
Characterizing Touch Discrimination Impairment from Pooled Stroke Samples Using the Tactile Discrimination Test: Updated Criteria for Interpretation and Brief Test Version for Use in Clinical Practice Settings

Abstract
:1. Introduction
- characterize the distribution, frequency, and severity of impaired touch discrimination, based on the quantitative TDT, in a larger stroke sample;
- establish updated normative standards and criteria of abnormality using the new PMA scoring;
- compare the distribution and frequency of impaired stroke TDT scores across test versions (50, 25, 15, and 12 trials);
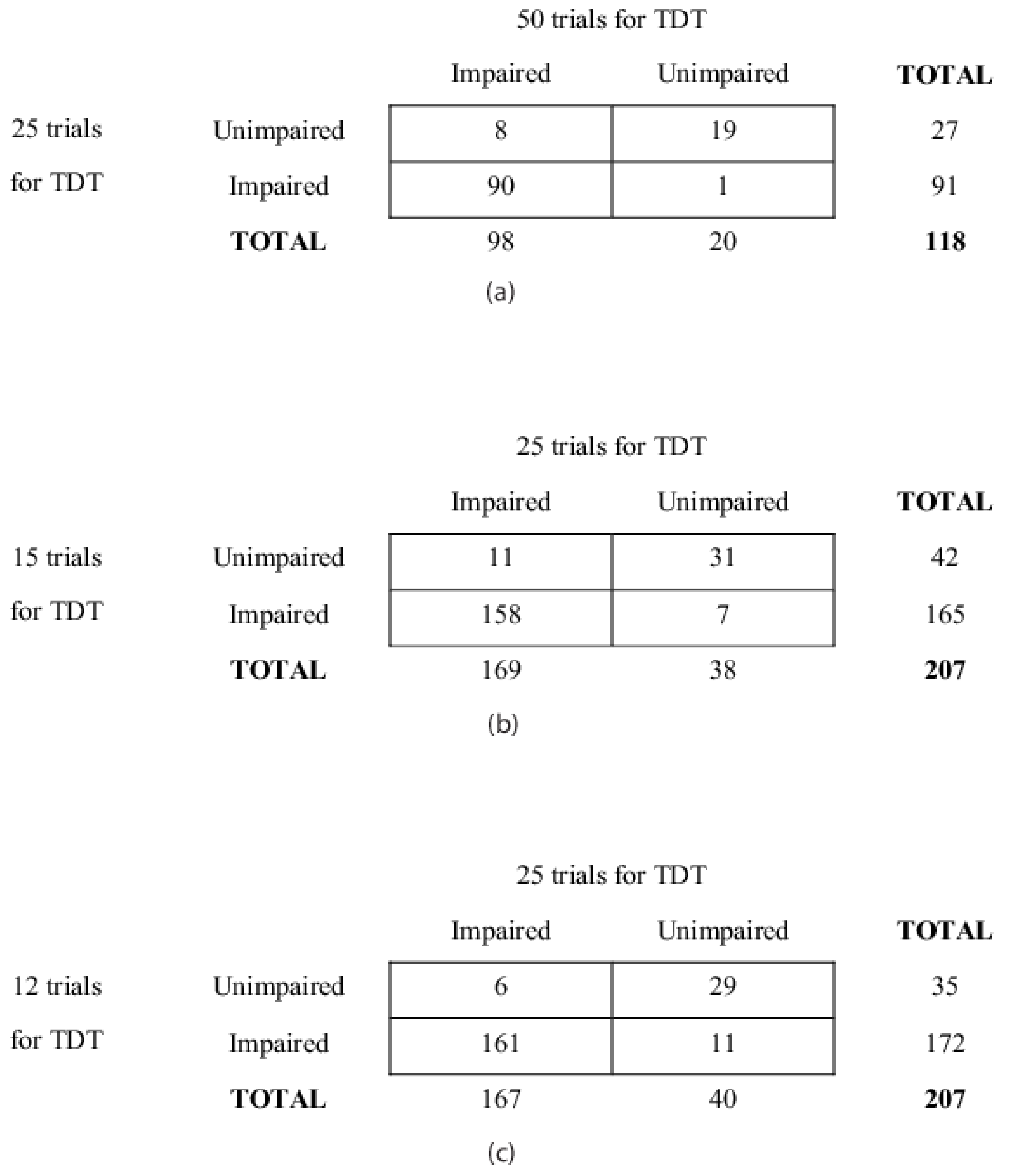
- determine the sensitivity and specificity for briefer versions of the TDT (25, 15, and 12 trials) to accurately assess the presence of somatosensory loss in stroke survivors.
