demonstration of standard hand movements. The assessment items included three parts as forearm, wrist and hand, with a total of 10 movements, including ulnar wrist deviation, wrist dorsiextension, five fingers adduction and abduction, forearm pronation, forearm supination, spherical grip, cylindrical grip, thumb flexion and extension, thumb abduction and thumb rotation.
- (2)
- Measuring AROM with protractor: A universal protractor was used to measure the forearm pronation, forearm supination, ulnar deviation, wrist dorsiextension and the angle between the fingers of the five fingers [9].
- (3)
- FMA-UE [15,16]: It mainly includes movement, speed, coordination and reflex activities, with a total of 66 points, and each item is scored on a 3-level scale: that is, 0 points, unable to perform; 1 point, partially implemented; 2 points, fully implemented. Among them FMA-W/H is a part of the FMA rating scale, which evaluates the wrist and hand. There are 12 items in total, each item is 0~2 points, full score is 24 points. The higher the score, the better the motor function of the upper limb is indicated.
- (4)
- Brunnstrom Scale [7,17]: upper limb and hand parts; each is divided into stage I–VI, and the higher the level, the better the motor function. Stage I: no exercise; Stage II: slight flexion; Stage III: flexion but not extension; Stage IV: the thumb can be pinched and loosened, and the fingers can be extended semi-randomly in a small area; Stage V: can do spherical or cylindrical grip, and can be free to extend the whole finger, but the range of size is not equal; Stage VI: full range extension of various grips, but with less speed and accuracy than the healthy side.
- (5)
