Infiltration of FoxP3+ Regulatory T Cells is a Strong and Independent Prognostic Factor in Head and Neck Squamous Cell Carcinoma

 , ,
, ,
Abstract
:1. Introduction
2. Results
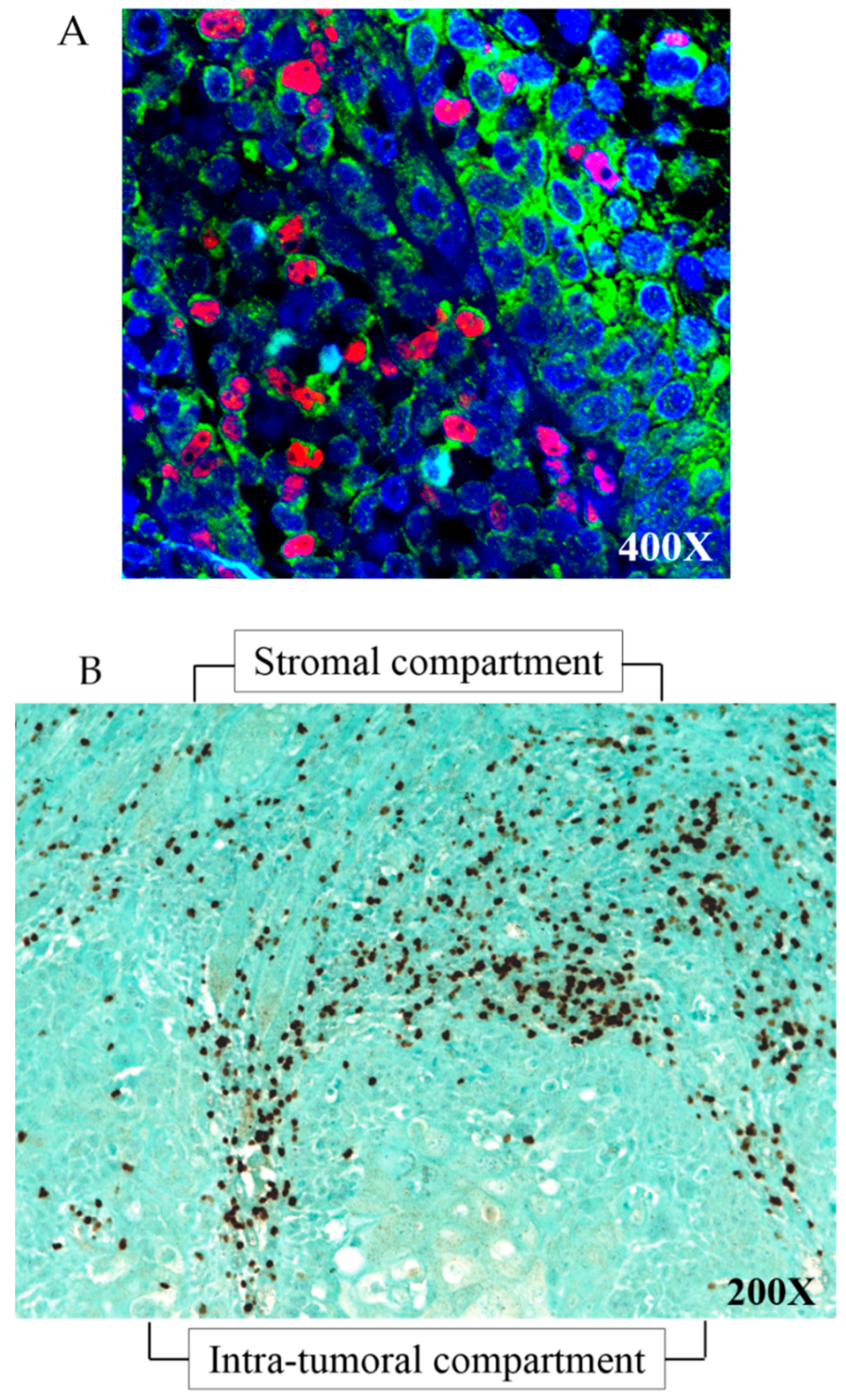
2.1. FoxP3+ Cells Correspond to FoxP3+/CD4+ Treg Cells
2.2. FoxP3+ Treg Infiltration in Stromal and Intra-Tumoral Compartments are Significantly Correlated to Each Other
2.3. FoxP3+ Treg Infiltration Correlated with Some Clinical Characteristics
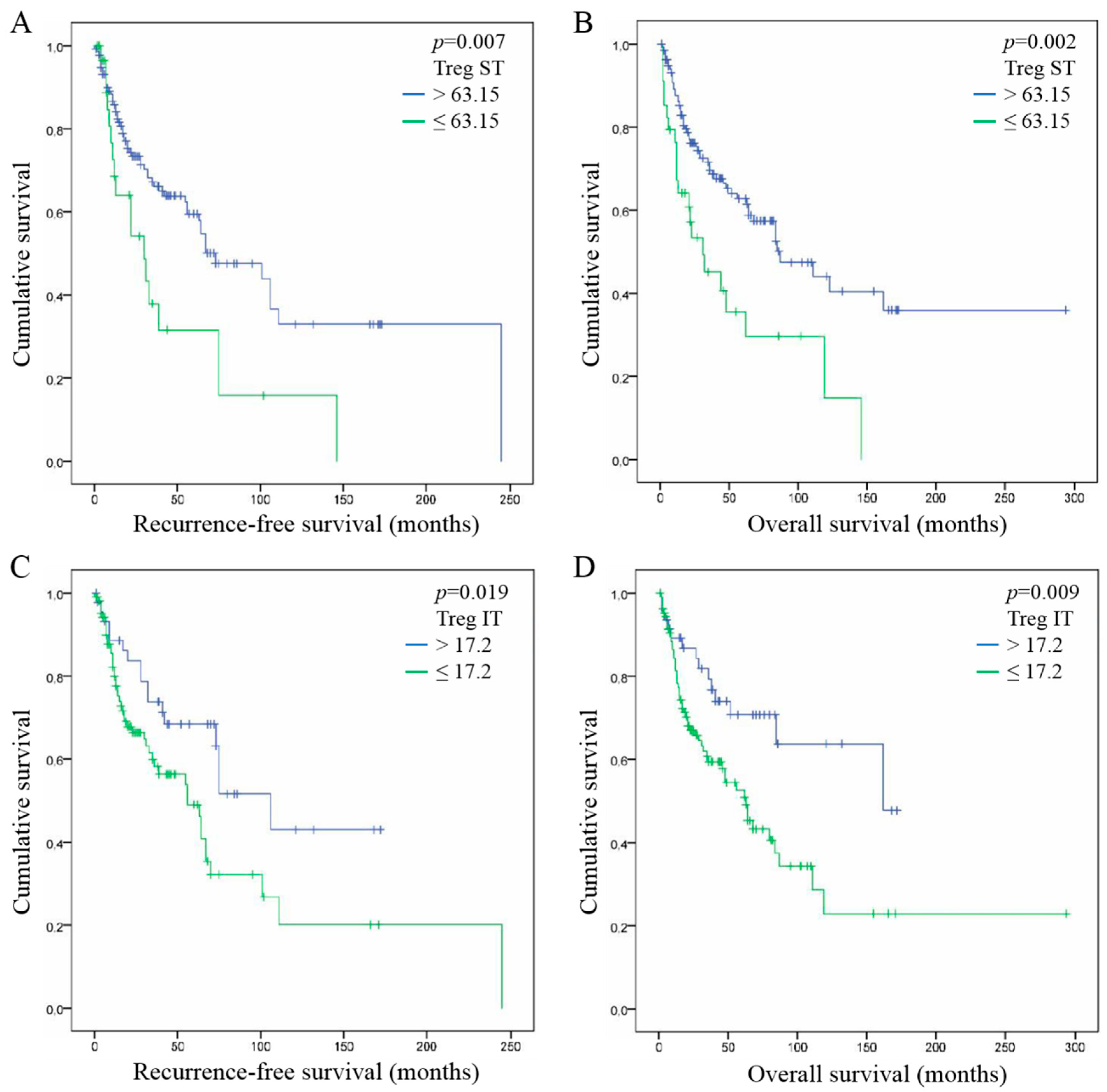
2.4. High FoxP3+ Tregs Infiltration is Associated with Good Prognosis in HNSCC
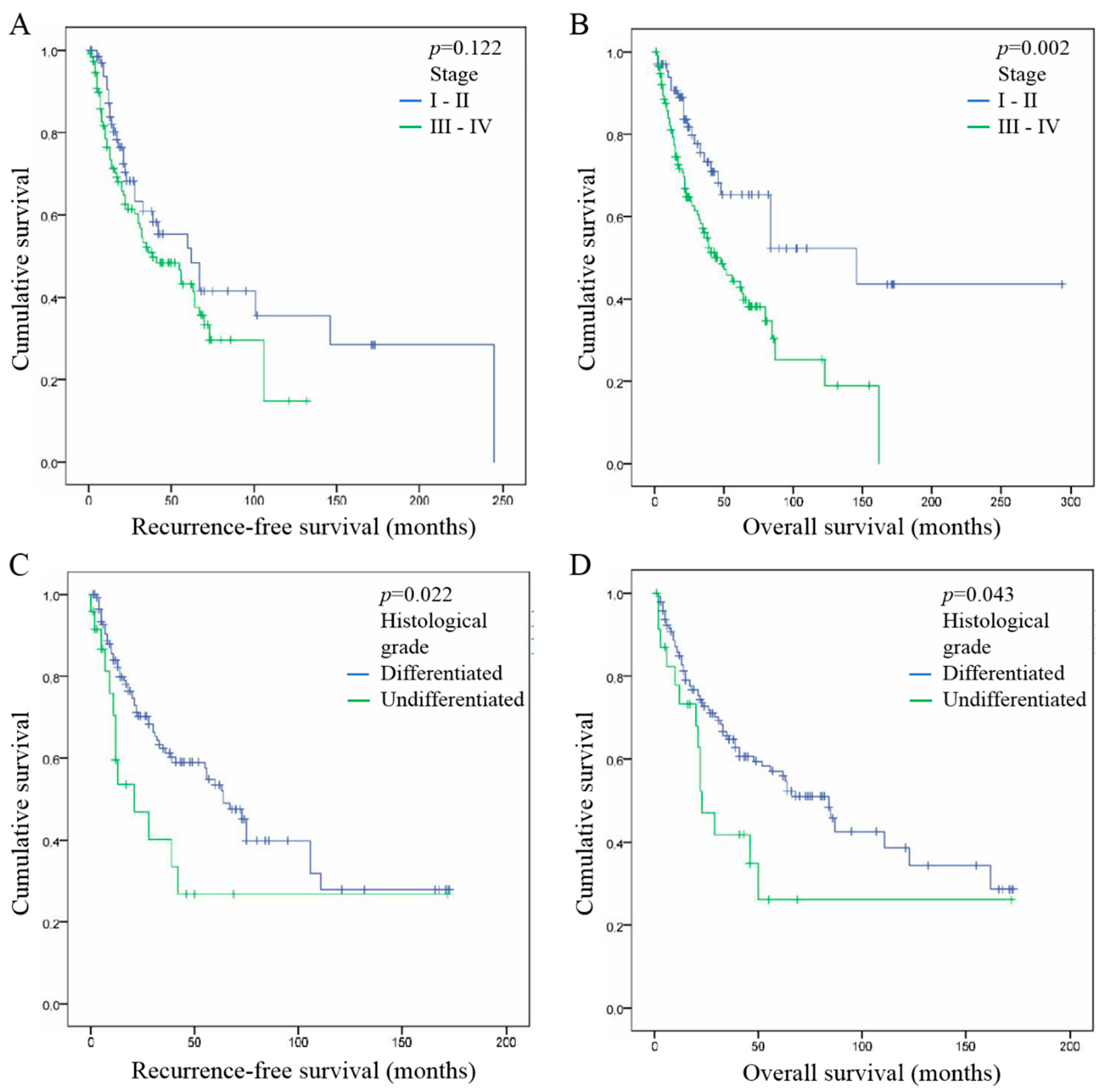
2.5. Tumor Stage and Histological Grade are Both Associated with Good Prognosis in HNSCC
2.6. FoxP3+ Treg Infiltration, Tumor Stage and Histological Grade are Independent Prognostic Factor of HNSCC
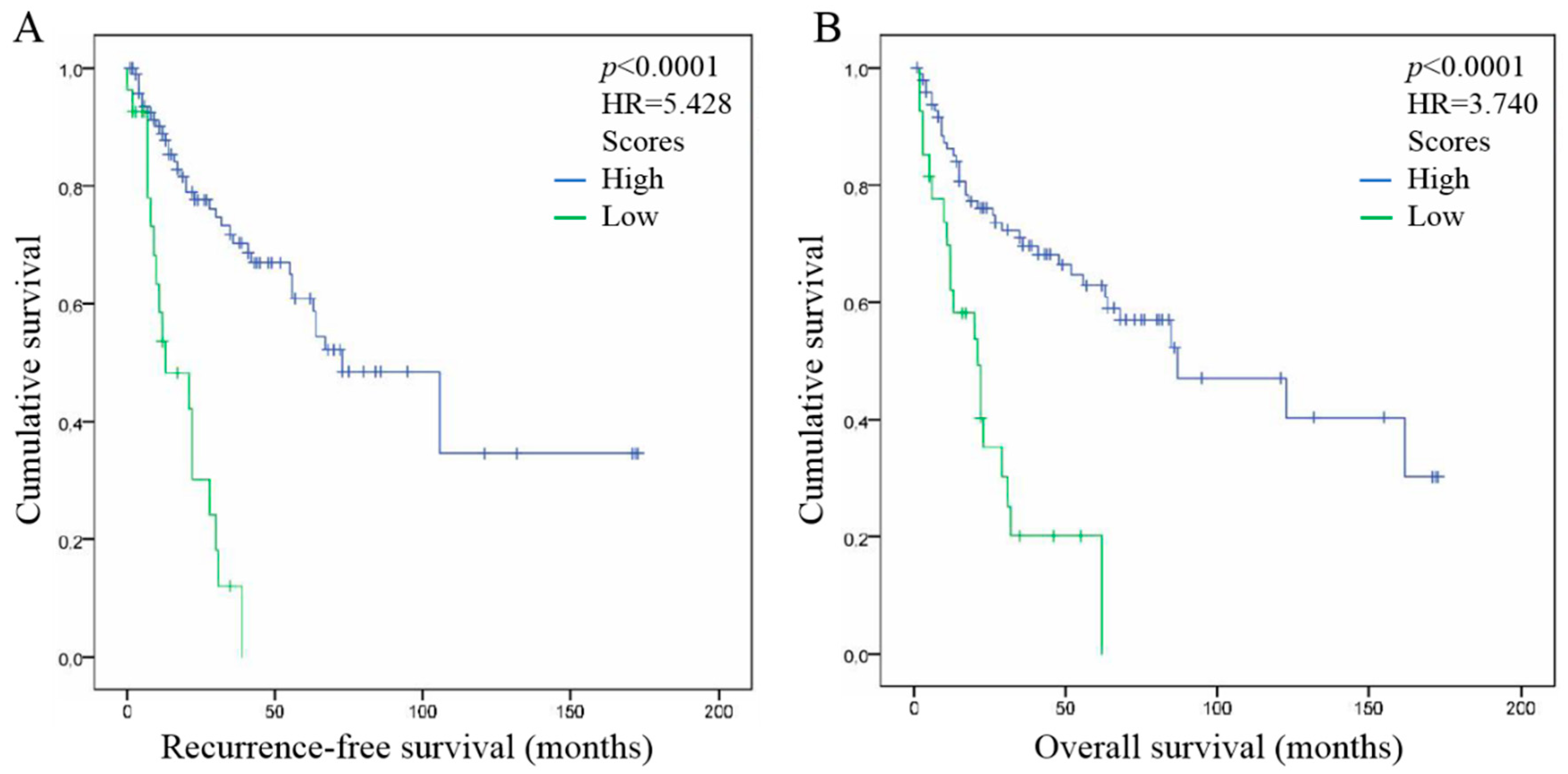
2.7. Combination of FoxP3+ Treg Infiltration in ST, Tumor Stage and Histological Grade Improve the Prediction of HNSCC Patient Outcome
3. Discussion
4. Materials and Methods
4.1. Patients and Clinical Data
4.2. Determination of HPV Status
4.2.1. DNA Extraction
4.2.2. HPV Detection by Polymerase Chain Reaction (PCR) Amplification
4.2.3. Real-Time Quantitative PCR Amplification of HPV Type-Specific DNA
4.2.4. p16 Immunohistochemistry
4.3. Evaluation of Tregs Recruitment
4.3.1. FoxP3 Immunohistochemistry
4.3.2. FoxP3 CD4 Double Immunofluorescence
4.4. Statistical Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Warnakulasuriya, S. Global epidemiology of oral and oropharyngeal cancer. Oral Oncol. 2009, 45, 309–316. [Google Scholar] [CrossRef]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2018. CA Cancer J. Clin. 2018, 68, 7–30. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Strategy to Reduce Harmful Use of Alcohol; World Health Organization: Geneva, Switzerland, 2010; ISBN 978 92 4 159993 1. [Google Scholar]
- World Health Organization. Global Report on Trends in Prevalence of Tobacco Smoking; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-151417-0. [Google Scholar]