2. Materials and Methods
2.1. Study Design and Samples
2.2. Measure: Tactile Discrimination Test (TDT)
2.3. Data Analysis
3. Results
3.1. Background Characteristics of the Samples
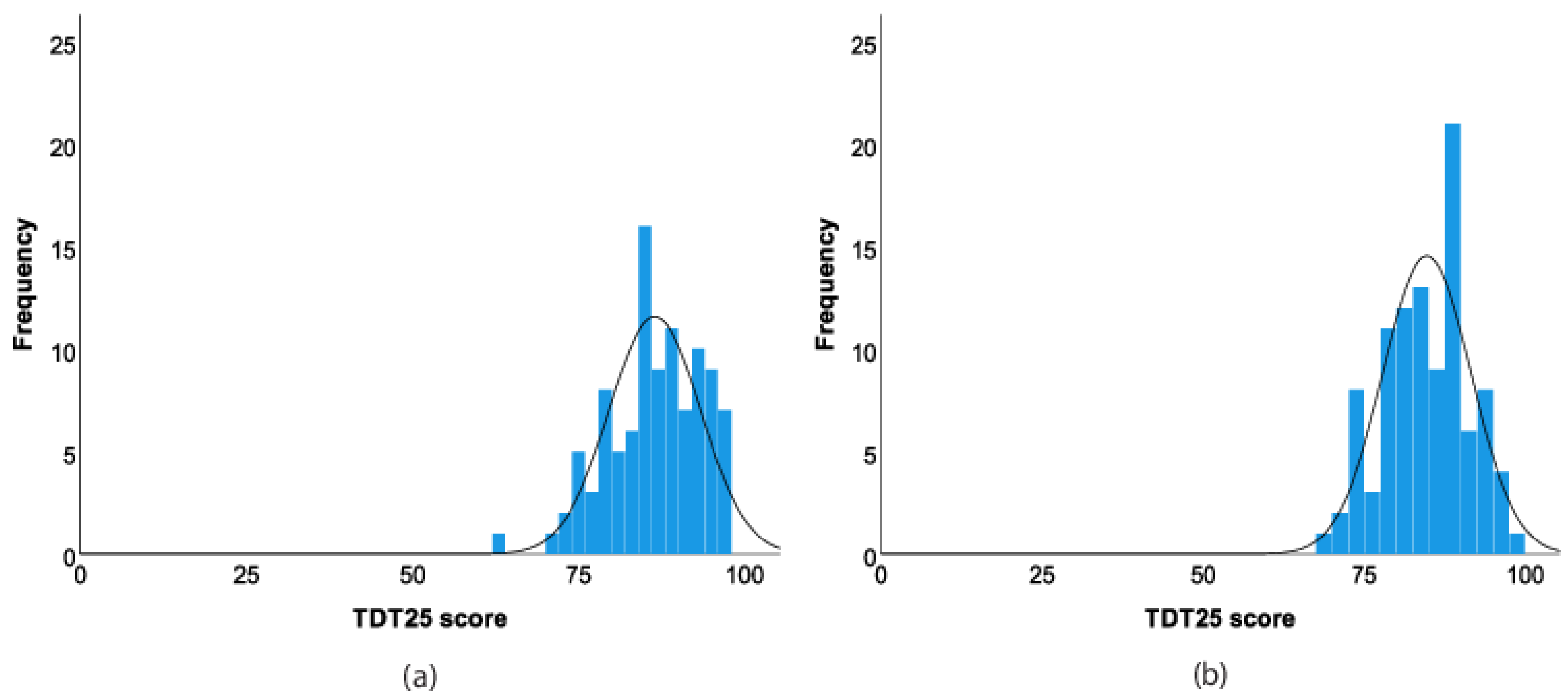
3.2. Frequency Distribution of Tactile Discrimination in Pooled Sample of Healthy Older Adults (n = 100)
3.3. Updated Normative Standards and Criteria of Abnormality
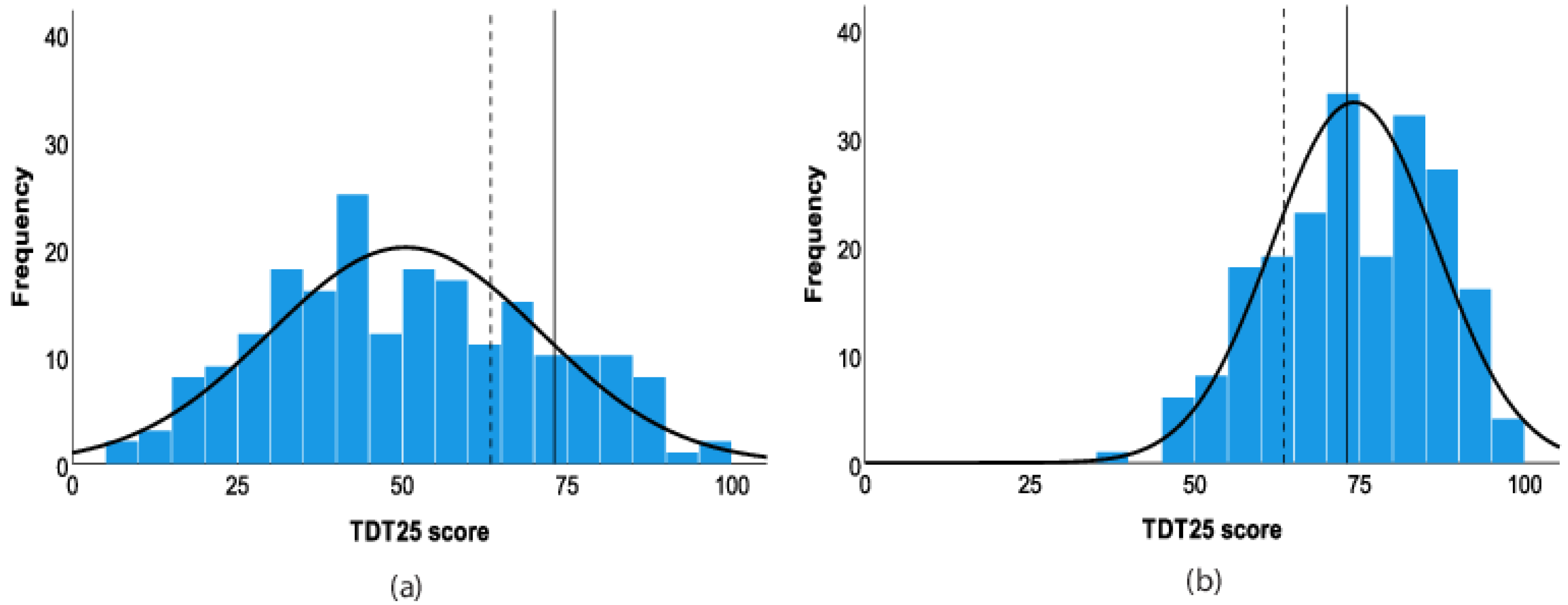
3.4. Frequency Distributions of Tactile Discrimination in Pooled Sample of Stroke Survivors (n = 207)
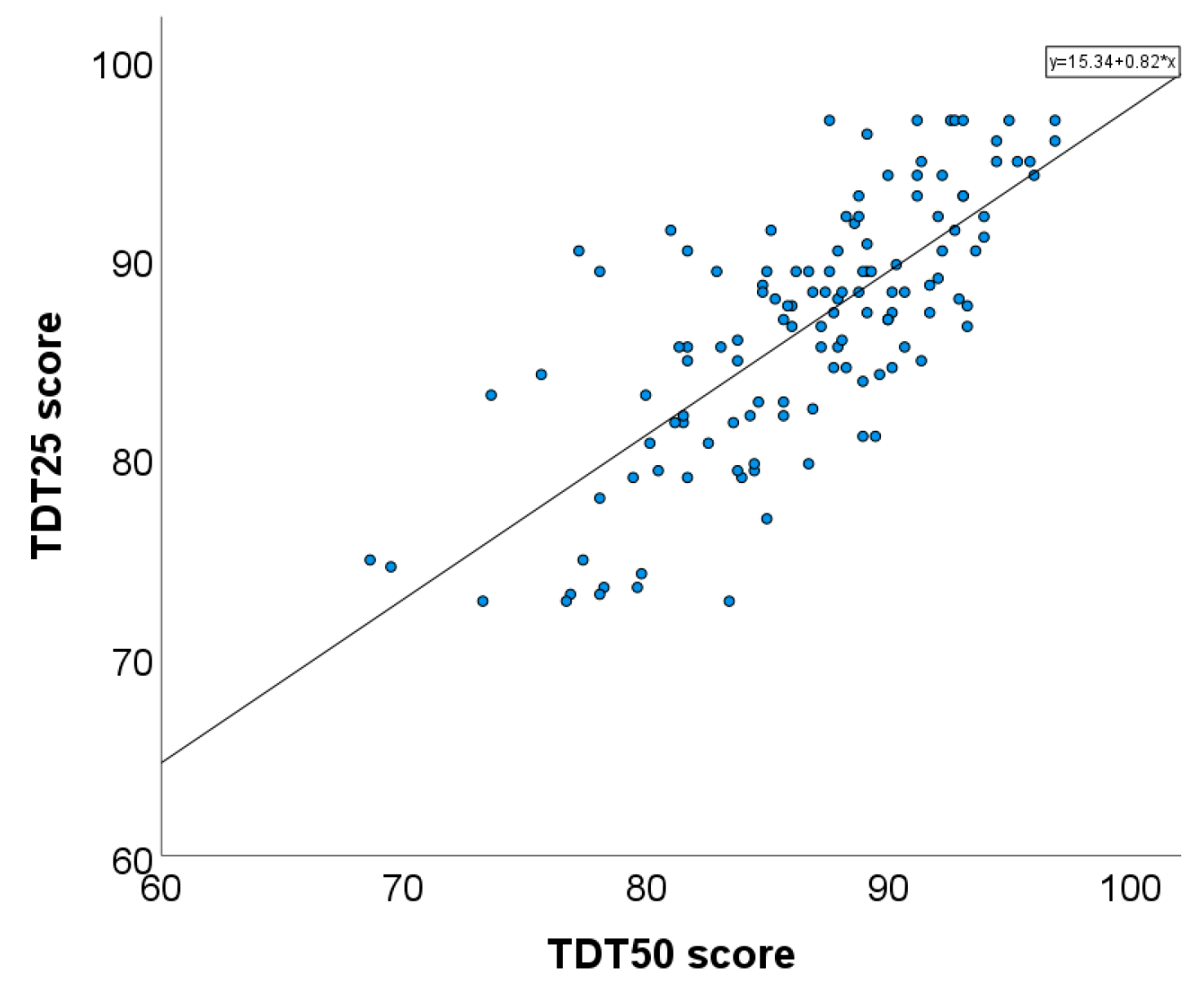
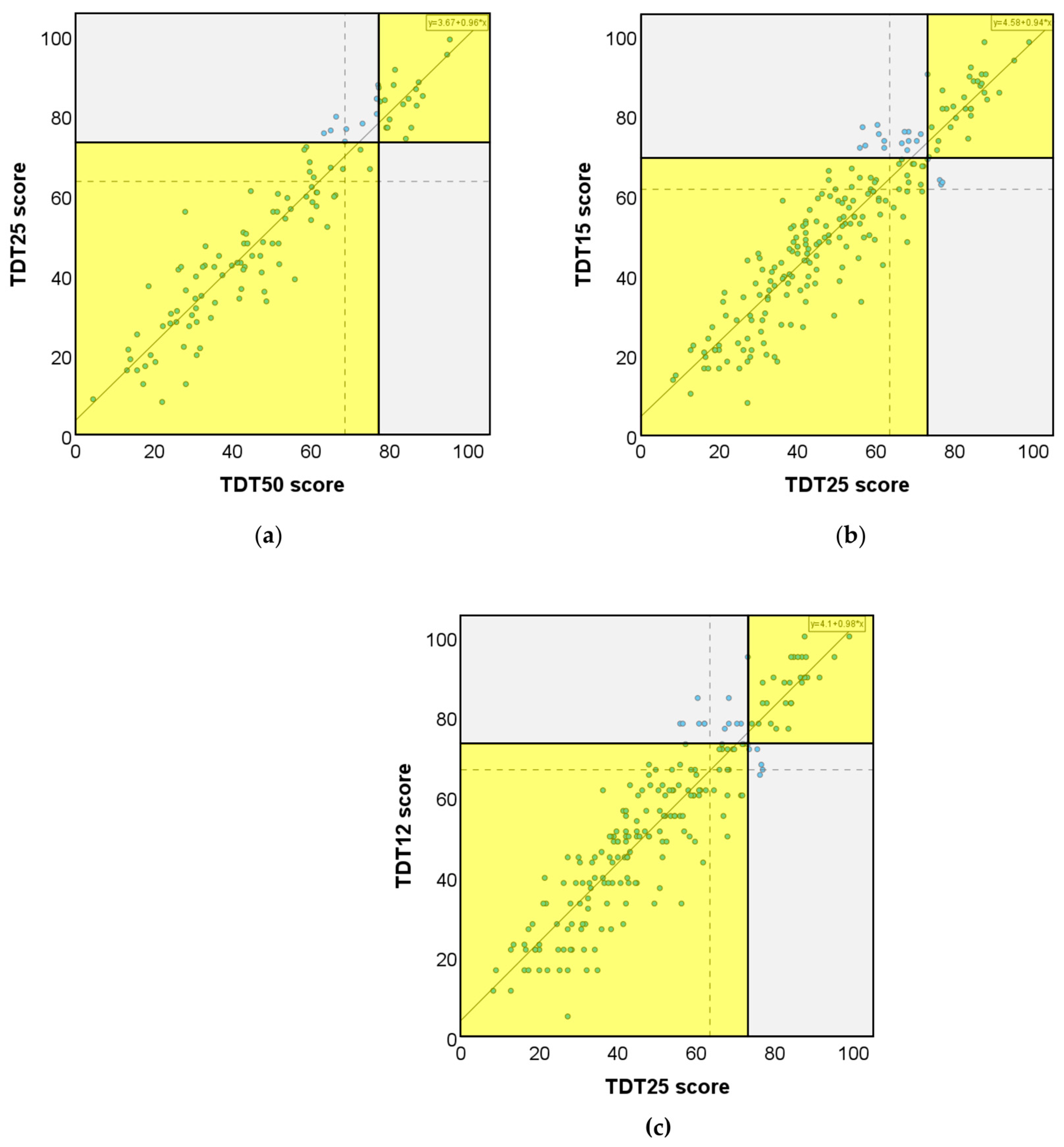
3.5. Association between Test Scores for Brief Test Versions Relative to Original TDT50 and TDT25 Test Versions
3.6. Sensitivity and Specificity for Briefer Versions of the TDT (25, 15, and 12 Trials)
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2016 Lifetime Risk of Stroke Collaborators. Global, regional, and country-specific lifetime risks of stroke, 1990 and 2016. N. Engl. J. Med. 2018, 379, 2429–2437. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.M.; Matyas, T.A. Frequency of discriminative sensory loss in the hand after stroke in a rehabilitation setting. J. Rehabil. Med. 2011, 43, 257–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cirstea, M.C.; Levin, M.F. Compensatory strategies for reaching in stroke. Brain 2000, 123, 940–953. [Google Scholar] [CrossRef] [Green Version]