- ARAT [18,19]: Consisting of 4 subscales (grasp, grip, pinch and gross motion), which mainly evaluates the ability of the affected hand to handle objects of different sizes, weights and shapes. ARAT requires a standardized assessment toolbox, consisting of 19 items with a full score of 57, and each item is scored in a 4-point order (0: unable to complete any part of the task within 60 s, 1: complete part of the task within 60 s, 2: The task is completed, but the difficulty is very high or the time is too long (5~60 s), 3 points: the normal completion within 5 s). Each of ARAT’s subscales is arranged in a hierarchical order, testing the most difficult items first, then the easiest and then increasing the items in turn. The higher the score, the better the feature.
2.3. MDIVQAS
2.3.1. Overall Design Scheme of MDIVQAS
2.3.2. Hardware Platform of MDIVQAS
2.4. Statistical Analysis
3. Results
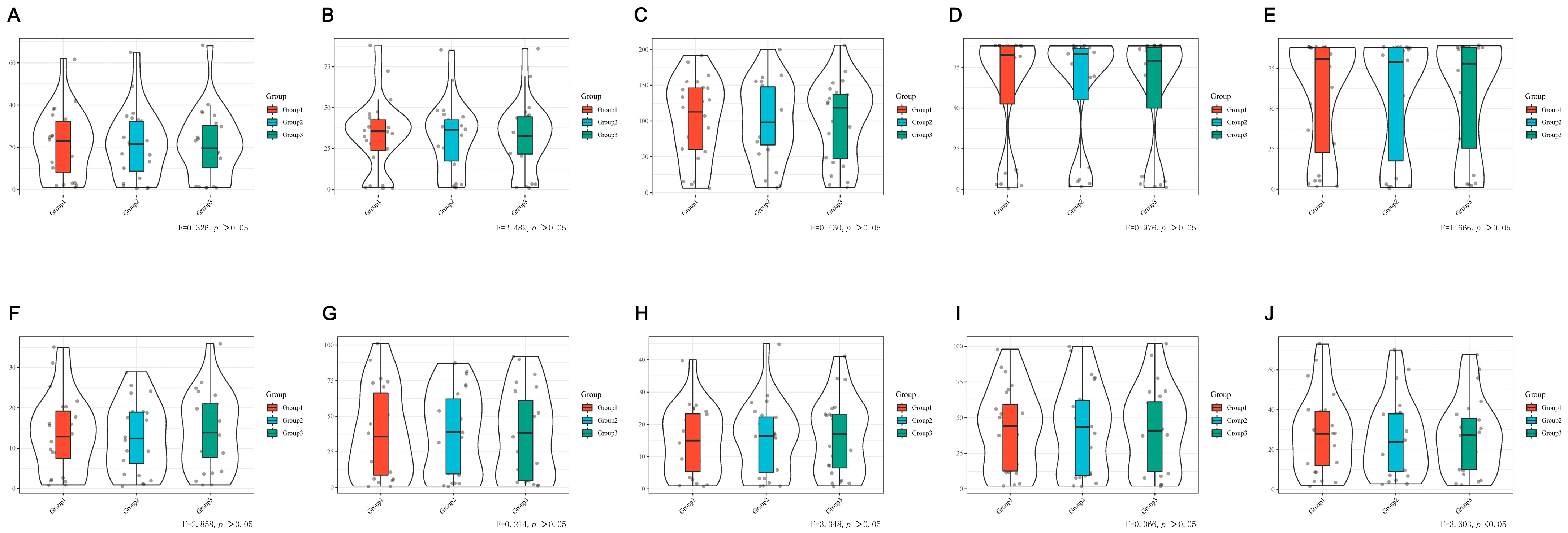
3.1. Reliability of MDIVQAS
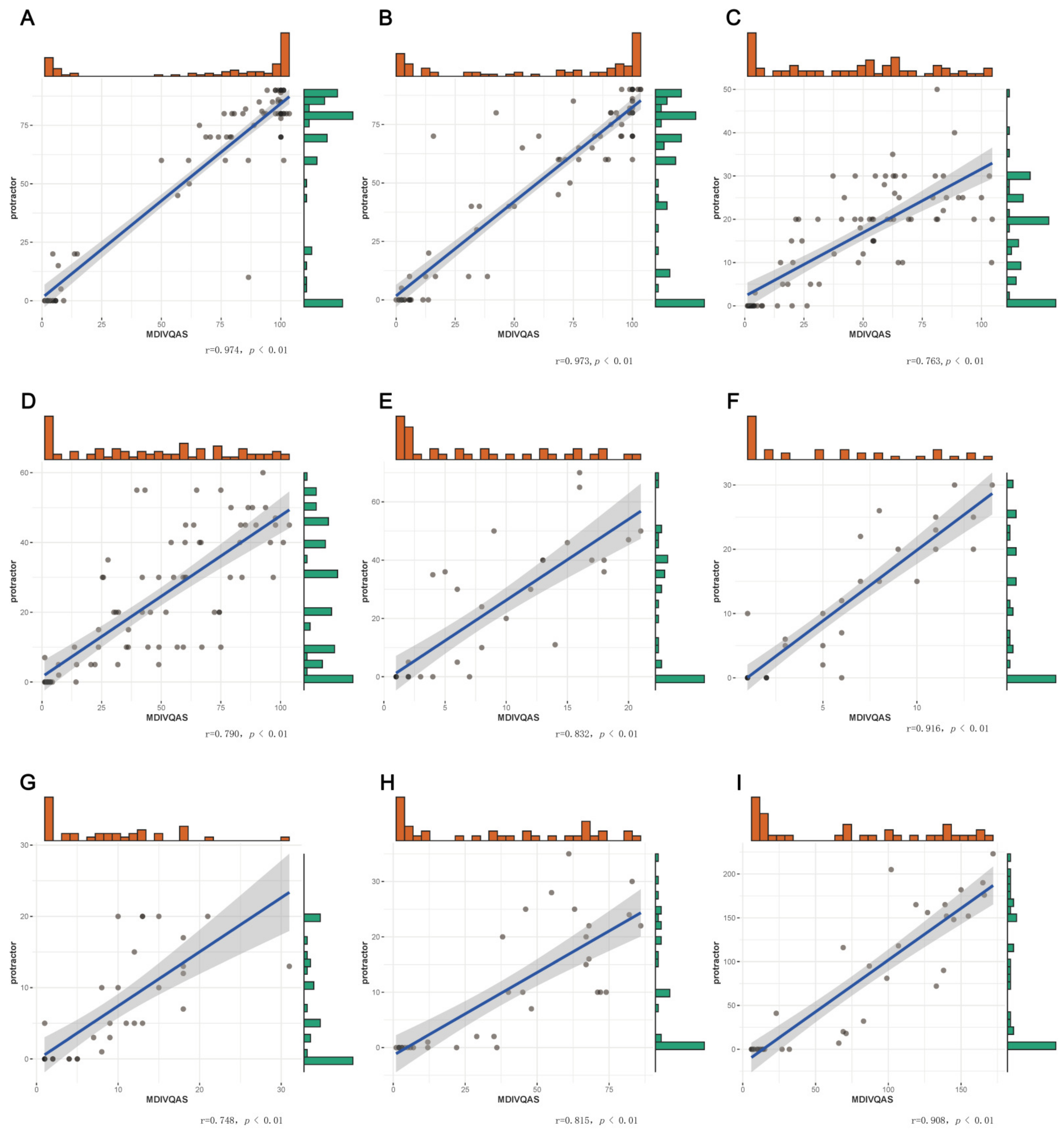
3.2. Validity of MDIVQAS
3.2.1. Correlation between MDIVQAS, FMA-W/H, Brunnstrom and ARAT Assessment
3.2.2. Correlations MDIVQAS and Protractor Measurement
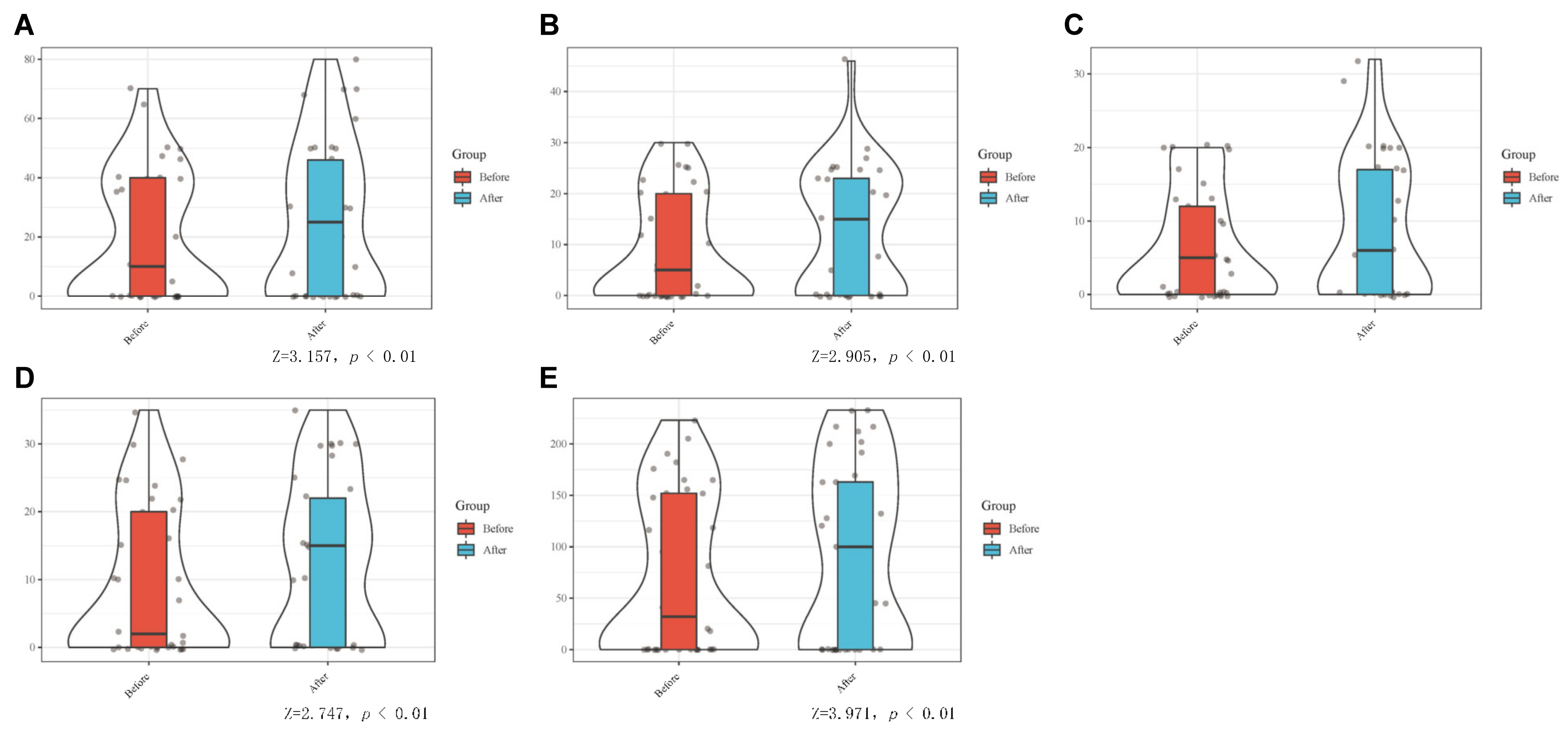
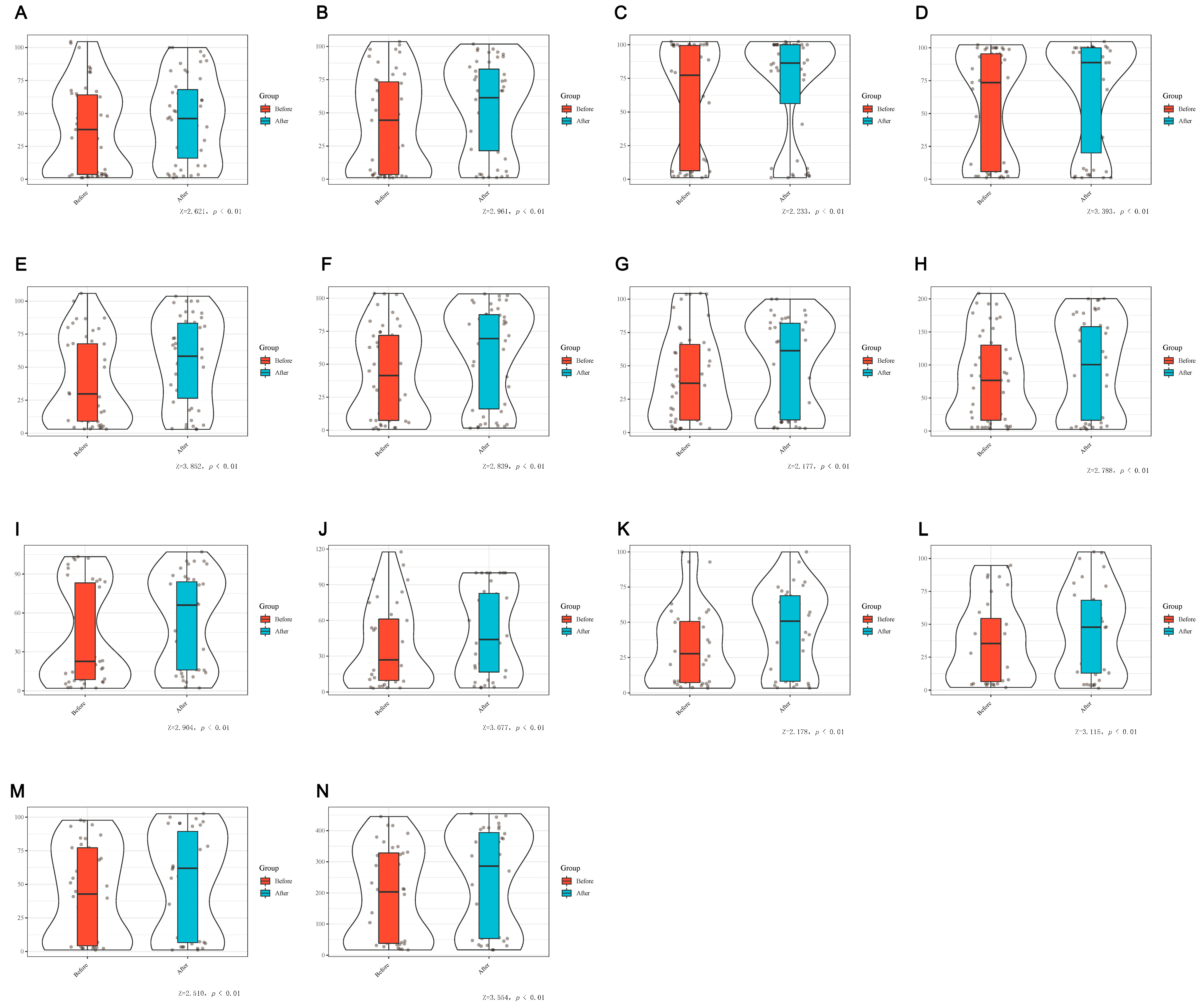
3.3. Reactivity before and after Treatment
3.3.1. Comparison of Differences of MDIVQAS, FMA-UE, FMA-W/H, Brunnstrom and ARAT before and after Treatment
3.3.2. Comparison of the Difference between MDIVQAS and Protractor Measurement of AROM in the Increase of Joint Motion before and after Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Feigin, V.L.; Stark, B.A.; Johnson, C.O.; Roth, G.A.; Bisignano, C.; Abady, G.G.; Abbasifard, M.; Abbasi-Kangevari, M.; Abd-Allah, F.; Abedi, V.; et al. Global, regional, and national burden of stroke and its risk factors, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. 2021, 20, 795–820. [Google Scholar] [CrossRef] [PubMed]
- Pila, O.; Duret, C.; Laborne, F.X.; Gracies, J.M.; Bayle, N.; Hutin, E. Pattern of improvement in upper limb pointing task kinematics after a 3-month training program with robotic assistance in stroke. J. Neuroeng. Rehabil. 2017, 14, 105. [Google Scholar] [CrossRef]
