Fibroblasts as Modulators of Local and Systemic Cancer Metabolism

1
Department of Cell, Developmental & Cancer Biology, Oregon Health & Science University, Portland, OR 97201, USA
2
Knight Cancer Institute, Oregon Health & Science University, Portland, OR 97201, USA
*
Author to whom correspondence should be addressed.
†
Co-first authors.
Cancers 2019, 11(5), 619; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050619
Submission received: 8 April 2019
/
Revised: 30 April 2019
/
Accepted: 1 May 2019
/
Published: 3 May 2019
(This article belongs to the Special Issue Metabolic Reprogramming and Vulnerabilities in Cancer)
{kind=link}
{kind=link}
Abstract
:Fibroblast activation is an accompanying feature of solid tumor progression, resembling a conserved host response to tissue damage. Cancer-associated fibroblasts (CAFs) comprise a heterogeneous and plastic population with increasingly appreciated roles in tumor growth, metastatic capacity, and response to therapy. Classical features of fibroblasts in a wound-healing response, including profound extracellular matrix production and cytokine release, are recapitulated in cancer. Emerging evidence suggests that fibroblastic cells in the microenvironments of solid tumors also critically modulate cellular metabolism in the neoplastic compartment through mechanisms including paracrine transfer of metabolites or non-cell-autonomous regulation of metabolic signaling pathways. These metabolic functions may represent common mechanisms by which fibroblasts stimulate growth of the regenerating epithelium during a wound-healing reaction, or may reflect unique co-evolution of cancer cells and surrounding stroma within the tumor microenvironment. Here we review the recent literature supporting an important role for CAFs in regulation of cancer cell metabolism, and relevant pathways that may serve as targets for therapeutic intervention.
1. Introduction
The increasingly appreciated role of activated fibroblasts in cancer progression and response to therapy [1] has prompted investigation of growth-permissive fibroblast functions in cancer. Cancer-associated fibroblasts (CAFs) derived from activated resident fibroblast pools or from mesenchymal progenitors recruited to the tumor microenvironment [2,3,4] have displayed diverse pro-tumorigenic functions that cooperate with cell-autonomous mechanisms to promote the hallmarks of cancer [5]. While CAF functional diversity is increasingly appreciated across tissue sites [6,7,8] and precise functions may vary in a tissue-specific manner, CAFs have conserved and well-documented roles in establishing key components of a wound-healing reaction in solid tumor tissues. While fibroblastic cells evolved to play roles in tissue homeostasis and wound healing, CAFs reflect both the classical role of fibroblasts in tissue biology and unique roles resulting from co-evolution with neoplastic growths. CAFs are typically abundant in solid tumors [9], and are the principal producers of extracellular matrix (ECM) components and remodeling enzymes [10]. In addition, CAFs secrete numerous signaling proteins including mitogenic growth factors that can stimulate proliferation in the epithelial compartment [1], as well as pro-inflammatory mediators that can modulate intratumoral immune infiltration [7,11,12,13]. These established CAF functions resemble those of activated fibroblasts to support regeneration and repair. More recently, however, evidence has emerged to support a critical role for CAFs as regulators of critical metabolic processes in cancer [14]. These metabolic roles may be specific to fibroblastic cells in tumor microenvironments, as adaptive mechanisms to support the metabolic demands of rapidly proliferating cancer cells. Supporting this connection, recent analysis of metabolic networks in human breast cancer in situ showed significant correlation of intracellular metabolic states of cancer cells and adjacent CAFs [15], and mechanistic studies are beginning to uncover the importance of this bioenergetic coupling of tumor and stroma. Below, we discuss the emerging roles of CAFs in regulation of cellular and organismal metabolism in cancer.
2. Wound-Healing Mediators as Metabolic Regulators
As critical regulators of the wound-healing reaction, activated fibroblasts are key producers of soluble secreted factors such as cytokines, growth factors, and ECM components that orchestrate wounding-associated inflammation, regeneration, and tissue repair. CAFs similarly produce classical wound-healing mediators, and emerging evidence suggests that beyond their long-appreciated roles in repair processes, these factors also regulate metabolic functions of neighboring cancer cells. Among solid tumors, pancreatic ductal adenocarcinoma (PDAC) has a particularly prominent stromal compartment, characterized in part by a prominent CAF population and a dense, collagen-rich ECM [16]. This ECM has been shown to restrict vascular perfusion in the PDAC tumor microenvironment (TME) [17,18], and perhaps due to low serum availability, the PDAC milieu is nutrient-poor [19]. Under conditions of low nutrients, mutant KRAS, a main oncogene of PDAC, is able to drive macropinocytosis as a source of amino acids from extracellular proteins for the cancer cells [20]. Recent work has shown that the abundant, CAF-derived collagen in the PDAC ECM can serve as an extracellular protein source, and one particularly rich in prolines (25% of the amino acids in collagen) [21]. PDAC cells can take up collagen fragments, through macropinocytosis-dependent and -independent mechanisms, and subsequently metabolize proline via proline oxidase (POX/PRODH1) to fuel the TCA cycle and promote proliferation and survival under nutrient-restricted conditions in vitro or during tumor growth in vivo. Consistent with this study, soluble CAF-derived proteins together with 3D type I collagen induce transcriptional and metabolic alterations in PDAC cells supporting anabolic programs, which overlaps significantly with networks regulated by oncogenic KRAS and suggests points of convergence between cell-intrinsic and microenvironmental mechanisms that regulate cancer cell metabolism [22]. CAF-derived cytokines including CCL5, IL6, and CXCL10 can also regulate cancer cell metabolism by promoting phosphorylation of phosphoglucomutase 1 and increasing glycogen mobilization in cancer cells, promoting NADPH synthesis and the TCA cycle and thus enabling cancer cell proliferation and metastatic spread of ovarian cancer cells [23] (Figure 1).
Beyond uptake, ECM components produced by CAFs also regulate cancer cell metabolism via activation of diverse signaling mechanisms. In addition to collagens, CAFs also produce and secrete high levels of hyaluronan (HA), as well as enzymes that break down and remodel the ECM. A recent study demonstrated that HA fragments can signal through receptor tyrosine kinases to induce ZFP36, causing degradation of TXNIP transcripts and subsequently blocking TXNIP-mediated internalization of glucose transporter GLUT1 [24]. This leads to an increase of GLUT1 transporter on the plasma membrane, increasing the amount of glucose transport, and inducing glycolysis within the cancer cell. ECM signals act on TXNIP for acute and protracted regulation of glucose uptake, showing that external cues can regulate cellular metabolism and migration. Increased ECM stiffness during tumor progression and downstream mechanosensing induces CAFs to release aspartate, supporting cancer cell proliferation, while cancer cells in turn secrete glutamate and balance the redox state of CAFs to further promote ECM remodeling [25]. A stiff ECM mechanoactivates the YAP/TAZ pathway which plays a central role in cell proliferation, survival, and polarity, especially in tumor cells. Mechanostimuli of the ECM is thus linked to tumor cell metabolism, while tumor cell metabolism is linked to responses by the CAFs to increase ECM stiffness, resulting in a positive feedback between CAFs and cancer cells. While ECM stiffness and poor perfusion can reduce drug delivery and promote chemoresistance, CAFs can also promote chemoresistance through the release of glutathione and cysteine [26]. Glutathione and cysteine are released by CAFs leading to increased GSH levels in cancer cells, and to a reduction of platinum accumulation in cells treated with platinum-based therapies. Interestingly, CD8 T cells reverse this chemoresistance mechanism through release of interferon-gamma, which causes upregulation of gamma-glutamyltransferase activity in CAFs and to transcriptional repression of system xc- cystine and glutamate antiporter via JAK/STAT signaling.
