Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search
2.2. Eligibility Criteria
2.3. Data Extraction
3. Results
3.1. Clinical Staging
3.2. Diagnostic Laparoscopy
3.3. Biliary Drainage
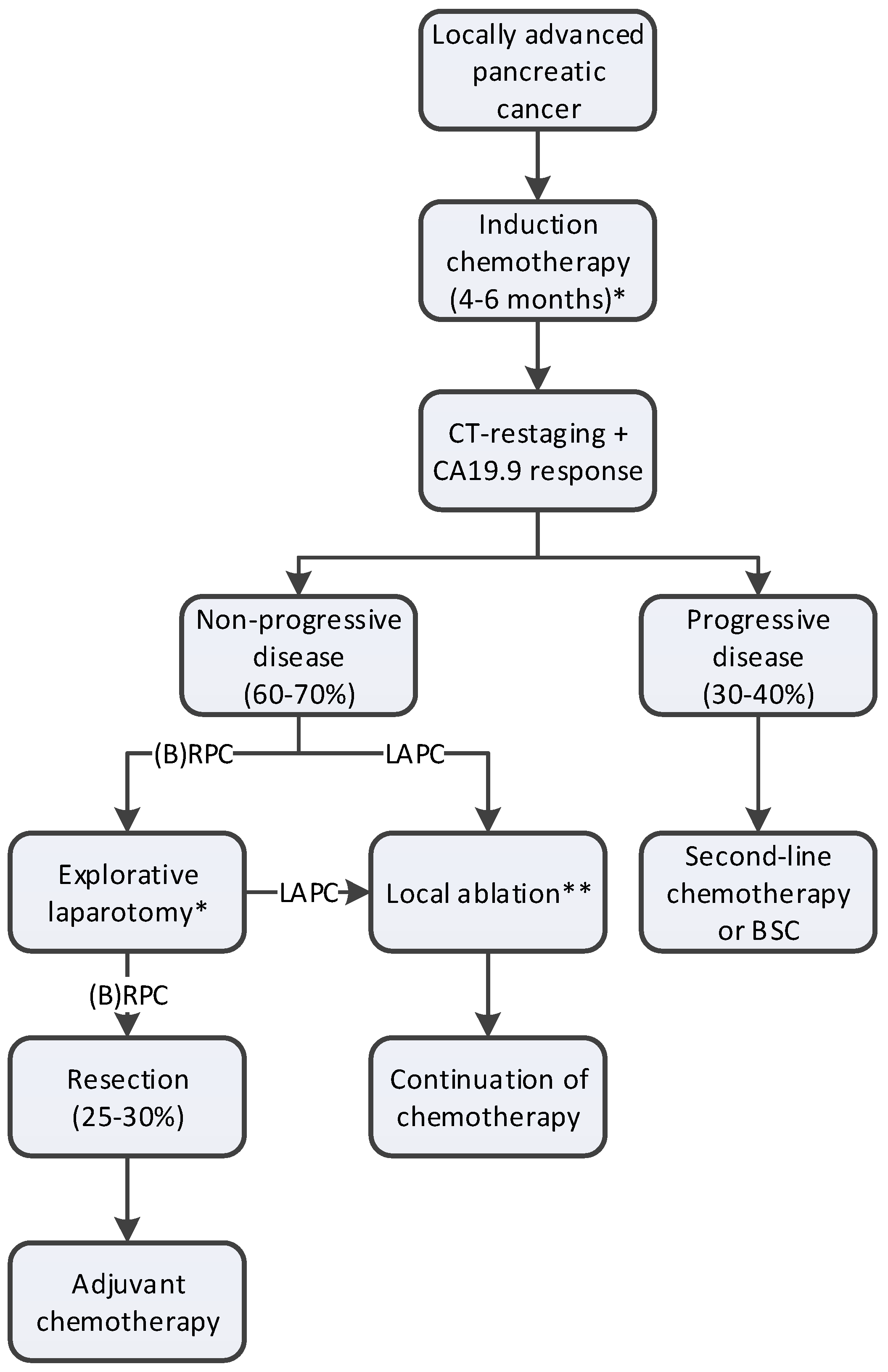
3.4. Induction Chemotherapy
3.5. Restaging after Chemotherapy
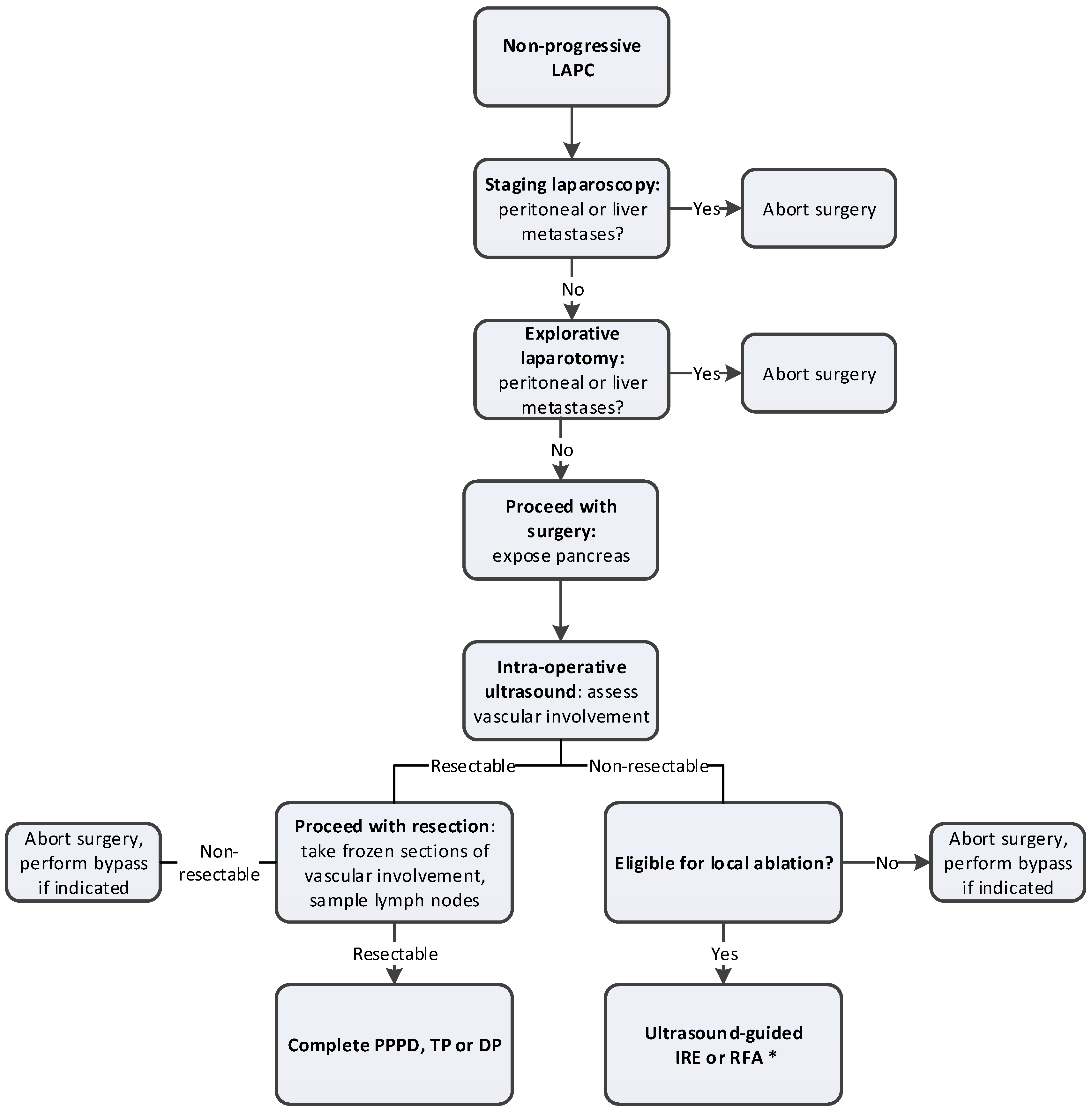
3.6. Selection for Surgery
3.7. Local Ablative Therapy
3.7.1. Irreversible Electroporation (IRE)
3.7.2. Radiofrequency Ablation (RFA)
3.7.3. Stereotactic Body Radiation Therapy (SBRT)
3.8. Surgical Procedure
3.9. Postoperative Care
4. Future Directions on the Management of Locally Advanced Pancreatic Cancer
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Search Strategy: PubMed
References
- Ferlay, J.; Soerjomataram, I.; Ervik, M.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11; International Agency for Research on Cancer: Lyon, France, 2014. [Google Scholar]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2015. CA Cancer J. Clin. 2015, 65, 5–29. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.; Naishadham, D.; Jemal, A. Cancer statistics, 2013. CA Cancer J. Clin. 2013, 63, 11–30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goere, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2015, 26 (Suppl. 5), v56–v68. [Google Scholar] [CrossRef] [PubMed]
- Rombouts, S.J.; Mungroop, T.H.; Heilmann, M.N.; van Laarhoven, H.W.; Busch, O.R.; Molenaar, I.Q.; Besselink, M.G.; Wilmink, J.W. FOLFIRINOX in Locally Advanced and Metastatic Pancreatic Cancer: A Single Centre Cohort Study. J. Cancer 2016, 7, 1861–1866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suker, M.; Beumer, B.R.; Sadot, E.; Marthey, L.; Faris, J.E.; Mellon, E.A.; El-Rayes, B.F.; Wang-Gillam, A.; Lacy, J.; Hosein, P.J.; et al. FOLFIRINOX for locally advanced pancreatic cancer: A systematic review and patient-level meta-analysis. Lancet Oncol. 2016, 17, 801–810. [Google Scholar] [CrossRef]
- Rombouts, S.J.; Walma, M.S.; Vogel, J.A.; van Rijssen, L.B.; Wilmink, J.W.; Mohammad, N.H.; van Santvoort, H.C.; Molenaar, I.Q.; Besselink, M.G. Systematic Review of Resection Rates and Clinical Outcomes After FOLFIRINOX-Based Treatment in Patients with Locally Advanced Pancreatic Cancer. Ann. Surg. Oncol. 2016, 23, 4352–4360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petrelli, F.; Coinu, A.; Borgonovo, K.; Cabiddu, M.; Ghilardi, M.; Lonati, V.; Aitini, E.; Barni, S.; Gruppo Italiano per lo Studio dei Carcinomi dell’Apparato Digerente (GISCAD). FOLFIRINOX-based neoadjuvant therapy in borderline resectable or unresectable pancreatic cancer: A meta-analytical review of published studies. Pancreas 2015, 44, 515–521. [Google Scholar] [CrossRef] [PubMed]
