Prognostic Impact of Tumor-Infiltrating Lymphocytes and Neutrophils on Survival of Patients with Upfront Resection of Pancreatic Cancer

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
2.1. Demographical Data, Tumor Size, and Grade of Necrosis
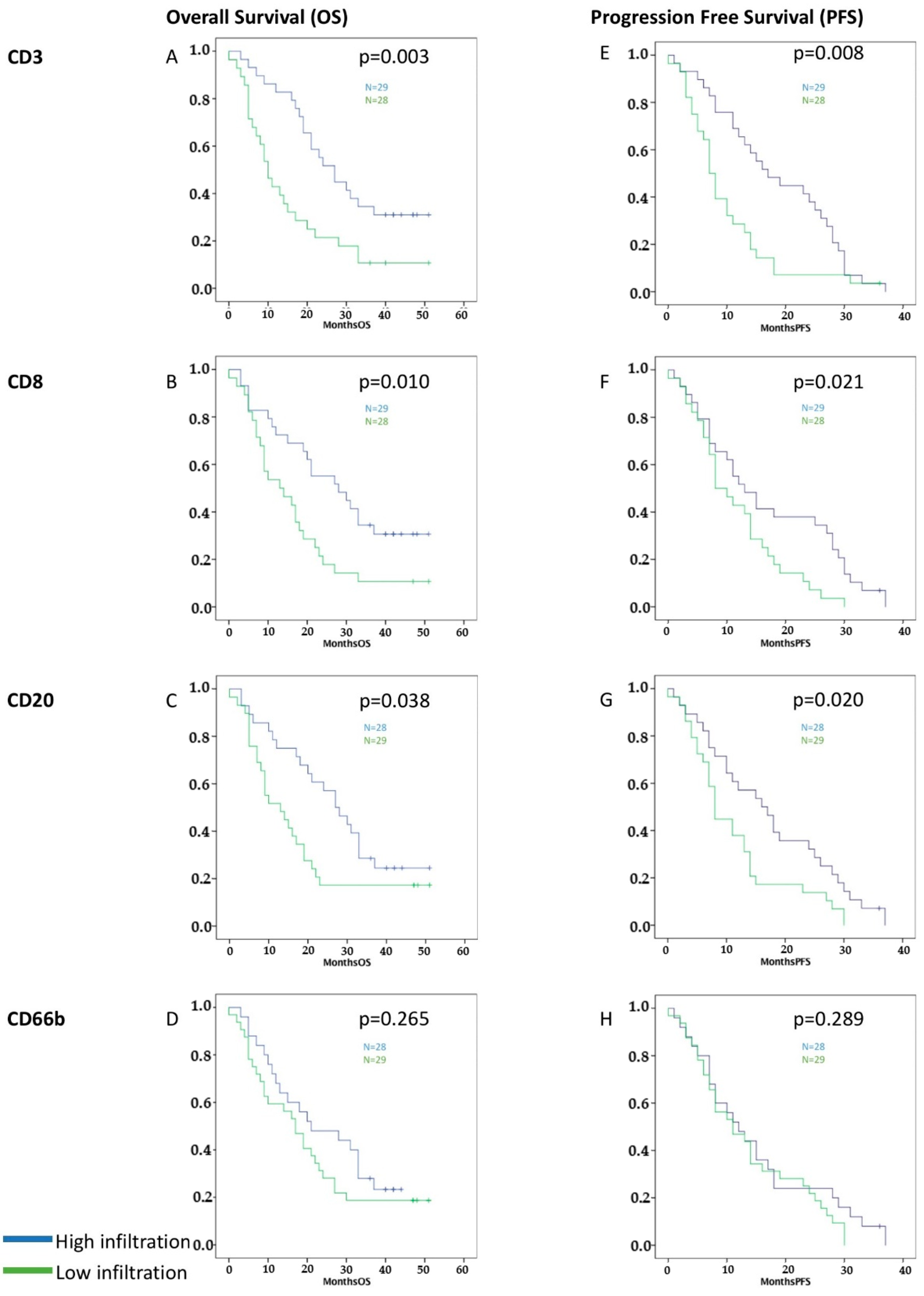
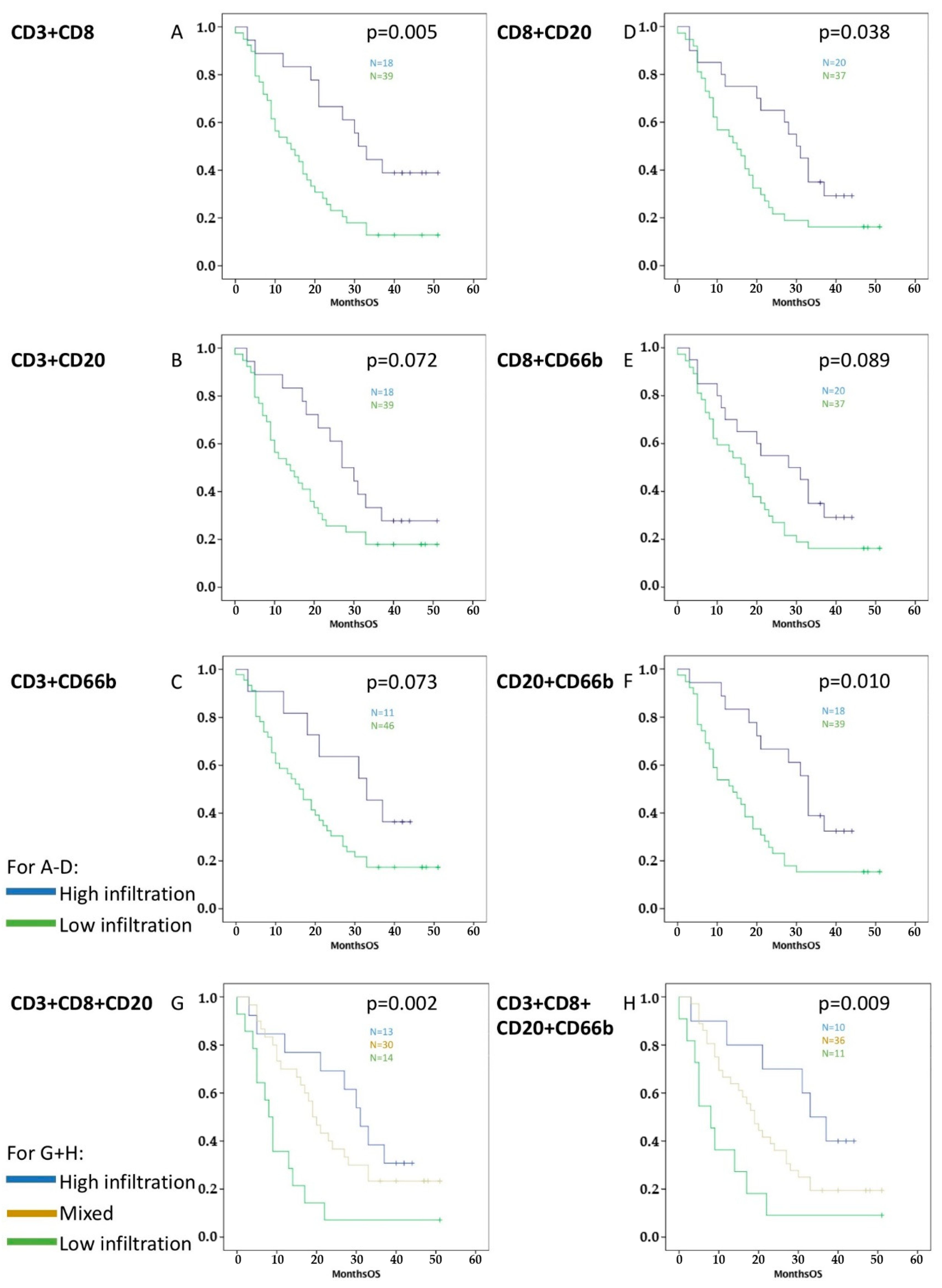
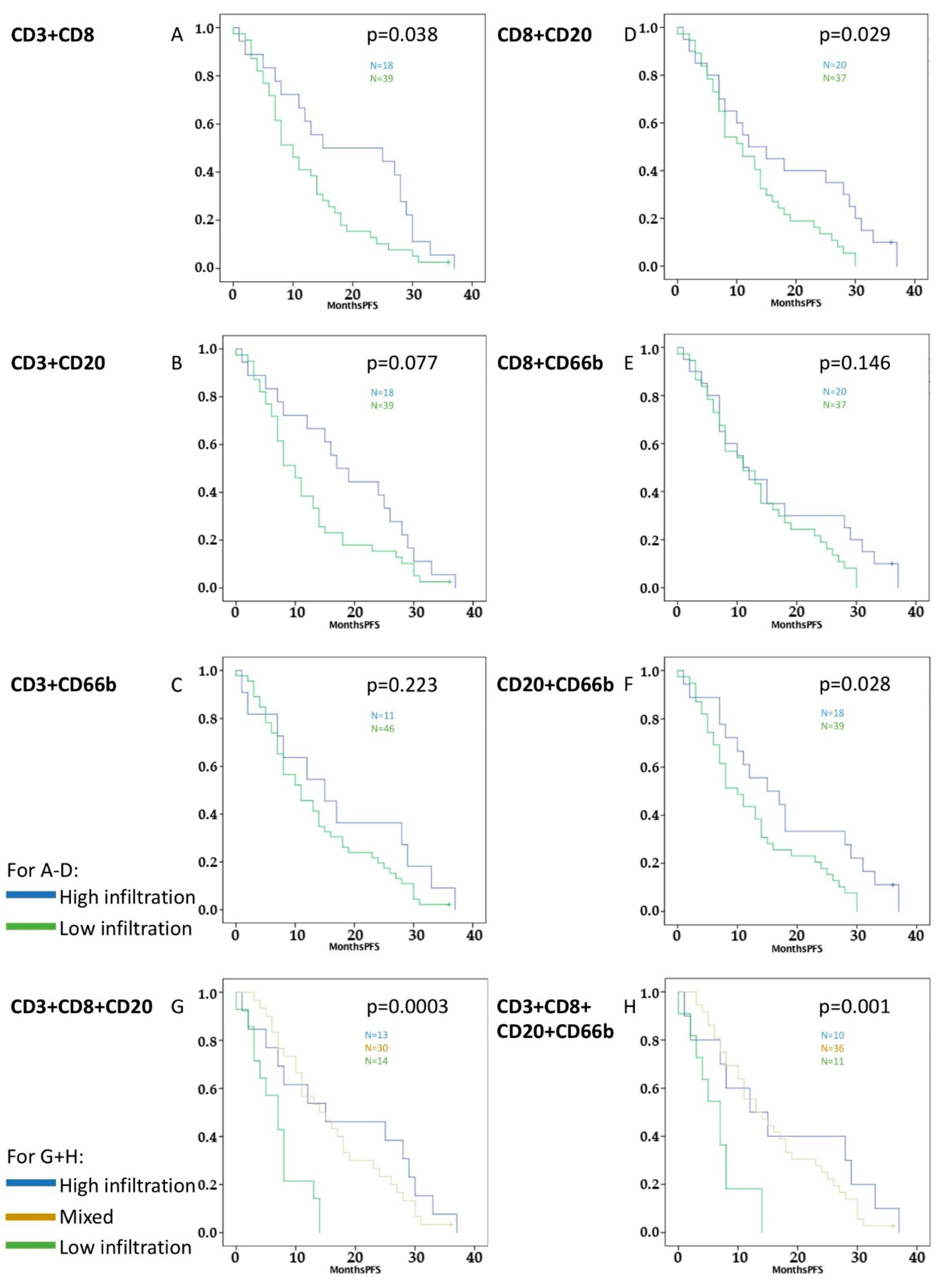
2.2. Accumulation of Peritumoral TILs in PDAC Correlates with Better Survival
2.3. CD3+, CD8+, and CD20+ TILs Predict Survival of Patients with PDAC after 24 Months
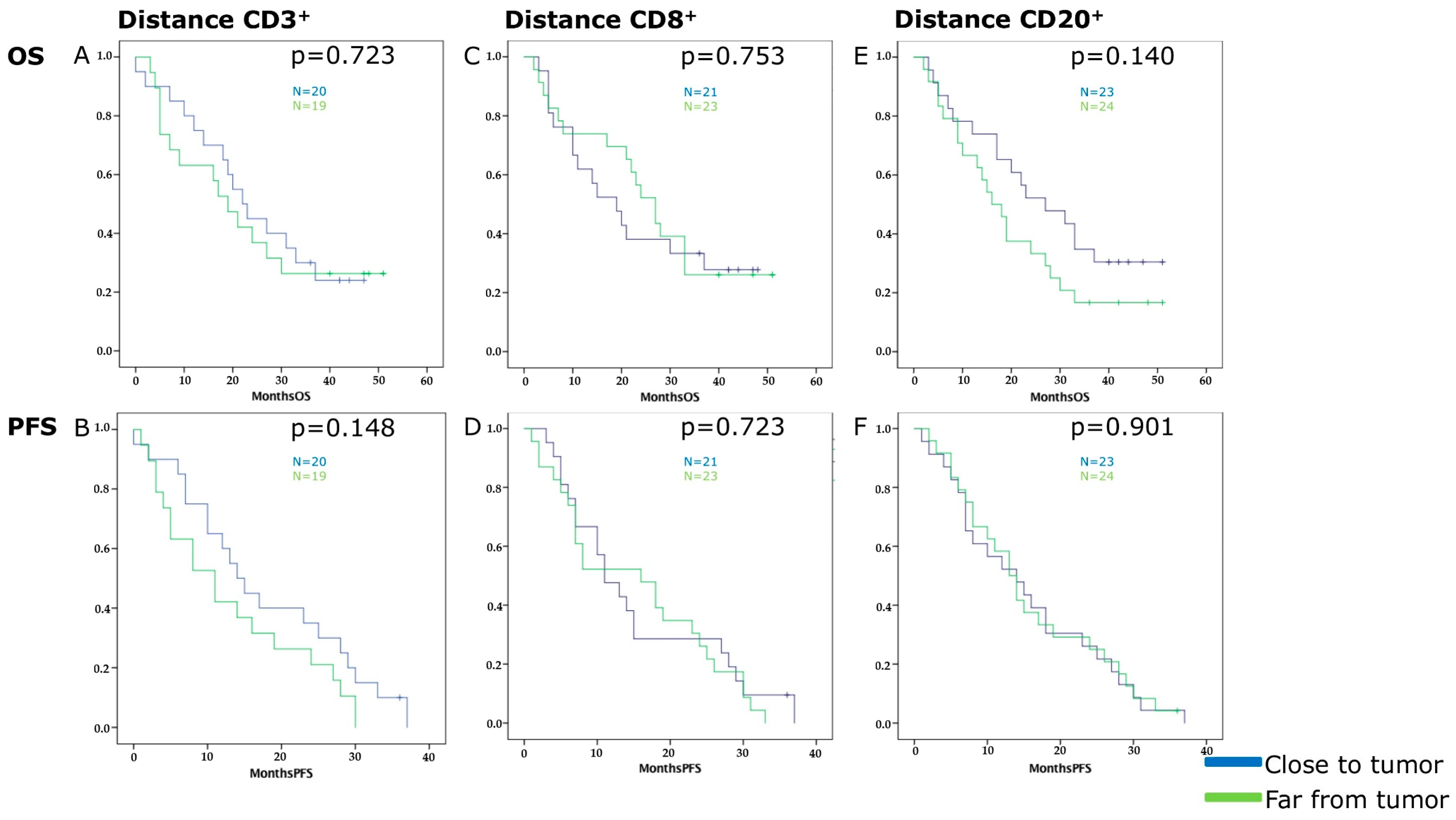
2.4. Distance of TILs’ Hot Spots to the Tumor Front Has No Influence on Survival
2.5. High Accumulation of CD3+ TILs and High Density of Collagen Correlate with Improved Survival in a Multivariate Analysis
3. Discussion
4. Material and Methods
4.1. Patients and Clinical Data
4.2. Material
4.3. Immunohistochemistry
4.4. Analysis of Immunohistochemistry
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2012. CA Cancer J. Clin. 2012, 62, 10–29. [Google Scholar] [CrossRef] [PubMed]
- Qiu, D.; Kurosawa, M.; Lin, Y.; Inaba, Y.; Matsuba, T.; Kikuchi, S.; Yagyu, K.; Motohashi, Y.; Tamakoshi, A. Overview of the epidemiology of pancreatic cancer focusing on the JACC Study. J. Epidemiol. 2005, 15 (Suppl. 2), S157–S167. [Google Scholar] [CrossRef]
- Talamini, G.; Bassi, C.; Falconi, M.; Sartori, N.; Salvia, R.; Rigo, L.; Castagnini, A.; Di Francesco, V.; Frulloni, L.; Bovo, P.; et al. Alcohol and smoking as risk factors in chronic pancreatitis and pancreatic cancer. Dig. Dis. Sci. 1999, 44, 1303–1311. [Google Scholar] [CrossRef] [PubMed]
- Yadav, D.; Whitcomb, D.C. The role of alcohol and smoking in pancreatitis. Nat. Rev. Gastroenterol. Hepatol. 2010, 7, 131–145. [Google Scholar] [CrossRef] [PubMed]
- Raimondi, S.; Maisonneuve, P.; Lowenfels, A.B. Epidemiology of pancreatic cancer: An overview. Nat. Rev. Gastroenterol. Hepatol. 2009, 6, 699–708. [Google Scholar] [CrossRef] [PubMed]
- Hartwig, W.; Strobel, O.; Hinz, U.; Fritz, S.; Hackert, T.; Roth, C.; Buchler, M.W.; Werner, J. CA19-9 in potentially resectable pancreatic cancer: Perspective to adjust surgical and perioperative therapy. Ann. Surg. Oncol. 2013, 20, 2188–2196. [Google Scholar] [CrossRef] [PubMed]
- Lowenfels, A.B.; Maisonneuve, P.; Cavallini, G.; Ammann, R.W.; Lankisch, P.G.; Andersen, J.R.; DiMagno, E.P.; Andren-Sandberg, A.; Domellof, L.; Di Francesco, V.; et al. Prognosis of chronic pancreatitis: An international multicenter study. Am. J. Gastroenterol. 1994, 89, 1467–1471. [Google Scholar]
- Coveler, A.L.; Herman, J.M.; Simeone, D.M.; Chiorean, E.G. Localized pancreatic cancer: Multidisciplinary management. Am. Soc. Clin. Oncol. Educ. Book 2016, 35, e217–e226. [Google Scholar] [CrossRef]
- Hartwig, W.; Werner, J.; Buchler, M.W. Prognosis of resected pancreatic cancer: Is the refined resection margin status dispensable? Langenbecks Arch. Surg. 2012, 397, 859–860. [Google Scholar] [CrossRef]
- Kamarajah, S.K.; Burns, W.R.; Frankel, T.L.; Cho, C.S.; Nathan, H. Validation of the American Joint Commission on Cancer (AJCC) 8th edition staging system for patients with pancreatic adenocarcinoma: A Surveillance, Epidemiology and End Results (SEER) analysis. Ann. Surg. Oncol. 2017, 24, 2023–2030. [Google Scholar] [CrossRef]
- Yao, W.; He, J.C.; Yang, Y.; Wang, J.M.; Qian, Y.W.; Yang, T.; Ji, L. The prognostic value of tumor-infiltrating lymphocytes in hepatocellular carcinoma: A systematic review and meta-analysis. Sci. Rep. 2017, 7, 7525. [Google Scholar] [CrossRef] [PubMed]
