A Novel Predictor Tool of Biochemical Recurrence after Radical Prostatectomy Based on a Five-MicroRNA Tissue Signature


Abstract
:1. Introduction
2. Results
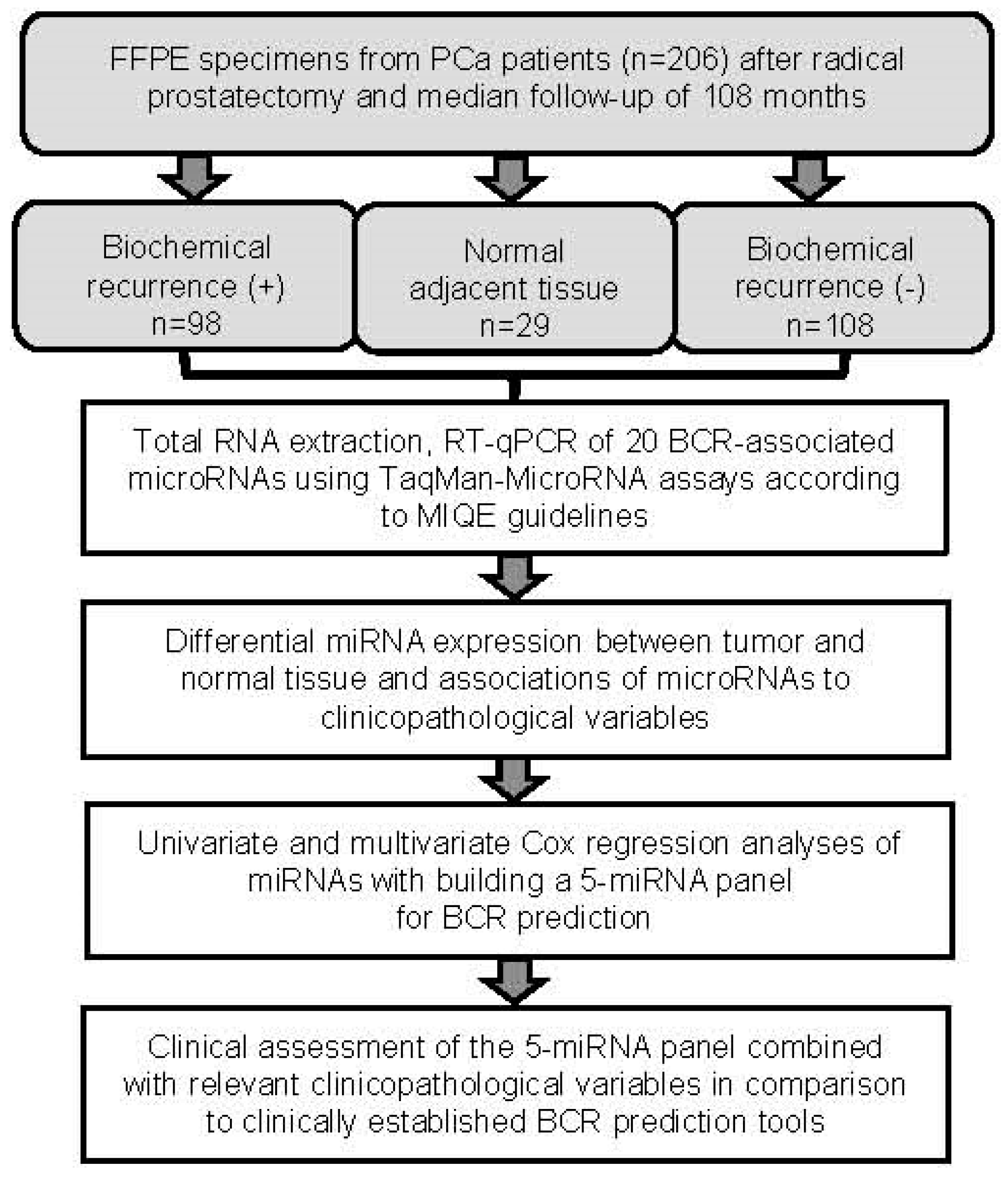
2.1. Patient Characteristics and Flow Chart of the Study
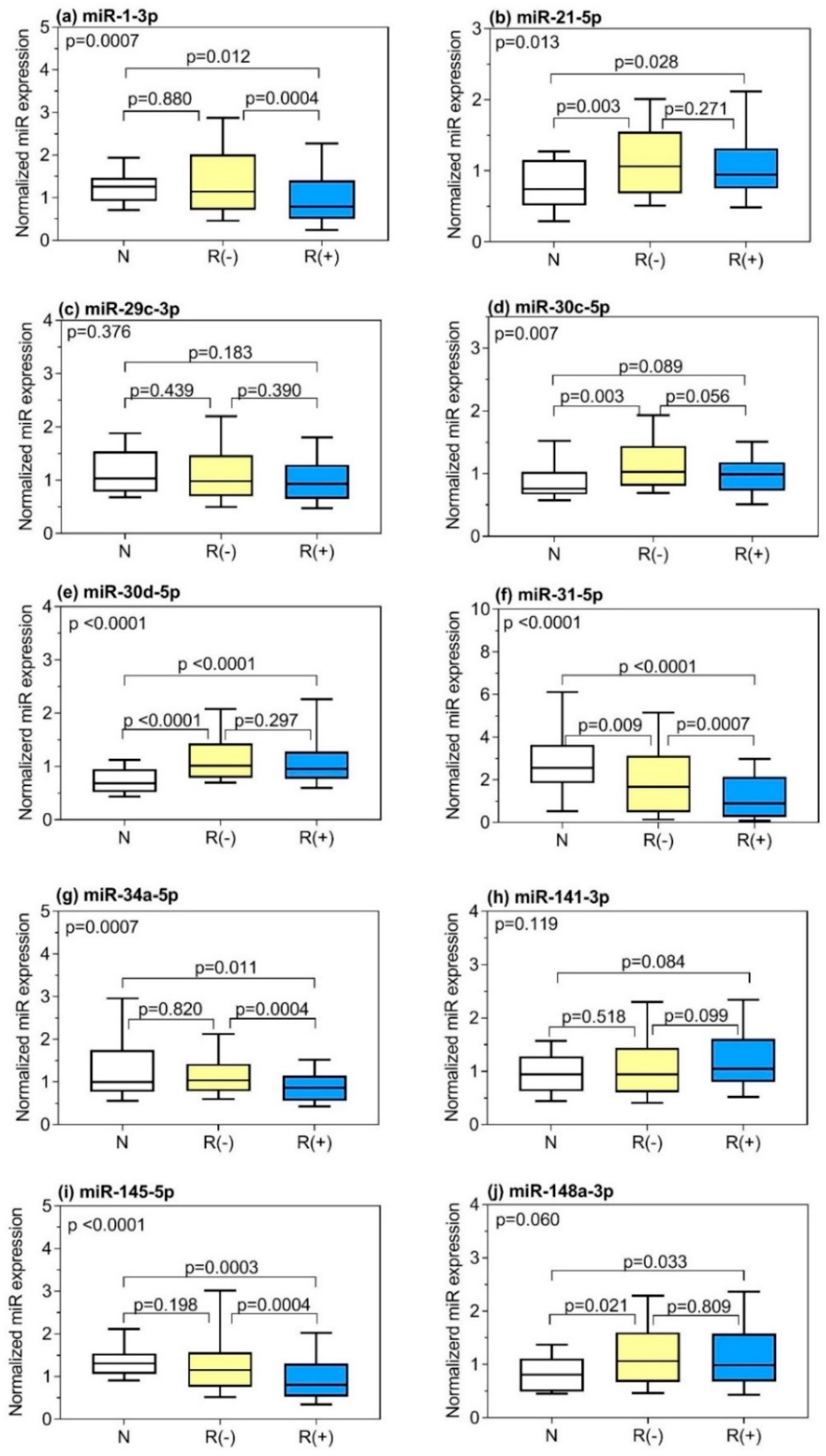
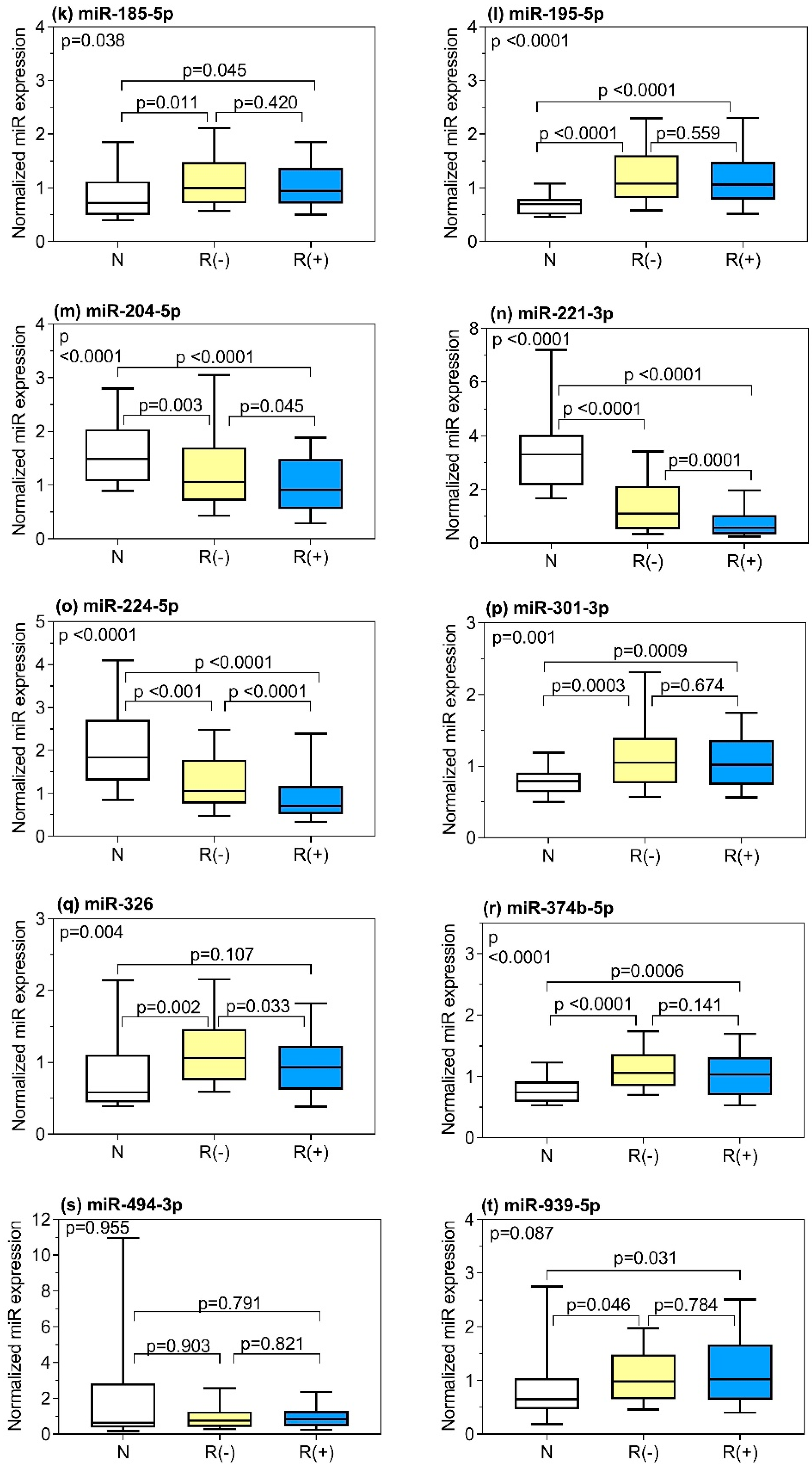
2.2. Selection of BCR-Related miRNAs and Their Differential Expression between Tumor and Normal Tissue and between the Samples from Patients with and without BCR
2.3. Correlations of Clinicopathological Variables with miRNAs and Correlations between miRNAs
2.4. Prognostic Potential of miRNAs Predicting BCR
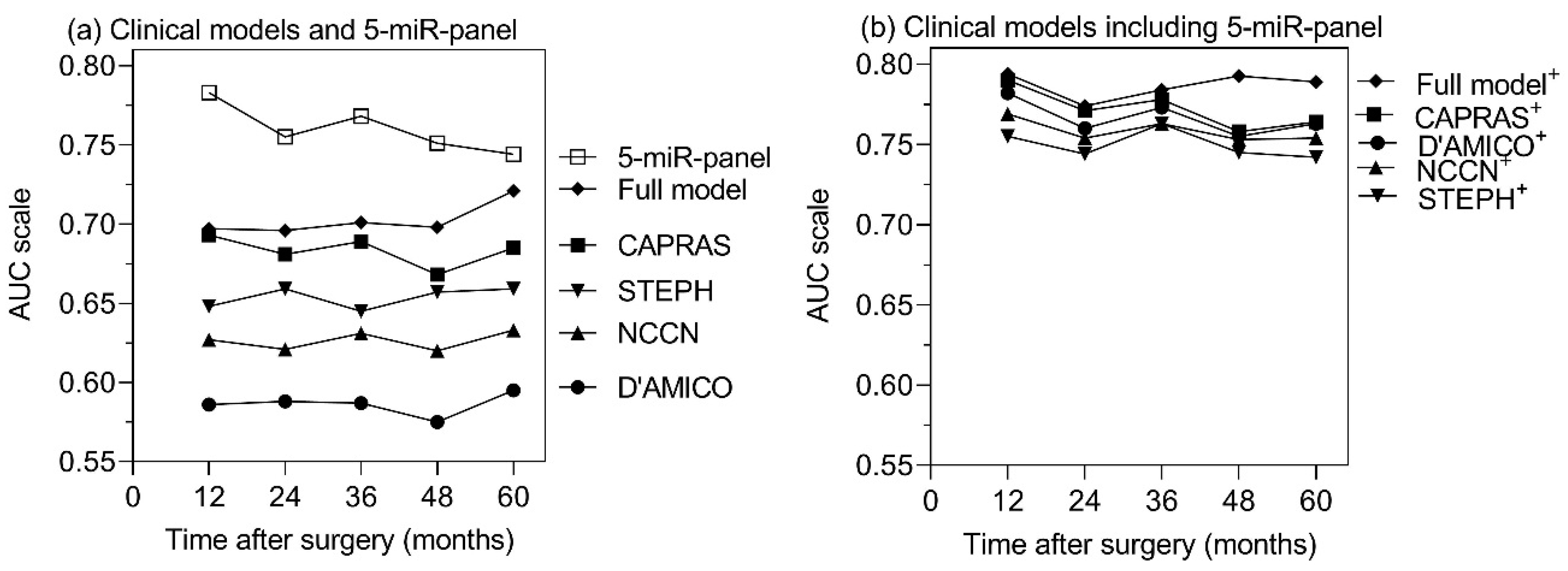
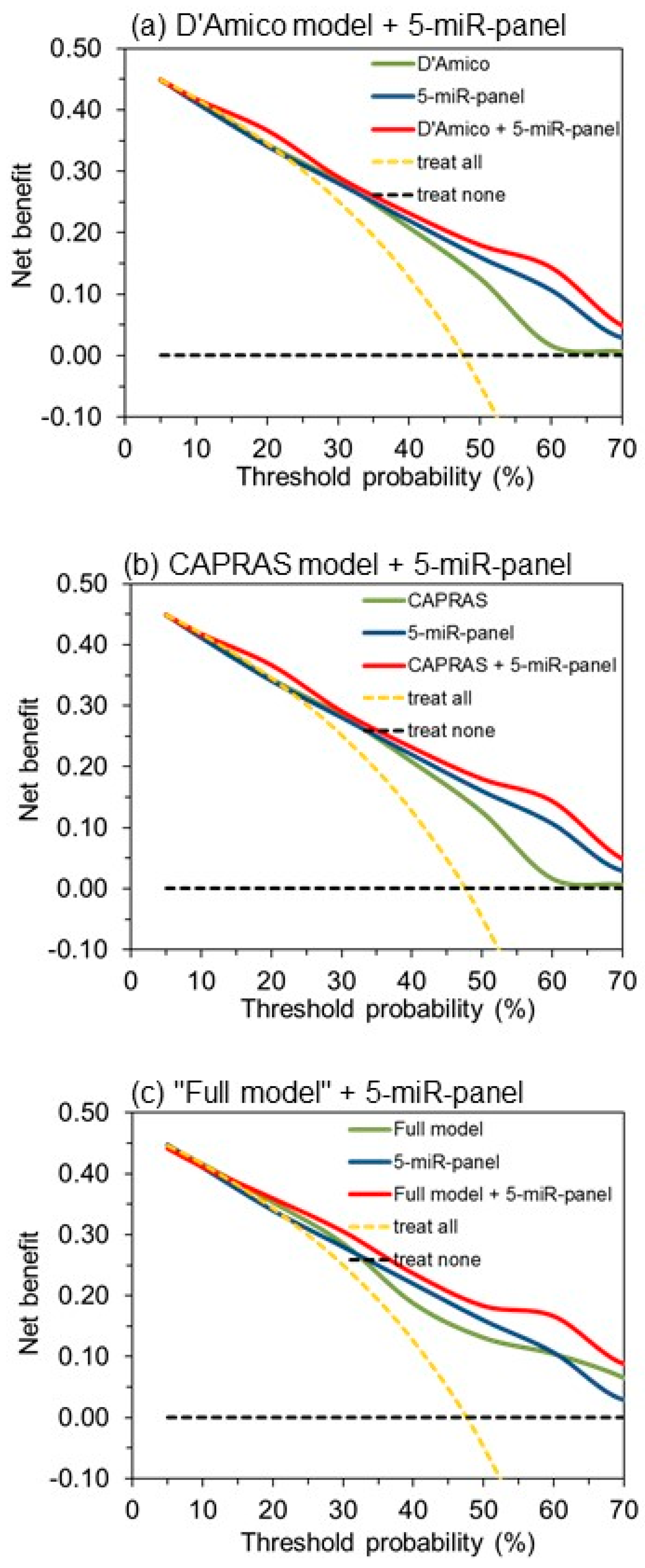
2.5. 5-miR-Panel Outperformed Models Based only on Clinicopathological Variables in Predicting BCR
2.6. Functional Links Between miRNAs of the 5-miR-Panel and Prostate Cancer
3. Discussion
4. Materials and Methods
4.1. Patient Selection and Data Collection
4.2. RNA Extraction and Reverse Transcription Quantitative Real-Time Polymerase Chain Reaction (RT-qPCR)