- Marthey, L.; Sa-Cunha, A.; Blanc, J.F.; Gauthier, M.; Cueff, A.; Francois, E.; Trouilloud, I.; Malka, D.; Bachet, J.B.; Coriat, R.; et al. FOLFIRINOX for locally advanced pancreatic adenocarcinoma: Results of an AGEO multicenter prospective observational cohort. Ann. Surg. Oncol. 2015, 22, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.R.; Marchegiani, G.; Hong, T.S.; Ryan, D.P.; Deshpande, V.; McDonnell, E.I.; Sabbatino, F.; Santos, D.D.; Allen, J.N.; Blaszkowsky, L.S.; et al. Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer. Ann. Surg. 2015, 261, 12–17. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Bagla, S.; Papadouris, D. Percutaneous irreversible electroporation of surgically unresectable pancreatic cancer: A case report. J. Vasc. Interv. Radiol. 2012, 23, 142–145. [Google Scholar] [CrossRef] [PubMed]
- Rombouts, S.J.; Vogel, J.A.; van Santvoort, H.C.; van Lienden, K.P.; van Hillegersberg, R.; Busch, O.R.; Besselink, M.G.; Molenaar, I.Q. Systematic review of innovative ablative therapies for the treatment of locally advanced pancreatic cancer. Br. J. Surg. 2015, 102, 182–193. [Google Scholar] [CrossRef] [PubMed]
- Tsai, S.; Christians, K.K.; Ritch, P.S.; George, B.; Khan, A.H.; Erickson, B.; Evans, D.B. Multimodality Therapy in Patients With Borderline Resectable or Locally Advanced Pancreatic Cancer: Importance of Locoregional Therapies for a Systemic Disease. J. Oncol. Pract. 2016, 12, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Chiorean, E.G.; Czito, B.; Scaife, C.; Narang, A.K.; Fountzilas, C.; Wolpin, B.M.; Al-Hawary, M.; Asbun, H.; et al. Pancreatic Adenocarcinoma, Version 1.2019. J. Natl. Compr. Cancer Netw. 2019, 17, 202–210. [Google Scholar] [CrossRef]
- Alizadeh, A.H.M.; Shahrokh, S.; Hadizadeh, M.; Padashi, M.; Zali, M.R. Diagnostic potency of EUS-guided FNA for the evaluation of pancreatic mass lesions. Endosc. Ultrasound 2016, 5, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Tyng, C.J.; Almeida, M.F.; Barbosa, P.N.; Bitencourt, A.G.; Berg, J.A.; Maciel, M.S.; Coimbra, F.J.; Schiavon, L.H.; Begnami, M.D.; Guimaraes, M.D.; et al. Computed tomography-guided percutaneous core needle biopsy in pancreatic tumor diagnosis. World J. Gastroenterol. 2015, 21, 3579–3586. [Google Scholar] [CrossRef] [PubMed]
- Wu, E.; Zhou, S.; Bhat, K.; Ma, Q. CA 19-9 and pancreatic cancer. Clin. Adv. Hematol. Oncol. 2013, 11, 53–55. [Google Scholar] [PubMed]