- Fukunaga, A.; Miyamoto, M.; Cho, Y.; Murakami, S.; Kawarada, Y.; Oshikiri, T.; Kato, K.; Kurokawa, T.; Suzuoki, M.; Nakakubo, Y.; et al. CD8+ tumor-infiltrating lymphocytes together with CD4+ tumor-infiltrating lymphocytes and dendritic cells improve the prognosis of patients with pancreatic adenocarcinoma. Pancreas 2004, 28, e26–e31. [Google Scholar] [CrossRef] [PubMed]
- Bazhin, A.V.; Bayry, J.; Umansky, V.; Werner, J.; Karakhanova, S. Overcoming immunosuppression as a new immunotherapeutic approach against pancreatic cancer. Oncoimmunology 2013, 2, e25736. [Google Scholar] [CrossRef] [PubMed]
- Bazhin, A.V.; Shevchenko, I.; Umansky, V.; Werner, J.; Karakhanova, S. Two immune faces of pancreatic adenocarcinoma: Possible implication for immunotherapy. Cancer Immunol. Immunother. 2014, 63, 59–65. [Google Scholar] [CrossRef] [PubMed]
- Nejati, R.; Goldstein, J.B.; Halperin, D.M.; Wang, H.; Hejazi, N.; Rashid, A.; Katz, M.H.; Lee, J.E.; Fleming, J.B.; Rodriguez-Canales, J.; et al. Prognostic significance of tumor-infiltrating lymphocytes in patients with pancreatic ductal adenocarcinoma treated with neoadjuvant chemotherapy. Pancreas 2017, 46, 1180–1187. [Google Scholar] [CrossRef] [PubMed]
- Hall, M.; Liu, H.; Malafa, M.; Centeno, B.; Hodul, P.J.; Pimiento, J.; Pilon-Thomas, S.; Sarnaik, A.A. Expansion of tumor-infiltrating lymphocytes (TIL) from human pancreatic tumors. J. Immunother. Cancer 2016, 4, 61. [Google Scholar] [CrossRef] [PubMed]
- Shibuya, K.C.; Goel, V.K.; Xiong, W.; Sham, J.G.; Pollack, S.M.; Leahy, A.M.; Whiting, S.H.; Yeh, M.M.; Yee, C.; Riddell, S.R.; et al. Pancreatic ductal adenocarcinoma contains an effector and regulatory immune cell infiltrate that is altered by multimodal neoadjuvant treatment. PLoS ONE 2014, 9, e96565. [Google Scholar] [CrossRef] [PubMed]
- Tjomsland, V.; Niklasson, L.; Sandstrom, P.; Borch, K.; Druid, H.; Bratthall, C.; Messmer, D.; Larsson, M.; Spangeus, A. The desmoplastic stroma plays an essential role in the accumulation and modulation of infiltrated immune cells in pancreatic adenocarcinoma. Clin. Dev. Immunol. 2011, 2011, 212810. [Google Scholar] [CrossRef] [PubMed]
- Karakhanova, S.; Ryschich, E.; Mosl, B.; Harig, S.; Jager, D.; Schmidt, J.; Hartwig, W.; Werner, J.; Bazhin, A.V. Prognostic and predictive value of immunological parameters for chemoradioimmunotherapy in patients with pancreatic adenocarcinoma. Br. J. Cancer 2015, 112, 1027–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahkola, K.; Mecklin, J.P.; Wirta, E.V.; Ahtiainen, M.; Helminen, O.; Bohm, J.; Kellokumpu, I. High immune cell score predicts improved survival in pancreatic cancer. Virchows Arch. 2018, 472, 653–665. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Pages, F.; Marincola, F.M.; Thurin, M.; Trinchieri, G.; Fox, B.A.; Gajewski, T.F.; Ascierto, P.A. The immune score as a new possible approach for the classification of cancer. J. Transl. Med. 2012, 10, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mlecnik, B.; Bindea, G.; Kirilovsky, A.; Angell, H.K.; Obenauf, A.C.; Tosolini, M.; Church, S.E.; Maby, P.; Vasaturo, A.; Angelova, M.; et al. The tumor microenvironment and immunoscore are critical determinants of dissemination to distant metastasis. Sci. Transl. Med. 2016, 8, 327ra326. [Google Scholar] [CrossRef] [PubMed]
- Anitei, M.G.; Zeitoun, G.; Mlecnik, B.; Marliot, F.; Haicheur, N.; Todosi, A.M.; Kirilovsky, A.; Lagorce, C.; Bindea, G.; Ferariu, D.; et al. Prognostic and predictive values of the immunoscore in patients with rectal cancer. Clin. Cancer Res. 2014, 20, 1891–1899. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pages, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, density, and location of immune cells within human colorectal tumors predict clinical outcome. Science 2006, 313, 1960–1964. [Google Scholar] [CrossRef] [PubMed]