- Jou, A.; Hess, J. Epidemiology and Molecular Biology of Head and Neck Cancer. Oncol. Res. Treat. 2017, 40, 328–332. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.A.; Helder, M.N.; de Visscher, J.G.; Leemans, C.R.; Braakhuis, B.J.; de Vet, H.C.W.; Forouzanfar, T. Global incidence of oral and oropharynx cancer in patients younger than 45 years versus older patients: A systematic review. Eur. J. Cancer 2017, 82, 115–127. [Google Scholar] [CrossRef]
- GLOBOCAN. International Agency for Research on Cancer; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Descamps, G.; Karaca, Y.; Lechien, J.R.; Kindt, N.; Decaestecker, C.; Remmelink, M.; Larsimont, D.; Andry, G.; Hassid, S.; Rodriguez, A.; et al. Classical risk factors, but not HPV status, predict survival after chemoradiotherapy in advanced head and neck cancer patients. J. Cancer Res. Clin. Oncol. 2016, 142, 2185–2196. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved survival of patients with human papillomavirus-positive head and neck squamous cell carcinoma in a prospective clinical trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef]
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Rosenquist, K.; Wennerberg, J.; Annertz, K.; Schildt, E.B.; Hansson, B.G.; Bladström, A.; Andersson, G. Recurrence in patients with oral and oropharyngeal squamous cell carcinoma: Human papillomavirus and other risk factors. Acta Otolaryngol. 2007, 127, 980–987. [Google Scholar] [CrossRef]
- Lee, L.A.; Huang, C.G.; Liao, C.T.; Lee, L.Y.; Hsueh, C.; Chen, T.C.; Lin, C.Y.; Fan, K.H.; Wang, H.M.; Huang, S.F.; et al. Human papillomavirus-16 infection in advanced oral cavity cancer patients is related to an increased risk of distant metastases and poor survival. PLoS ONE 2012, 7, e40767. [Google Scholar] [CrossRef]
- Duray, A.; Descamps, G.; Decaestecker, C.; Remmelink, M.; Sirtaine, N.; Lechien, J.; Ernoux-Neufcoeur, P.; Bletard, N.; Somja, J.; Depuydt, C.E.; et al. Human papillomavirus DNA strongly correlates with a poorer prognosis in oral cavity carcinoma. Laryngoscope 2012, 122, 1558–1565. [Google Scholar] [CrossRef] [PubMed]