- Tsai, S.; George, B.; Wittmann, D.; Ritch, P.S.; Krepline, A.N.; Aldakkak, M.; Barnes, C.A.; Christians, K.K.; Dua, K.; Griffin, M.; et al. Importance of Normalization of CA19-9 Levels Following Neoadjuvant Therapy in Patients With Localized Pancreatic Cancer. Ann. Surg. 2018. Epub ahead of print (accessed on 1 July 2019). [Google Scholar] [CrossRef] [PubMed]
- Ballehaninna, U.K.; Chamberlain, R.S. The clinical utility of serum CA 19-9 in the diagnosis, prognosis and management of pancreatic adenocarcinoma: An evidence based appraisal. J. Gastrointest. Oncol. 2012, 3, 105–119. [Google Scholar] [CrossRef] [PubMed]
- Meijer, L.L.; Garajova, I.; Caparello, C.; Le Large, T.Y.S.; Frampton, A.E.; Vasile, E.; Funel, N.; Kazemier, G.; Giovannetti, E. Plasma miR-181a-5p Downregulation Predicts Response and Improved Survival After FOLFIRINOX in Pancreatic Ductal Adenocarcinoma. Ann. Surg. 2018. Epub ahead of print (accessed on 1 July 2019). [Google Scholar] [CrossRef] [PubMed]
- Tjensvoll, K.; Lapin, M.; Buhl, T.; Oltedal, S.; Steen-Ottosen Berry, K.; Gilje, B.; Soreide, J.A.; Javle, M.; Nordgard, O.; Smaaland, R. Clinical relevance of circulating KRAS mutated DNA in plasma from patients with advanced pancreatic cancer. Mol. Oncol. 2016, 10, 635–643. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.E.; Warshaw, A.L.; Rattner, D.W.; Willett, C.G.; McGrath, D.; Fernandez-del Castillo, C. Impact of laparoscopic staging in the treatment of pancreatic cancer. Arch. Surg. 2000, 135, 409–414. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.C.; Traverso, L.W. Diagnostic laparoscopy improves staging of pancreatic cancer deemed locally unresectable by computed tomography. Surg. Endosc. 2005, 19, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Allen, V.B.; Gurusamy, K.S.; Takwoingi, Y.; Kalia, A.; Davidson, B.R. Diagnostic accuracy of laparoscopy following computed tomography (CT) scanning for assessing the resectability with curative intent in pancreatic and periampullary cancer. Cochrane Database Syst. Rev. 2016, 7, CD009323. [Google Scholar] [CrossRef] [PubMed]
- Tol, J.A.; van Hooft, J.E.; Timmer, R.; Kubben, F.J.; van der Harst, E.; de Hingh, I.H.; Vleggaar, F.P.; Molenaar, I.Q.; Keulemans, Y.C.; Boerma, D.; et al. Metal or plastic stents for preoperative biliary drainage in resectable pancreatic cancer. Gut 2015, 65, 1981–1987. [Google Scholar] [CrossRef] [PubMed]
- Coelen, R.J.S.; Roos, E.; Rauws, E.A.J.; van Lienden, K.P.; van Delden, O.M.; van Gulik, T.M. Preoperative drainage for perihilar cholangiocarcinoma—Authors’ reply. Lancet Gastroenterol. Hepatol. 2019, 4, 11–12. [Google Scholar] [CrossRef]
- Conroy, T.; Desseigne, F.; Ychou, M.; Bouche, O.; Guimbaud, R.; Becouarn, Y.; Adenis, A.; Raoul, J.L.; Gourgou-Bourgade, S.; de la Fouchardiere, C.; et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N. Engl. J. Med. 2011, 364, 1817–1825. [Google Scholar] [CrossRef] [PubMed]