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: Globocan estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.; Cammann, H.; Meyer, H.-A.; Jung, K.; Lu, H.; Leva, N.; Magheli, A.; Stephan, C.; Busch, J. Risk prediction models for biochemical recurrence after radical prostatectomy using prostate-specific anitigen and Gleason score. Asian J. Androl. 2014, 16, 897–901. [Google Scholar] [PubMed]
- Tilki, D.; Mandel, P.; Schlomm, T.; Chun, F.K.; Tennstedt, P.; Pehrke, D.; Haese, A.; Huland, H.; Graefen, M.; Salomon, G. External validation of the CAPRA-S score to predict biochemical recurrence, metastasis and mortality after radical prostatectomy in a European cohort. J. Urol. 2015, 193, 1970–1975. [Google Scholar] [CrossRef] [PubMed]
- Liesenfeld, L.; Kron, M.; Gschwend, J.E.; Herkommer, K. Prognostic Factors for Biochemical Recurrence More than 10 Years after Radical Prostatectomy. J. Urol. 2017, 197, 143–148. [Google Scholar] [CrossRef]
- Ludwig, W.W.; Feng, Z.; Trock, B.J.; Humphreys, E.; Walsh, P.C. Prostate specific antigen testing after radical prostatectomy—Can we stop at 20 years? J. Urol. 2018, 199, 114–119. [Google Scholar] [CrossRef]