- Curigliano, G.; Perez, E.A. Immunoscoring breast cancer: TILs remember what they target. Ann. Oncol. 2014, 25, 1455–1456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romagnoli, G.; Wiedermann, M.; Hubner, F.; Wenners, A.; Mathiak, M.; Rocken, C.; Maass, N.; Klapper, W.; Alkatout, I. Morphological evaluation of tumor-infiltrating lymphocytes (TILs) to investigate invasive breast cancer immunogenicity, reveal lymphocytic networks and help relapse prediction: A retrospective study. Int. J. Mol. Sci. 2017, 18, 1936. [Google Scholar] [CrossRef]
- Donnem, T.; Kilvaer, T.K.; Andersen, S.; Richardsen, E.; Paulsen, E.E.; Hald, S.M.; Al-Saad, S.; Brustugun, O.T.; Helland, A.; Lund-Iversen, M.; et al. Strategies for clinical implementation of tnm-immunoscore in resected nonsmall-cell lung cancer. Ann. Oncol. 2016, 27, 225–232. [Google Scholar] [CrossRef]
- Birnbaum, D.J.; Bertucci, F.; Finetti, P.; Birnbaum, D.; Mamessier, E. Molecular classification as prognostic factor and guide for treatment decision of pancreatic cancer. Biochim. Biophys. Acta 2018, 1869, 248–255. [Google Scholar] [CrossRef]
- Arnes, L.; Liu, Z.; Wang, J.; Carlo Maurer, H.; Sagalovskiy, I.; Sanchez-Martin, M.; Bommakanti, N.; Garofalo, D.C.; Balderes, D.A.; Sussel, L.; et al. Comprehensive characterisation of compartment-specific long non-coding RNAs associated with pancreatic ductal adenocarcinoma. Gut 2018. [Google Scholar] [CrossRef]
- Martinelli, P.; Carrillo-de Santa Pau, E.; Cox, T.; Sainz, B., Jr.; Dusetti, N.; Greenhalf, W.; Rinaldi, L.; Costello, E.; Ghaneh, P.; Malats, N.; et al. GATA6 regulates EMT and tumour dissemination, and is a marker of response to adjuvant chemotherapy in pancreatic cancer. Gut 2017, 66, 1665–1676. [Google Scholar] [CrossRef]
- Sahin, I.H.; Lowery, M.A.; Stadler, Z.K.; Salo-Mullen, E.; Iacobuzio-Donahue, C.A.; Kelsen, D.P.; O’Reilly, E.M. Genomic instability in pancreatic adenocarcinoma: A new step towards precision medicine and novel therapeutic approaches. Expert Rev. Gastroenterol. Hepatol. 2016, 10, 893–905. [Google Scholar] [CrossRef] [PubMed]
- Erkan, M.; Hausmann, S.; Michalski, C.W.; Fingerle, A.A.; Dobritz, M.; Kleeff, J.; Friess, H. The role of stroma in pancreatic cancer: Diagnostic and therapeutic implications. Nat. Rev. Gastroenterol. Hepatol. 2012, 9, 454–467. [Google Scholar] [CrossRef]
- Erkan, M.; Michalski, C.W.; Rieder, S.; Reiser-Erkan, C.; Abiatari, I.; Kolb, A.; Giese, N.A.; Esposito, I.; Friess, H.; Kleeff, J. The activated stroma index is a novel and independent prognostic marker in pancreatic ductal adenocarcinoma. Clin. Gastroenterol. Hepatol. 2008, 6, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Neumann, C.C.M.; von Horschelmann, E.; Reutzel-Selke, A.; Seidel, E.; Sauer, I.M.; Pratschke, J.; Bahra, M.; Schmuck, R.B. Tumor-stromal cross-talk modulating the therapeutic response in pancreatic cancer. Hepatobiliary Pancreat. Dis. Int. 2018, 17, 461–472. [Google Scholar] [CrossRef] [PubMed]
- Kabacaoglu, D.; Ciecielski, K.J.; Ruess, D.A.; Algul, H. Immune checkpoint inhibition for pancreatic ductal adenocarcinoma: Current limitations and future options. Front. Immunol. 2018, 9, 1878. [Google Scholar] [CrossRef]
- Martinez-Bosch, N.; Vinaixa, J.; Navarro, P. Immune evasion in pancreatic cancer: From mechanisms to therapy. Cancers 2018, 10, 6. [Google Scholar] [CrossRef]
