Comparative Effectiveness of Gemcitabine plus Nab-Paclitaxel and FOLFIRINOX in the First-Line Setting of Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Results
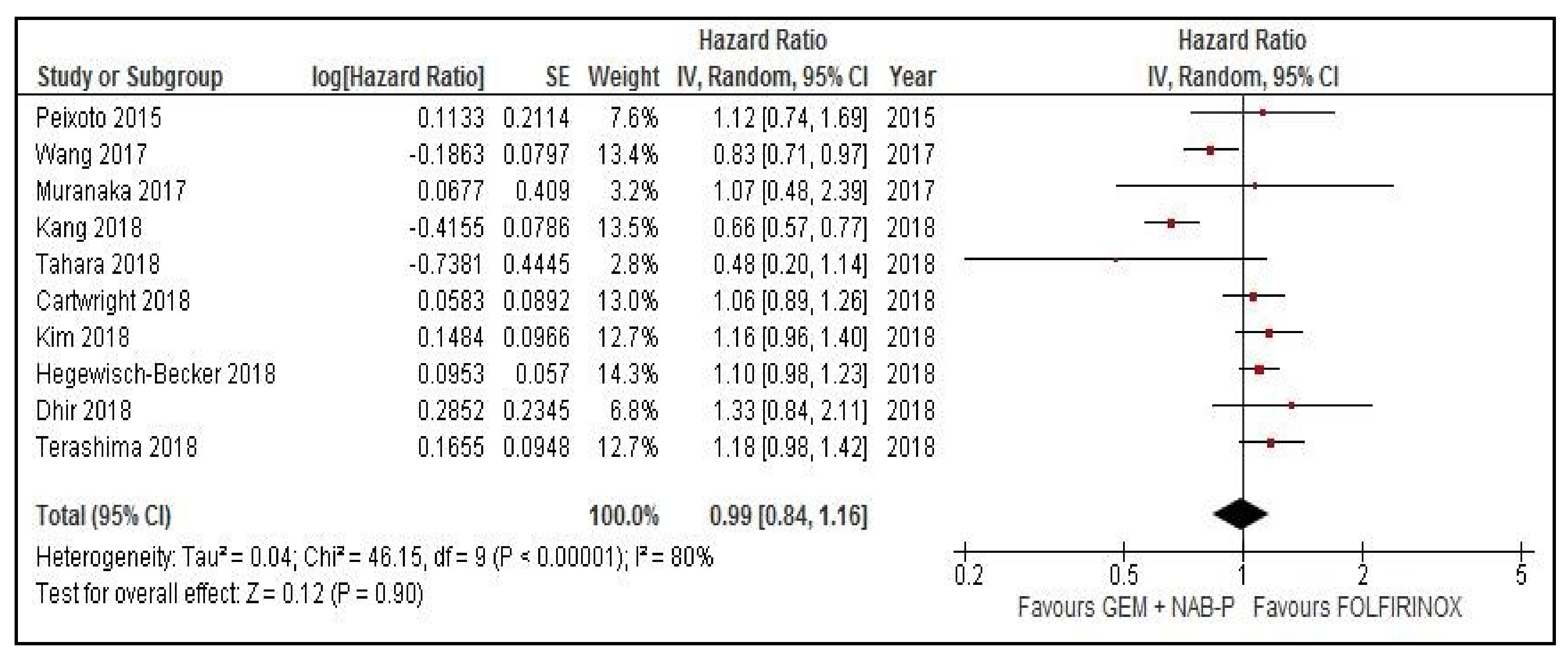
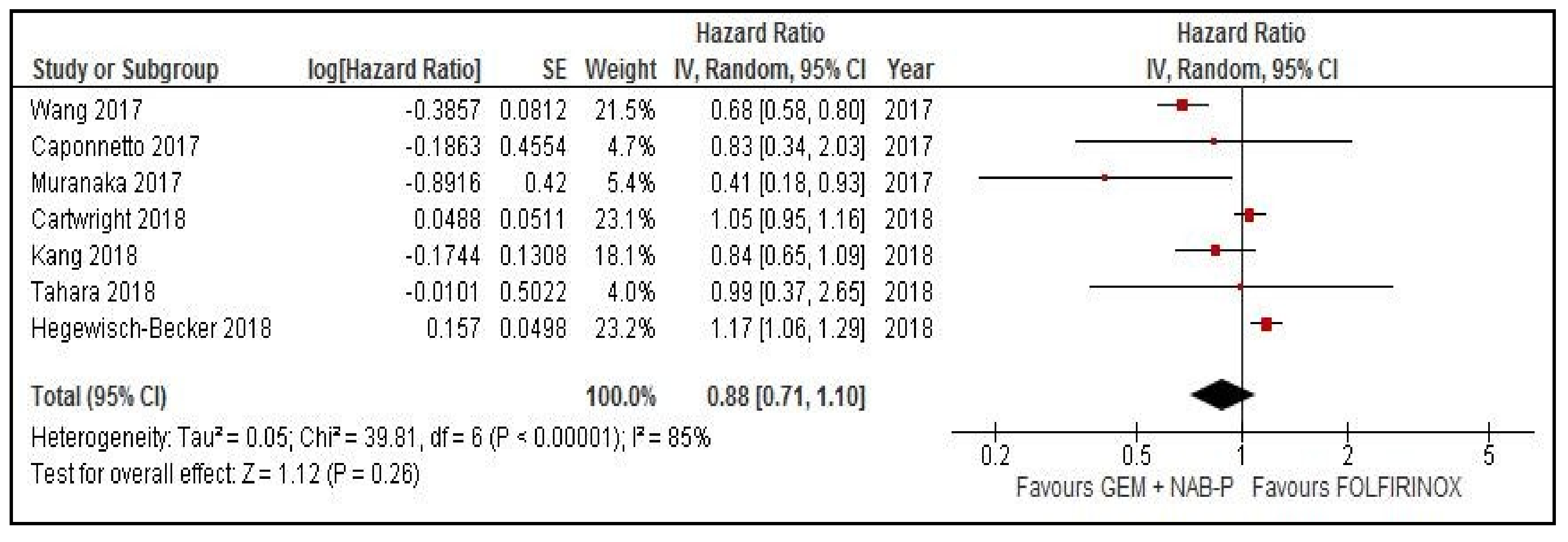
2.1. Meta-Analysis of OS and PFS
2.2. Meta-Analysis of Overall Response Rates (ORR)
2.3. Toxicities
2.4. Sensitivity Analysis
2.5. Publication Bias
3. Discussion
4. Materials and Methods
4.1. Search Strategy and Inclusion Criteria
4.2. Data Extraction and Quality Assessment
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed]
- Sohal, D.P.; Mangu, P.B.; Khorana, A.A.; Shah, M.A.; Philip, P.A.; O’Reilly, E.M.; Uronis, H.E.; Ramanathan, R.K.; Crane, C.H.; Engebretson, A.; et al. Metastatic Pancreatic Cancer: American Society of Clinical Oncology Clinical Practice Guideline. J. Clin. Oncol. 2016, 34, 2784–2796. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, S.L.; Durkal, V.; Jayavalsan, S.P.; Thomas, J.P.; Ritch, P.S.; Erickson, B.; Christians, K.K.; Tsai, S.; Evans, D.B.; George, B. Outcomes in metastatic pancreatic adenocarcinoma (MPAC) patients treated with FOLFIRINOX (FFX)/FOLFOX(FX) and gemcitabine + nab-paclitaxel (NabG). J. Clin. Oncol. 2016, 34, 397–397. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Cartwright, T.H.; Parisi, M.; Espirito, J.L.; Wilson, T.W.; Pelletier, C.; Patel, M.; Babiker, H.M. Clinical Outcomes with First-Line Chemotherapy in a Large Retrospective Study of Patients with Metastatic Pancreatic Cancer Treated in a US Community Oncology Setting. Drugs Real World Outcomes 2018, 5, 149–159. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, R.D.; Ho, M.; Renouf, D.J.; Lim, H.J.; Gill, S.; Ruan, J.Y.; Cheung, W.Y. Eligibility of Metastatic Pancreatic Cancer Patients for First-Line Palliative Intent nab-Paclitaxel Plus Gemcitabine Versus FOLFIRINOX. Am. J. Clin. Oncol. 2017, 40, 507–511. [Google Scholar] [CrossRef]
- Kang, J.; Hwang, I.; Yoo, C.; Kim, K.P.; Jeong, J.H.; Chang, H.M.; Lee, S.S.; Park, D.H.; Song, T.J.; Seo, D.W.; et al. Nab-paclitaxel plus gemcitabine versus FOLFIRINOX as the first-line chemotherapy for patients with metastatic pancreatic cancer: Retrospective analysis. Invest. New Drugs 2018, 36, 732–741. [Google Scholar] [CrossRef]