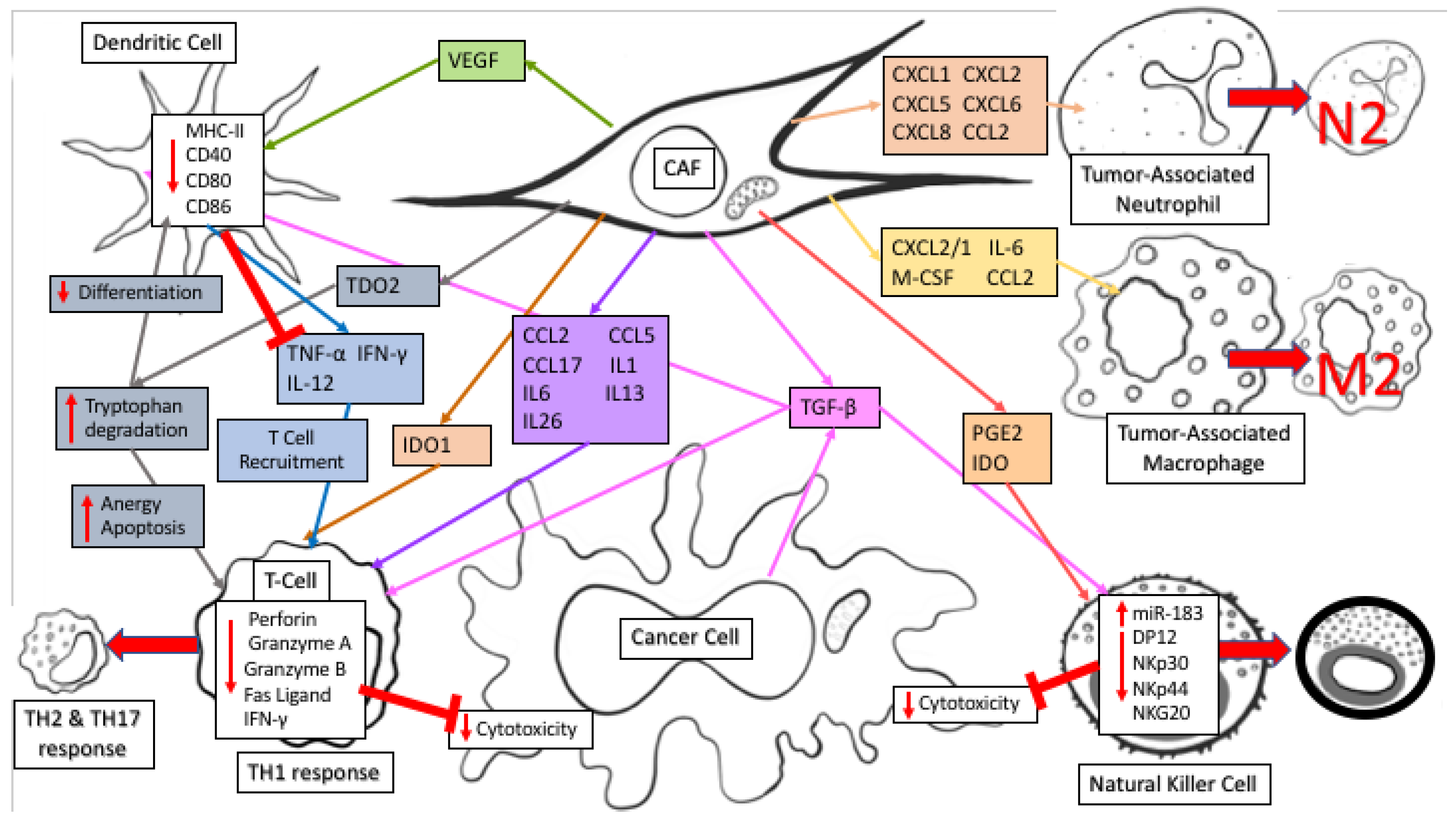
CAFs regulate the anti-tumor immune response through secretion of numerous immunomodulatory factors (reviewed in reference [27]). Fibroblasts secrete similar factors as part of the wound-healing response to recruit immune factors to an injury, however during cancer progression CAF secreted factors generally have an immune-suppressive function. The immune cells regulated by CAFs can in turn impact cancer cell metabolism, highlighting the complexity of metabolic regulation within an intact TME. CAF secretion of CXCL12/SDF1, M-CSF/CSF-1, IL-6, and CCL2/MCP-1 recruits tumor-associated macrophages (TAM) to the TME and actively differentiates TAMs into an M2 immunosuppressive phenotype. In addition, CAF secretion of CXCL1, CXCL2, CXCL5, CXCL6, CXCL8, and CCL2 recruits tumor-associated neutrophils (TANs) to the TME and polarizes them to an N2 pro-tumoral phenotype. TGF-β, secreted by CAFs, induces miR-183 to inhibit DAP12 transcription and results in reduced natural killer (NK) activating receptors (NKp30, NKp44, NKG2D) on the NK cell surface. Along with its impact on NK cells, TGF-β also causes dendritic cells (DC) to downregulate MHC class II expression, along with CD40, CD80, and CD86 leading to decreased antigen presentation efficiency and decreased production of TNF-α, IFN-γ, and IL-12, ultimately causing a reduction in T cell recruitment and survival in the TME. PGE2 and IDO secretion by CAFs affects NK cells by decreasing their cytotoxicity against cancer cells [28]. In lung cancer, TDO2 secretion by CAFs promotes tryptophan metabolism to kynurenines (Kyn), inhibiting DC differentiation while VEGF secretion inhibits DC generation and maturation by reducing MHC class II expression and antigen presenting abilities [29]. TGF-β promotes cell death of CD8+ T cells by inhibiting expression of the pro-survival factor Bcl-2. IDO1 secretion further damages T cell response by catabolizing tryptophan degradation into Kyn, creating an immunosuppressive TME and causing T cell anergy and apoptosis through depletion of tryptophan combined with an accumulation of immunosuppressive tryptophan catabolites. CD4+ helper T lymphocytes react to CAF secretion of CCL2, CCL5, and CCL17 along with polarizing cytokines IL-1, IL-6, IL-13, and IL-26 by switching from an anti-tumor TH1 response to a pro-tumor TH2 and TH17 response. CAFs secrete immunomodulatory factors that regulate the immune response within the tumor niche by creating an immunosuppressive environment which decreases the antigen presenting capabilities of NKs and DCs while simultaneously decreasing cytotoxicity and survival of T cells. Together, these immunomodulatory functions of CAFs can profoundly impact cancer metabolism, and regulate cancer progression through both immune effector and metabolic mechanisms.
Aging adds another variable to the impact of the TME on cancer development. The effect of age on the TME is so significant that genetically identical cells can have varying metastasis levels and therapy response based on whether they are in an aged TME or young TME, suggesting that the aged TME is capable of profoundly influencing cancer cell behavior [30]. Indeed, aged fibroblasts secrete sFRP2, a Wnt antagonist, which causes a downstream cascade of signals and subsequent loss of β-catenin and MITF, as well as redox effector APE1. This loss of APE1 makes melanoma cells less responsive to ROS-induced DNA damage and causes an increase in targeted therapy resistance. sFRP2-induced β-catenin loss promotes invasion and causes increases in ROS, which has been linked to BRAF inhibitor resistance, suggesting that aged patients could benefit from anti-oxidant therapy more than younger patients. The TME is a complicated, unique aspect of cancer which warrants consideration for personalized oncology wherein age, genetics, and tumor mutational load are combined to generate the ideal cancer treatment plan. While much previous research into cancer has focused on genetic modifications and oncogenes, such as KRAS, it has become increasingly clear that a dynamic ECM and TME co-evolving with tumor cells may have a profound effect on proliferation, immune evasion, and metastasis together with the underlying genetic mutations which support tumor initiation. Though tissue-specific aspects of CAF-cancer cell interaction have been reported, other tumor-stroma effects are seen across cancer types and relate to conserved features of a wound-healing response, suggesting a potential avenue for stroma-directed and broadly applicable anticancer therapies.
3. A Role for Fibroblast-Derived Metabolites in Tumor-Stroma Interaction
Upon activation, quiescent fibroblasts undergo transcriptomic and metabolic programming that mimics the “Warburg Effect” metabolic phenotype, which is further exaggerated in the hypoxic TME [1,31,32] (Figure 2). The hypoxia response is a universally conserved response to insufficient oxygen availability wherein the hypoxia-inducible factor (HIF) complex is stabilized and transported to hypoxia response element (HRE) promoter sequences to engage in transcription of over 100 genes, many of which are directly involved in increasing anaerobic glycolysis rate [33]. Competition for glucose between CAFs and cancer cells seems counterproductive for tumorigenesis. Instead there are several lines of evidence suggesting metabolic reprogramming to coordinate glucose and lactate metabolism in the TME. Metabolic tracing experiments have shown that well-oxygenated cancer cells support high glycolysis rate of cells in hypoxia by increasing lactate uptake [34,35]. This is further validated by differential expression of monocarboxylate transporters (MCT) with cells experiencing hypoxia increasing MCT4 levels, lactate efflux, and cells in normoxia increasing MCT1 for lactate import [34,35]. In the context of tumor metabolism, this phenomenon has been dubbed as the “Reverse Warburg Effect,” from the perspective of cancer cells reacting to metabolic reprogramming in CAFs [36]. This observation was first made in genetic analyses of breast cancer CAFs that exhibited low caveolin-1 (CAV1) expression [37]. Upon knockout of CAV1, fibroblasts gained myofibroblastic markers and increased rate of aerobic glycolysis [37]. Further analysis demonstrated that the metabolic program of CAFs in breast cancer is supported by cancer cells’ increased lactate uptake to support their own bioenergetic needs [37,38]. The same metabolic reprogramming has been shown in prostate cancer CAFs upon direct contact with cancer cells in co-culture studies [39]. The “Warburg Effect” in CAFs is also exhibited through classic fibroblast activators, TGF-β and PDGF, which have been shown to downregulate isocitrate dehydrogenase (IDH) expression resulting in decreased of cellular levels of α-ketogluterate (α-KG), due to impaired isocitrate to α-KG conversion [40]. α-KG and oxygen are critical co-factors for PHD enzymes, which negatively regulate stability of glycolysis master regulator HIF1α by promoting its ubiquitin-mediated proteosome degradation in normoxia [40,41]. Moreover, TGF-β signaling in CAFs has been shown to trigger increased oxidative stress, autophagy/mitophagy, and aerobic glycolysis—all known factors enhancing HIF1α stability [42,43]. The “Reverse Warburg Effect” does not reflect all metabolic crosstalk across fibrotic tumors as evidenced by studies in breast and pancreatic cancer showing CAFs increasing lactate uptake and re-purposing it for bioenergetics [44,45]. In turn, clearance of lactate by CAFs enhances higher glycolysis rate in cancer cells. It is not clear why well-oxygenated cancer cells will switch to lactate in preference of glucose, but these observations showing the “Reverse Warburg Effect” seem to conform with the concept of metabolic symbiosis required for tumor progression wherein CAFs’ ability to support cancer cell metabolism through glycolysis byproducts is necessary for tumor formation.
Upon malignant transformation, cancer cells become increasingly dependent on an exogenous supply of amino acids, especially glutamine, the most abundant amino acid in plasma [46]. In ovarian cancer, CAFs have been shown to harness carbon and nitrogen from aspartate, asparagine, and lactate to generate glutamine [47]. Thus, through upregulation of anapleurotic glutamine metabolism CAFs are able to support glutamine-addicted cancer cells in the glutamine-starved TME. This relationship was shown by blocking expression of glutamate ammonia ligase, thereby impairing CAF ability to provide glutamine to cancer cells, which hindered tumor growth [47]. A similar effect was achieved by blocking glutamine catabolism through genetic ablation of glutamate synthase. Combining the effects of inhibiting glutamine synthesis in CAFs and glutamine catabolism in cancer cells prevented formation and metastasis of ovarian cancer. In the nutrient-poor PDAC TME, alanine derived from autophagic CAFs is utilized by pancreatic cancer cells as a carbon source to fuel bioenergetic and biosynthetic processes, compensating for low levels of glucose/glutamine in the TME [44]. Moreover, through the provision of alanine, CAFs further enhance carcinogenesis by allowing cancer cells to fuel TCA cycle, support lipid and NEAA synthesis, as well as diverting glucose metabolism to serine and glycine synthesis both of which are essential for cancer cell survival [44,48]. In contrast to autophagy activation in pancreatic cancer, genetic analyses of prostate and liver tumor stroma shows a decrease of autophagy substrate signaling adaptor protein, p62, resulting in defective autophagy [49,50]. p62 depletion increases expression of ATF4, targeted for ubiquitin-mediated proteasomal degradation in normal fibroblasts with normal expression of p62 [51]. ATF4-positive CAFs support neoplastic cell growth in low glutamine conditions through activation of the pyruvate carboxylase-asparagine synthase pathway [51]. In this instance, CAF-derived asparagine supports cancer cells bioenergetics and nitrogen needs in the glutamine-poor TME. These studies reveal the significance of CAFs as regulators of TME metabolism by providing glutamine and amino acids that serve as intermediates to glutamine metabolic pathways, supporting tumor establishment and metastasis.