- Franceschini, M.; Goffredo, M.; Pournajaf, S.; Paravati, S.; Agosti, M.; De Pisi, F.; Galafate, D.; Posteraro, F. Predictors of activities of daily living outcomes after upper limb robot-assisted therapy in subacute stroke patients. PLoS ONE 2018, 13, e193235. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Veldema, J.; Nowak, D.A.; Gharabaghi, A. Resting motor threshold in the course of hand motor recovery after stroke: A systematic review. J. NeuroEng. Rehabil. 2021, 18, 158. [Google Scholar] [CrossRef] [PubMed]
- Pan, B.; Huang, Z.; Jin, T.; Wu, J.; Zhang, Z.; Shen, Y. Motor Function Assessment of Upper Limb in Stroke Patients. J. Healthc. Eng. 2021, 2021, 6621950. [Google Scholar] [CrossRef]
- Hernandez, E.D.; Galeano, C.P.; Barbosa, N.E.; Forero, S.M.; Nordin, Å.; Sunnerhagen, K.S.; Alt Murphy, M. Intra- and inter-rater reliability of Fugl-Meyer Assessment of Upper Extremity in stroke. J. Rehabil. Med. 2019, 51, 652–659. [Google Scholar] [CrossRef] [Green Version]
- Meng, L.; Jiang, X.; Qin, H.; Fan, J.; Zeng, Z.; Chen, C.; Zhang, A.; Dai, C.; Wu, X.; Akay, Y.M.; et al. Automatic Upper-Limb Brunnstrom Recovery Stage Evaluation via Daily Activity Monitoring. IEEE Trans. Neural Syst. Rehabil. Eng. 2022, 30, 2589–2599. [Google Scholar] [CrossRef]
- Nakazono, T.; Takahashi, K.; Suzuki, Y.; Mizuno, K.; Nomura, Y.; Hiraga, Y.; Matsumoto, S.; Nishiyama, K.; Fukuda, M. Reliability and validity of Japanese version of Fugl-Meyer assessment for the lower extremities. Top. Stroke Rehabil. 2022, 29, 125–132. [Google Scholar] [CrossRef]
- van Kooij, Y.E.; Fink, A.; Nijhuis-van der Sanden, M.W.; Speksnijder, C.M. The reliability and measurement error of protractor-based goniometry of the fingers: A systematic review. J. Hand Ther. 2017, 30, 457–467. [Google Scholar] [CrossRef]