- Shevchenko, I.; Karakhanova, S.; Soltek, S.; Link, J.; Bayry, J.; Werner, J.; Umansky, V.; Bazhin, A.V. Low-dose gemcitabine depletes regulatory t cells and improves survival in the orthotopic panc02 model of pancreatic cancer. Int. J. Cancer 2013, 133, 98–107. [Google Scholar] [CrossRef]
- Karakhanova, S.; Link, J.; Heinrich, M.; Shevchenko, I.; Yang, Y.; Hassenpflug, M.; Bunge, H.; von Ahn, K.; Brecht, R.; Mathes, A.; et al. Characterization of myeloid leukocytes and soluble mediators in pancreatic cancer: Importance of myeloid-derived suppressor cells. Oncoimmunology 2015, 4, e998519. [Google Scholar] [CrossRef]
- Miksch, R.C.; Hao, J.; Schoenberg, M.B.; Dotzer, K.; Schluter, F.; Weniger, M.; Yin, S.; Ormanns, S.; D’Haese, J.G.; Guba, M.O.; et al. Development of a reliable and accurate algorithm to quantify the tumor immune stroma (QTiS) across tumor types. Oncotarget 2017, 8, 114935–114944. [Google Scholar] [CrossRef]
- Gooden, M.J.; de Bock, G.H.; Leffers, N.; Daemen, T.; Nijman, H.W. The prognostic influence of tumour-infiltrating lymphocytes in cancer: A systematic review with meta-analysis. Br. J. Cancer 2011, 105, 93–103. [Google Scholar] [CrossRef]
- Yang, J.J.; Hu, Z.G.; Shi, W.X.; Deng, T.; He, S.Q.; Yuan, S.G. Prognostic significance of neutrophil to lymphocyte ratio in pancreatic cancer: A meta-analysis. World J. Gastroenterol. 2015, 21, 2807–2815. [Google Scholar] [CrossRef] [PubMed]
- Feng, M.; Xiong, G.; Cao, Z.; Yang, G.; Zheng, S.; Song, X.; You, L.; Zheng, L.; Zhang, T.; Zhao, Y. PD-1/PD-L1 and immunotherapy for pancreatic cancer. Cancer Lett. 2017, 407, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, L.; Rodriguez-Abreu, D.; Gadgeel, S.; Esteban, E.; Felip, E.; De Angelis, F.; Domine, M.; Clingan, P.; Hochmair, M.J.; Powell, S.F.; et al. Pembrolizumab plus chemotherapy in metastatic non-small-cell lung cancer. N. Engl. J. Med. 2018, 378, 2078–2092. [Google Scholar] [CrossRef] [PubMed]
- Eggermont, A.M.M.; Blank, C.U.; Mandala, M.; Long, G.V.; Atkinson, V.; Dalle, S.; Haydon, A.; Lichinitser, M.; Khattak, A.; Carlino, M.S.; et al. Adjuvant pembrolizumab versus placebo in resected stage iii melanoma. N. Engl. J. Med. 2018, 378, 1789–1801. [Google Scholar] [CrossRef] [PubMed]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch repair deficiency predicts response of solid tumors to PD-1 blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garg, B.; Giri, B.; Modi, S.; Sethi, V.; Castro, I.; Umland, O.; Ban, Y.; Lavania, S.; Dawra, R.; Banerjee, S.; et al. Nfkappab in pancreatic stellate cells reduces infiltration of tumors by cytotoxic t cells and killing of cancer cells, via up-regulation of CXCL12. Gastroenterology 2018, 155, 880–891.e8. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, V.P.; Luksza, M.; Zhao, J.N.; Makarov, V.; Moral, J.A.; Remark, R.; Herbst, B.; Askan, G.; Bhanot, U.; Senbabaoglu, Y.; et al. Identification of unique neoantigen qualities in long-term survivors of pancreatic cancer. Nature 2017, 551, 512–516. [Google Scholar] [CrossRef]
- Puleo, F.; Nicolle, R.; Blum, Y.; Cros, J.; Marisa, L.; Demetter, P.; Quertinmont, E.; Svrcek, M.; Elarouci, N.; Iovanna, J.; et al. Stratification of pancreatic ductal adenocarcinomas based on tumor and microenvironment features. Gastroenterology 2018, 155, 1999.e3–2013.e3. [Google Scholar] [CrossRef]
- Mahajan, U.M.; Langhoff, E.; Goni, E.; Costello, E.; Greenhalf, W.; Halloran, C.; Ormanns, S.; Kruger, S.; Boeck, S.; Ribback, S.; et al. Immune cell and stromal signature associated with progression-free survival of patients with resected pancreatic ductal adenocarcinoma. Gastroenterology 2018, 155, 1625.e2–1639.e2. [Google Scholar] [CrossRef]
