Improved Central Nervous System Symptoms in People with HIV without Objective Neuropsychiatric Complaints Switching from Efavirenz to Rilpivirine Containing cART


 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Participants and Data Collection
2.2. Study Assessments
2.3. Neuropsychiatric Symptoms and Patient Reported Outcome Measures
2.4. Cognitive Testing
2.5. Statistical Analysis
3. Results
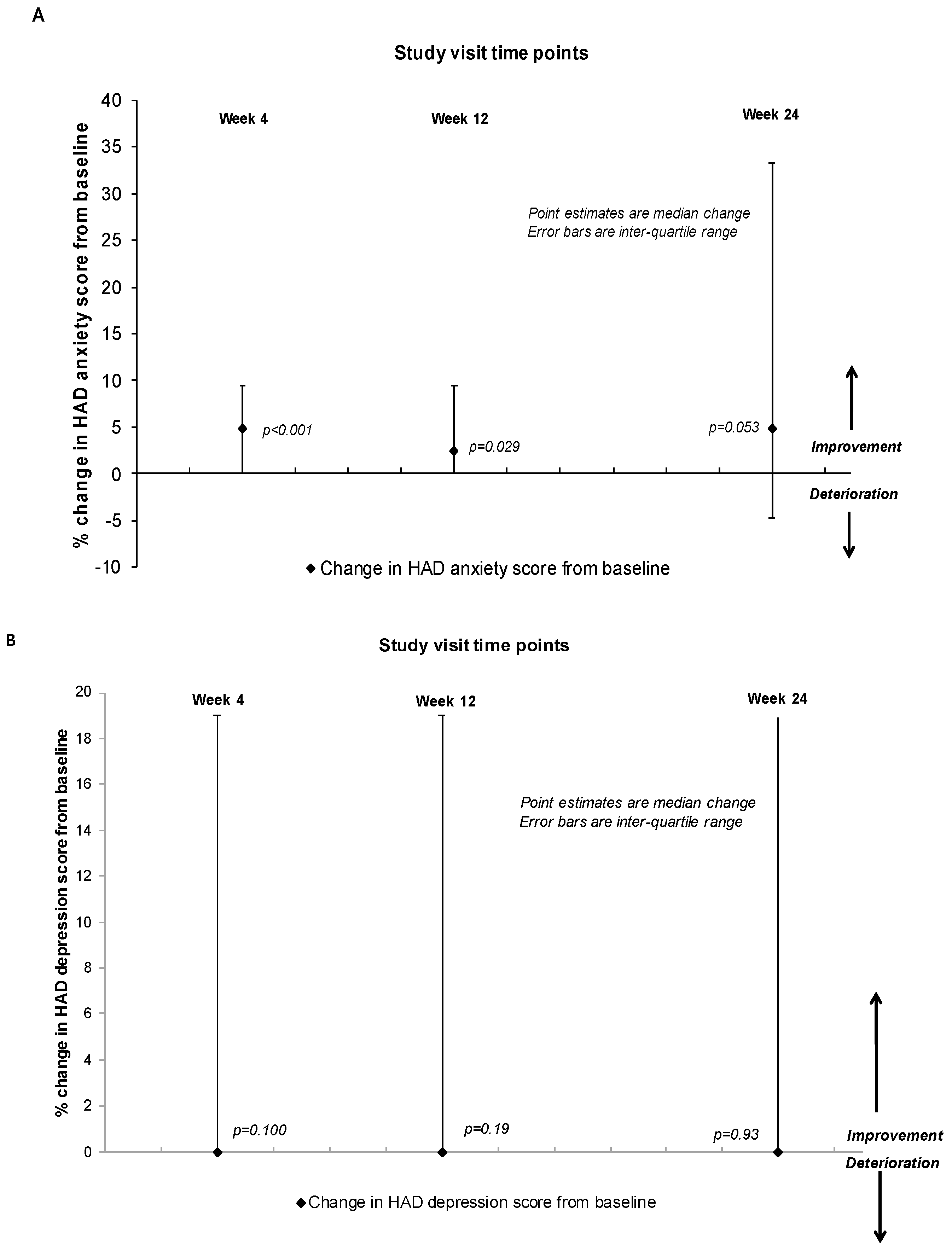
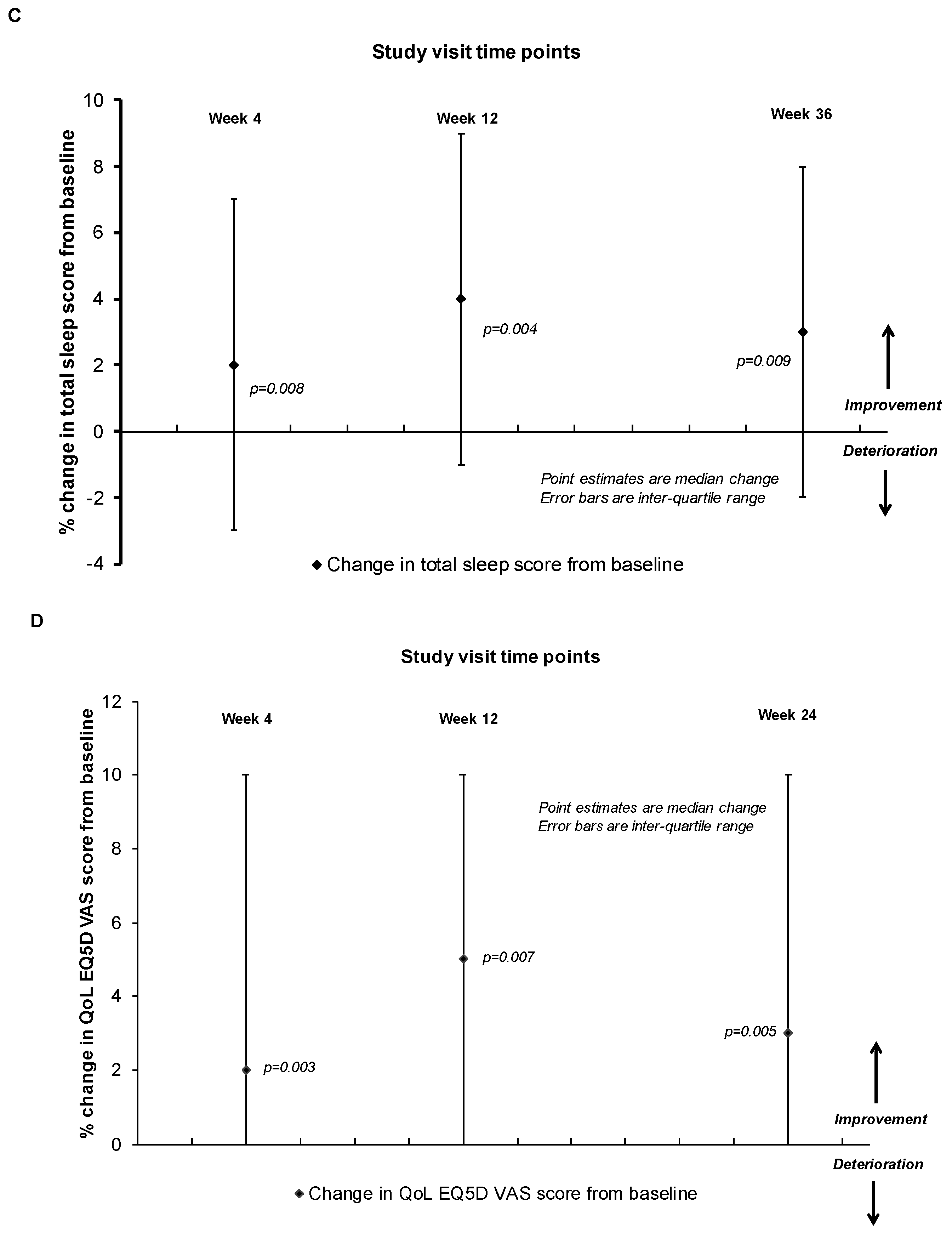
3.1. Change in Central Nervous Symptoms and Patient Reported Outcomes for Sleep, Anxiety and Depression
3.2. Change in Health-Related Quality of Life
3.3. Change in Cognitive Function
3.4. Virological and Immunological Efficacy
3.5. Lipids
3.6. Non-Central Nervous System Adverse Events and Laboratory Abnormalities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Elzi, L.; Marzolini, C.; Furrer, H.; Ledergerber, B.; Cavassini, M.; Hirschel, B.; Vernazza, P.; Bernasconi, E.; Weber, R.; Battegay, M.; et al. Treatment modification in human immunodeficiency virus-infected individuals starting combination antiretroviral therapy between 2005 and 2008. Arch. Intern. Med. 2010, 170, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Davidson, I.; Beardsell, H.; Smith, B.; Mandalia, S.; Bower, M.; Gazzard, B.; Nelson, M.; Stebbing, J. The frequency and reasons for antiretroviral switching with specific antiretroviral associations: The SWITCH study. Antivir. Res. 2010, 86, 227–229. [Google Scholar] [CrossRef] [PubMed]
- WHO. Consolidated Guidelines on HIV Prevention, Diagnosis, Treatment and Care for Key Populations—2016. 2016. Available online: http:// www.ncbi.mlm.nih.gov/books/NBK379694. (accessed on 26 February 2019).