- Pak, S.; You, D.; Jeong, I.G.; Kim, Y.S.; Hong, J.H.; Kim, C.S.; Ahn, H. Time to biochemical relapse after radical prostatectomy and efficacy of salvage radiotherapy in patients with prostate cancer. Int. J. Clin. Oncol. 2019, 24, 1238–1246. [Google Scholar] [CrossRef]
- Loeb, S.; Zhu, X.; Schröder, F.H.; Roobol, M.J. Long-term radical prostatectomy outcomes among participants from the European Randomized Study of Screening for Prostate Cancer (ERSPC) Rotterdam. BJU Int. 2012, 110, 1678–1683. [Google Scholar] [CrossRef]
- Cornford, P.; Bellmunt, J.; Bolla, M.; Briers, E.; De Santis, M.; Gross, T.; Henry, A.M.; Joniau, S.; Lam, T.B.; Mason, M.D.; et al. EAU-ESTRO-SIOG Guidelines on Prostate Cancer. Part II: Treatment of relapsing, metastatic, and castration-resistant prostate cancer. Eur. Urol. 2017, 71, 630–642. [Google Scholar] [CrossRef]
- Cookson, M.S.; Aus, G.; Burnett, A.L.; Canby-Hagino, E.D.; D’Amico, A.V.; Dmochowski, R.R.; Eton, D.T.; Forman, J.D.; Goldenberg, S.L.; Hernandez, J.; et al. Variation in the definition of biochemical recurrence in patients treated for localized prostate cancer: The American Urological Association Prostate Guidelines for Localized Prostate Cancer Update Panel report and recommendations for a standard in the reporting of surgical outcomes. J. Urol. 2007, 177, 540–545. [Google Scholar]