- Duray, A.; Descamps, G.; Decaestecker, C.; Sirtaine, N.; Gilles, A.; Khalifé, M.; Chantrain, G.; Depuydt, C.E.; Delvenne, P.; Saussez, S. Human papillomavirus predicts the outcome following concomitant chemoradiotherapy in patients with head and neck squamous cell carcinomas. Oncol. Rep. 2013, 30, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Moy, J.D.; Moskovitz, J.M.; Ferris, R.L. Biological mechanisms of immune escape and implications for immunotherapy in head and neck squamous cell carcinoma. Eur. J. Cancer 2017, 76, 152–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vignali, D.A.; Collison, L.W.; Workman, C.J. How regulatory T cells work. Nat. Rev. Immunol. 2008, 8, 523–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soerens, A.G.; Da Costa, A.; Lund, J.M. Regulatory T cells are essential to promote proper CD4 T-cell priming upon mucosal infection. Mucosal Immunol. 2016, 9, 1395–1406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakaguchi, S.; Yamaguchi, T.; Nomura, T.; Ono, M. Regulatory T cells and immune tolerance. Cell 2008, 133, 775–787. [Google Scholar] [CrossRef] [PubMed]
- Shang, B.; Liu, Y.; Jiang, S.J.; Liu, Y. Prognostic value of tumor-infiltrating FoxP3+ regulatory T cells in cancers: A systematic review and meta-analysis. Sci. Rep. 2015, 5, 15179. [Google Scholar] [CrossRef] [PubMed]
- Kindt, N.; Descamps, G.; Seminerio, I.; Bellier, J.; Lechien, J.R.; Mat, Q.; Pottier, C.; Delvenne, P.; Journé, F.; Saussez, S. High stromal Foxp3-positive T cell number combined to tumor stage improved prognosis in head and neck squamous cell carcinoma. Oral Oncol. 2017, 67, 183–191. [Google Scholar] [CrossRef]
- Budczies, J.; Klauschen, F.; Sinn, B.V.; Győrffy, B.; Schmitt, W.D.; Darb-Esfahani, S.; Denkert, C. Cutoff Finder: A comprehensive and straightforward Web application enabling rapid biomarker cutoff optimization. PLoS ONE 2012, 7, e51862. [Google Scholar] [CrossRef]