- Arribas, J.R.; Pozniak, A.L.; Gallant, J.E.; Dejesus, E.; Gazzard, B.; Campo, R.E.; Chen, S.S.; McColl, D.; Holmes, C.B.; Enejose, J.; et al. Tenofovir disoproxil fumarate, emtricitabine, and efavirenz compared with zidovudine/lamivudine and efavirenz in treatment-naive patients: 144-week analysis. J. Acquir. Immune Defic. Syndr. 2008, 47, 74–78. [Google Scholar] [CrossRef] [PubMed]
- Group, E.S. Efficacy of 400 mg efavirenz versus standard 600 mg dose in HIV-infected, antiretroviral-naive adults (ENCORE1): A randomised, double-blind, placebo-controlled, non-inferiority trial. Lancet 2014, 383, 1474–1482. [Google Scholar]
- Ldt BMSP. Sustiva Summary of Product Characteristics 2016. Available online: http://www.medicines.org.uk/EMC/ (accessed on 26 February 2019).
- Clifford, D.B.; Evans, S.; Yang, Y.J.; Acosta, E.P.; Ribaudo, H.; Gulick, R.M.; the Study Team. Long-term impact of efavirenz on neuropsychological performance and symptoms in HIV-infected individuals (ACTG 5097s). HIV Clin. Trials 2009, 10, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Waters, L.; Fisher, M.; Winston, A.; Higgs, C.; Hadley, W.; Garvey, L.; Mandalia, S.; Perry, N.; Nicola, M.; Nelson, M. A phase IV, double-blind, multicentre, randomized, placebo-controlled, pilot study to assess the feasibility of switching individuals receiving efavirenz with continuing central nervous system adverse events to etravirine. AIDS 2011, 25, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Fumaz, C.R.; Munoz-Moreno, J.A.; Molto, J.; Negredo, E.; Ferrer, M.J.; Sirera, G.; Pérez-Alvarez, N.; Gómez, G.; Burger, D.; Clotet, B. Long-term neuropsychiatric disorders on efavirenz-based approaches: Quality of life, psychologic issues, and adherence. J. Acquir. Immune Defic. Syndr. 2005, 38, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Rihs, T.A.; Begley, K.; Smith, D.E.; Sarangapany, J.; Callaghan, A.; Kelly, M.; Post, J.J.; Gold, J. Efavirenz and chronic neuropsychiatric symptoms: A cross-sectional case control study. HIV Med. 2006, 7, 544–548. [Google Scholar] [CrossRef]
- Nguyen, A.; Calmy, A.; Delhumeau, C.; Mercier, I.; Cavassini, M.; Mello, A.F.; Elzi, L.; Rauch, A.; Bernasconi, E.; Schmid, P.; et al. A randomized cross-over study to compare raltegravir and efavirenz (SWITCH-ER study). AIDS 2011, 25, 1481–1487. [Google Scholar] [CrossRef]
- Mills, A.M.; Cohen, C.; Dejesus, E.; Brinson, C.; Williams, S.; Yale, K.L.; Ramanathan, S.; Wang, M.H.; White, K.; Chuck, S.K.; et al. Efficacy and safety 48 weeks after switching from efavirenz to rilpivirine using emtricitabine/tenofovir disoproxil fumarate-based single-tablet regimens. HIV Clin. Trials 2013, 14, 216–223. [Google Scholar] [CrossRef]
- Pozniak, A.; Markowitz, M.; Mills, A.; Stellbrink, H.J.; Antela, A.; Domingo, P.; Girard, P.-M.; Henry, K.; Nguyen, T.; Piontkowsky, D.; et al. Switching to coformulated elvitegravir, cobicistat, emtricitabine, and tenofovir versus continuation of non-nucleoside reverse transcriptase inhibitor with emtricitabine and tenofovir in virologically suppressed adults with HIV (STRATEGY-NNRTI): 48 week results of a randomised, open-label, phase 3b non-inferiority trial. Lancet Infect. Dis. 2014, 14, 590–599. [Google Scholar] [PubMed]