- Stephenson, A.J.; Kattan, M.W.; Eastham, J.A.; Dotan, Z.A.; Bianco, F.J.; Lilja, H.; Scardino, P.T. Defining biochemical recurrence of prostate cancer after radical prostatectomy: A proposal for a standardized definition. J. Clin. Oncol. 2006, 24, 3973–3978. [Google Scholar] [CrossRef]
- Tourinho-Barbosa, R.; Srougi, V.; Nunes-Silva, I.; Baghdadi, M.; Rembeyo, G.; Eiffel, S.S.; Barret, E.; Rozet, F.; Galiano, M.; Cathelineau, X.; et al. Biochemical recurrence after radical prostatectomy: What does it mean? Int. Braz. J. Urol 2018, 44, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Van den Broeck, T.; van den Bergh, R.C.N.; Arfi, N.; Gross, T.; Moris, L.; Briers, E.; Cumberbatch, M.; De, S.M.; Tilki, D.; Fanti, S.; et al. Prognostic value of biochemical recurrence following treatment with curative intent for prostate cancer: A systematic review. Eur. Urol. 2019, 75, 967–987. [Google Scholar] [CrossRef] [PubMed]
- Pound, C.R.; Partin, A.W.; Eisenberger, M.A.; Chan, D.W.; Pearson, J.D.; Walsh, P.C. Natural history of progression after PSA elevation following radical prostatectomy. JAMA 1999, 281, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Brockman, J.A.; Alanee, S.; Vickers, A.J.; Scardino, P.T.; Wood, D.P.; Kibel, A.S.; Lin, D.W.; Bianco, F.J.; Rabah, D.M.; Klein, E.A.; et al. Nomogram predicting prostate cancer-specific mortality for men with biochemical recurrence after radical prostatectomy. Eur. Urol. 2015, 67, 1160–1167. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Pasta, D.J.; Elkin, E.P.; Litwin, M.S.; Latini, D.M.; Du Chane, J.; Carroll, P.R. The University of California, San Francisco Cancer of the Prostate Risk Assessment score: A straightforward and reliable preoperative predictor of disease recurrence after radical prostatectomy. J. Urol. 2005, 173, 1938–1942. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Scardino, P.T.; Eastham, J.A.; Bianco, F.J.; Dotan, Z.A.; DiBlasio, C.J.; Reuther, A.; Klein, E.A.; Kattan, M.W. Postoperative nomogram predicting the 10-year probability of prostate cancer recurrence after radical prostatectomy. J. Clin. Oncol. 2005, 23, 7005–7012. [Google Scholar] [CrossRef]
- Mohler, J.L. The 2010 NCCN clinical practice guidelines in oncology on prostate cancer. J. Natl. Compr. Cancer Netw. 2010, 8, 145. [Google Scholar] [CrossRef]