One of the challenges in understanding the role of CAFs in carcinogenesis is the fact that fibroblasts are found in most tissues, yet they remain poorly characterized. Interestingly, a well-known feature of particular pancreatic fibroblasts and hepatic fibroblasts, known as pancreatic and hepatic stellate cells, is their ability to store lipids in their quiescent phenotype [52]. Upon activation and during carcinogenesis, stellate cells lose their ability to store lipids, but the relevance of stromal lipid metabolism in cancer remains poorly understood. Interestingly, metabolomic studies of KRAS mutant cells experiencing hypoxia demonstrate inability to undergo de novo lipogenesis and instead show more reliance on lipid scavenging, suggesting a potential metabolic function of lipids secreted by activated fibroblasts [53]. Recently, work from our lab demonstrated that activated stellate cells secrete abundant lysophosphatidylcholines (LPC), the preferred fatty acid scavenging substrate for RAS-transformed cells, which can support PDAC cells growth both via uptake and biomass production and via hydrolysis by the secreted enzyme autotaxin to yield mitogenic lysophosphatidic acid (LPA) [54]. Reprogramming of lipid metabolism has also been demonstrated in prostate CAFs compared to normal prostate fibroblasts [55]. Prostate CAFs have elevated neutral lipid storage, and these lipid stores cooperate with pigment epithelium-derived growth factor to amplify microtubule-organizing centers. Further roles of CAF lipid secretion remain to be elucidated as several lines of evidence suggest that exogenous lipids support auxotrophic cancer cell growth [56,57].
Another little-explored aspect of CAFs is exosome-mediated metabolic crosstalk. Recent studies have shown that exosomes carry proteins, nucleic acids, miRNAs, and metabolic molecules [58]. CAF-derived exosomes, CDEs, of prostate and pancreatic cancer have been shown to reprogram metabolism of cancer cells by significantly up-regulating glycolysis while down-regulating oxidative metabolism by promoting glutamine decarboxylation and at the same time generating metabolites for de novo lipogenesis [59]. Metabolomic analysis of CDE contents reveal that they carry lactate, acetate, and amino acids—shown to be taken by cancer cells through carbon tracing analyses. Interestingly, CDE metabolic reprogramming was shown to be independent of oncogenic KRAS in pancreatic cancer, thereby demonstrating CAFs’ ability to reprogram and support cancer cell metabolism independent of oncogene activation. CDEs have been shown to enhance gemcitabine resistance in pancreatic cancer cells by enhancing proliferation and glycolysis [60]. The extent to which CDEs modulate the metabolism of cells in the TME remains to be further explored.
The TME is highly dynamic and the accessibility to oxygen and nutrients is never constant forcing cancer cells to reprogram their metabolism accordingly. The studies summarized in this section highlight the role CAFs play in sustaining tumor cell metabolism. Further studies are required to understand the way in which CAFs provide metabolic support to cancer cells in order to identify novel therapeutic avenues.
4. Fibroblasts as Determinants of Systemic Metabolism in Cancer
Beyond metabolic dysregulation in its local tissue context, cancer is associated with metabolic alterations in the host [61]. Abnormal whole-body metabolic responses to cancer include cancer cachexia, a potentially lethal wasting syndrome driven by negative energy balance and associated with loss of adipose and muscle tissue [62]. Cachexia has been mechanistically linked to the inflammatory response to cancer, and particularly to elevated levels of systemic pro-inflammatory cytokines [63]. Cachexia is a common and early event in the pathogenesis of some cancer types, and evidence of tissue breakdown associated with cachexia may even be a biomarker of early tumorigenesis [64,65]. Though mechanisms driving cancer cachexia are complex and remain to be elucidated, early evidence has emerged that CAFs may play a role in tissue wasting, in part by mediating an inflammatory response and in part through direct interactions with relevant host tissues. Fibroblast activation protein-α (FAPα) marks activated fibroblastic cells in tumors [66] and other pathologic inflammatory conditions, including atherosclerosis [67]. FAPα-positive cells in the primary tumor microenvironment have been associated with immune suppression, promoting T cell exclusion via secretion of CXCL12 [68]. However, recent work using a FAPα reporter in mice showed that these FAPα-expressing fibroblastic cells can be found in numerous tissues in the adult mouse, including skeletal muscle [69]. FAPα-positive cells across tissue contexts have similar transcriptomes, suggesting a common lineage. Depletion of FAPα-positive cells in healthy mice caused a cachexia-like syndrome, characterized by rapid weight loss and reduced muscle mass despite adequate food intake. FAPα-positive fibroblasts in skeletal muscle were shown to be the predominant source of Lama2 and Follistatin (Fst288 and Fst315), key regulators of myofiber thickness and muscle growth. Thus, loss of FAPα-positive fibroblasts from skeletal muscle was proposed to play a causal role in the muscle-wasting aspect of cachexia. Strikingly, the authors observed significant loss of FAPα-positive cells from skeletal muscle in cachectic tumor models. These findings implicate fibroblastic cells in maintenance of muscle mass, and raise the possibility that fibroblast loss from skeletal muscle promotes the muscle wasting observed in cancer cachexia, with major implications for systemic metabolism.
The host metabolic perturbations associated with cancer progression have been partly attributed to increased systemic levels of pro-inflammatory cytokines [63]. IL6 in particular has been functionally linked to cachexia [70,71,72,73,74,75,76,77], and is elevated in patients with cachexia-associated cancers [78,79,80]. Further, activation of STAT3 downstream of IL6 has been linked to muscle wasting in cancer [81]. In multiple cancer types, CAFs are reported as a significant source of IL6 in the tumor microenvironment [7,82,83,84,85], highlighting CAF-derived IL6 as a potential link to cancer cachexia. Shining light on the role of IL6 in cancer cachexia, recent work demonstrated that the elevated IL6 in cachexia-associated tumor models suppresses hepatic ketogenesis, by downregulating expression of master ketogenic regulator PPARα in the liver [70]. IL6 promoted metabolic stress in response to caloric restriction, including elevated corticosterone levels, and recombinant IL6 lowered fasting ketone and glucose levels. Interestingly, the increase in systemic glucocorticoids in response to IL6-mediated suppression of hepatic ketogenesis was associated with a suppression of anti-tumor immunity. Reduced food intake was a driver of the increase in glucocorticoids and immune suppression, and caloric deficiency is commonly seen among patients with cachexia-associated cancers. Notably, IL6 can also directly regulate the hypothalamic-pituitary-adrenal axis [86], and may further contribute to cachexia through its activity in the brain. While CAFs can function to locally suppress anti-tumor immunity, these findings raise the possibility that CAFs participate in a complex metabolic and inflammatory host response, leading to systemic elevation of glucocorticoids and immune suppression. The role of IL6 specifically derived from CAFs has yet to be tested in this axis.
While studies of the metabolic, immune-modulatory, or paracrine signaling functions of CAFs in various solid tumors suggest tumor-supportive roles for these cells, three papers published in 2014 demonstrated a protective role for CAFs in pancreatic cancer with respect to survival outcome [87,88,89]. To probe the roles of the abundant CAF population in these tumors, the authors used genetic or pharmacologic approaches to ablate CAFs during pancreatic tumorigenesis, either ablating Shh-dependent CAFs [87,89] or αSMA-positive CAFs [88]. Though these different systems yielded somewhat different results, these studies together provide compelling evidence that CAF ablation causes mice to succumb significantly earlier to the disease compared to CAF-replete controls. Interestingly, in the study by Rhim et al. employing both genetic and pharmacologic inhibition of Shh to ablate CAFs, the authors report that mice succumb with very small tumors, but with severe cachexia, including wasting of adipose tissue and muscle exceeding that seen in controls. Data are shown from systemic Shh inhibition, but the authors report that the same phenotype was observed in their genetic model which specifically targets Shh in the pancreas, and therefore specifically inhibits Shh-dependent CAFs within the local tumor microenvironment. This raises the intriguing possibility that pancreatic CAFs promote improved survival outcomes in part by inhibiting pro-cachectic mechanisms within the primary tumor. A mechanistic connection between Shh-dependent CAF function and critical mediators of cancer cachexia has not been established. However, further investigation into this axis may be warranted, as therapies targeting pancreatic CAFs would ideally leave any such cachexia-suppressive mechanisms intact.
Likely related to their evolutionary role in the wound-healing response, CAFs are important sources of growth factors in the tumor microenvironment, as discussed above. In multiple solid tumor types, CAFs have been described as significant sources of growth factor ligands for the epidermal growth factor receptor (EGFR), including high-affinity ligands betacellulin (BTC) [90] and heparin-binding EGF-like growth factor (HB-EGF) [91] as well as lower-affinity ligand epiregulin (EREG) [92]. CAFs and normal fibroblasts are also prominent producers of parathyroid hormone-related protein (PTHrP) [93,94], a developmental regulatory molecule activated by EGFR signaling [95]. A recent study aimed to identify novel regulators of cancer cachexia, and found a novel connection between factors that promote adipose tissue browning and the onset of features of cachexia including weight loss and muscle atrophy [96]. Cachexia is characterized in part by increased resting energy expenditure, which has been linked to increased thermogenesis by brown adipose tissue [97,98,99,100] and to browning of white adipose tissue [101]. Kir et al. found that Lewis lung carcinoma (LLC) cells induce adipose tissue browning and cachexia. By comparing gene expression in more thermogenic versus less thermogenic clones, they identified candidate paracrine thermogenic regulators. By testing candidate recombinant proteins, the authors found that the 3 EGFR ligands discussed above—BTC, HB-EGF, and EREG—as well as PTHrP all stimulate thermogenic gene expression in primary adipocytes. Though the study focused on cancer cell-derived PTHrP as a key regulator of adipose tissue browning in the LLC system, a link between EGFR ligand production and cancer cachexia is intriguing and warrants further study. Activation of EGFR/MEK signaling in the primary tumor has been recently linked to MEK activation and wasting in host tissues [102], and while CAFs as a source for these ligands or for PTHrP have not been specifically addressed, EGFR signaling has been functionally linked to cachexia and/or energy expenditure in additional systems [103,104]. Providing ligands which act either via tumor cells or directly on adipocytes to promote thermogenesis might suggest a deleterious role for CAFs as promoters of cancer cachexia, and such a role may indeed be tissue- and context-dependent.