- Braiteh, F.; Patel, M.B.; Parisi, M.; Ni, Q.; Park, S.; Faria, C. Comparative effectiveness and resource utilization of nab-paclitaxel plus gemcitabine vs. FOLFIRINOX or gemcitabine for the first-line treatment of metastatic pancreatic adenocarcinoma in a US community setting. Cancer Manag. Res. 2017, 9, 141–148. [Google Scholar] [CrossRef]
- Dhir, M.; Zenati, M.S.; Hamad, A.; Singhi, A.D.; Bahary, N.; Hogg, M.E.; Zeh, H.J., 3rd; Zureikat, A.H. FOLFIRINOX Versus Gemcitabine/Nab-Paclitaxel for Neoadjuvant Treatment of Resectable and Borderline Resectable Pancreatic Head Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 1896–1903. [Google Scholar] [CrossRef]
- Hegewisch-Becker, S.; Aldaoud, A.; Wolf, T.; Krammer-Steiner, B.; Linde, H.; Scheiner-Sparna, R.; Hamm, D.; Janicke, M.; Marschner, N.; TPK-Group. Results from the prospective German TPK clinical cohort study: Treatment algorithms and survival of 1174 patients with locally advanced, inoperable, or metastatic pancreatic ductal adenocarcinoma. Int. J. Cancer 2019, 144, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Signorovitch, J.E.; Yang, H.; Patterson-Lomba, O.; Xiang, C.Q.; Ung, B.; Parisi, M.; Marshall, J.L. Comparative Effectiveness of nab-Paclitaxel Plus Gemcitabine vs. FOLFIRINOX in Metastatic Pancreatic Cancer: A Retrospective Nationwide Chart Review in the United States. Adv. Ther. 2018, 35, 1564–1577. [Google Scholar] [CrossRef] [PubMed]
- Muranaka, T.; Kuwatani, M.; Komatsu, Y.; Sawada, K.; Nakatsumi, H.; Kawamoto, Y.; Yuki, S.; Kubota, Y.; Kubo, K.; Kawahata, S.; et al. Comparison of efficacy and toxicity of FOLFIRINOX and gemcitabine with nab-paclitaxel in unresectable pancreatic cancer. J. Gastrointest. Oncol. 2017, 8, 566–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tahara, J.; Shimizu, K.; Otsuka, N.; Akao, J.; Takayama, Y.; Tokushige, K. Gemcitabine plus nab-paclitaxel vs. FOLFIRINOX for patients with advanced pancreatic cancer. Cancer Chemother. Pharmacol. 2018, 82, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Terashima, T.; Yamashita, T.; Sakai, A.; Ohta, H.; Hinoue, Y.; Toya, D.; Kawai, H.; Yonejima, M.; Urabe, T.; Noda, Y.; et al. Treatment patterns and outcomes of unresectable pancreatic cancer patients in real-life practice: A region-wide analysis. Jpn. J. Clin. Oncol. 2018, 48, 966–973. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Camateros, P.; Cheung, W.Y. A Real-World Comparison of FOLFIRINOX, Gemcitabine Plus nab-Paclitaxel, and Gemcitabine in Advanced Pancreatic Cancers. J. Gastrointest. Cancer 2017, 50, 62–68. [Google Scholar] [CrossRef] [PubMed]