- Wang, C.; Peng, L.; Hou, Z.G.; Li, J.; Zhang, T.; Zhao, J. Quantitative Assessment of Upper-Limb Motor Function for Post-Stroke Rehabilitation Based on Motor Synergy Analysis and Multi-Modality Fusion. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 943–952. [Google Scholar] [CrossRef]
- Sinha, S.; Bhowmick, B.; Chakravarty, K.; Sinha, A.; Das, A. Accurate upper body rehabilitation system using kinect. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Orlando, FL, USA, 16–20 August 2016; Volume 2016, pp. 4605–4609. [Google Scholar]
- Antico, M.; Balletti, N.; Laudato, G.; Lazich, A.; Notarantonio, M.; Oliveto, R.; Ricciardi, S.; Scalabrino, S.; Simeone, J. Postural control assessment via Microsoft Azure Kinect DK: An evaluation study. Comput. Methods Programs Biomed. 2021, 209, 106324. [Google Scholar] [CrossRef]
- Xie, C.; Yang, Q.; Huang, Y.; Su, S.W.; Xu, T.; Song, R. A Hybrid Arm-Hand Rehabilitation Robot With EMG-Based Admittance Controller. IEEE Trans. Biomed. Circuits Syst. 2021, 15, 1332–1342. [Google Scholar] [CrossRef]
- Cerebrovascular Disease Group Chinese Association of Neurology; Zeng, J.S.; Liu, M.; Cui, L.Y. Diagnostic criteria of cerebrovascular diseases in China (version 2019). Chin. J. Neurol. 2019, 52, 710–715. [Google Scholar]
- Fugl-Meyer, A.R.; Jääskö, L.; Leyman, I.; Olsson, S.; Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 1975, 7, 13–31. [Google Scholar]
- Lee, S.; Lee, Y.S.; Kim, J. Automated Evaluation of Upper-Limb Motor Function Impairment Using Fugl-Meyer Assessment. IEEE Trans. Neural Syst. Rehabil. Eng. 2018, 26, 125–134. [Google Scholar] [CrossRef]
- Brunnstrom, S. Motor testing procedures in hemiplegia: Based on sequential recovery stages. Phys. Ther. 1966, 46, 357–375. [Google Scholar] [CrossRef] [Green Version]
- Lyle, R.C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 1981, 4, 483–492. [Google Scholar] [CrossRef]