5. Conclusions and Future Directions
Non-malignant cells of the tumor microenvironment, including but not limited to CAFs, exert an important influence on key metabolic pathways in cancer cells and on intratumoral metabolite levels. The significance of these paracrine interactions warrants further study in vivo, as cancer cells exhibit specific and complex metabolic requirements within host tissues [105,106,107,108,109] that are difficult to model using in vitro systems. CAFs present a limitation in this regard, as specific Cre lines to achieve genetic manipulation in these cells are presently lacking. Further, while studies of metabolite exchange in vitro have established important modes of cell-cell contact within the tumor microenvironment, validation and further investigation of these interactions will be bolstered by emerging means to study intercellular metabolic relationships within tissues [15]. In considering CAF-cancer cell interactions as potential therapeutic targets, it will be important to understand the critical and non-redundant metabolic functions of CAFs that enable cancer cells to maintain their proliferative capacity within a nutrient-poor tumor microenvironment. As cancer cells exhibit metabolic plasticity [110,111], therapies targeting metabolism-modulating pathways will likely need to target parallel mechanisms fulfilling bioenergetic needs, or to combine metabolic inhibitors with therapeutic interventions that suppress cancer cell plasticity and thus the capacity for metabolic adaptation. Further, as suppression of anti-tumor immunity is increasingly linked to intratumoral metabolite levels and to activity of key metabolic pathways in immune cells [112], the consequence of the CAF secretome on the metabolism and function of immune cells in the tumor microenvironment warrants investigation.
Funding
J.A. is supported by an OHSU Fellowship for Diversity in Research. M.H.S. is supported by NIH grants R00 CA188259 and R01 CA229580, American Cancer Society Research Scholar Grant 132898-RSG-18-142-01-CSM, V Foundation V Scholar Award, DOD Peer Reviewed Cancer Research Program Career Development Award W81XWH-18-1-0437, Hirshberg Foundation Seed Grant, Medical Research Foundation New Investigator Grant, OHSU Brenden-Colson Center Pilot Award, start-up funds from the OHSU Knight Cancer Institute, and an OHSU Cancer Early Detection Advanced Research Pilot Award.
Acknowledgments
We thank Erin Helms and Kathrina Onate for their constructive input.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kalluri, R. The biology and function of fibroblasts in cancer. Nat. Rev. Cancer 2016, 16, 582–598. [Google Scholar] [CrossRef]
- Pietras, K.; Ostman, A. Hallmarks of cancer: Interactions with the tumor stroma. Exp. Cell Res. 2010, 316, 1324–1331. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Coussens, L.M. Accessories to the crime: Functions of cells recruited to the tumor microenvironment. Cancer Cell 2012, 21, 309–322. [Google Scholar] [CrossRef]
- Paunescu, V.; Bojin, F.M.; Tatu, C.A.; Gavriliuc, O.I.; Rosca, A.; Gruia, A.T.; Tanasie, G.; Bunu, C.; Crisnic, D.; Gherghiceanu, M.; et al. Tumour-associated fibroblasts and mesenchymal stem cells: More similarities than differences. J. Cell. Mol. Med. 2011, 15, 635–646. [Google Scholar] [CrossRef] [PubMed]
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef]
- Raz, Y.; Cohen, N.; Shani, O.; Bell, R.E.; Novitskiy, S.V.; Abramovitz, L.; Levy, C.; Milyavsky, M.; Leider-Trejo, L.; Moses, H.L.; et al. Bone marrow-derived fibroblasts are a functionally distinct stromal cell population in breast cancer. J. Exp. Med. 2018, 215, 3075–3093. [Google Scholar] [CrossRef]
- Ohlund, D.; Handly-Santana, A.; Biffi, G.; Elyada, E.; Almeida, A.S.; Ponz-Sarvise, M.; Corbo, V.; Oni, T.E.; Hearn, S.A.; Lee, E.J.; et al. Distinct populations of inflammatory fibroblasts and myofibroblasts in pancreatic cancer. J. Exp. Med. 2017, 214, 579–596. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biffi, G.; Oni, T.E.; Spielman, B.; Hao, Y.; Elyada, E.; Park, Y.; Preall, J.; Tuveson, D.A. IL-1-induced JAK/STAT signaling is antagonized by TGF-beta to shape CAF heterogeneity in pancreatic ductal adenocarcinoma. Cancer Discov. 2018. [Google Scholar] [CrossRef]
- Cirri, P.; Chiarugi, P. Cancer associated fibroblasts: The dark side of the coin. Am. J. Cancer Res. 2011, 1, 482–497. [Google Scholar]
- Kalluri, R.; Zeisberg, M. Fibroblasts in cancer. Nat. Rev. Cancer 2006, 6, 392–401. [Google Scholar] [CrossRef]
- Celis, J.E.; Moreira, J.M.; Gromova, I.; Cabezon, T.; Ralfkiaer, U.; Guldberg, P.; Straten, P.T.; Mouridsen, H.; Friis, E.; Holm, D.; et al. Towards discovery-driven translational research in breast cancer. FEBS J. 2005, 272, 2–15. [Google Scholar] [CrossRef] [PubMed]
- Dirat, B.; Bochet, L.; Dabek, M.; Daviaud, D.; Dauvillier, S.; Majed, B.; Wang, Y.Y.; Meulle, A.; Salles, B.; Le Gonidec, S.; et al. Cancer-associated adipocytes exhibit an activated phenotype and contribute to breast cancer invasion. Cancer Res. 2011, 71, 2455–2465. [Google Scholar] [CrossRef] [PubMed]
- Erez, N.; Truitt, M.; Olson, P.; Arron, S.T.; Hanahan, D. Cancer-Associated Fibroblasts Are Activated in Incipient Neoplasia to Orchestrate Tumor-Promoting Inflammation in an NF-kappaB-Dependent Manner. Cancer Cell 2010, 17, 135–147. [Google Scholar] [CrossRef]
- Chiarugi, P.; Cirri, P. Metabolic exchanges within tumor microenvironment. Cancer Lett. 2016, 380, 272–280. [Google Scholar] [CrossRef]
- Miller, A.; Nagy, C.; Knapp, B.; Laengle, J.; Ponweiser, E.; Groeger, M.; Starkl, P.; Bergmann, M.; Wagner, O.; Haschemi, A. Exploring Metabolic Configurations of Single Cells within Complex Tissue Microenvironments. Cell Metab. 2017, 26, 788–800.e6. [Google Scholar] [CrossRef] [PubMed]
- Neesse, A.; Algul, H.; Tuveson, D.A.; Gress, T.M. Stromal biology and therapy in pancreatic cancer: A changing paradigm. Gut 2015, 64, 1476–1484. [Google Scholar] [CrossRef]
- Provenzano, P.P.; Cuevas, C.; Chang, A.E.; Goel, V.K.; Von Hoff, D.D.; Hingorani, S.R. Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 2012, 21, 418–429. [Google Scholar] [CrossRef] [Green Version]
- Jacobetz, M.A.; Chan, D.S.; Neesse, A.; Bapiro, T.E.; Cook, N.; Frese, K.K.; Feig, C.; Nakagawa, T.; Caldwell, M.E.; Zecchini, H.I.; et al. Hyaluronan impairs vascular function and drug delivery in a mouse model of pancreatic cancer. Gut 2013, 62, 112–120. [Google Scholar] [CrossRef]
- Kamphorst, J.J.; Nofal, M.; Commisso, C.; Hackett, S.R.; Lu, W.; Grabocka, E.; Vander Heiden, M.G.; Miller, G.; Drebin, J.A.; Bar-Sagi, D.; et al. Human pancreatic cancer tumors are nutrient poor and tumor cells actively scavenge extracellular protein. Cancer Res. 2015, 75, 544–553. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Commisso, C.; Davidson, S.M.; Soydaner-Azeloglu, R.G.; Parker, S.J.; Kamphorst, J.J.; Hackett, S.; Grabocka, E.; Nofal, M.; Drebin, J.A.; Thompson, C.B.; et al. Macropinocytosis of protein is an amino acid supply route in Ras-transformed cells. Nature 2013, 497, 633–637. [Google Scholar] [CrossRef]
- Olivares, O.; Mayers, J.R.; Gouirand, V.; Torrence, M.E.; Gicquel, T.; Borge, L.; Lac, S.; Roques, J.; Lavaut, M.N.; Berthezene, P.; et al. Collagen-derived proline promotes pancreatic ductal adenocarcinoma cell survival under nutrient limited conditions. Nat. Commun. 2017, 8, 16031. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sherman, M.H.; Yu, R.T.; Tseng, T.W.; Sousa, C.M.; Liu, S.; Truitt, M.L.; He, N.; Ding, N.; Liddle, C.; Atkins, A.R.; et al. Stromal cues regulate the pancreatic cancer epigenome and metabolome. Proc. Natl. Acad. Sci. USA 2017, 114, 1129–1134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Curtis, M.; Kenny, H.A.; Ashcroft, B.; Mukherjee, A.; Johnson, A.; Zhang, Y.; Helou, Y.; Batlle, R.; Liu, X.; Gutierrez, N.; et al. Fibroblasts Mobilize Tumor Cell Glycogen to Promote Proliferation and Metastasis. Cell Metab. 2019, 29, 141–155.e9. [Google Scholar] [CrossRef]