- Carlsson, H.; Gard, G.; Brogårdh, C. Upper-limb sensory impairments after stroke: Self-reported experiences of daily life and rehabilitation. JRM 2018, 50, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Blennerhassett, J.M.; Matyas, T.A.; Carey, L.M. Impaired discrimination of surface friction contributes to pinch grip deficit after stroke. Neurorehabil. Neural Repair 2007, 21, 263–272. [Google Scholar] [CrossRef] [PubMed]
- Nowak, D.A.; Hermsdörfer, J. Grip force behavior during object manipulation in neurological disorders: Toward an objective evaluation of manual performance deficits. Mov. Disord. 2005, 20, 11–25. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.M. Review on somatosensory loss after stroke. Crit. Rev. Phys. Rehabil. Med. 2017, 29, 1–41. [Google Scholar] [CrossRef]
- Borstad, A.L.; Nichols-Larsen, D.S. Assessing and treating higher level somatosensory impairments post stroke. Top. Stroke Rehabil. 2014, 21, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.M.; Mak-Yuen, Y.Y.K.; Matyas, T.A. The functional tactile object recognition test: A unidimensional measure with excellent internal consistency for haptic sensing of real objects after stroke. Front. Neurosci. 2020, 14, 542590. [Google Scholar] [CrossRef]
- Connell, L.A.; Lincoln, N.B.; Radford, K.A. Somatosensory impairment after stroke: Frequency of different deficits and their recovery. Clin. Rehabil. 2008, 22, 758–767. [Google Scholar] [CrossRef]
- Pumpa, L.U.; Cahill, L.S.; Carey, L.M. Somatosensory assessment and treatment after stroke: An evidence-practice gap. Aust. Occup. Ther. J. 2015, 62, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Winward, C.E.; Halligan, P.W.; Wade, D.T. Current practice and clinical relevance of somatosensory assessment after stroke. Clin. Rehabil. 