- Lim, K.P.; Chun, N.A.; Ismail, S.M.; Abraham, M.T.; Yusoff, M.N.; Zain, R.B.; Ngeow, W.C.; Ponniah, S.; Cheong, S.C. CD4+CD25hiCD127low regulatory T cells are increased in oral squamous cell carcinoma patients. PLoS ONE 2014, 9, e103975. [Google Scholar] [CrossRef]
- Sun, W.; Li, W.J.; Fu, Q.L.; Wu, C.Y.; Lin, J.Z.; Zhu, X.L.; Hou, W.J.; Wei, Y.; Wen, Y.H.; Wang, Y.J.; et al. Functionally distinct subsets of CD4⁺ regulatory T cells in patients with laryngeal squamous cell carcinoma are indicative of immune deregulation and disease progression. Oncol. Rep. 2015, 33, 354–362. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, C.; Kim, G.G.; Albers, A.; Hoermann, K.; Myers, E.N.; Whiteside, T.L. Characteristics of CD4+CD25+ regulatory T cells in the peripheral circulation of patients with head and neck cancer. Br. J. Cancer 2005, 92, 913–920. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bron, L.; Jandus, C.; Andrejevic-Blant, S.; Speiser, D.E.; Monnier, P.; Romero, P.; Rivals, J.P. Prognostic value of arginase-II expression and regulatory T-cell infiltration in head and neck squamous cell carcinoma. Int. J. Cancer 2013, 132, E85–E93. [Google Scholar] [CrossRef]
- Mandal, R.; Şenbabaoğlu, Y.; Desrichard, A.; Havel, J.J.; Dalin, M.G.; Riaz, N.; Lee, K.W.; Ganly, I.; Hakimi, A.A.; Chan, T.A.; et al. The head and neck cancer immune landscape and its immunotherapeutic implications. JCI Insight 2016, 1, e89829. [Google Scholar] [CrossRef] [PubMed]
- Maggioni, D.; Pignataro, L.; Garavello, W. T-helper and T-regulatory cells modulation in head and neck squamous cell carcinoma. Oncoimmunology 2017, 6, e1325066. [Google Scholar] [CrossRef] [PubMed]
- Strauss, L.; Bergmann, C.; Gooding, W.; Johnson, J.T.; Whiteside, T.L. The frequency and suppressor function of CD4+CD25highFoxp3+ T cells in the circulation of patients with squamous cell carcinoma of the head and neck. Clin. Cancer Res. 2007, 13, 6301–6311. [Google Scholar] [CrossRef] [PubMed]
- Al-Qahtani, D.; Anil, S.; Rajendran, R. Tumour infiltrating CD25+ FoxP3+ regulatory T cells (Tregs) relate to tumour grade and stromal inflammation in oral squamous cell carcinoma. J. Oral Pathol. Med. 2011, 40, 636–642. [Google Scholar] [CrossRef]