- Caponnetto, S.; Gelibter, A.; Mosillo, C.; Magri, V.; Scagnoli, S.; Pomati, G.; Piesco, G.; Verkhovskaya, S.; Pisegna, S.; Sirgiovanni, G.; et al. D27Comparative effects of Folfirinox and Gemcitabine/nab-paclitaxel as first and second line chemotherapy for metastatic pancreatic cancer: Single choice or sequence. Ann. Oncol. 2017, 28, mdx425.026. [Google Scholar] [CrossRef]
- Cho, I.; Kang, H.; Jo, J.; Lee, H.; Chung, M.; Park, J.; Park, S.; Song, S.; Park, M.; An, C.; et al. P-161FOLFIRINOX versus gemcitabine plus nab-paclitaxel for treatment of metastatic pancreatic cancer: A single-center cohort study. Ann. Oncol. 2018, 29, mdy151.160. [Google Scholar] [CrossRef]
- Kasi, A.; Middinti, A.; Cao, A.; Vekaria, P.; Patel, D.; Subramaniam, D.; Chen, G.J.; Saeed, A.M.; Paluri, R.K. FOLFIRINOX versus gemcitabine nab-paclitaxel for advanced pancreatic cancer: KU Cancer Center experience. J. Clin. Oncol. 2017, 35, e15744. [Google Scholar] [CrossRef]
- Yamamoto, S.; Ueno, H.; Tanaka, M.; Inagaki, Y.; Ohba, A.; Sakamoto, Y.; Kondo, S.; Morizane, C.; Okusaka, T. O2-16-6Comparative effectiveness of gemcitabine vs. gemcitabine + nab-paclitaxel vs. FOLFIRINOX for unresectable pancreatic cancer. Ann. Oncol. 2017, 28, mdx697.062. [Google Scholar] [CrossRef]
- Gresham, G.K.; Wells, G.A.; Gill, S.; Cameron, C.; Jonker, D.J. Chemotherapy regimens for advanced pancreatic cancer: A systematic review and network meta-analysis. BMC Cancer 2014, 14, 471. [Google Scholar] [CrossRef] [PubMed]
- Tong, H.; Fan, Z.; Liu, B.; Lu, T. The benefits of modified FOLFIRINOX for advanced pancreatic cancer and its induced adverse events: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 8666. [Google Scholar] [CrossRef] [PubMed]