1999, 13, 48–55. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Oke, L.E. Evaluation of impaired fingertip texture discrimination and wrist position sense in patients affected by stroke: Comparison of clinical and new quantitative measures. J. Hand Ther. 2002, 15, 71–82. [Google Scholar] [CrossRef]
- Kim, J.S.; Choi-Kwon, S. Discriminative sensory dysfunction after unilateral stroke. Stroke 1996, 27, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Patel, A.T.; Duncan, P.W.; Lai, S.-M.; Studenski, S. The relation between impairments and functional outcomes poststroke. Arch. Phys. Med. Rehabil. 2000, 81, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Tyson, S.F.; Hanley, M.; Chillala, J.; Selley, A.B.; Tallis, R.C. Sensory loss in hospital-admitted people with stroke: Characteristics, associated factors, and relationship with function. Neurorehabil. Neural Repair 2008, 22, 166–172. [Google Scholar] [CrossRef]
- Carey, L.M.; Lamp, G.; Turville, M. The state-of-the-science on somatosensory function and its impact on daily life in adults and older adults, and following stroke. OTJR 2016, 36 (Suppl. S2), 27S–41S. [Google Scholar] [CrossRef]
- Carey, L.M.; Matyas, T.A.; Oke, L.E. Sensory loss in stroke patients: Effective training of tactile and proprioceptive discrimination. Arch. Phys. Med. Rehabil. 1993, 74, 602–611. [Google Scholar] [CrossRef]
- Winward, C.E.; Halligan, P.W.; Wade, D.T. The Rivermead Assessment of Somatosensory Performance (RASP): Standardization and reliability data. Clin. Rehabil. 2002, 16, 523–533. [Google Scholar] [CrossRef]