- Liang, Y.J.; Liu, H.C.; Su, Y.X.; Zhang, T.H.; Chu, M.; Liang, L.Z.; Liao, G.Q. Foxp3 expressed by tongue squamous cell carcinoma cells correlates with clinicopathologic features and overall survival in tongue squamous cell carcinoma patients. Oral Oncol. 2011, 47, 566–570. [Google Scholar] [CrossRef]
- Badoual, C.; Hans, S.; Rodriguez, J.; Peyrard, S.; Klein, C.; Agueznay Nel, H.; Mosseri, V.; Laccourreye, O.; Bruneval, P.; Fridman, W.H.; et al. Prognostic value of tumor-infiltrating CD4+ T-cell subpopulations in head and neck cancers. Clin. Cancer Res. 2006, 12, 465–472. [Google Scholar] [CrossRef]
- Kim, H.R.; Ha, S.J.; Hong, M.H.; Heo, S.J.; Koh, Y.W.; Choi, E.C.; Kim, E.K.; Pyo, K.H.; Jung, I.; Seo, D.; et al. PD-L1 expression on immune cells, but not on tumor cells, is a favorable prognostic factor for head and neck cancer patients. Sci. Rep. 2016, 6, 36956. [Google Scholar] [CrossRef] [Green Version]
- Saito, T.; Nishikawa, H.; Wada, H.; Nagano, Y.; Sugiyama, D.; Atarashi, K.; Maeda, Y.; Hamaguchi, M.; Ohkura, N.; Sato, E.; et al. Two FOXP3(+)CD4(+) T cell subpopulations distinctly control the prognosis of colorectal cancers. Nat. Med. 2016, 22, 679–684. [Google Scholar] [CrossRef] [PubMed]
- Dahm, V.; Haitel, A.; Kaider, A.; Stanisz, I.; Beer, A.; Lill, C. Cancer stage and pack-years, but not p16 or HPV, are relevant for survival in hypopharyngeal and laryngeal squamous cell carcinomas. Eur. Arch. Otorhinolaryngol. 2018, 275, 1837–1843. [Google Scholar] [CrossRef] [PubMed]
- Masoudi, S.; Montazeri, S.A.; Pourdanesh, F.; Biglarian, A.; Kazemi, M.; Rahgozar, M. A New Approach to Survival Analysis of Head and Neck Squamous Cell Carcinoma. Arch. Iran. Med. 2017, 20, 503–510. [Google Scholar] [PubMed]
- Lukesova, E.; Boucek, J.; Rotnaglova, E.; Salakova, M.; Koslabova, E.; Grega, M.; Eckschlager, T.; Rihova, B.; Prochazka, B.; Klozar, J.; et al. High level of Tregs is a positive prognostic marker in patients with HPV-positive oral and oropharyngeal squamous cell carcinomas. BioMed Res. Int. 2014, 2014, 303929. [Google Scholar] [CrossRef] [PubMed]