- Ino, Y.; Yamazaki-Itoh, R.; Shimada, K.; Iwasaki, M.; Kosuge, T.; Kanai, Y.; Hiraoka, N. Immune cell infiltration as an indicator of the immune microenvironment of pancreatic cancer. Br. J. Cancer 2013, 108, 914–923. [Google Scholar] [CrossRef] [Green Version]
- Reid, M.D.; Basturk, O.; Thirabanjasak, D.; Hruban, R.H.; Klimstra, D.S.; Bagci, P.; Altinel, D.; Adsay, V. Tumor-infiltrating neutrophils in pancreatic neoplasia. Mod. Pathol. 2011, 24, 1612–1619. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hiraoka, N.; Onozato, K.; Kosuge, T.; Hirohashi, S. Prevalence of FOXP3+ regulatory T cells increases during the progression of pancreatic ductal adenocarcinoma and its premalignant lesions. Clin. Cancer Res. 2006, 12, 5423–5434. [Google Scholar] [CrossRef] [PubMed]
- Hiraoka, N.; Ino, Y.; Yamazaki-Itoh, R.; Kanai, Y.; Kosuge, T.; Shimada, K. Intratumoral tertiary lymphoid organ is a favourable prognosticator in patients with pancreatic cancer. Br. J. Cancer 2015, 112, 1782–1790. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tewari, N.; Zaitoun, A.M.; Arora, A.; Madhusudan, S.; Ilyas, M.; Lobo, D.N. The presence of tumour-associated lymphocytes confers a good prognosis in pancreatic ductal adenocarcinoma: An immunohistochemical study of tissue microarrays. BMC Cancer 2013, 13, 436. [Google Scholar] [CrossRef] [PubMed]
- Lohneis, P.; Sinn, M.; Bischoff, S.; Juhling, A.; Pelzer, U.; Wislocka, L.; Bahra, M.; Sinn, B.V.; Denkert, C.; Oettle, H.; et al. Cytotoxic tumour-infiltrating T lymphocytes influence outcome in resected pancreatic ductal adenocarcinoma. Eur. J. Cancer 2017, 83, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Ansari, D.; Aronsson, L.; Sasor, A.; Welinder, C.; Rezeli, M.; Marko-Varga, G.; Andersson, R. The role of quantitative mass spectrometry in the discovery of pancreatic cancer biomarkers for translational science. J. Transl. Med. 2014, 12, 87. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, D.; Friess, H.; Bauden, M.; Samnegard, J.; Andersson, R. Pancreatic cancer: Disease dynamics, tumor biology and the role of the microenvironment. Oncotarget 2018, 9, 6644–6651. [Google Scholar] [CrossRef]
- Wartenberg, M.; Zlobec, I.; Perren, A.; Koelzer, V.H.; Gloor, B.; Lugli, A.; Karamitopoulou, E. Accumulation of FOXP3+T-cells in the tumor microenvironment is associated with an epithelial-mesenchymal-transition-type tumor budding phenotype and is an independent prognostic factor in surgically resected pancreatic ductal adenocarcinoma. Oncotarget 2015, 6, 4190–4201. [Google Scholar] [CrossRef] [Green Version]
- Murakami, T.; Homma, Y.; Matsuyama, R.; Mori, R.; Miyake, K.; Tanaka, Y.; Den, K.; Nagashima, Y.; Nakazawa, M.; Hiroshima, Y.; et al. Neoadjuvant chemoradiotherapy of pancreatic cancer induces a favorable immunogenic tumor microenvironment associated with increased major histocompatibility complex class I-related chain A/B expression. J. Surg. Oncol. 2017, 116, 416–426. [Google Scholar] [CrossRef]
- Tang, Y.; Xu, X.; Guo, S.; Zhang, C.; Tang, Y.; Tian, Y.; Ni, B.; Lu, B.; Wang, H. An increased abundance of tumor-infiltrating regulatory T cells is correlated with the progression and prognosis of pancreatic ductal adenocarcinoma. PLoS ONE 2014, 9, e91551. [Google Scholar] [CrossRef]