- Petrelli, F.; Coinu, A.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Lonati, V.; Aitini, E.; Barni, S.; Gruppo Italiano per lo Studio dei Carcinomi dell’Apparato Digerente (GISCAD). FOLFIRINOX-based neoadjuvant therapy in borderline resectable or unresectable pancreatic cancer: A meta-analytical review of published studies. Pancreas 2015, 44, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Conroy, T.; Hammel, P.; Hebbar, M.; Ben Abdelghani, M.; Wei, A.C.; Raoul, J.L.; Chone, L.; Francois, E.; Artru, P.; Biagi, J.J.; et al. FOLFIRINOX or Gemcitabine as Adjuvant Therapy for Pancreatic Cancer. N. Engl. J. Med. 2018, 379, 2395–2406. [Google Scholar] [CrossRef] [PubMed]
- Chung, M.J.; Kang, H.; Kim, H.G.; Hyun, J.J.; Lee, J.K.; Lee, K.H.; Noh, M.H.; Kang, D.H.; Lee, S.H.; Bang, S.; et al. Multicenter phase II trial of modified FOLFIRINOX in gemcitabine-refractory pancreatic cancer. World J. Gastrointest. Oncol. 2018, 10, 505–515. [Google Scholar] [CrossRef]
- Tempero, M.A.; Cardin, D.B.; Goldstein, D.; O’Reilly, E.M.; Philip, P.A.; Riess, H.; Macarulla, T.; Yung, L.; Li, M.; Lu, B.D.; et al. APACT: Phase III randomized trial of adjuvant treatment with nab-paclitaxel (nab-P) plus gemcitabine (Gem) versus Gem alone in patients (pts) with resected pancreatic cancer (PC). J. Clin. Oncol. 2016, 34, TPS473. [Google Scholar] [CrossRef]
- Hammel, P.; Lacy, J.; Portales, F.; Sobrero, A.F.; Cid, R.A.P.; Mozo, J.L.M.; Terrebonne, E.; Dowden, S.D.; Li, J.S.; Ong, T.J.; et al. Phase II LAPACT trial of nab-paclitaxel (nab-P) plus gemcitabine (G) for patients with locally advanced pancreatic cancer (LAPC). J. Clin. Oncol. 2018, 36, 204. [Google Scholar] [CrossRef]
- McBride, A.; Bonafede, M.; Cai, Q.; Princic, N.; Tran, O.; Pelletier, C.; Parisi, M.; Patel, M. Comparison of treatment patterns and economic outcomes among metastatic pancreatic cancer patients initiated on nab-paclitaxel plus gemcitabine versus FOLFIRINOX. Expert Rev. Clin. Pharmacol. 2017, 10, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.P.; Parisi, M.F.; Patel, M.B.; Pelletier, C.L.; Belk, K.W. Comparison of treatment patterns, resource utilization, and cost of care in patients with metastatic pancreatic cancer treated with first-line nab-paclitaxel plus gemcitabine or FOLFIRINOX. Expert Rev. Clin. Pharmacol. 2017, 10, 559–565. [Google Scholar] [CrossRef]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef]