- Weinstein, S. Fifty years of somatosensory research: From the Semmes-Weinstein monofilaments to the Weinstein Enhanced Sensory Test. J. Hand Ther. 1993, 6, 11–22. [Google Scholar] [CrossRef]
- Miller, K.; Phillips, B.; Martin, C.; Wheat, H.; Goodwin, A.; Galea, M. The AsTex ®: Clinimetric properties of a new tool for evaluating hand sensation following stroke. Clin. Rehabil. 2009, 23, 1104–1115. [Google Scholar] [CrossRef] [PubMed]
- Van Boven, R.W.; Johnson, K.O. The limit of tactile spatial resolution in humans: Grating orientation discrimination at the lip, tongue, and finger. Neurology 1994, 44, 2361–2366. [Google Scholar] [CrossRef] [PubMed]
- Carey, L.M.; Oke, L.E.; Matyas, T.A. Impaired touch discrimination after stroke: A quantitative test. J. Neurol. Rehabil. 1997, 11, 219–232. [Google Scholar] [CrossRef] [Green Version]
- Darian-Smith, I.; Kenins, P. Innervation density of mechanoreceptive fibres supplying glabrous skin of the monkey’s index finger. J. Physiol. 1980, 309, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Lamp, G.; Goodin, P.; Palmer, S.; Low, E.; Barutchu, A.; Carey, L.M. Activation of bilateral secondary somatosensory cortex with right hand touch stimulation: A meta-analysis of functional neuroimaging studies. Front. Neurol. 2018, 9, 1129. [Google Scholar] [CrossRef]
- Carey, L.; Macdonell, R.; Matyas, T.A. SENSe: Study of the Effectiveness of Neurorehabilitation on Sensation. Neurorehabil. Neural Repair 2011, 25, 304–313. [Google Scholar] [CrossRef]