- Khouja, M.H.; Baekelandt, M.; Sarab, A.; Nesland, J.M.; Holm, R. Limitations of tissue microarrays compared with whole tissue sections in survival analysis. Oncol. Lett. 2010, 1, 827–831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckel-Passow, J.E.; Lohse, C.M.; Sheinin, Y.; Crispen, P.L.; Krco, C.J.; Kwon, E.D. Tissue microarrays: One size does not fit all. Diagn. Pathol. 2010, 5, 48. [Google Scholar] [CrossRef] [PubMed]
- Chavan, S.S.; Ravindra, S.; Prasad, M. Breast biomarkers-comparison on whole section and tissue microarray section. J. Clin. Diagn. Res. 2017, 11, ec40–ec44. [Google Scholar] [CrossRef] [PubMed]
- Kyndi, M.; Sorensen, F.B.; Knudsen, H.; Overgaard, M.; Nielsen, H.M.; Andersen, J.; Overgaard, J. Tissue microarrays compared with whole sections and biochemical analyses. A subgroup analysis of DBCG 82 b&c. Acta Oncol. 2008, 47, 591–599. [Google Scholar] [PubMed]
- Foucher, E.D.; Ghigo, C.; Chouaib, S.; Galon, J.; Iovanna, J.; Olive, D. Pancreatic ductal adenocarcinoma: A strong imbalance of good and bad immunological cops in the tumor microenvironment. Front. Immunol. 2018, 9, 1044. [Google Scholar] [CrossRef] [PubMed]
- Pergamo, M.; Miller, G. Myeloid-derived suppressor cells and their role in pancreatic cancer. Cancer Gene Ther. 2017, 24, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Ren, B.; Cui, M.; Yang, G.; Wang, H.; Feng, M.; You, L.; Zhao, Y. Tumor microenvironment participates in metastasis of pancreatic cancer. Mol. Cancer 2018, 17, 108. [Google Scholar] [CrossRef]
- Habtezion, A.; Edderkaoui, M.; Pandol, S.J. Macrophages and pancreatic ductal adenocarcinoma. Cancer Lett. 2016, 381, 211–216. [Google Scholar] [CrossRef] [Green Version]
- Schoenberg, M.; Hao, J.; Bucher, J.N.; Miksch, R.C.; Anger, H.J.W.; Mayer, B.; Mayerle, J.; Neumann, J.; Guba, M.O.; Werner, J.; et al. Perivascular tumor-infiltrating leukocyte scoring for prognosis of resected hepatocellular carcinoma patients. Cancers 2018, 10, 389. [Google Scholar] [CrossRef]
- Pages, F.; Mlecnik, B.; Marliot, F.; Bindea, G.; Ou, F.S.; Bifulco, C.; Lugli, A.; Zlobec, I.; Rau, T.T.; Berger, M.D.; et al. International validation of the consensus immunoscore for the classification of colon cancer: A prognostic and accuracy study. Lancet 2018, 391, 2128–2139. [Google Scholar] [CrossRef]
- Maxwell, P.; McCluggage, W.G. Audit and internal quality control in immunohistochemistry. J. Clin. Pathol. 2000, 53, 929–932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Results |
|---|---|
| Age (Year, Mean ± SD) | 70.44 ± 8.328 |
| Gender (Female/Male) | 31 (54.4%)/26 (45.6%) |
| Operation | 23 PrPD (40.4%) 15 PPPD (26.3%) 13 Left resection (22.8%) 6 Pancreatectomy (10.5%) |
| Location | 38 Head (66.7%) 7 Corpus (12.3%) 11 Tail (19.3%) 1 Corpus + tail (1.8%) |
| TNM Classification Grading | 3 G1 (5.3%) 15 G2 (26.3%) 38 G3 (66.7%) 1 G4 (1.8%) |
| TNM Classification Tumor | 1 T2 (1.8%) 55 T3 (96.5%) 1 T4 (1.8%) |
| TNM Classification Lymph Nodes | 23 N0 (40.4%) 33 N1 (57.9%) 1 N2 (1.8%) |
| TNM Classification Resection | 57 R0 (100%) |
| TNM Classification Metastasis | 57 M0 (100%) |
| Tumor size (Centimetres) | 1.4–8.0 cm (median 3.2 cm) |
| Necrosis | 28 Grade 0 (49.1%) 19 Grade 1 (33.3%) 10 Grade 2 (17.5%) |
| CD3+ TILs (concentration) | 0–39.667 (median 101)/0.145 mm2 |
| CD8+ TILs (concentration) | 0–72.467 (median 83)/0.145 mm2 |
| CD20+ TILs (concentration) | 0–752.333 (median 121)/0.145 mm2 |
| CD66b+ TINs (concentration) | 0–429.667 (median 59.333)/0.145 mm2 |
| CAFs (Mean pixels) | 0.390–46.752 (median 17.089) |
| Collagen (Mean pixels) | 2.354–168.373 (median 56.37) |
| Variables | CD3 | CD8 | CD20 | CD66b | α-sma | Collagen |
|---|---|---|---|---|---|---|