- Stein, S.M.; James, E.S.; Deng, Y.; Cong, X.; Kortmansky, J.S.; Li, J.; Staugaard, C.; Indukala, D.; Boustani, A.M.; Patel, V.; et al. Final analysis of a phase II study of modified FOLFIRINOX in locally advanced and metastatic pancreatic cancer. Br. J. Cancer 2016, 114, 737–743. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef]
- Muranaka, T.; Kuwatani, M.; Komatsu, Y.; Sawada, K.; Nakatsumi, H.; Kawamoto, Y.; Yuki, S.; Kubota, Y.; Kubo, K.; Kawahata, S.; et al. Comparison of efficacy and toxicity of FOLFIRINOX and gemcitabine with nab-paclitaxel in unresectable pancreatic cancer. J. Gastrointest. Oncol. 2017, 8, 566–571. [Google Scholar] [CrossRef] [Green Version]
- Dhir, M.; Zenati, M.S.; Hamad, A.; Singhi, A.D.; Bahary, N.; Hogg, M.E.; Zeh, H.J., III; Zureikat, A.H. FOLFIRINOX Versus Gemcitabine/Nab-Paclitaxel for Neoadjuvant Treatment of Resectable and Borderline Resectable Pancreatic Head Adenocarcinoma. Ann. Surg. Oncol. 2018, 25, 1896–1903. [Google Scholar] [CrossRef] [PubMed]
- Clinicaltrials.gov. Pancreatic Carcinoma: Chemoradiation Compared with Chemotherapy Alone after Induction Chemotherapy (CONKO-007). Available online: https://clinicaltrials.gov/ct2/show/NCT01827553 (accessed on 1 July 2019).
- Clinicaltrials.gov. Trial to Investigate Intensified Neoadjuvant Chemotherapy in Locally Advanced Pancreatic Cancer (NEOLAP). Available online: https://clinicaltrials.gov/ct2/show/NCT02125136 (accessed on 1 July 2019).
- Clinicaltrials.gov. Effect of Tumor Treating Fields (TTFields, 150 kHz) as Front-Line Treatment of Locally-advanced Pancreatic Adenocarcinoma Concomitant with Gemcitabine and Nab-Paclitaxel (PANOVA-3). Available online: https://clinicaltrials.gov/ct2/show/NCT03377491 (accessed on 1 July 2019).
- Clinicaltrials.gov. Effect of Intratumoral Injection of Gene Therapy for Locally Advanced Pancreatic Cancer (THERGAP-02). Available online: https://clinicaltrials.gov/ct2/show/NCT02806687 (accessed on 1 July 2019).
- Clinicaltrials.gov. Comparing the Efficacy of Irreversible Electroporation with Radiotherapy (CROSSFIRE). Available online: https://clinicaltrials.gov/ct2/show/NCT02791503 (accessed on 1 July 2019).
- Clinicaltrials.gov. Phase III FOLFIRINOX (mFFX) +/- SBRT in Locally Advanced Pancreatic Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT01926197 (accessed on 1 July 2019).
- Netherlands Trial Register. Pancreatic Locally Advanced Irresectable Cancer Ablation in the Netherlands (PELICAN). Available online: https://www.trialregister.nl/trial/4997 (accessed on 1 July 2019).