- Sullivan, W.J.; Mullen, P.J.; Schmid, E.W.; Flores, A.; Momcilovic, M.; Sharpley, M.S.; Jelinek, D.; Whiteley, A.E.; Maxwell, M.B.; Wilde, B.R.; et al. Extracellular Matrix Remodeling Regulates Glucose Metabolism through TXNIP Destabilization. Cell 2018, 175, 117–132.e121. [Google Scholar] [CrossRef] [PubMed]
- Bertero, T.; Oldham, W.M.; Grasset, E.M.; Bourget, I.; Boulter, E.; Pisano, S.; Hofman, P.; Bellvert, F.; Meneguzzi, G.; Bulavin, D.V.; et al. Tumor-Stroma Mechanics Coordinate Amino Acid Availability to Sustain Tumor Growth and Malignancy. Cell Metab. 2019, 29, 124–140.e10. [Google Scholar] [CrossRef] [PubMed]
- Wang, W.; Kryczek, I.; Dostal, L.; Lin, H.; Tan, L.; Zhao, L.; Lu, F.; Wei, S.; Maj, T.; Peng, D.; et al. Effector T Cells Abrogate Stroma-Mediated Chemoresistance in Ovarian Cancer. Cell 2016, 165, 1092–1105. [Google Scholar] [CrossRef]
- Ziani, L.; Chouaib, S.; Thiery, J. Alteration of the Antitumor Immune Response by Cancer-Associated Fibroblasts. Front. Immunol. 2018, 9, 414. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Yang, Y.; Hua, X.; Wang, G.; Liu, W.; Jia, C.; Tai, Y.; Zhang, Q.; Chen, G. Hepatocellular carcinoma-associated fibroblasts trigger NK cell dysfunction via PGE2 and IDO. Cancer Lett. 2012, 318, 154–161. [Google Scholar] [CrossRef]
- Hsu, Y.L.; Hung, J.Y.; Chiang, S.Y.; Jian, S.F.; Wu, C.Y.; Lin, Y.S.; Tsai, Y.M.; Chou, S.H.; Tsai, M.J.; Kuo, P.L. Lung cancer-derived galectin-1 contributes to cancer associated fibroblast-mediated cancer progression and immune suppression through TDO2/kynurenine axis. Oncotarget 2016, 7, 27584–27598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, A.; Webster, M.R.; Marchbank, K.; Behera, R.; Ndoye, A.; Kugel, C.H., 3rd; Dang, V.M.; Appleton, J.; O’Connell, M.P.; Cheng, P.; et al. sFRP2 in the aged microenvironment drives melanoma metastasis and therapy resistance. Nature 2016, 532, 250–254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eales, K.L.; Hollinshead, K.E.; Tennant, D.A. Hypoxia and metabolic adaptation of cancer cells. Oncogenesis 2016, 5, e190. [Google Scholar] [CrossRef]
- Vander Heiden, M.G.; Cantley, L.C.; Thompson, C.B. Understanding the Warburg effect: The metabolic requirements of cell proliferation. Science 2009, 324, 1029–1033. [Google Scholar] [CrossRef]
- Majmundar, A.J.; Wong, W.J.; Simon, M.C. Hypoxia-inducible factors and the response to hypoxic stress. Mol. Cell 2010, 40, 294–309. [Google Scholar] [CrossRef] [PubMed]
- Sonveaux, P.; Vegran, F.; Schroeder, T.; Wergin, M.C.; Verrax, J.; Rabbani, Z.N.; De Saedeleer, C.J.; Kennedy, K.M.; Diepart, C.; Jordan, B.F.; et al. Targeting lactate-fueled respiration selectively kills hypoxic tumor cells in mice. J. Clin. Invest. 2008, 118, 3930–3942. [Google Scholar] [CrossRef] [Green Version]
- Guillaumond, F.; Leca, J.; Olivares, O.; Lavaut, M.N.; Vidal, N.; Berthezene, P.; Dusetti, N.J.; Loncle, C.; Calvo, E.; Turrini, O.; et al. Strengthened glycolysis under hypoxia supports tumor symbiosis and hexosamine biosynthesis in pancreatic adenocarcinoma. Proc. Natl. Acad. Sci. USA 2013, 110, 3919–3924. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, Y.; Liu, S.; Yin, S.; Niu, W.; Xiong, W.; Tan, M.; Li, G.; Zhou, M. The reverse Warburg effect is likely to be an Achilles’ heel of cancer that can be exploited for cancer therapy. Oncotarget 2017, 8, 57813–57825. [Google Scholar] [CrossRef] [PubMed]
- Pavlides, S.; Whitaker-Menezes, D.; Castello-Cros, R.; Flomenberg, N.; Witkiewicz, A.K.; Frank, P.G.; Casimiro, M.C.; Wang, C.; Fortina, P.; Addya, S.; et al. The reverse Warburg effect: Aerobic glycolysis in cancer associated fibroblasts and the tumor stroma. Cell Cycle 2009, 8, 3984–4001. [Google Scholar] [CrossRef] [Green Version]
- Sotgia, F.; Martinez-Outschoorn, U.E.; Pavlides, S.; Howell, A.; Pestell, R.G.; Lisanti, M.P. Understanding the Warburg effect and the prognostic value of stromal caveolin-1 as a marker of a lethal tumor microenvironment. Breast Cancer Res. 2011, 13, 213. [Google Scholar] [CrossRef]
- Fiaschi, T.; Marini, A.; Giannoni, E.; Taddei, M.L.; Gandellini, P.; De Donatis, A.; Lanciotti, M.; Serni, S.; Cirri, P.; Chiarugi, P. Reciprocal metabolic reprogramming through lactate shuttle coordinately influences tumor-stroma interplay. Cancer Res. 2012, 72, 5130–5140. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Wang, Y.; Shi, Z.; Liu, J.; Sun, P.; Hou, X.; Zhang, J.; Zhao, S.; Zhou, B.P.; Mi, J. Metabolic reprogramming of cancer-associated fibroblasts by IDH3alpha downregulation. Cell Rep. 2015, 10, 1335–1348. [Google Scholar] [CrossRef] [PubMed]
- Iommarini, L.; Porcelli, A.M.; Gasparre, G.; Kurelac, I. Non-Canonical Mechanisms Regulating Hypoxia-Inducible Factor 1 Alpha in Cancer. Front. Oncol. 2017, 7, 286. [Google Scholar] [CrossRef] [PubMed]
- Fuyuhiro, Y.; Yashiro, M.; Noda, S.; Kashiwagi, S.; Matsuoka, J.; Doi, Y.; Kato, Y.; Hasegawa, T.; Sawada, T.; Hirakawa, K. Upregulation of cancer-associated myofibroblasts by TGF-beta from scirrhous gastric carcinoma cells. Br. J. Cancer 2011, 105, 996–1001. [Google Scholar] [CrossRef] [PubMed]
- Guido, C.; Whitaker-Menezes, D.; Capparelli, C.; Balliet, R.; Lin, Z.; Pestell, R.G.; Howell, A.; Aquila, S.; Ando, S.; Martinez-Outschoorn, U.; et al. Metabolic reprogramming of cancer-associated fibroblasts by TGF-beta drives tumor growth: Connecting TGF-beta signaling with “Warburg-like” cancer metabolism and L-lactate production. Cell Cycle 2012, 11, 3019–3035. [Google Scholar] [CrossRef] [PubMed]
- Sousa, C.M.; Biancur, D.E.; Wang, X.; Halbrook, C.J.; Sherman, M.H.; Zhang, L.; Kremer, D.; Hwang, R.F.; Witkiewicz, A.K.; Ying, H.; et al. Pancreatic stellate cells support tumour metabolism through autophagic alanine secretion. Nature 2016, 536, 479–483. [Google Scholar] [CrossRef] [Green Version]
- Rattigan, Y.I.; Patel, B.B.; Ackerstaff, E.; Sukenick, G.; Koutcher, J.A.; Glod, J.W.; Banerjee, D. Lactate is a mediator of metabolic cooperation between stromal carcinoma associated fibroblasts and glycolytic tumor cells in the tumor microenvironment. Exp. Cell Res. 2012, 318, 326–335. [Google Scholar] [CrossRef]
- Wise, D.R.; Thompson, C.B. Glutamine addiction: A new therapeutic target in cancer. Trends Biochem. Sci. 2010, 35, 427–433. [Google Scholar] [CrossRef]
- Yang, L.; Achreja, A.; Yeung, T.L.; Mangala, L.S.; Jiang, D.; Han, C.; Baddour, J.; Marini, J.C.; Ni, J.; Nakahara, R.; et al. Targeting Stromal Glutamine Synthetase in Tumors Disrupts Tumor Microenvironment-Regulated Cancer Cell Growth. Cell Metab. 2016, 24, 685–700. [Google Scholar] [CrossRef]
- Amelio, I.; Cutruzzola, F.; Antonov, A.; Agostini, M.; Melino, G. Serine and glycine metabolism in cancer. Trends Biochem. Sci. 2014, 39, 191–198. [Google Scholar] [CrossRef] [PubMed]
- Valencia, T.; Kim, J.Y.; Abu-Baker, S.; Moscat-Pardos, J.; Ahn, C.S.; Reina-Campos, M.; Duran, A.; Castilla, E.A.; Metallo, C.M.; Diaz-Meco, M.T.; et al. Metabolic reprogramming of stromal fibroblasts through p62-mTORC1 signaling promotes inflammation and tumorigenesis. Cancer Cell 2014, 26, 121–135. [Google Scholar] [CrossRef] [Green Version]
- Duran, A.; Hernandez, E.D.; Reina-Campos, M.; Castilla, E.A.; Subramaniam, S.; Raghunandan, S.; Roberts, L.R.; Kisseleva, T.; Karin, M.; Diaz-Meco, M.T.; et al. p62/SQSTM1 by Binding to Vitamin D Receptor Inhibits Hepatic Stellate Cell Activity, Fibrosis, and Liver Cancer. Cancer Cell 2016, 30, 595–609. [Google Scholar] [CrossRef]
- Linares, J.F.; Cordes, T.; Duran, A.; Reina-Campos, M.; Valencia, T.; Ahn, C.S.; Castilla, E.A.; Moscat, J.; Metallo, C.M.; Diaz-Meco, M.T. ATF4-Induced Metabolic Reprograming Is a Synthetic Vulnerability of the p62-Deficient Tumor Stroma. Cell Metab. 2017, 26, 817–829.e6. [Google Scholar] [CrossRef]
- Sherman, M.H. Stellate Cells in Tissue Repair, Inflammation, and Cancer. Annu. Rev. Cell Dev. Biol. 2018, 34, 333–355. [Google Scholar] [CrossRef]