- Ciccarelli, N.; Fabbiani, M.; Di Giambenedetto, S.; Fanti, I.; Baldonero, E.; Bracciale, L.; Tamburrini, E.; Cauda, R.; De Luca, A.; Silveri, M.C. Efavirenz associated with cognitive disorders in otherwise asymptomatic HIV-infected patients. Neurology 2011, 76, 1403–1409. [Google Scholar] [CrossRef] [PubMed]
- Ma, Q.; Vaida, F.; Wong, J.; Sanders, C.A.; Kao, Y.T.; Croteau, D.; Clifford, D.B.; Collier, A.C.; Gelman, B.B.; Marra, C.M.; et al. Long-term efavirenz use is associated with worse neurocognitive functioning in HIV-infected patients. J. Neurovirol. 2016, 22, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Hakkers, C.S.; Arends, J.E.; van den Berk, G.E.; Ensing, M.H.M.; Hooijenga, I.; Vink, M.; van Zandvoort, M.J.E.; Hoepelman, A.I.M. Objective and Subjective Improvement of Cognition After Discontinuing Efavirenz in Asymptomatic Patients: A Randomized Controlled Trial. J. Acquir. Immune Defic. Syndr. 2019, 80, e14–e22. [Google Scholar] [CrossRef] [PubMed]
- Lapadula, G.B.D.; Bai, F.; Di Biagio, A.; Foca, E.; Bonora, S.; Castelli, F.; Viscoli, C.; Bandera, A.; Monforte, A.; Gori, A. No change in neurocognitive function after switching from efavirenz to rilpivirine. In Proceedings of the CROI Conference, Boston, MA, USA, 4–7 March 2018; p. 418. [Google Scholar]
- Payne, B.; Chadwick, T.J.; Blamire, A.; Anderson, K.N.; Parikh, J.; Qian, J.; Hynes, A.M.; Wilkinson, J.; Price, D.A.; Efficacy of Switch to Lopinavir/Ritonavir in Improving Cognitive Function in Efavirenz-treated Patients Study Team. Does efavirenz replacement improve neurological function in treated HIV infection? HIV Med. 2017, 18, 690–695. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Molina, J.M.; Cahn, P.; Grinsztejn, B.; Lazzarin, A.; Mills, A.; Saag, M.; Supparatpinyo, K.; Walmsley, S.; Crauwels, H.; Rimsky, L.T.; et al. Rilpivirine versus efavirenz with tenofovir and emtricitabine in treatment-naive adults infected with HIV-1 (ECHO): A phase 3 randomised double-blind active-controlled trial. Lancet 2011, 378, 238–246. [Google Scholar] [CrossRef]
- Molina, J.M.; Clumeck, N.; Orkin, C.; Rimsky, L.T.; Vanveggel, S.; Stevens, M.; ECHO and THRIVE Study Groups. Week 96 analysis of rilpivirine or efavirenz in HIV-1-infected patients with baseline viral load </= 100 000 copies/mL in the pooled ECHO and THRIVE phase 3, randomized, double-blind trials. HIV Med. 2014, 15, 57–62. [Google Scholar]
- U.S. Department of Health and Human Services NIoH, National Institute of Allergy and Infectious Diseases, Division of AIDS. Division of AIDS (DAIDS), 2017 Corrected Version 2.1. Available from: Table for Grading the Severity of Adult and Pediatric Adverse Events. Available online: https://rscniaidnihgov/sites/default/files/daidsgradingcorrectedv21pdf (accessed on 26 February 2019).