- Vogel, J.A.; Rombouts, S.J.; de Rooij, T.; van Delden, O.M.; Dijkgraaf, M.G.; van Gulik, T.M.; van Hooft, J.E.; van Laarhoven, H.W.; Martin, R.C.; Schoorlemmer, A.; et al. Induction Chemotherapy Followed by Resection or Irreversible Electroporation in Locally Advanced Pancreatic Cancer (IMPALA): A Prospective Cohort Study. Ann. Surg. Oncol. 2017, 24, 2734–2743. [Google Scholar] [CrossRef] [PubMed]
- Boone, B.A.; Steve, J.; Zenati, M.S.; Hogg, M.E.; Singhi, A.D.; Bartlett, D.L.; Zureikat, A.H.; Bahary, N.; Zeh, H.J., III. Serum CA 19-9 response to neoadjuvant therapy is associated with outcome in pancreatic adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 4351–4358. [Google Scholar] [CrossRef] [PubMed]
- Van Veldhuisen, E.; Vogel, J.A.; Klompmaker, S.; Busch, O.R.; van Laarhoven, H.W.M.; van Lienden, K.P.; Wilmink, J.W.; Marsman, H.A.; Besselink, M.G. Added value of CA19-9 response in predicting resectability of locally advanced pancreatic cancer following induction chemotherapy. HPB (Oxford) 2018, 20, 605–611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hackert, T.; Sachsenmaier, M.; Hinz, U.; Schneider, L.; Michalski, C.W.; Springfeld, C.; Strobel, O.; Jager, D.; Ulrich, A.; Buchler, M.W. Locally Advanced Pancreatic Cancer: Neoadjuvant Therapy with Folfirinox Results in Resectability in 60% of the Patients. Ann. Surg. 2016, 264, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Bachellier, P.; Addeo, P.; Faitot, F.; Nappo, G.; Dufour, P. Pancreatectomy with Arterial Resection for Pancreatic Adenocarcinoma: How Can It Be Done Safely and With Which Outcomes? A Single Institution’s Experience with 118 Patients. Ann. Surg. 2018. Epub ahead of print (accessed on 1 July 2019). [Google Scholar] [CrossRef]
- Del Chiaro, M.; Rangelova, E.; Halimi, A.; Ateeb, Z.; Scandavini, C.; Valente, R.; Segersvard, R.; Arnelo, U.; Verbeke, C.S. Pancreatectomy with arterial resection is superior to palliation in patients with borderline resectable or locally advanced pancreatic cancer. HPB (Oxford) 2019, 21, 219–225. [Google Scholar] [CrossRef] [PubMed]
- Michelakos, T.; Pergolini, I.; Castillo, C.F.; Honselmann, K.C.; Cai, L.; Deshpande, V.; Wo, J.Y.; Ryan, D.P.; Allen, J.N.; Blaszkowsky, L.S.; et al. Predictors of Resectability and Survival in Patients with Borderline and Locally Advanced Pancreatic Cancer who Underwent Neoadjuvant Treatment With FOLFIRINOX. Ann. Surg. 2019, 269, 733–740. [Google Scholar] [CrossRef]
- Rangelova, E.; Wefer, A.; Persson, S.; Valente, R.; Tanaka, K.; Orsini, N.; Segersvard, R.; Arnelo, U.; Del Chiaro, M. Surgery Improves Survival After Neoadjuvant Therapy for Borderline and Locally Advanced Pancreatic Cancer: A Single Institution Experience. Ann. Surg. 2019. [Google Scholar] [CrossRef]
- Tee, M.C.; Krajewski, A.C.; Groeschl, R.T.; Farnell, M.B.; Nagorney, D.M.; Kendrick, M.L.; Cleary, S.P.; Smoot, R.L.; Croome, K.P.; Truty, M.J. Indications and Perioperative Outcomes for Pancreatectomy with Arterial Resection. J. Am. Coll. Surg. 2018, 227, 255–269. [Google Scholar] [CrossRef]
- Gemenetzis, G.; Groot, V.P.; Blair, A.B.; Laheru, D.A.; Zheng, L.; Narang, A.K.; Fishman, E.K.; Hruban, R.H.; Yu, J.; Burkhart, R.A.; et al. Survival in Locally Advanced Pancreatic Cancer After Neoadjuvant Therapy and Surgical Resection. Ann. Surg. 2018, 91. [Google Scholar] [CrossRef] [PubMed]
- Al-Sakere, B.; Bernat, C.; Andre, F.; Connault, E.; Opolon, P.; Davalos, R.V.; Mir, L.M. A study of the immunological response to tumor ablation with irreversible electroporation. Technol. Cancer Res. Treat. 2007, 6, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Napoletano, C.; Taurino, F.; Biffoni, M.; De Majo, A.; Coscarella, G.; Bellati, F.; Rahimi, H.; Pauselli, S.; Pellicciotta, I.; Burchell, J.M.; et al. RFA strongly modulates the immune system and anti-tumor immune responses in metastatic liver patients. Int. J. Oncol. 2008, 32, 481–490. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.; Wen, X.F.; Tian, L.; Li, T.T.; Xu, C.Y.; Wen, X.X.; Melancon, M.P.; Gupta, S.; Shen, B.Z.; Peng, W.Y.; et al. Irreversible electroporation reverses resistance to immune checkpoint blockade in pancreatic cancer. Nat. Commun. 2019, 10, 899. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Alnaggar, M.; Liang, S.; Wang, X.; Liang, Y.; Zhang, M.; Chen, J.; Niu, L.; Xu, K. An important discovery on combination of irreversible electroporation and allogeneic natural killer cell immunotherapy for unresectable pancreatic cancer. Oncotarget 2017, 8, 101795–101807. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dababou, S.; Marrocchio, C.; Rosenberg, J.; Bitton, R.; Pauly, K.B.; Napoli, A.; Hwang, J.H.; Ghanouni, P. A meta-analysis of palliative treatment of pancreatic cancer with high intensity focused ultrasound. J. Ther. Ultrasound 2017, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Sugar, I.P.; Neumann, E. Stochastic model for electric field-induced membrane pores electroporation. Biophys. Chem. 1984, 19, 211–225. [Google Scholar] [CrossRef] [Green Version]