- Zhao, J.L.; Zhang, T.; Xu, Z.Q.; Ding, M.H.; Leng, Y.; Bian, R.H.; Mao, Y.R.; Huang, D.F. Responsiveness and Predictive Ability of the Chinese Version of the Action Research Arm Test in People with Cerebral Infarction. BioMed Res. Int. 2019, 2019, 8270187. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Z.; Lu, X.; Zhu, M.; Zhao, S.; Zhong, B.; Jie, J.; Chen, S. Post-stroke hand rehabilitation assessment of multi-terminal cloud platform design. Electron. Meas. Technol. 2018, 41, 10–14. [Google Scholar]
- Braitman, L.E. Statistical power analysis in medical research. Ann. Intern. Med. 1983, 99, 269–271. [Google Scholar] [CrossRef]
- Loria, A. Tamaño de muestra de protocolos clínicos. Gac. Médica México 2018, 154, 409–412. [Google Scholar] [CrossRef] [PubMed]
- Murphy, M.A.; Björkdahl, A.; Forsberg-Wärleby, G.; Persson, C.U. Implementation of evidence-based assessment of upper extremity in stroke rehabilitation: From evidence to clinical practice. J. Rehabil. Med. 2021, 53, m148. [Google Scholar] [CrossRef] [PubMed]
- de los Reyes-Guzmán, A.; Dimbwadyo-Terrer, I.; Trincado-Alonso, F.; Monasterio-Huelin, F.; Torricelli, D.; Gil-Agudo, A. Quantitative assessment based on kinematic measures of functional impairments during upper extremity movements: A review. Clin. Biomech. 2014, 29, 719–727. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.; Chen, S.; Qian, Y.; Lu, X.; Long, H.; Cui, X.; Jia, J. Feasibility of Multi-dimensional Visual Hand Function Rehabilitation Quantitative Assessment System in Assess-ing Hand Function for Stroke Patients. Chin. J. Rehabil. Theory Pract. 2018, 24, 1380–1383. [Google Scholar]
- Lu, Y.; Ling, X.; Cong, W.; Zhao, Z.; Jie, J.; Chen, S. Quantitative evaluation method of wrist extension based on hand function evaluation system. Electron. Meas. Technol. 2017, 40, 127–133. [Google Scholar]
- Ma, H.; Shi, Y.; Mu, Y.; Jia, J.; Lu, X.; Fu, J.; Chu, T.; Li, D.; Zhu, L.; Wang, B. The reliability and validity of multi-dimensional, quantitative video evaluation of the hand function of stroke survivors. Chin. J. Phys. Med. Rehabil. 2022, 44, 116–120. [Google Scholar]