| Age | 0.508 | 0.558 | 0.840 | 0.583 | 0.876 | 0.805 |
| Gender | 0.682 | 0.238 | 0.347 | 0.829 | 1.000 | 0.768 |
| Operation | 0.603 | 0.996 | 0.793 | 0.209 | 1.000 | 0.746 |
| Location | 0.316 | 0.483 | 0.597 | 0.748 | 0.561 | 0.711 |
| TNM Grading | 0.609 | 0.719 | 0.105 | 0.734 | 0.323 | 0.421 |
| TNM Tumor | 0.999 | 1.000 | 0.999 | 1.000 | 0.999 | 0.999 |
| TNM Nodes | 0.361 | 0.682 | 0.682 | 0.740 | 0.093 | 0.372 |
| Tumor size | 0.330 | 0.310 | 0.399 | 0.580 | 0.392 | 0.081 |
| Necrosis | 0.094 | 0.684 | 0.684 | 0.308 | 1.000 | 0.101 |
| Thrombocytes | 0.417 | 0.269 | 0.774 | 0.882 | 0.213 | 0.168 |
| Albumin | 0.362 | 0.301 | 0.735 | 0.467 | 0.799 | 0.078 |
| CRP | 0.796 | 0.673 | 0.079 | 0.870 | 0.877 | 0.220 |
| Leukocytes | 0.686 | 0.313 | 0.849 | 0.894 | 0.029 | 0.953 |
| Haemoglobin | 0.565 | 0.117 | 0.106 | 0.258 | 0.422 | 0.218 |
| Creatinine | 0.357 | 0.542 | 0.546 | 0.910 | 0.283 | 0.098 |
| Bilirubin | 0.194 | 0.303 | 0.889 | 0.819 | 0.699 | 0.136 |
| γ-GT | 0.433 | 0.694 | 0.854 | 0.479 | 0.924 | 0.576 |
| AP | 0.590 | 0.305 | 0.940 | 0.413 | 0.795 | 0.085 |
| Lipase | 0.404 | 0.804 | 0.717 | 0.923 | 0.997 | 0.601 |
| CEA | 0.073 | 0.543 | 0.229 | 0.356 | 0.733 | 0.444 |
| CA 19-9 | 0.501 | 0.842 | 0.185 | 0.880 | 0.242 | 0.987 |
| CD3 | 0.088 | 0.049 | 0.360 | 1.000 | 0.363 | |
| CD8 | 0.088 | 0.003 | * | 0.127 | 0.537 | |
| CD20 | 0.049 | 0.003 | 0.003 | 0.120 | 0.191 | |
| CD66b | 0.360 | * | 0.003 | 0.001 | 0.516 | |
| α-sma | 1.000 | 0.127 | 0.120 | 0.001 | 0.537 | |
| Collagen | 0.363 | 0.537 | 0.191 | 0.516 | 0.537 |
| TILs | AUC | 95% CI | 95% CI | p-Value |
|---|---|---|---|---|
| CD3 | 0.678 | 0.534 | 0.822 | 0.025 |
| CD8 | 0.678 | 0.534 | 0.822 | 0.025 |
| CD20 | 0.729 | 0.593 | 0.866 | 0.004 |
| CD66b | 0.587 | 0.434 | 0.740 | 0.272 |
| CD3 + 8 | 0.687 | 0.539 | 0.835 | 0.018 |
| CD3 + 20 | 0.687 | 0.539 | 0.835 | 0.018 |
| CD3 + 66b | 0.602 | 0.446 | 0.758 | 0.198 |
| CD8 + 20 | 0.695 | 0.549 | 0.841 | 0.014 |
| CD8 + 66b | 0.621 | 0.469 | 0.774 | 0.125 |
| CD20 + 66b | 0.687 | 0.539 | 0.835 | 0.018 |
| CD3 + 8 + 20 | 0.737 | 0.607 | 0.867 | 0.003 |
| CD3 + 8 + 20 + 66b | 0.693 | 0.554 | 0.832 | 0.015 |
| Variables | Overall Survival | Progression-Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| β Coefficient | 95% CI | p-Value | β-Coefficient | 95% CI | p-Value | |||
| Age | 0.000 | −0.494 | 0.495 | 0.999 | −0.053 | −0.383 | 0.277 | 0.747 |
| Gender | −4.736 | −12.830 | 3.359 | 0.246 | −3.351 | −8.753 | 2.050 | 0.219 |
| Operation | 0.872 | −4.301 | 3.659 | 0.872 | 0.342 | −2.317 | 3.001 | 0.797 |
| Location | −0.634 | −5.384 | 4.116 | 0.790 | −0.377 | −3.552 | 2.798 | 0.813 |
| TNM Grading | 0.681 | 0.840 | −6.045 | 0.406 | −0.957 | −5.446 | 3.531 | 0.671 |
| TNM Tumor | −20.500 | −41.575 | 0.575 | 0.056 | −12.000 | −26.197 | 2.197 | 0.096 |
| TNM Nodes | 1.000 | −6.821 | 8.821 | 0.799 | 0.284 | −4.945 | 5.513 | 0.914 |
| Tumor size | −0.870 | −4.119 | 2.378 | 0.593 | −0.822 | −2.987 | 1.344 | 0.450 |
| Necrosis | −5.692 | −10.890 | −0.494 | 0.032 | −3.638 | −7.125 | −0.152 | 0.041 |
| CD3 | −12.930 | −20.309 | −5.550 | 0.001 | −8.555 | −13.498 | −3.613 | 0.001 |
| CD8 | −9.280 | −17.050 | −1.509 | 0.020 | −5.256 | −10.525 | 0.012 | 0.051 |
| CD20 | −8.340 | −16.188 | −0.492 | 0.038 | −5.975 | −11.188 | −0.763 | 0.025 |
| CD66b | −3.395 | −11.570 | 4.780 | 0.409 | −1.344 | −6.829 | 4.142 | 0.625 |
| α-sma | 4.810 | −5.050 | 14.669 | 0.330 | 1.095 | −4.707 | 6.897 | 0.705 |
| Collagen | −11.427 | −20.726 | −2.128 | 0.017 | −6.864 | −12.254 | −1.473 | 0.014 |