- Kamphorst, J.J.; Cross, J.R.; Fan, J.; de Stanchina, E.; Mathew, R.; White, E.P.; Thompson, C.B.; Rabinowitz, J.D. Hypoxic and Ras-transformed cells support growth by scavenging unsaturated fatty acids from lysophospholipids. Proc. Natl. Acad. Sci. USA 2013, 110, 8882–8887. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auciello, F.R.; Bulusu, V.; Oon, C.; Tait-Mulder, J.; Berry, M.; Bhattacharyya, S.; Tumanov, S.; Allen-Petersen, B.L.; Link, J.; Kendsersky, N.D.; et al. A stromal lysolipid-autotaxin signaling axis promotes pancreatic tumor progression. Cancer Discov. 2019. [Google Scholar] [CrossRef] [PubMed]
- Nardi, F.; Fitchev, P.; Franco, O.E.; Ivanisevic, J.; Scheibler, A.; Hayward, S.W.; Brendler, C.B.; Welte, M.A.; Crawford, S.E. PEDF regulates plasticity of a novel lipid-MTOC axis in prostate cancer-associated fibroblasts. J. Cell Sci. 2018, 131. [Google Scholar] [CrossRef] [PubMed]
- Vasseur, S.; Guillaumond, F. LDL Receptor: An open route to feed pancreatic tumor cells. Mol. Cell Oncol 2016, 3, e1033586. [Google Scholar] [CrossRef]
- Garcia-Bermudez, J.; Baudrier, L.; Bayraktar, E.C.; Shen, Y.; La, K.; Guarecuco, R.; Yucel, B.; Fiore, D.; Tavora, B.; Freinkman, E.; et al. Squalene accumulation in cholesterol auxotrophic lymphomas prevents oxidative cell death. Nature 2019, 567, 118–122. [Google Scholar] [CrossRef]
- Gangoda, L.; Boukouris, S.; Liem, M.; Kalra, H.; Mathivanan, S. Extracellular vesicles including exosomes are mediators of signal transduction: Are they protective or pathogenic? Proteomics 2015, 15, 260–271. [Google Scholar] [CrossRef]
- Zhao, H.; Yang, L.; Baddour, J.; Achreja, A.; Bernard, V.; Moss, T.; Marini, J.C.; Tudawe, T.; Seviour, E.G.; San Lucas, F.A.; et al. Tumor microenvironment derived exosomes pleiotropically modulate cancer cell metabolism. Elife 2016, 5, e10250. [Google Scholar] [CrossRef]
- Richards, K.E.; Zeleniak, A.E.; Fishel, M.L.; Wu, J.; Littlepage, L.E.; Hill, R. Cancer-associated fibroblast exosomes regulate survival and proliferation of pancreatic cancer cells. Oncogene 2017, 36, 1770–1778. [Google Scholar] [CrossRef]
- Petruzzelli, M.; Wagner, E.F. Mechanisms of metabolic dysfunction in cancer-associated cachexia. Genes Dev. 2016, 30, 489–501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fearon, K.; Strasser, F.; Anker, S.D.; Bosaeus, I.; Bruera, E.; Fainsinger, R.L.; Jatoi, A.; Loprinzi, C.; MacDonald, N.; Mantovani, G.; et al. Definition and classification of cancer cachexia: An international consensus. Lancet Oncol. 2011, 12, 489–495. [Google Scholar] [CrossRef]
- Fearon, K.C.; Glass, D.J.; Guttridge, D.C. Cancer cachexia: Mediators, signaling, and metabolic pathways. Cell Metab. 2012, 16, 153–166. [Google Scholar] [CrossRef] [PubMed]
- Mayers, J.R.; Wu, C.; Clish, C.B.; Kraft, P.; Torrence, M.E.; Fiske, B.P.; Yuan, C.; Bao, Y.; Townsend, M.K.; Tworoger, S.S.; et al. Elevation of circulating branched-chain amino acids is an early event in human pancreatic adenocarcinoma development. Nat. Med. 2014, 20, 1193–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, M.; Haji, S.; Amagai, T. High Serum Essential Amino Acids as a Predictor of Skeletal Muscle Depletion in Patients With Cachexia and Advanced Gastrointestinal Cancers. Nutr. Clin. Pract. 2017, 32, 645–651. [Google Scholar] [CrossRef]
- Garin-Chesa, P.; Old, L.J.; Rettig, W.J. Cell surface glycoprotein of reactive stromal fibroblasts as a potential antibody target in human epithelial cancers. Proc. Natl. Acad. Sci. USA 1990, 87, 7235–7239. [Google Scholar] [CrossRef]
- Brokopp, C.E.; Schoenauer, R.; Richards, P.; Bauer, S.; Lohmann, C.; Emmert, M.Y.; Weber, B.; Winnik, S.; Aikawa, E.; Graves, K.; et al. Fibroblast activation protein is induced by inflammation and degrades type I collagen in thin-cap fibroatheromata. Eur. Heart J. 2011, 32, 2713–2722. [Google Scholar] [CrossRef] [Green Version]
- Feig, C.; Jones, J.O.; Kraman, M.; Wells, R.J.; Deonarine, A.; Chan, D.S.; Connell, C.M.; Roberts, E.W.; Zhao, Q.; Caballero, O.L.; et al. Targeting CXCL12 from FAP-expressing carcinoma-associated fibroblasts synergizes with anti-PD-L1 immunotherapy in pancreatic cancer. Proc. Natl. Acad. Sci. USA 2013, 110, 20212–20217. [Google Scholar] [CrossRef]
- Roberts, E.W.; Deonarine, A.; Jones, J.O.; Denton, A.E.; Feig, C.; Lyons, S.K.; Espeli, M.; Kraman, M.; McKenna, B.; Wells, R.J.; et al. Depletion of stromal cells expressing fibroblast activation protein-alpha from skeletal muscle and bone marrow results in cachexia and anemia. J. Exp. Med. 2013, 210, 1137–1151. [Google Scholar] [CrossRef]
- Flint, T.R.; Janowitz, T.; Connell, C.M.; Roberts, E.W.; Denton, A.E.; Coll, A.P.; Jodrell, D.I.; Fearon, D.T. Tumor-Induced IL-6 Reprograms Host Metabolism to Suppress Anti-tumor Immunity. Cell Metab. 2016, 24, 672–684. [Google Scholar] [CrossRef] [Green Version]
- Argiles, J.M.; Busquets, S.; Lopez-Soriano, F.J. Cytokines in the pathogenesis of cancer cachexia. Curr Opin Clin. Nutr. Metab. Care 2003, 6, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Ohe, Y.; Podack, E.R.; Olsen, K.J.; Miyahara, Y.; Miura, K.; Saito, H.; Koishihara, Y.; Ohsugi, Y.; Ohira, T.; Nishio, K.; et al. Interleukin-6 cDNA transfected Lewis lung carcinoma cells show unaltered net tumour growth rate but cause weight loss and shortened survival in syngeneic mice. Br. J. Cancer 1993, 67, 939–944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsujinaka, T.; Ebisui, C.; Fujita, J.; Kishibuchi, M.; Morimoto, T.; Ogawa, A.; Katsume, A.; Ohsugi, Y.; Kominami, E.; Monden, M. Muscle undergoes atrophy in association with increase of lysosomal cathepsin activity in interleukin-6 transgenic mouse. Biochem. Biophys Res. Commun. 1995, 207, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Black, K.; Garrett, I.R.; Mundy, G.R. Chinese hamster ovarian cells transfected with the murine interleukin-6 gene cause hypercalcemia as well as cachexia, leukocytosis and thrombocytosis in tumor-bearing nude mice. Endocrinology 1991, 128, 2657–2659. [Google Scholar] [CrossRef]
- Strassmann, G.; Fong, M.; Kenney, J.S.; Jacob, C.O. Evidence for the involvement of interleukin 6 in experimental cancer cachexia. J. Clin. Invest. 1992, 89, 1681–1684. [Google Scholar] [CrossRef]
- Strassmann, G.; Fong, M.; Freter, C.E.; Windsor, S.; D’Alessandro, F.; Nordan, R.P. Suramin interferes with interleukin-6 receptor binding in vitro and inhibits colon-26-mediated experimental cancer cachexia in vivo. J. Clin. Invest. 1993, 92, 2152–2159. [Google Scholar] [CrossRef]
- Tamura, S.; Ouchi, K.F.; Mori, K.; Endo, M.; Matsumoto, T.; Eda, H.; Tanaka, Y.; Ishitsuka, H.; Tokita, H.; Yamaguchi, K. Involvement of human interleukin 6 in experimental cachexia induced by a human uterine cervical carcinoma xenograft. Clin. Cancer Res. 1995, 1, 1353–1358. [Google Scholar]
- Staal-van den Brekel, A.J.; Dentener, M.A.; Schols, A.M.; Buurman, W.A.; Wouters, E.F. Increased resting energy expenditure and weight loss are related to a systemic inflammatory response in lung cancer patients. J. Clin. Oncol. 1995, 13, 2600–2605. [Google Scholar] [CrossRef]
- Fearon, K.C.; McMillan, D.C.; Preston, T.; Winstanley, F.P.; Cruickshank, A.M.; Shenkin, A. Elevated circulating interleukin-6 is associated with an acute-phase response but reduced fixed hepatic protein synthesis in patients with cancer. Ann. Surg. 1991, 213, 26–31. [Google Scholar] [CrossRef]
- Okada, S.; Okusaka, T.; Ishii, H.; Kyogoku, A.; Yoshimori, M.; Kajimura, N.; Yamaguchi, K.; Kakizoe, T. Elevated serum interleukin-6 levels in patients with pancreatic cancer. Jpn. J. Clin. Oncol. 1998, 28, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Bonetto, A.; Aydogdu, T.; Kunzevitzky, N.; Guttridge, D.C.; Khuri, S.; Koniaris, L.G.; Zimmers, T.A. STAT3 activation in skeletal muscle links muscle wasting and the acute phase response in cancer cachexia. PLoS One 2011, 6, e22538. [Google Scholar] [CrossRef] [PubMed]
- Qiao, Y.; Zhang, C.; Li, A.; Wang, D.; Luo, Z.; Ping, Y.; Zhou, B.; Liu, S.; Li, H.; Yue, D.; et al. IL6 derived from cancer-associated fibroblasts promotes chemoresistance via CXCR7 in esophageal squamous cell carcinoma. Oncogene 2018, 37, 873–883. [Google Scholar] [CrossRef]
- Wu, X.; Tao, P.; Zhou, Q.; Li, J.; Yu, Z.; Wang, X.; Li, J.; Li, C.; Yan, M.; Zhu, Z.; et al. IL-6 secreted by cancer-associated fibroblasts promotes epithelial-mesenchymal transition and metastasis of gastric cancer via JAK2/STAT3 signaling pathway. Oncotarget 2017, 8, 20741–20750. [Google Scholar] [CrossRef] [Green Version]