- Beebe, S.J.; Fox, P.M.; Rec, L.J.; Willis, E.L.; Schoenbach, K.H. Nanosecond, high-intensity pulsed electric fields induce apoptosis in human cells. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2003, 17, 1493–1495. [Google Scholar] [CrossRef] [PubMed]
- Davalos, R.V.; Mir, I.L.; Rubinsky, B. Tissue ablation with irreversible electroporation. Ann. Biomed. Eng. 2005, 33, 223–231. [Google Scholar] [CrossRef]
- Miller, L.; Leor, J.; Rubinsky, B. Cancer cells ablation with irreversible electroporation. Technol. Cancer Res. Treat. 2005, 4, 699–705. [Google Scholar] [CrossRef] [PubMed]
- Edd, J.F.; Horowitz, L.; Davalos, R.V.; Mir, L.M.; Rubinsky, B. In vivo results of a new focal tissue ablation technique: Irreversible electroporation. IEEE Trans. Biomed. Eng. 2006, 53, 1409–1415. [Google Scholar] [CrossRef] [PubMed]
- Al-Sakere, B.; Andre, F.; Bernat, C.; Connault, E.; Opolon, P.; Davalos, R.V.; Rubinsky, B.; Mir, L.M. Tumor ablation with irreversible electroporation. PLoS ONE 2007, 2, e1135. [Google Scholar] [CrossRef] [PubMed]
- Daniels, C.; Rubinsky, B. Electrical field and temperature model of nonthermal irreversible electroporation in heterogeneous tissues. J. Biomech. Eng. 2009, 131, 071006. [Google Scholar] [CrossRef] [PubMed]
- Rubinsky, B.; Onik, G.; Mikus, P. Irreversible electroporation: A new ablation modality—Clinical implications. Technol. Cancer Res. Treat. 2007, 6, 37–48. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., II; Kwon, D.; Chalikonda, S.; Sellers, M.; Kotz, E.; Scoggins, C.; McMasters, K.M.; Watkins, K. Treatment of 200 locally advanced (stage III) pancreatic adenocarcinoma patients with irreversible electroporation: Safety and efficacy. Ann. Surg. 2015, 262, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Hosein, P.J.; Beulaygue, I.C.; Froud, T.; Scheffer, H.J.; Venkat, S.R.; Echenique, A.M.; Hevert, E.C.; Livingstone, A.S.; Rocha-Lima, C.M.; et al. Percutaneous Image-Guided Irreversible Electroporation for the Treatment of Unresectable, Locally Advanced Pancreatic Adenocarcinoma. J. Vasc. Interv. Radiol. 2017, 28, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Scheffer, H.J.; Vroomen, L.G.; de Jong, M.C.; Melenhorst, M.C.; Zonderhuis, B.M.; Daams, F.; Vogel, J.A.; Besselink, M.G.; van Kuijk, C.; Witvliet, J.; et al. Ablation of Locally Advanced Pancreatic Cancer with Percutaneous Irreversible Electroporation: Results of the Phase I/II PANFIRE Study. Radiology 2017, 282, 585–597. [Google Scholar] [CrossRef] [Green Version]
- Vogel, J.A.; van Veldhuisen, E.; Agnass, P.; Crezee, J.; Dijk, F.; Verheij, J.; van Gulik, T.M.; Meijerink, M.R.; Vroomen, L.G.; van Lienden, K.P.; et al. Time-Dependent Impact of Irreversible Electroporation on Pancreas, Liver, Blood Vessels and Nerves: A Systematic Review of Experimental Studies. PLoS ONE 2016, 11, e0166987. [Google Scholar] [CrossRef] [PubMed]
- Martin, R.C., II; Durham, A.N.; Besselink, M.G.; Iannitti, D.; Weiss, M.J.; Wolfgang, C.L.; Huang, K.W. Irreversible electroporation in locally advanced pancreatic cancer: A call for standardization of energy delivery. J. Surg. Oncol. 2016, 114, 865–871. [Google Scholar] [CrossRef]
- Scheffer, H.J.; Vogel, J.A.; van den Bos, W.; Neal, R.E., II; van Lienden, K.P.; Besselink, M.G.; van Gemert, M.J.; van der Geld, C.W.; Meijerink, M.R.; Klaessens, J.H.; et al. The Influence of a Metal Stent on the Distribution of Thermal Energy during Irreversible Electroporation. PLoS ONE 2016, 11, e0148457. [Google Scholar] [CrossRef]
- Kluger, M.D.; Epelboym, I.; Schrope, B.A.; Mahendraraj, K.; Hecht, E.M.; Susman, J.; Weintraub, J.L.; Chabot, J.A. Single-Institution Experience with Irreversible Electroporation for T4 Pancreatic Cancer: First 50 Patients. Ann. Surg. Oncol. 2016, 23, 1736–1743. [Google Scholar] [CrossRef] [PubMed]
- Ruarus, A.; Vroomen, L.; Puijk, R.; Scheffer, H.; Meijerink, M. Locally Advanced Pancreatic Cancer: A Review of Local Ablative Therapies. Cancers 2018, 10, 16. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; Crosara, S.; De Robertis, R.; Butturini, G.; Salvia, R.; Paiella, S.; Bassi, C.; Mucelli, R.P. Percutaneous Radiofrequency Ablation of Unresectable Locally Advanced Pancreatic Cancer: Preliminary Results. Technol. Cancer Res. Treat. 2017, 16, 285–294. [Google Scholar] [CrossRef] [PubMed]
- D’Onofrio, M.; Barbi, E.; Girelli, R.; Martone, E.; Gallotti, A.; Salvia, R.; Martini, P.T.; Bassi, C.; Pederzoli, P.; Pozzi Mucelli, R. Radiofrequency ablation of locally advanced pancreatic adenocarcinoma: An overview. World J. Gastroenterol. 2010, 16, 3478–3483. [Google Scholar] [CrossRef] [PubMed]
- U.S. National Library of Medicine. Clinical Trials. Pancreatic Locally Advanced Irresectable Cancer Ablation (PELICAN). Available online: https://clinicaltrials.gov/ct2/show/NCT03690323 (accessed on 1 July 2019).