- Goodin, P.; Lamp, G.; Vidyasagar, R.; McArdle, D.; Seitz, R.J.; Carey, L.M. Altered functional connectivity differs in stroke survivors with impaired touch sensation following left and right hemisphere lesions. NeuroImage Clin. 2018, 18, 342–355. [Google Scholar] [CrossRef]
- Turville, M.; Carey, L.M.; Matyas, T.A.; Blennerhassett, J. Change in functional arm use is associated with somatosensory skills after sensory retraining poststroke. Am. J. Occup. Ther. 2017, 71, 7103190070p1–7103190070p9. [Google Scholar] [CrossRef]
- Carey, L.M.; Abbott, D.F.; Lamp, G.; Puce, A.; Seitz, R.J.; Donnan, G.A. Same intervention–different reorganization. Neurorehabil. Neural Repair 2016, 30, 988–1000. [Google Scholar] [CrossRef] [Green Version]
- Bannister, L.C.; Crewther, S.G.; Gavrilescu, M.; Carey, L.M. Improvement in touch sensation after stroke is associated with resting functional connectivity changes. Front. Neurol. 2015, 6, 165. [Google Scholar] [CrossRef] [Green Version]
- Dunn, W.; Griffith, J.W.; Morrison, M.T.; Tanquary, J.; Sabata, D.; Victorson, D.; Carey, L.M.; Gershon, R.C. Somatosensation assessment using the NIH Toolbox. Neurology 2013, 80 (Suppl. S3), S41–S44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carey, L.M. Network of Sites and ‘Up-Skilled’ Therapists to Deliver Best-Practice Stroke Rehabilitation of the Upper Limb. Australian New Zealand Clinical Trials Registry; ACTRN12618001389291; Clinical Trials Centre: Camperdown, Australia, 2018; Available online: https://www.anzctr.org.au/Trial/Registration/TrialReview.aspx?id=375706&isReview=true (accessed on 25 February 2023).