- Duluc, C.; Moatassim-Billah, S.; Chalabi-Dchar, M.; Perraud, A.; Samain, R.; Breibach, F.; Gayral, M.; Cordelier, P.; Delisle, M.B.; Bousquet-Dubouch, M.P.; et al. Pharmacological targeting of the protein synthesis mTOR/4E-BP1 pathway in cancer-associated fibroblasts abrogates pancreatic tumour chemoresistance. EMBO Mol. Med. 2015, 7, 735–753. [Google Scholar] [CrossRef]
- Zhang, Y.; Yan, W.; Collins, M.A.; Bednar, F.; Rakshit, S.; Zetter, B.R.; Stanger, B.Z.; Chung, I.; Rhim, A.D.; di Magliano, M.P. Interleukin-6 is required for pancreatic cancer progression by promoting MAPK signaling activation and oxidative stress resistance. Cancer Res. 2013, 73, 6359–6374. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Dunn, A.J. Mouse interleukin-6 stimulates the HPA axis and increases brain tryptophan and serotonin metabolism. Neurochem. Int. 1998, 33, 143–154. [Google Scholar] [CrossRef]
- Lee, J.J.; Perera, R.M.; Wang, H.; Wu, D.C.; Liu, X.S.; Han, S.; Fitamant, J.; Jones, P.D.; Ghanta, K.S.; Kawano, S.; et al. Stromal response to Hedgehog signaling restrains pancreatic cancer progression. Proc. Natl. Acad. Sci. USA 2014, 111, E3091–E3100. [Google Scholar] [CrossRef] [Green Version]
- Ozdemir, B.C.; Pentcheva-Hoang, T.; Carstens, J.L.; Zheng, X.; Wu, C.C.; Simpson, T.R.; Laklai, H.; Sugimoto, H.; Kahlert, C.; Novitskiy, S.V.; et al. Depletion of carcinoma-associated fibroblasts and fibrosis induces immunosuppression and accelerates pancreas cancer with reduced survival. Cancer Cell 2014, 25, 719–734. [Google Scholar] [CrossRef]
- Rhim, A.D.; Oberstein, P.E.; Thomas, D.H.; Mirek, E.T.; Palermo, C.F.; Sastra, S.A.; Dekleva, E.N.; Saunders, T.; Becerra, C.P.; Tattersall, I.W.; et al. Stromal elements act to restrain, rather than support, pancreatic ductal adenocarcinoma. Cancer Cell 2014, 25, 735–747. [Google Scholar] [CrossRef] [Green Version]
- Sherman, M.H.; Yu, R.T.; Engle, D.D.; Ding, N.; Atkins, A.R.; Tiriac, H.; Collisson, E.A.; Connor, F.; Van Dyke, T.; Kozlov, S.; et al. Vitamin D receptor-mediated stromal reprogramming suppresses pancreatitis and enhances pancreatic cancer therapy. Cell 2014, 159, 80–93. [Google Scholar] [CrossRef]
- Murata, T.; Mizushima, H.; Chinen, I.; Moribe, H.; Yagi, S.; Hoffman, R.M.; Kimura, T.; Yoshino, K.; Ueda, Y.; Enomoto, T.; et al. HB-EGF and PDGF mediate reciprocal interactions of carcinoma cells with cancer-associated fibroblasts to support progression of uterine cervical cancers. Cancer Res. 2011, 71, 6633–6642. [Google Scholar] [CrossRef]
- Neufert, C.; Becker, C.; Tureci, O.; Waldner, M.J.; Backert, I.; Floh, K.; Atreya, I.; Leppkes, M.; Jefremow, A.; Vieth, M.; et al. Tumor fibroblast-derived epiregulin promotes growth of colitis-associated neoplasms through ERK. J. Clin. Invest. 2013, 123, 1428–1443. [Google Scholar] [CrossRef] [PubMed]
- Cros, M.; Cataisson, C.; Cho, Y.M.; Berthois, Y.; Bernard-Poenaru, O.; Denne, M.; Graulet, A.M.; De Vernejoul, M.C.; Foley, J.; Bouizar, Z. Constitutive production of parathyroid hormone-related protein (PTHrP) by fibroblasts derived from normal and pathological human breast tissue. Oncol. Res. 2002, 13, 137–146. [Google Scholar]
- Blomme, E.A.; Sugimoto, Y.; Lin, Y.C.; Capen, C.C.; Rosol, T.J. Parathyroid hormone-related protein is a positive regulator of keratinocyte growth factor expression by normal dermal fibroblasts. Mol. Cell Endocrinol. 1999, 152, 189–197. [Google Scholar] [CrossRef]
- Foley, J.; Nickerson, N.; Riese, D.J., 2nd; Hollenhorst, P.C.; Lorch, G.; Foley, A.M. At the crossroads: EGFR and PTHrP signaling in cancer-mediated diseases of bone. Odontology 2012, 100, 109–129. [Google Scholar] [CrossRef] [Green Version]
- Kir, S.; White, J.P.; Kleiner, S.; Kazak, L.; Cohen, P.; Baracos, V.E.; Spiegelman, B.M. Tumour-derived PTH-related protein triggers adipose tissue browning and cancer cachexia. Nature 2014, 513, 100–104. [Google Scholar] [CrossRef]
- Bing, C.; Brown, M.; King, P.; Collins, P.; Tisdale, M.J.; Williams, G. Increased gene expression of brown fat uncoupling protein (UCP)1 and skeletal muscle UCP2 and UCP3 in MAC16-induced cancer cachexia. Cancer Res. 2000, 60, 2405–2410. [Google Scholar]
- Brooks, S.L.; Neville, A.M.; Rothwell, N.J.; Stock, M.J.; Wilson, S. Sympathetic activation of brown-adipose-tissue thermogenesis in cachexia. Biosci. Rep. 1981, 1, 509–517. [Google Scholar] [CrossRef] [Green Version]
- Shellock, F.G.; Riedinger, M.S.; Fishbein, M.C. Brown adipose tissue in cancer patients: Possible cause of cancer-induced cachexia. J. Cancer Res. Clin. Oncol. 1986, 111, 82–85. [Google Scholar] [CrossRef] [PubMed]
- Tsoli, M.; Moore, M.; Burg, D.; Painter, A.; Taylor, R.; Lockie, S.H.; Turner, N.; Warren, A.; Cooney, G.; Oldfield, B.; et al. Activation of thermogenesis in brown adipose tissue and dysregulated lipid metabolism associated with cancer cachexia in mice. Cancer Res. 2012, 72, 4372–4382. [Google Scholar] [CrossRef]
- Kir, S.; Spiegelman, B.M. Cachexia & Brown Fat: A Burning Issue in Cancer. Trends Cancer 2016, 2, 461–463. [Google Scholar] [CrossRef]
- Song, W.; Kir, S.; Hong, S.; Hu, Y.; Wang, X.; Binari, R.; Tang, H.W.; Chung, V.; Banks, A.S.; Spiegelman, B.; et al. Tumor-Derived Ligands Trigger Tumor Growth and Host Wasting via Differential MEK Activation. Dev. Cell 2019. [Google Scholar] [CrossRef] [PubMed]
- Yasmeen, R.; Shen, Q.; Lee, A.; Leung, J.H.; Kowdley, D.; DiSilvestro, D.J.; Xu, L.; Yang, K.; Maiseyeu, A.; Bal, N.C.; et al. Epiregulin induces leptin secretion and energy expenditure in high-fat diet-fed mice. J. Endocrinol. 2018, 239, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Hicks, M.J.; Chiuchiolo, M.J.; Ballon, D.; Dyke, J.P.; Aronowitz, E.; Funato, K.; Tabar, V.; Havlicek, D.; Fan, F.; Sondhi, D.; et al. Anti-Epidermal Growth Factor Receptor Gene Therapy for Glioblastoma. PLoS ONE 2016, 11, e0162978. [Google Scholar] [CrossRef] [PubMed]
- Hensley, C.T.; Faubert, B.; Yuan, Q.; Lev-Cohain, N.; Jin, E.; Kim, J.; Jiang, L.; Ko, B.; Skelton, R.; Loudat, L.; et al. Metabolic Heterogeneity in Human Lung Tumors. Cell 2016, 164, 681–694. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Udayakumar, D.; Cai, L.; Hu, Z.; Kapur, P.; Kho, E.Y.; Pavia-Jimenez, A.; Fulkerson, M.; de Leon, A.D.; Yuan, Q.; et al. Addressing metabolic heterogeneity in clear cell renal cell carcinoma with quantitative Dixon MRI. JCI Insight 2017, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muir, A.; Danai, L.V.; Vander Heiden, M.G. Microenvironmental regulation of cancer cell metabolism: Implications for experimental design and translational studies. Dis. Model. Mech. 2018, 11. [Google Scholar] [CrossRef]
- Mayers, J.R.; Torrence, M.E.; Danai, L.V.; Papagiannakopoulos, T.; Davidson, S.M.; Bauer, M.R.; Lau, A.N.; Ji, B.W.; Dixit, P.D.; Hosios, A.M.; et al. Tissue of origin dictates branched-chain amino acid metabolism in mutant Kras-driven cancers. Science 2016, 353, 1161–1165. [Google Scholar] [CrossRef]
- Gui, D.Y.; Sullivan, L.B.; Luengo, A.; Hosios, A.M.; Bush, L.N.; Gitego, N.; Davidson, S.M.; Freinkman, E.; Thomas, C.J.; Vander Heiden, M.G. Environment Dictates Dependence on Mitochondrial Complex I for NAD+ and Aspartate Production and Determines Cancer Cell Sensitivity to Metformin. Cell Metab. 2016, 24, 716–727. [Google Scholar] [CrossRef] [PubMed]
- Hulea, L.; Gravel, S.P.; Morita, M.; Cargnello, M.; Uchenunu, O.; Im, Y.K.; Lehuede, C.; Ma, E.H.; Leibovitch, M.; McLaughlan, S.; et al. Translational and HIF-1alpha-Dependent Metabolic Reprogramming Underpin Metabolic Plasticity and Responses to Kinase Inhibitors and Biguanides. Cell Metab. 2018, 28, 817–832.e818. [Google Scholar] [CrossRef]
- Campbell, S.L.; Wellen, K.E. Metabolic Signaling to the Nucleus in Cancer. Mol. Cell 2018, 71, 398–408. [Google Scholar] [CrossRef] [PubMed]
- Buck, M.D.; Sowell, R.T.; Kaech, S.M.; Pearce, E.L. Metabolic Instruction of Immunity. Cell 2017, 169, 570–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
Figure 1.