- Remmers, S.; Verbeek, J.F.M.; Noeboer, D.; van der Kwast, T.; Roobol, M.J. Predicting biochemical recurrence and prostate cancer specific mortality after radical prostatectomy: Comparison of six prediction models in a cohort of screen and clinically detected prostate cancer patients. BJU Int. 2019, 124, 635–642. [Google Scholar] [CrossRef]
- Shariat, S.F.; Karakiewicz, P.I.; Suardi, N.; Kattan, M.W. Comparison of nomograms with other methods for predicting outcomes in prostate cancer: A critical analysis of the literature. Clin. Cancer Res. 2008, 14, 4400–4407. [Google Scholar] [CrossRef]
- Kang, M.; Jeong, C.W.; Choi, W.S.; Park, Y.H.; Cho, S.Y.; Lee, S.; Lee, S.B.; Ku, J.H.; Hong, S.K.; Byun, S.S.; et al. Pre- and post-operative nomograms to predict recurrence-free probability in korean men with clinically localized prostate cancer. PLoS ONE 2014, 9, e100053. [Google Scholar] [CrossRef] [PubMed]
- Goodman, M.; Ward, K.C.; Osunkoya, A.O.; Datta, M.W.; Luthringer, D.; Young, A.N.; Marks, K.; Cohen, V.; Kennedy, J.C.; Haber, M.J.; et al. Frequency and determinants of disagreement and error in gleason scores: A population-based study of prostate