- Xu, Q.S.; Wang, C.; Li, B.; Li, J.Z.; Mao, M.H.; Qin, L.Z.; Li, H.; Huang, X.; Han, Z.; Feng, Z. Prognostic value of pathologic grade for patients with oral squamous cell carcinoma. Oral Dis. 2018, 24, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Wen, Y.H.; Lin, H.Q.; Li, H.; Zhao, Y.; Lui, V.W.Y.; Chen, L.; Wu, X.M.; Sun, W.; Wen, W.P. Stromal interleukin-33 promotes regulatory T cell-mediated immunosuppression in head and neck squamous cell carcinoma and correlates with poor prognosis. Cancer Immunol. Immunother. 2018. [Google Scholar] [CrossRef] [PubMed]
- Oweida, A.; Hararah, M.K.; Phan, A.; Binder, D.; Bhatia, S.; Lennon, S.; Bukkapatnam, S.; Van Court, B.; Uyanga, N.; Darragh, L.; et al. Resistance to Radiotherapy and PD-L1 Blockade Is Mediated by TIM-3 Upregulation and Regulatory T-Cell Infiltration. Clin. Cancer Res. 2018, 24, 5368–5380. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, C.E.; Benoy, I.H.; Bailleul, E.J.; Vandepitte, J.; Vereecken, A.J.; Bogers, J.J. Improved endocervical sampling and HPV viral load detection by Cervex-Brush Combi. Cytopathology 2006, 17, 374–381. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, C.E.; Boulet, G.A.; Horvath, C.A.; Benoy, I.H.; Vereecken, A.J.; Bogers, J.J. Comparison of MY09/11 consensus PCR and type-specific PCRs in the detection of oncogenic HPV types. J. Cell. Mol. Med. 2007, 11, 881–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindt, N.; Descamps, G.; Seminerio, I.; Bellier, J.; Lechien, J.R.; Pottier, C.; Larsimont, D.; Journé, F.; Delvenne, P.; Saussez, S. Langerhans cell number is a strong and independent prognostic factor for head and neck squamous cell carcinomas. Oral Oncol. 2016, 62, 1–10. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Number of Cases (N = 205) | p Value FoxP3 in Stromal Compartment n > 63.15 = 38 n ≤ 63.15 = 164 * | p Value FoxP3 in Intra-Tumoral Compartment n > 17.2 = 119 n ≤ 17.2 = 52 * |
|---|---|---|---|