CAF secretions of immunomodulatory factors regulate anti-tumor immune response. CAF secretion of CXCL12/SDF1, M-CSF/CSF-1, IL-6, and CCL2/MCP-1 recruits tumor-associated macrophages to the TME and helps differentiate them to an M2 Immunosuppressive phenotype. CXCL1, CXCL2, CXCL5, CXCL6, CXCL8, and CCL2 recruits tumor-associated neutrophils and polarizes them to an N2 pro-tumoral phenotype. CAF and cancer cell secretion of TGF-β induces miR-183 to inhibit DAP12 transcription and reduce natural killer (NK) activating receptors (NKp30, NKp44, NKG2D), while PGE2 and IDO secretion decreases NK cell cytotoxicity against cancer cells. TGF-β also promotes cell death of CD8+ T cells by inhibiting expression of Bcl-2 and causes dendritic cells (DC) to downregulate expression of MHC class II, CD40, CD80, and CD86 leading to decreased antigen presentation efficiency along with decreased production of TNF-α, IFN-γ, and IL-12. TDO2 and IDO1 secretion promotes tryptophan metabolism to kynurenines (Kyn), inhibiting DC differentiation and damages T cell response by catabolizing tryptophan degradation into Kyn, causing T cell anergy and apoptosis through depletion of tryptophan and accumulation of immunosuppressive tryptophan catabolites. VEGF secretion inhibits DC generation and maturation by reducing MHC class II expression and antigen presenting abilities. Secretion of CCL2, CCL5, and CCL17 along with polarizing cytokines IL-1, IL-6, IL-13, and IL-26 switch CD4+ helper T lymphocytes from an anti-tumor TH1 response to a pro-tumor TH2 and TH17 response.
Figure 1.
CAF secretions of immunomodulatory factors regulate anti-tumor immune response. CAF secretion of CXCL12/SDF1, M-CSF/CSF-1, IL-6, and CCL2/MCP-1 recruits tumor-associated macrophages to the TME and helps differentiate them to an M2 Immunosuppressive phenotype. CXCL1, CXCL2, CXCL5, CXCL6, CXCL8, and CCL2 recruits tumor-associated neutrophils and polarizes them to an N2 pro-tumoral phenotype. CAF and cancer cell secretion of TGF-β induces miR-183 to inhibit DAP12 transcription and reduce natural killer (NK) activating receptors (NKp30, NKp44, NKG2D), while PGE2 and IDO secretion decreases NK cell cytotoxicity against cancer cells. TGF-β also promotes cell death of CD8+ T cells by inhibiting expression of Bcl-2 and causes dendritic cells (DC) to downregulate expression of MHC class II, CD40, CD80, and CD86 leading to decreased antigen presentation efficiency along with decreased production of TNF-α, IFN-γ, and IL-12. TDO2 and IDO1 secretion promotes tryptophan metabolism to kynurenines (Kyn), inhibiting DC differentiation and damages T cell response by catabolizing tryptophan degradation into Kyn, causing T cell anergy and apoptosis through depletion of tryptophan and accumulation of immunosuppressive tryptophan catabolites. VEGF secretion inhibits DC generation and maturation by reducing MHC class II expression and antigen presenting abilities. Secretion of CCL2, CCL5, and CCL17 along with polarizing cytokines IL-1, IL-6, IL-13, and IL-26 switch CD4+ helper T lymphocytes from an anti-tumor TH1 response to a pro-tumor TH2 and TH17 response.

Figure 2.
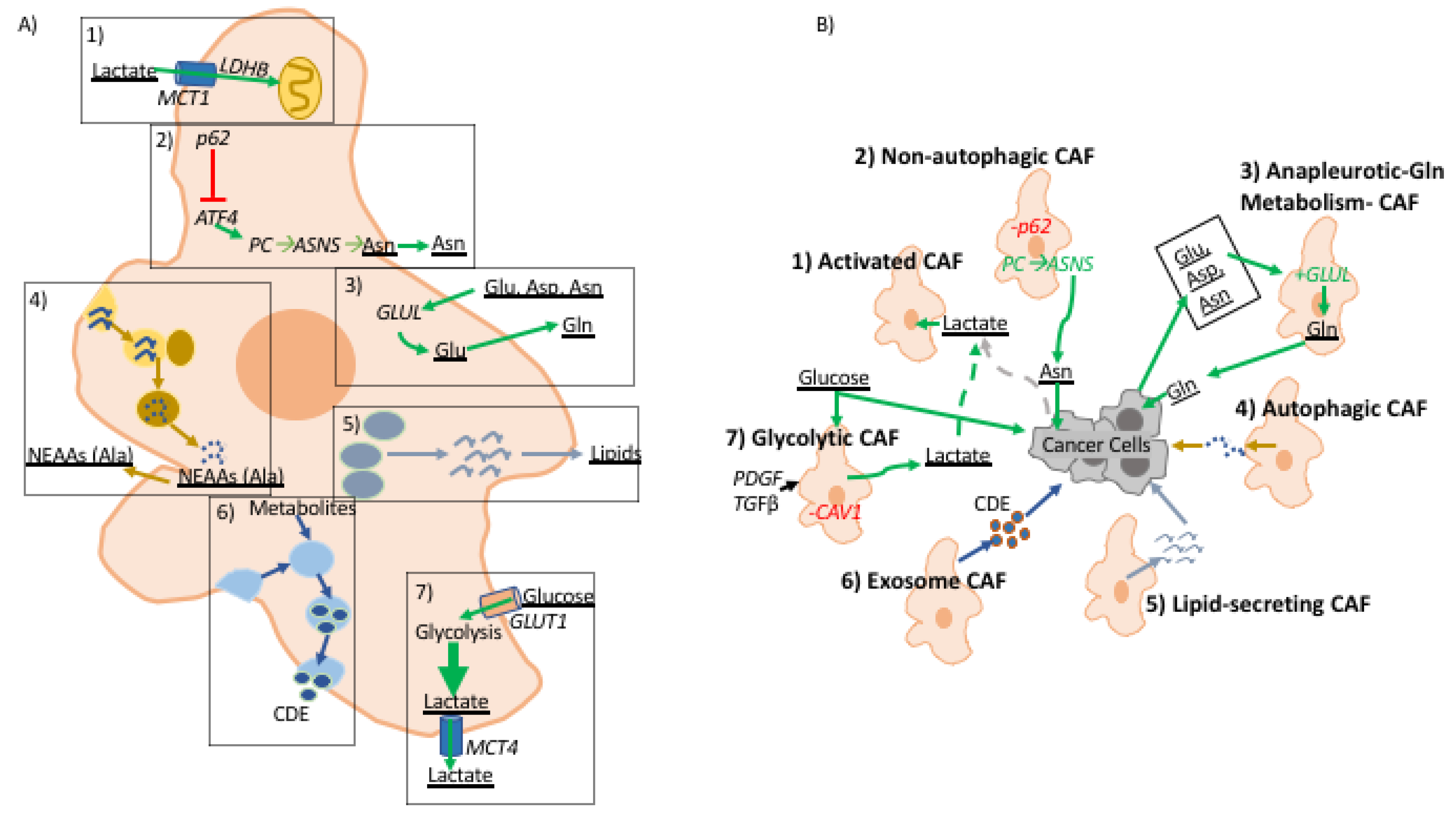
A role for fibroblast-derived metabolites in tumor-stroma interactions. (A) illustrates metabolic reprogramming in CAFs and (B) illustrates the effect of metabolites derived from CAFs to cancer cells in the TME. (1) Activated CAFs uptake excess TME lactate produced by glycolytic cells in the TME. (2) p62 deficient CAFs are autophagy defective and have upregulation of ATF4 which activates metabolic flux through pyruvate carboxylase (PC) → asparagine synthase (ASNS) pathway producing asparagine that is consumed by cancer cells. (3) CAFs characterized by upregulation of anapleurotic glutamine metabolism where cancer cell-derived aspartate, asparagine, and glutamate are used to generate glutamate that is fed to cancer cells; glutamine amino ligase (GLUL) is overexpressed in these CAFs. (4) Cancer cells induce autophagy in CAFs increasing turnover of non-essential amino acids, alanine has been shown to be up-taken by cancer cells to support growth. (5) Upon activation pancreatic and hepatic CAFs shift from lipid storing to lipid-secreting wherein CAF-derived lipids support proliferation and migratory potential of cancer cells. (6) Exosome releasing CAFs pack metabolic molecules used by cancer cells. (7) CAV1 deficient CAFs are known to upregulate glycolytic metabolism, as well as, fibroblast activation by PDGF and TGFβ. (A) describes metabolic alterations in CAFs in dashed boxes. In both figures metabolic pathways are denoted with green arrows, cellular processes are assigned specific colors, and metabolic molecules are underlined.
Figure 2.
A role for fibroblast-derived metabolites in tumor-stroma interactions. (A) illustrates metabolic reprogramming in CAFs and (B) illustrates the effect of metabolites derived from CAFs to cancer cells in the TME. (1) Activated CAFs uptake excess TME lactate produced by glycolytic cells in the TME. (2) p62 deficient CAFs are autophagy defective and have upregulation of ATF4 which activates metabolic flux through pyruvate carboxylase (PC) → asparagine synthase (ASNS) pathway producing asparagine that is consumed by cancer cells. (3) CAFs characterized by upregulation of anapleurotic glutamine metabolism where cancer cell-derived aspartate, asparagine, and glutamate are used to generate glutamate that is fed to cancer cells; glutamine amino ligase (GLUL) is overexpressed in these CAFs. (4) Cancer cells induce autophagy in CAFs increasing turnover of non-essential amino acids, alanine has been shown to be up-taken by cancer cells to support growth. (5) Upon activation pancreatic and hepatic CAFs shift from lipid storing to lipid-secreting wherein CAF-derived lipids support proliferation and migratory potential of cancer cells. (6) Exosome releasing CAFs pack metabolic molecules used by cancer cells. (7) CAV1 deficient CAFs are known to upregulate glycolytic metabolism, as well as, fibroblast activation by PDGF and TGFβ. (A) describes metabolic alterations in CAFs in dashed boxes. In both figures metabolic pathways are denoted with green arrows, cellular processes are assigned specific colors, and metabolic molecules are underlined.

© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sanford-Crane, H.; Abrego, J.; Sherman, M.H. Fibroblasts as Modulators of Local and Systemic Cancer Metabolism. Cancers 2019, 11, 619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050619
AMA Style
Sanford-Crane H, Abrego J, Sherman MH. Fibroblasts as Modulators of Local and Systemic Cancer Metabolism. Cancers. 2019; 11(5):619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050619
Chicago/Turabian StyleSanford-Crane, Hannah, Jaime Abrego, and Mara H. Sherman. 2019. "Fibroblasts as Modulators of Local and Systemic Cancer Metabolism" Cancers 11, no. 5: 619. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11050619
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.