- Stang, A. Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur. J. Epidemiol. 2010, 25, 603–605. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Author/Year | N° pts | Country | Type of Study | Follow up (Months) | PS 0–1% GN/F | Median Age GN/F (Years) | Stage (LAD/Metastatic) GN vs. F | Abnormal Bilirubin % GN vs. F | Liver Metastases % GN vs. F | Location(Head) GN vs. F | CA 19.9 (Median) GN vs. F | Biliary Stent % GN vs. F |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Braiteh 2017 [9] | 202 | USA | Retrospective | - | 82 vs. 82 | 69/61.5 | 0/88 vs. 0/89 | - | 64 vs. 73 | - | 48 vs. 37 | - |
| Dhir 2018 [10] | 193 | USA | Retrospective | 27.5 | - | 69/63 | 59.2 vs. 79.4/0 vs. 0 | - | - | - | 235 vs 243 | - |
| Cartwright 2018 [6] | 314 | USA | Retrospective | - | 76.8/90.5 | 68/61 | 0/100 vs. 0/100 | - | 33.1 vs. 33.5 | - | - | - |
| Kang 2018 [8] | 308 | Korea | Retrospective | 19.6 | 96.6/99. 4 | 62/60 | 0/100 vs. 0/100 | - | 61.1 vs. 67.9 | 32.2 vs. 39.7 | 443 vs. 576 | - |
| Hegewisch-Becker 2018 [11] | 773 | Germany | Retrospective | - | 89.6 vs. 95.8 | 71/60 | -/89 vs. 90 | 9.8 vs. 7.4 | - | 52.4 vs. 52.5 | - | - |
| Kim 2018 [12] | 654 | USA | Retrospective | 9 | 70.3 vs. 91.5 | 64.59/59.03 | 0/100 vs. 100 | - | 75.34 vs. 75.73 | 50.5 vs. 51.3 | - | - |
| Muranaka 2017 [13] | 38 | Japan | Retrospective | 11.9–8.3 (F-GN) | 100 vs. 100 | 66.5/63 | 13.6 vs. 43.8/86.4 vs. 56.2 | - | - | - | 305.6 vs. 128.7 | 9.1 vs. 18.8 |
| Peixoto 2015 [7] | 331 | Canada | Retrospective | - | - | - | - | - | - | - | - | - |
| Tahara 2018 [14] | 27 | Japan | Retrospective | - | 100/100 | 63 vs. 62 | - | 0 vs. 0 | 26.6 vs. 16.6 | 66.6 vs. 50 | - | - |
| Terashima 2018 [15] | 67 | Japan | Retrospective | 5.6 | - vs. 85.1 | - | - | - | - | - | - | - |
| Wang 2017 [16] | 179 | Canada | Retrospective | 8.5 | 59/93 | 68/60 | -/75.9 vs. 59.8 | 10 vs. 10 | 34.8 vs. 30.1 | 48.3 vs. 67.4 | 1228 vs. 415 | 20.7 vs. 32.6 |
| Caponnetto 2017 [17] | 43 | Italy | Retrospective | - | 100/100 | - | 0/100 vs. 0/100 | - | - | - | - | - |
| Cho 2018 [18] | 167 | Korea | Cohort study | 7.9 | - | 65/54 | 0/100 vs. 0/100 | - | - | - | - | - |
| Kasi 2017 [19] | 154 | US | Retrospective | - | 83/90 | 63/61 | 30/70 vs. 48/52 | - | - | 55 vs. 63 | - | 20/41 |
| Schmidt 2016 [3] | 56 | US | Retrospective | - | - | - | 100/100 | - | - | - | - | - |
| Yamamoto 2017 [20] | 207 | Japan | Retrospective | - | - | - | - | - | - | - | - | - |