- Matyas, T.A.; Mak-Yuen, Y.Y.K.; Boelsen-Robinson, T.; Carey, L.M. Calibration of impairment severity to enable comparison across somatosensory domains. Brain Sci. 2023; submitted. [Google Scholar]
- Carey, L.M. Effective Sensory Rehabilitation after Stroke: Targeting Viable Brain Networks: Australian and New Zealand Clinical Trials Registry; ACTRN12613001136796; Clinical Trials Centre: Camperdown, Australia, 2013. [Google Scholar]
- Tactile Discrimination Test. Online Image. Available online: https://sensetherapy.net.au/sense-assess/tactile-discrimination-test/ (accessed on 26 February 2023).
- Carey, L.M. SENSe Helping Stroke Survivors Regain a Sense of Touch: An Evidence-Based Approach to Sensory Rehabilitation after Stroke: A Manual for Therapists; Florey Neuroscience Institute: Heidelberg, VIC, Australia, 2012. [Google Scholar]
- Portney, L.G. Foundations of Clinical Research: Applications to Practice, 3rd ed.; Pearson: Harlow, UK, 2014. [Google Scholar]
- Spearman, C. Correlation calculated from faulty data. Br. J. Psychol. 1910, 3, 271–295. [Google Scholar] [CrossRef]
- Brown, W. Some experimental results in the correlation of mental abilities. Br. J. Psychol. 1910, 3, 296–322. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Reorganization of cerebral networks after stroke: New insights from neuroimaging with connectivity approaches. Brain 2011, 134 Pt 5, 1264–1276. [Google Scholar] [CrossRef] [Green Version]
- Nowak, D.A.; Grefkes, C.; Ameli, M.; Fink, G.R. Interhemispheric competition after stroke: Brain stimulation to enhance recovery of function of the affected hand. Neurorehabil. Neural Repair 2009, 23, 641–656. [Google Scholar] [CrossRef] [PubMed]
- Kessner, S.S.; Bingel, U.; Thomalla, G. Somatosensory deficits after stroke: A scoping review. Top. Stroke Rehabil. 2016, 23, 136–146. [Google Scholar] [CrossRef]
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographic Information | Pooled Sample (n = 207) | Discriminative Validity a (n = 50) | SENSe Trial b (n = 46) | IN_TOUCH Trial c (n = 22) | CoNNECT Trial d (n = 45) | NIH Trial e (n = 9) | SENSe CONNECT f (n = 35) |
|---|---|---|---|---|---|---|---|
| Age, years = | |||||||
| M (SD) | 56.4 (14.5) | 52 (14.4) | 61.4 (11.9) | 59.7 (15.1) | 52.8 (14.1) | 65.2 (12.6) | 56.1 (15.6) |
| Min, Max | 18, 87 | 18, 79 | 32, 87 | 18, 79 | 26, 82 | 41, 78 | 19–81 |
| Gender, n% | |||||||
| Male | 144 (70) | 36 (72) | 33 (72) | 14 (64) | 32 (71) | 6 (67) | 23 (66) |
| Female | 63 (30) | 14 (28) | 13 (28) | 8 (36) | 13 (29) | 3 (33) | 12 (34) |
| Hemisphere affected, n% | |||||||
| Right | 95 (46) | 21 (42) | 20 (43) | 8 (36) | 20 (45) | 5 (56) | 21 (60) |
| Left | 109 (53) | 29 (58) | 26 (57) | 14 (64) | 23 (51) | 4 (44) | 13 (37) |
| Both | 3 (1) | 0 (0) | 0 (0) | 0 (0) | 2 (4) | 0 (0) | 1 (3) |
| Affected side, n% | |||||||
| Dominant | 105 (51) | 47 (94) | 26 (57) | 13 (59) | 23 (51) | 5 (56) | 13 (37) |
| Non dominant | 102 (49 | 3 (6) | 9 (41) | 9 (41) | 22 (49) | 4 (44) | 22 (63) |
| Lesion Level, n% | (n = 198) * | ||||||
| Cortical | 88 (44) | 15 (30) | 18 (39) | 13 (59) | 26 (58) | - | 16 (29) |
| Subcortical | 55 (28) | 9 (18) | 13 (28) | 8 (36) | 15 (33) | - | 10 (46) |