- Buysse, D.J.; Reynolds, C.F., 3rd; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef]
- EuroQol, G. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar]
- Cysique, L.A.; Maruff, P.; Darby, D.; Brew, B.J. The assessment of cognitive function in advanced HIV-1 infection and AIDS dementia complex using a new computerised cognitive test battery. Arch. Clin. Neuropsychol. 2006, 21, 185–194. [Google Scholar] [CrossRef] [Green Version]
- Gutierrez, F.; Navarro, A.; Padilla, S.; Anton, R.; Masia, M.; Borras, J.; Martin-Hidalgo, A. Prediction of neuropsychiatric adverse events associated with long-term efavirenz therapy, using plasma drug level monitoring. Clin. Infect. Dis. 2005, 41, 1648–1653. [Google Scholar] [CrossRef]
- ECHO Study Group; Carey, D.; Puls, R.; Amin, J.; Losso, M.; Phanupak, P.; Foulkes, S.; Mohapi, L.; Crabtree-Ramirez, B.; Jessen, H.; et al. Efficacy and safety of efavirenz 400 mg daily versus 600 mg daily: 96-week data from the randomised, double-blind, placebo-controlled, non-inferiority ENCORE1 study. Lancet Infect. Dis. 2015, 15, 793–802. [Google Scholar] [Green Version]
- Robertson, K.; Liner, J.; Meeker, R.B. Antiretroviral neurotoxicity. J. Neurovirol. 2012, 18, 388–399. [Google Scholar] [CrossRef]
- Tovar-y-Romo, L.B.; Bumpus, N.N.; Pomerantz, D.; Avery, L.B.; Sacktor, N.; McArthur, J.C.; Haughey, N.J. Dendritic spine injury induced by the 8-hydroxy metabolite of efavirenz. J. Pharmacol. Exp. Ther. 2012, 343, 696–703. [Google Scholar] [CrossRef]
- Funes, H.A.; Blas-Garcia, A.; Esplugues, J.V.; Apostolova, N. Efavirenz alters mitochondrial respiratory function in cultured neuron and glial cell lines. J. Antimicrob. Chemother. 2015, 70, 2249–2254. [Google Scholar] [CrossRef] [Green Version]
- Freeman, D.; Levenson, J. Rilpivirine and Depression. Psychosomatics 2015, 56, 711–712. [Google Scholar] [CrossRef]
- Taramasso, L.; Tatarelli, P.; Ricci, E.; Madeddu, G.; Menzaghi, B.; Squillace, N.; De Socio, G.V.; Martinelli, C.; Gulminetti, R.; Maggi, P.; et al. Improvement of lipid profile after switching from efavirenz or ritonavir-boosted protease inhibitors to rilpivirine or once-daily integrase inhibitors: Results from a large observational cohort study (SCOLTA). BMC Infect. Dis. 2018, 18, 357. [Google Scholar]
- Haubrich, R.H.; Riddler, S.A.; DiRienzo, A.G.; Komarow, L.; Powderly, W.G.; Klingman, K.; Garren, K.W.; Butcher, D.L.; Rooney, J.F.; Haas, D.W.; et al. Metabolic outcomes in a randomized trial of nucleoside, nonnucleoside and protease inhibitor-sparing regimens for initial HIV treatment. AIDS 2009, 23, 1109–1118. [Google Scholar] [CrossRef] [Green Version]
- Ward, D.J.; Curtin, J.M. Switch from efavirenz to nevirapine associated with resolution of efavirenz-related neuropsychiatric adverse events and improvement in lipid profiles. AIDS Patient Care STDS 2006, 20, 542–548. [Google Scholar] [CrossRef]