| Age (years) | |||
| Median | 61 | ||
| Range | 29–90 | ||
| Gender | 0.044 | 0.21 | |
| Male | 138 | ||
| Female | 67 | ||
| Anatomic site | 0.031 | 0.024 | |
| Oral cavity | 99 | ||
| Oropharynx | 59 | ||
| Larynx | 32 | ||
| Hypopharynx | 14 | ||
| Nasopharynx | 1 | ||
| Tumor stage | 0.497 | 0.748 | |
| T1isN0 | 1 | ||
| T1N0 | 42 | ||
| T2N0 | 31 | ||
| T1N1 | 5 | ||
| T2N1 | 8 | ||
| T3N0 | 9 | ||
| T3N1 | 4 | ||
| T1N2 | 4 | ||
| T2N2 | 16 | ||
| T3N2 | 13 | ||
| T3N3 | 1 | ||
| T4aN0 | 24 | ||
| T4aN1 | 10 | ||
| T4aN2 | 19 | ||
| T4aN3 | 1 | ||
| T4bN2 | 1 | ||
| Unknown | 16 | ||
| Histological grade (differentiation) | 0.1 | 0.806 | |
| Undifferentiated | 26 | ||
| Moderate | 69 | ||
| Well | 96 | ||
| Unknown | 14 | ||
| Tumor invasion | 0.238 | 0.649 | |
| Yes | 142 | ||
| None | 54 | ||
| Unknown | 9 | ||
| Risk factors | |||
| Tobacco | 0.768 | 0.81 | |
| Smoker | 160 | ||
| Non smoker | 35 | ||
| Unknown | 10 | ||
| Alcohol | 0.732 | 0.72 | |
| Drinker | 111 | ||
| Non drinker | 73 | ||
| Unknown | 21 | ||
| HPV status | 0.814 | 0.502 | |
| Negative | 127 | ||
| Positive | 35 | ||
| p16 status | 0.064 | 0.007 | |
| Negative | 112 | ||
| Positive | 14 | ||
| HPV/p16 status | 0.357 | 0.097 | |
| Negative | 127 | ||
| Positive, p16 negative | 24 | ||
| Positive, p16 positive | 11 | ||
| Unknown | 43 | ||
| Recurrence (RFS) | |||
| Median (months) | 23 | ||
| Range (months) | 1–245 | ||
| Yes | 98 | ||
| None | 107 | ||
| Overall survival (OS) | |||
| Median (months) | 33 | ||
| Range (months) | 1–294 | ||
| Alive | 106 | ||
| Dead | 88 |
| Variables | RFS | OS | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| Univariate analysis | ||||
| Tregs ST (>63.15 vs. <63.15) | 2.08 (1.22–3.57) | 0.007 | 2.23 (1.35–3.69) | 0.002 |
| Tregs IT (>17.2 vs. <17.2) | 1.96 (1.11–3.44) | 0.019 | 2.19 (1.21–3.98) | 0.009 |
| Gender (male vs. female) | 1.43 (0.95–2.15) | 0.084 | 1.05 (0.69–1.60) | 0.812 |
| Tumor stage (I–II vs. III–IV) | 1.42 (0.90–2.23) | 0.122 | 2.20 (1.34–3.61) | 0.002 |