| Both | 25 (13) | 9 (18) | 10 (22) | 1 (5) | 4 (9) | - | 1 (3) |
| Unknown | 30 (15) | 17 (34) | 5 (11) | 0 (0) | 0 (0) | - | 8 (23) |
| Stroke type, n% | |||||||
| Ischemic | 143 (72) | 42 (84) | 31 (84) | 22 (100) | 31 (69) | - | 17 (48) |
| Hemorrhage | 52 (26) | 8 (16) | 15 (33) | 0 (0) | 14 (31) | - | 15 (43) |
| Unknown | 3 (2) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 3 (9) |
| Demographic Information | Pooled Sample (n = 100) | Normative Validity b (n = 50) | IN_TOUCH Trial c (n = 13) | CoNNECT Trial d (n = 26) | NIH Trial e (n = 11) |
|---|---|---|---|---|---|
| Age, years | |||||
| M (SD) | 52.7 (16.2) | 52.1 (12.9) | 58.6 (15.3) | 49.5 (17.9) | 56.1 (22.1) |
| Min, Max | 23, 89 | 23, 77 | 23, 79 | 26, 89 | 29, 81 |
| Gender, n% | |||||
| Male | 59 (59) | 34 (68) | 7 (54) | 13 (50) | 5 (45) |
| Female | 41 (41) | 16 (32) | 6 (46) | 13 (50) | 6 (55) |
| Hand Dominance a | |||||
| Right | 94 (96) | 46 (92) | 13 (100) | 26 (100) | 11 (100) |
| Left | 4 (4) | 4 (8) | 0 (0) | 0 (0) | 0 (0) |
| TDT: No. of Trials | Mean PMA | SD | Criterion of Abnormality | |
|---|---|---|---|---|
| 5th | 0th | |||
| 50 trials a | 86.69 | 5.70 | 76.98 | 68.62 |
| 25 trials | 85.58 | 6.91 | 73.10 | 63.45 |
| 15 trials | 85.02 | 8.58 | 69.45 | 61.49 |
| 12 trials b | 89.20 | 8.45 | 73.08 | 66.67 |
| No. of Trials | Mean | SD | Minimum | Maximum | Percentiles | ||
|---|---|---|---|---|---|---|---|
| PMA | 25th | 50th Median | 75th | ||||
| Contralesional | |||||||
| 50 trials | 50.21 | 22.21 | 4.48 | 95.34 | 30.86 | 48.62 | 66.38 |
| 25 trials | 50.50 | 20.57 | 8.28 | 98.97 | 34.83 | 49.31 | 66.90 |
| 15 trials | 52.00 | 20.94 | 8.05 | 98.28 | 37.36 | 52.30 | 67.24 |
| 12 trials a | 53.74 | 22.06 | 5.13 | 100 | 38.46 | 53.85 | 71.80 |
| Ipsilesional | |||||||
| 50 trials | 75.71 | 12.12 | 29.14 | 95.52 | 67.97 | 76.98 | 84.78 |
| 25 trials | 74.14 | 12.43 | 35.86 | 97.93 | 64.48 | 74.14 | 84.14 |
| 15 trials | 73.81 | 14.00 | 28.74 | 98.28 | 63.80 | 75.29 | 83.91 |
| 12 trials a | 77.12 | 14.83 | 28.20 | 100 | 66.67 | 78.21 | 89.74 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mak-Yuen, Y.Y.K.; Matyas, T.A.; Carey, L.M. Characterizing Touch Discrimination Impairment from Pooled Stroke Samples Using the Tactile Discrimination Test: Updated Criteria for Interpretation and Brief Test Version for Use in Clinical Practice Settings. Brain Sci. 2023, 13, 533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci13040533
Mak-Yuen YYK, Matyas TA, Carey LM. Characterizing Touch Discrimination Impairment from Pooled Stroke Samples Using the Tactile Discrimination Test: Updated Criteria for Interpretation and Brief Test Version for Use in Clinical Practice Settings. Brain Sciences. 2023; 13(4):533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci13040533
Chicago/Turabian StyleMak-Yuen, Yvonne Y. K., Thomas A. Matyas, and Leeanne M. Carey. 2023. "Characterizing Touch Discrimination Impairment from Pooled Stroke Samples Using the Tactile Discrimination Test: Updated Criteria for Interpretation and Brief Test Version for Use in Clinical Practice Settings" Brain Sciences 13, no. 4: 533. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci13040533