- Munoz-Moreno, J.A.; Fumaz, C.R.; Ferrer, M.J.; Gonzalez-Garcia, M.; Molto, J.; Negredo, E.; Clotet, B. Neuropsychiatric symptoms associated with efavirenz: Prevalence, correlates, and management. A neurobehavioral review. AIDS Rev. 2009, 11, 103–109. [Google Scholar]
- Ramachandran, G.; Hemanth Kumar, A.K.; Rajasekaran, S.; Kumar, P.; Ramesh, K.; Anitha, S.; Narendran, G.; Menon, P.; Gomathi, C.; Swaminathan, S. CYP2B6 G516T polymorphism but not rifampin coadministration influences steady-state pharmacokinetics of efavirenz in human immunodeficiency virus-infected patients in South India. Antimicrob. Agents Chemother. 2009, 53, 863–868. [Google Scholar] [CrossRef]
- Haas, D.W.; Ribaudo, H.J.; Kim, R.B.; Tierney, C.; Wilkinson, G.R.; Gulick, R.M.; Clifford, D.B.; Hulgan, T.; Marzolini, C.; Acosta, E.P. Pharmacogenetics of efavirenz and central nervous system side effects: An Adult AIDS Clinical Trials Group study. AIDS 2004, 18, 2391–2400. [Google Scholar]
- Marzolini, C.; Telenti, A.; Decosterd, L.A.; Greub, G.; Biollaz, J.; Buclin, T. Efavirenz plasma levels can predict treatment failure and central nervous system side effects in HIV-1-infected patients. AIDS 2001, 15, 71–75. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| CNS Side Effects | Baseline n = 41 | 4 Weeks n = 40 | 12 Weeks n = 39 | 24 Weeks n = 37 | |||
|---|---|---|---|---|---|---|---|
| Median change * p value | Median change * p value | Median change * p value | |||||
| Total CNS score, median (IQR) | 10 (2–23) | 7 (3–13) | 0.028 | 10 (3–17) | 0.064 | 7 (3–17) | 0.152 |
| Dizziness, n (%) | 10 (24) | 2 (5) | 0.005 | 5 (12) | 0.096 | 5 (13) | 0.103 |
| Depression/Low mood, n (%) | 14 (34) | 14 (35) | 0.65 | 16 (41) | 0.25 | 17 (46) | 0.04 |
| Insomnia/sleepiness, n (%) | 23 (56) | 15 (37) | 0.05 | 15 (38) | 0.134 | 19 (51) | 0.73 |
| Anxiety/nervousness, n (%) | 14 (34) | 12 (30) | 0.31 | 16 (41) | 0.56 | 15 (40) | 0.78 |
| Confusion, n (%) | 3 (7) | 7 (17) | 0.20 | 3 (7) | 0.99 | 5 (13) | 0.48 |
| Impaired concentration, n (%) | 14 (34) | 15 (37) | 0.52 | 11 (28) | 0.52 | 11 (29) | 0.48 |
| Somnolence, n (%) | 9 (22) | 16 (40) | 0.02 | 16 (41) | 0.02 | 10 (27) | 0.706 |
| Aggressive mood behaviour, n (%) | 9 (22) | 7 (17) | 0.65 | 5 (12) | 0.08 | 7 (18) | 0.56 |
| Abnormal dreams, n (%) | 22 (53) | 12 (30) | 0.003 | 10 (25) | 0.002 | 8 (21) | 0.001 |
| Headache, n (%) | 12 (29) | 7 (17) | 0.04 | 7 (18) | 0.15 | 7 (18) | 0.20 |
| Demographic/Clinical Parameter | Total |
|---|---|
| Number of subjects | 41 |
| Age, years, median, interquartile range (IQR) | 47.3 (31 to 68) |
| Male gender, n (%) | 38 (92) |
| Ethnicity, n (%) | |
| White. | 36 (85) |
| Afro-Caribeean | 4 (10) |
| Other | 2 (5) |
| Years on Atripla, median (IQR) | 5 (2–7) |
| Years since HIV diagnosis median (IQR) | 11(8–18) |
| Baseline CD4 cell count (cells/μL), median (IQR) | 563 (465–679) |
| Baseline plasma HIV RNA level < 50 copies/mL, n (%) | 41 (100) |
| Cognitive Tests | Cognitive Domain | Baseline n = 41 | 4 Weeks n = 40 | 24 Weeks n = 37 |