| Histological grade (differentiated vs. undifferentiated) | 2.01 (1.10–3.67) | 0.022 | 1.82 (1.01–3.25) | 0.043 |
| Tumor invasion (invasion vs. no invasion) | 1.60 (0.93–2.74) | 0.086 | 1.41 (0.85–2.33) | 0.183 |
| Tobacco (smokers vs. no smokers) | 1.35 (0.77–2.36) | 0.284 | 1.30 (0.74–2.27) | 0.356 |
| Alcohol (drinkers vs. no drinkers) | 1.11 (0.72–1.72) | 0.618 | 1.15 (0.74–1.80) | 0.519 |
| HPV status (positive vs. negative) | 1.54 (0.87–2.71) | 0.131 | 1.16 (0.69–1.95) | 0.562 |
| p16 status (positive vs. negative) | 2.12 (0.76–5.91) | 0.148 | 1.86 (0.67–5.18) | 0.229 |
| Multivariate analysis | ||||
| Tregs ST (>63.15 vs. <63.15) | 2.24 (1.00–5.02) | 0.05 | 2.32 (1.17–4.58) | 0.015 |
| Tregs IT (>17.2 vs. <17.2) | 1.85 (0.94–3.64) | 0.074 | 1.79 (0.92–3.47) | 0.083 |
| Tumor stage (I–II vs. III–IV) | 3.33 (1.44–7.70) | 0.005 | 3.72 (1.59–8.73) | 0.002 |
| Histological grade (differentiated vs. undifferentiated) | 4.76 (2.00–11.36) | <0.0001 | 2.53 (1.08–5.88) | 0.031 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seminerio, I.; Descamps, G.; Dupont, S.; de Marrez, L.; Laigle, J.-A.; Lechien, J.R.; Kindt, N.; Journe, F.; Saussez, S. Infiltration of FoxP3+ Regulatory T Cells is a Strong and Independent Prognostic Factor in Head and Neck Squamous Cell Carcinoma. Cancers 2019, 11, 227. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11020227
Seminerio I, Descamps G, Dupont S, de Marrez L, Laigle J-A, Lechien JR, Kindt N, Journe F, Saussez S. Infiltration of FoxP3+ Regulatory T Cells is a Strong and Independent Prognostic Factor in Head and Neck Squamous Cell Carcinoma. Cancers. 2019; 11(2):227. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11020227
Chicago/Turabian StyleSeminerio, Imelda, Géraldine Descamps, Sophie Dupont, Lisa de Marrez, Jean-Alexandre Laigle, Jérôme R Lechien, Nadège Kindt, Fabrice Journe, and Sven Saussez. 2019. "Infiltration of FoxP3+ Regulatory T Cells is a Strong and Independent Prognostic Factor in Head and Neck Squamous Cell Carcinoma" Cancers 11, no. 2: 227. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11020227