- Santisteban, L.; Térémetz, M.; Bleton, J.P.; Baron, J.C.; Maier, M.A.; Lindberg, P.G. Upper Limb Outcome Measures Used in Stroke Rehabilitation Studies: A Systematic Literature Review. PLoS ONE 2016, 11, e154792. [Google Scholar] [CrossRef]
- Öhberg, F.; Bäcklund, T.; Sundström, N.; Grip, H. Portable Sensors Add Reliable Kinematic Measures to the Assessment of Upper Extremity Function. Sensors 2019, 19, 1241. [Google Scholar] [CrossRef] [Green Version]
- Yurkewich, A.; Kozak, I.J.; Hebert, D.; Wang, R.H.; Mihailidis, A. Hand Extension Robot Orthosis (HERO) Grip Glove: Enabling independence amongst persons with severe hand impairments after stroke. J. Neuroeng. Rehabil. 2020, 17, 33. [Google Scholar] [CrossRef] [Green Version]
- Coskunsu, D.K.; Akcay, S.; Ogul, O.E.; Akyol, D.K.; Ozturk, N.; Zileli, F.; Tuzun, B.B.; Krespi, Y. Effects of robotic rehabilitation on recovery of hand functions in acute stroke: A preliminary randomized controlled study. Acta Neurol. Scand. 2022, 146, 499–511. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Movement (n = 24) | Cronbach’s Alpha | N of Items |
|---|---|---|
| Wrist ulnar deviation | 0.989 | 3 |
| Wrist dorsiextension | 0.993 | 3 |
| Finger adduction and abduction | 0.987 | 3 |
| Forearm pronation | 0.998 | 3 |
| Forearm supination | 0.998 | 3 |
| Cylindrical grip | 0.981 | 3 |
| Spherical grip | 0.990 | 3 |
| Thumb abduction | 0.976 | 3 |
| Thumb flexion and extension | 0.989 | 3 |
| Thumb rotation | 0.994 | 3 |
| Hand function 10 movements overall | 0.989 | 30 |
| Item | n | P25 | P50 | P75 | Z | P |
|---|---|---|---|---|---|---|
| Ulnar deviation increase A | 37 | 0.0 | 1.0 | 5.0 | −0.184 b | 0.854 |
| Ulnar deviation increase B | 37 | 0.0 | 0.0 | 6.0 | ||
| Forearm pronation increase A | 37 | −1.5 | 1.0 | 11.5 | −0.516 b | 0.606 |
| Forearm pronation increase B | 37 | 0.0 | 3.0 | 10.0 | ||