| Stroma index | −3.988 | −8.266 | 0.290 | 0.067 | −1.755 | −4.294 | 0.784 | 0.170 |
| Distance CD8 | 3.576 | −6.191 | 13.342 | 0.464 | −0.164 | −6.791 | 6.464 | 0.961 |
| Distance CD20 | −6.612 | −15.404 | 2.180 | 0.137 | 0.406 | −5.649 | 6.460 | 0.893 |
| Thrombocytes | 0.02 | −0.044 | 0.048 | 0.931 | 0.013 | −0.017 | 0.044 | 0.383 |
| Albumin | −2.121 | −8.740 | 4.498 | 0.517 | 0.551 | −4.426 | 5.528 | 0.822 |
| CRP | −0.718 | −2.121 | 0.685 | 0.309 | −0.343 | −1.263 | 0.576 | 0.457 |
| Leukocytes | 0.000 | −0.001 | 0.002 | 0.847 | 0.000 | −0.001 | 0.001 | 0.786 |
| Haemoglobin | 0.373 | −1.810 | 2.557 | 0.733 | 0.516 | −0.938 | 1.971 | 0.480 |
| Creatinine | −1.790 | −12.366 | 8.785 | 0.736 | −2.448 | −9.492 | 4.596 | 0.489 |
| Bilirubin | 0.523 | −0.240 | 1.286 | 0.175 | 0.276 | −0.237 | 0.789 | 0.285 |
| γ-GT | 0.001 | −0.005 | 0.008 | 0.730 | 0.002 | −0.002 | 0.006 | 0.341 |
| AP | 0.007 | −0.009 | 0.024 | 0.376 | 0.002 | −0.009 | 0.013 | 0.700 |
| Lipase | −0.058 | −0.174 | 0.057 | 0.309 | −0.019 | −0.096 | 0.057 | 0.610 |
| CEA | −0.037 | −0.071 | −0.003 | 0.033 | −0.016 | −0.039 | 0.008 | 0.181 |
| CA 19-9 | −0.329 | −0.972 | 0.314 | 0.309 | −0.297 | −0.729 | 0.134 | 0.172 |
| Adjuvant | 0.006 | −0.002 | 0.014 | 0.132 | 0.017 | 0.006 | 0.028 | 0.004 |
| CD3/α-sma | 0.282 | −0.004 | 0.567 | 0.053 | 0.205 | −0.292 | 0.701 | 0.410 |
| CD3/collagen | −0.030 | −0.402 | 0.343 | 0.873 | 0.123 | −0.499 | 0.746 | 0.691 |
| CD8/α-sma | −0.207 | −3.465 | 3.051 | 0.899 | 0.691 | −4.899 | 6.282 | 0.804 |
| CD8/collagen | −0.090 | −0.271 | 0.092 | 0.324 | −0.112 | −0.425 | 0.201 | 0.475 |
| CD20/α-sma | 0.484 | −0.561 | 1.529 | 0.355 | 0.438 | −1.370 | 2.246 | 0.627 |
| CD20/collagen | −0.107 | −0.501 | 0.287 | 0.586 | −0.034 | −0.713 | 0.644 | 0.919 |
| CD66b/α-sma | −0.599 | −2.122 | 0.925 | 0.432 | −0.526 | −3.059 | 2.007 | 0.678 |
| CD66b/collagen | −0.174 | −0.323 | −0.024 | 0.024 | −0.263 | −0.512 | −0.014 | 0.039 |
| Variables | Overall Survival | Progression-Free Survival | ||||||
|---|---|---|---|---|---|---|---|---|
| β Coefficient | 95% CI | p-Value | β-Coefficient | 95% CI | p-Value | |||
| CD3 | −9.477 | −18.012 | −0.943 | 0.031 | −6.250 | −11.413 | −1.087 | 0.019 |
| CD8 | −8.643 | −17.439 | 0.152 | 0.054 | ||||
| CD20 | −2.756 | −11.713 | 6.201 | 0.537 | −2.165 | −7.477 | 3.147 | 0.415 |
| Collagen | −10.763 | −19.181 | −2.346 | 0.014 | −6.416 | −11.669 | −1.163 | 0.018 |
| CEA | −0.024 | −0.059 | 0.011 | 0.166 | ||||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miksch, R.C.; Schoenberg, M.B.; Weniger, M.; Bösch, F.; Ormanns, S.; Mayer, B.; Werner, J.; Bazhin, A.V.; D’Haese, J.G. Prognostic Impact of Tumor-Infiltrating Lymphocytes and Neutrophils on Survival of Patients with Upfront Resection of Pancreatic Cancer. Cancers 2019, 11, 39. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11010039
Miksch RC, Schoenberg MB, Weniger M, Bösch F, Ormanns S, Mayer B, Werner J, Bazhin AV, D’Haese JG. Prognostic Impact of Tumor-Infiltrating Lymphocytes and Neutrophils on Survival of Patients with Upfront Resection of Pancreatic Cancer. Cancers. 2019; 11(1):39. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11010039
Chicago/Turabian StyleMiksch, Rainer C., Markus B. Schoenberg, Maximilian Weniger, Florian Bösch, Steffen Ormanns, Barbara Mayer, Jens Werner, Alexandr V. Bazhin, and Jan G. D’Haese. 2019. "Prognostic Impact of Tumor-Infiltrating Lymphocytes and Neutrophils on Survival of Patients with Upfront Resection of Pancreatic Cancer" Cancers 11, no. 1: 39. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11010039