- Kim, M.S.; Kim, W.; Park, I.H.; Kim, H.J.; Lee, E.; Jung, J.H.; Cho, L.C.; Song, C.W. Radiobiological mechanisms of stereotactic body radiation therapy and stereotactic radiation surgery. Radiat. Oncol. J. 2015, 33, 265–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moningi, S.; Dholakia, A.S.; Raman, S.P.; Blackford, A.; Cameron, J.L.; Le, D.T.; De Jesus-Acosta, A.M.C.; Hacker-Prietz, A.; Rosati, L.M.; Assadi, R.K.; et al. The Role of Stereotactic Body Radiation Therapy for Pancreatic Cancer: A Single-Institution Experience. Ann. Surg. Oncol. 2015, 22, 2352–2358. [Google Scholar] [CrossRef] [PubMed]
- Van Veldhuisen, E.; Walma, M.S.; van Rijssen, L.B.; Busch, O.R.; Bruijnen, R.C.G.; van Delden, O.M.; Haj Mohammad, N.; de Hingh, I.H.; Yo, L.S.; van Laarhoven, H.W.; et al. Added value of intra-operative ultrasound to determine the resectability of locally advanced pancreatic cancer following FOLFIRINOX chemotherapy (IMAGE): A prospective multicenter study. HPB (Oxford) 2019. Epub ahead of print (accessed on 1 July 2019). [Google Scholar] [CrossRef] [PubMed]
- Sanjay, P.; Takaori, K.; Govil, S.; Shrikhande, S.V.; Windsor, J.A. ‘Artery-first’ approaches to pancreatoduodenectomy. Br. J. Surg. 2012, 99, 1027–1035. [Google Scholar] [CrossRef]
- Del Chiaro, M.; Segersvard, R.; Rangelova, E.; Coppola, A.; Scandavini, C.M.; Ansorge, C.; Verbeke, C.; Blomberg, J. Cattell-Braasch Maneuver Combined with Artery-First Approach for Superior Mesenteric-Portal Vein Resection During Pancreatectomy. J. Gastrointest. Surg. 2015, 19, 2264–2268. [Google Scholar] [CrossRef]
- Hackert, T.; Werner, J.; Weitz, J.; Schmidt, J.; Buchler, M.W. Uncinate process first—A novel approach for pancreatic head resection. Langenbecks Arch. Surg. 2010, 395, 1161–1164. [Google Scholar] [CrossRef]
- Weitz, J.; Rahbari, N.; Koch, M.; Buchler, M.W. The “artery first” approach for resection of pancreatic head cancer. J. Am. Coll. Surg. 2010, 210, e1–e4. [Google Scholar] [CrossRef] [PubMed]
- Narayanan, G.; Hosein, P.J.; Arora, G.; Barbery, K.J.; Froud, T.; Livingstone, A.S.; Franceschi, D.; Rocha Lima, C.M.; Yrizarry, J. Percutaneous irreversible electroporation for downstaging and control of unresectable pancreatic adenocarcinoma. J. Vasc. Interv. Radiol. 2012, 23, 1613–1621. [Google Scholar] [CrossRef] [PubMed]
- Klompmaker, S.; Boggi, U.; Hackert, T.; Salvia, R.; Weiss, M.; Yamaue, H.; Zeh, H.J.; Besselink, M.G. Distal Pancreatectomy with Celiac Axis Resection (DP-CAR) for Pancreatic Cancer. How I do It. J. Gastrointest. Surg. 2018, 22, 1804–1810. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klompmaker, S.; de Rooij, T.; Korteweg, J.J.; van Dieren, S.; van Lienden, K.P.; van Gulik, T.M.; Busch, O.R.; Besselink, M.G. Systematic review of outcomes after distal pancreatectomy with coeliac axis resection for locally advanced pancreatic cancer. Br. J. Surg. 2016, 103, 941–949. [Google Scholar] [CrossRef] [PubMed]
- Klompmaker, S.; Peters, N.A.; van Hilst, J.; Bassi, C.; Boggi, U.; Busch, O.R.; Niesen, W.; Van Gulik, T.M.; Javed, A.A.; Kleeff, J.; et al. Outcomes and Risk Score for Distal Pancreatectomy with Celiac Axis Resection (DP-CAR): An International Multicenter Analysis. Ann. Surg. Oncol. 2019, 26, 772–781. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Registry Number | Acronym | Phase | Control | Interventions | Primary Outcome | Sample-Size | Centers | Country |
|---|---|---|---|---|---|---|---|---|
| NCT01827553 [33] | CONKO-007 | III | Chemotherapy alone | Chemoradiation + chemotherapy | OS | 830 | Multicenter | Germany |
| NCT02125136 [34] | NEOLAP | II | Gemcitabine-nab-paclitaxel | FOLFIRINOX | Resectability | 168 | Multicenter | Germany |
| NCT03377491 [35] | PANOVA-3 | III | Gemcitabine–nab-paclitaxel | Gemcitabine–nab-paclitaxel + NovoTTF-100L(P) | OS | 556 | Multicenter | Austria, Canada, France, Italy, Spain, Switzerland, USA |
| NCT02806687 [36] | THERGAP-02 | II | Gemcitabine | Gemcitabine + CYL-02 injection | PFS | 100 | Multicenter | France |
| NCT02791503 [37] | CROSSFIRE | III | Chemotherapy + SABR | Chemotherapy + IRE | OS | 138 | Multicenter | The Netherlands |
| NCT01926197 [38] | PANC0015 | III | mFOLFIRINOX | mFOLFIRINOX + SBRT | PFS | 172 | Multicenter | Canada, USA |
| NTR5517 [39] | PELICAN | III | Chemotherapy only | Chemotherapy + RFA | OS | 228 | Multicenter | The Netherlands |
| Subject | Current Evidence | Future Directions |
|---|---|---|