| Forearm supination increase A | 37 | −0.5 | 2.0 | 20.0 | −1.034 c | 0.301 |
| Forearm supination increase B | 37 | 0.0 | 0.0 | 10.0 | ||
| Wrist dorsiextension increase A | 37 | −0.5 | 3.0 | 17.5 | −0.403 c | 0.687 |
| Wrist dorsiextension increase B | 37 | 0.0 | 3.0 | 15.0 | ||
| Increase in angle between the fingers 1A | 37 | −0.5 | 1.0 | 7.0 | −1.267 b | 0.205 |
| Increase in angle between the fingers 1B | 37 | 0.0 | 0.0 | 12.0 | ||
| Increase in angle between the fingers 2A | 37 | 0.0 | 2.0 | 5.0 | −0.502 b | 0.616 |
| Increase in angle between the fingers 2B | 37 | 0.0 | 0.0 | 5.0 | ||
| Increase in angle between the fingers 3A | 37 | 0.0 | 1.0 | 4.0 | −0.868 b | 0.386 |
| Increase in angle between the fingers 3B | 37 | 0.0 | 0.0 | 7.0 | ||
| Increase in angle between the fingers 4A | 37 | 0.0 | 1.0 | 2.0 | −1.783 b | 0.075 |
| Increase in angle between the fingers 4B | 37 | 0.0 | 0.0 | 5.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, Y.; Shi, Y.; Ma, H.; Li, D.; Su, T.; Meidege, O.Z.; Wang, B.; Lu, X. Application of Multi-Dimensional Intelligent Visual Quantitative Assessment System to Evaluate Hand Function Rehabilitation in Stroke Patients. Brain Sci. 2022, 12, 1698. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12121698
Du Y, Shi Y, Ma H, Li D, Su T, Meidege OZ, Wang B, Lu X. Application of Multi-Dimensional Intelligent Visual Quantitative Assessment System to Evaluate Hand Function Rehabilitation in Stroke Patients. Brain Sciences. 2022; 12(12):1698. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12121698
Chicago/Turabian StyleDu, Yuying, Yu Shi, Hongmei Ma, Dong Li, Ting Su, Ou Zhabayier Meidege, Baolan Wang, and Xiaofeng Lu. 2022. "Application of Multi-Dimensional Intelligent Visual Quantitative Assessment System to Evaluate Hand Function Rehabilitation in Stroke Patients" Brain Sciences 12, no. 12: 1698. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci12121698