|---|---|---|---|---|
| OCL (one card learning) Higher score = better performance Median (IQR) | Learning | 0.95 (0.8 to 1) | 0.98 (0.8 to 1) | 1.1 (0.9 to 1) |
| 0.02 (−0.08 to 0.09) p = 0.547 | 0.05 (−0.0 to 0.14) p = 0.035 | |||
| ONB (one back memory) Higher score = better performance Median (IQR) | Working memory | 1.32 (1.1 to 1.39) | 1.32 (1.1 to 1.39) | 1.39 (1.32 to 1.39) |
| −0.05 (−0.17 to 0.16) p = 0.55 | 0.07 (0.00 to 0.20) p = 0.164 | |||
| TWOB (two back memory) Higher score = better performance | Working memory | 1.19 (1.11 to 1.33) | 1.27 (1.02 to 1.33) | 1.33 (1.19 to 1.40) |
| Median (IQR) | 0.05 (−0.05 to 0.17) p = 0.55 | 0.07 (0.00 to 0.17) p = 0.164 | ||
| DET (Detection) Lower score = better performance | Speed | 2.51 (2.47 to 2.63) | 2.57 (2.47 to 2.65) | 2.57 (2.47 to 2.61) |
| Median (IQR) | −0.01 (−0.03 to 0.06) p = 0.581 | 0.01 (−0.02 to 0.07) p = 0.723 | ||
| IDN (Identification) Lower score = better performance | Attention | 2.71 (2.67 to 2.76) | 2.71 (2.69 to 2.82) | 2.75 (2.68 to 2.81) |
| Median (IQR) | −0.01 (−0.03 to 0.05) p = 0.24 | 0.02 (−0.02 to 0.08) p = 0.023 | ||
| GML (Groton maize learning tests) Lower score = better performance Median (IQR) | Executive function | 13 (7 to 24) | 10 (6 to 20) | 10 (6 to 17) |
| −7 (−19 to 5) p = 0.147 | −8 (−25 to 7) p = 0.011 | |||
| SETSID (Intradimensional shift) Lower score = better performance Median (IQR) | Executive function | 1.05 (1.00 to 1.29) | 1.08 (1.00 to 1.29) | 1.19 (1.02 to 1.29) |
| −0.03 (−0.09 to 0.19) p = 0.347 | 0.10 (−0.05 to 0.23) p = 0.004 | |||
| Global cognitive Z score Z score based on normative data Median (IQR) | All domains | −0.12 (−0.78 to 0.47) | −0.06 (−0.78 to 0.72) p = 0.758 | 0.04 (−0.37 to 0.58) p = 0.497 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vera, J.H.; Bracchi, M.; Alagaratnam, J.; Lwanga, J.; Fox, J.; Winston, A.; Boffito, M.; Nelson, M. Improved Central Nervous System Symptoms in People with HIV without Objective Neuropsychiatric Complaints Switching from Efavirenz to Rilpivirine Containing cART. Brain Sci. 2019, 9, 195. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9080195
Vera JH, Bracchi M, Alagaratnam J, Lwanga J, Fox J, Winston A, Boffito M, Nelson M. Improved Central Nervous System Symptoms in People with HIV without Objective Neuropsychiatric Complaints Switching from Efavirenz to Rilpivirine Containing cART. Brain Sciences. 2019; 9(8):195. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9080195
Chicago/Turabian StyleVera, Jaime H., Margherita Bracchi, Jasmini Alagaratnam, Julianne Lwanga, Julie Fox, Alan Winston, Marta Boffito, and Mark Nelson. 2019. "Improved Central Nervous System Symptoms in People with HIV without Objective Neuropsychiatric Complaints Switching from Efavirenz to Rilpivirine Containing cART" Brain Sciences 9, no. 8: 195. https://0-doi-org.brum.beds.ac.uk/10.3390/brainsci9080195