| Toxicity G 3–4 GEM-NAB vs. FOLFIRINOX | N° Studies | Pooled Effect (OR, 95% CI) | I2 (%) | Analysis Model | p |
|---|---|---|---|---|---|
| Hematologic | |||||
| Neutropenia | 8 | 0.71 (0.54–0.92) | 0 | Fixed | 0.01 * |
| FN | 5 | 0.45 (0.29–0.7) | 0 | Fixed | <0.001 * |
| Anemia | 7 | 2.5 (1.5–4.3) | 0 | Fixed | <0.001 * |
| Thrombocytopenia | 6 | 0.89 (0.37–2.1) | 0 | Random | 0.79 |
| Non-hematologic | |||||
| Stomatitis | NA | ||||
| Diarrhea | 5 | 0.27 (0.03–2.2) | 0 | Fixed | 0.23 |
| Nausea | 2 | 0.11 (0.03–0.34) | 0 | Fixed | <0.001 * |
| Vomiting | 2 | 0.76 (0.03–19.5) | 0 | Fixed | 0.87 |
| Anorexia | 2 | 0.41 (0.05–3.2) | 0 | Fixed | 0.4 |
| Fatigue | 2 | 1 (0.2–4.9) | 0 | Fixed | 1 |
| Neurotoxicity | 5 | 2.8 (1.4–5.7) | 31.9 | Fixed | 0.027 * |
| Infections/sepsis | NA | ||||
| ALT increase | NA° | ||||
| AST increase | NA° | ||||
| Toxic deaths | NA° | ||||
| Thrombosis | NA | ||||
| Dose reduction | 4 | 0.81 (0.46–1.4) | 69.9 | Random | 0.45 |
| Discontinuations | 2 | 1.26 (0.23–6.87) | 79.3 | Random | 0.78 |
| Median cycle | 3 | 3 vs. 5.4 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pusceddu, S.; Ghidini, M.; Torchio, M.; Corti, F.; Tomasello, G.; Niger, M.; Prinzi, N.; Nichetti, F.; Coinu, A.; Di Bartolomeo, M.; et al. Comparative Effectiveness of Gemcitabine plus Nab-Paclitaxel and FOLFIRINOX in the First-Line Setting of Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis. Cancers 2019, 11, 484. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11040484
Pusceddu S, Ghidini M, Torchio M, Corti F, Tomasello G, Niger M, Prinzi N, Nichetti F, Coinu A, Di Bartolomeo M, et al. Comparative Effectiveness of Gemcitabine plus Nab-Paclitaxel and FOLFIRINOX in the First-Line Setting of Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis. Cancers. 2019; 11(4):484. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11040484
Chicago/Turabian StylePusceddu, Sara, Michele Ghidini, Martina Torchio, Francesca Corti, Gianluca Tomasello, Monica Niger, Natalie Prinzi, Federico Nichetti, Andrea Coinu, Maria Di Bartolomeo, and et al. 2019. "Comparative Effectiveness of Gemcitabine plus Nab-Paclitaxel and FOLFIRINOX in the First-Line Setting of Metastatic Pancreatic Cancer: A Systematic Review and Meta-Analysis" Cancers 11, no. 4: 484. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11040484