| Chemotherapy | Promising results are reported for the use of FOLFIRINOX and gemcitabine-nab-paclitaxel as induction treatment of LAPC. It currently remains unknown which of the two regimen is superior as first-line treatment of LAPC. | The results of the ongoing NEOLAP study will assess the superiority of either FOLFIRINOX or gemcitabine-nab-paclitaxel as induction treatment for LAPC. |
| There currently is no consensus on the optimal duration of induction treatment of LAPC. Some centers advocate two months treatment duration, whereas other centers routinely treat patients for four months. This also accounts for the use of adjuvant chemotherapy after initial induction treatment | Future studies should also determine the optimal duration of induction chemotherapy and added value of adjuvant chemotherapy for LAPC after resection. | |
| Response evaluation | Current imaging modalities often underestimate the response of LAPC to induction chemotherapy, as they cannot distinguish fibrosis from vital tumor tissue. Biomarkers may aid in selecting patients with good overall response to chemotherapy but lack specificity. | New response evaluation criteria and/or imaging modalities are required to more accurately determine resectability after induction chemotherapy. |
| The added value of biomarkers to predict response to induction chemotherapy should be established in future studies. | ||
| Surgery | Current evidence on resection of LAPC after induction chemotherapy is promising, but randomized trials confirming the additional value of surgery after chemotherapy are lacking. | Future randomized trials should establish the added value of surgery compared with that of chemotherapy alone in LAPC. |
| Because of the lack of accuracy of current imaging modalities to predict resectability of LAPC, several centers advocate routine surgical exploration in patients with at least stable disease after induction chemotherapy. | The optimal selection criteria for surgical exploration of LAPC after induction chemotherapy should be established. | |
| Neoadjuvant radiotherapy | Some centers perform routine SBRT of LAPC prior to surgical exploration after induction chemotherapy to improve the chance of a radical resection, decrease local recurrence, and improve OS. The added value of this approach has not yet been determined. | The added value of SBRT prior to surgical exploration should be compared with that of chemotherapy alone in patients with LAPC undergoing surgical exploration after induction chemotherapy. |
| Ablative therapies | Local ablative therapies are considered in some centers in patients with persistent LAPC after induction chemotherapy. Randomized trials to determine the added value of ablative therapies to chemotherapy-alone are lacking. | The results of the currently ongoing PELICAN trial will assess the added value of RFA to chemotherapy-alone. |
| Currently there are no completed trials comparing multiple ablative modalities. Therefore, the superiority of either technique (IRE, RFA, SBRT) remains unknown. | The ongoing CROSSFIRE trial will determine the superiority of either IRE or SABR in patients with LAPC after induction chemotherapy. Future comparative studies are needed to determine the most effective local ablative treatment in LAPC. | |
| There is increasing evidence that local ablative therapies can induce a systemic anti-tumor response (i.e., abscopal effect). It is suggested to combine local treatment with immunotherapy to both increase local-and distant disease control | Future studies should focus on combining local ablative therapy with (systemic) immunotherapy. |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Veldhuisen, E.; van den Oord, C.; Brada, L.J.; Walma, M.S.; Vogel, J.A.; Wilmink, J.W.; del Chiaro, M.; van Lienden, K.P.; Meijerink, M.R.; van Tienhoven, G.; et al. Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies. Cancers 2019, 11, 976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070976
van Veldhuisen E, van den Oord C, Brada LJ, Walma MS, Vogel JA, Wilmink JW, del Chiaro M, van Lienden KP, Meijerink MR, van Tienhoven G, et al. Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies. Cancers. 2019; 11(7):976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070976
Chicago/Turabian Stylevan Veldhuisen, Eran, Claudia van den Oord, Lilly J. Brada, Marieke S. Walma, Jantien A. Vogel, Johanna W. Wilmink, Marco del Chiaro, Krijn P. van Lienden, Martijn R. Meijerink, Geertjan van Tienhoven, and et al. 2019. "Locally Advanced Pancreatic Cancer: Work-Up, Staging, and Local Intervention Strategies" Cancers 11, no. 7: 976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11070976