cancer. Prostate 2012, 72, 1389–1398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jung, J.W.; Lee, J.K.; Hong, S.K.; Byun, S.S.; Lee, S.E. Stratification of patients with intermediate-risk prostate cancer. BJU Int. 2015, 115, 907–912. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siadat, F.; Sykes, J.; Zlotta, A.R.; Aldaoud, N.; Egawa, S.; Pushkar, D.; Kuk, C.; Bristow, R.G.; Montironi, R.; van der Kwast, T. Not all gleason pattern 4 prostate cancers are created equal: A study of latent prostatic carcinomas in a cystoprostatectomy and autopsy series. Prostate 2015, 75, 1277–1284. [Google Scholar] [CrossRef] [PubMed]
- Lorent, M.; Maalmi, H.; Tessier, P.; Supiot, S.; Dantan, E.; Foucher, Y. Meta-analysis of predictive models to assess the clinical validity and utility for patient-centered medical decision making: Application to the CAncer of the Prostate Risk Assessment (CAPRA). BMC Med. Inform. Decis. Mak. 2019, 19, 2. [Google Scholar] [CrossRef] [PubMed]
- Meurs, P.; Galvin, R.; Fanning, D.M.; Fahey, T. Prognostic value of the CAPRA clinical prediction rule: A systematic review and meta-analysis. BJU Int. 2013, 111, 427–436. [Google Scholar] [CrossRef] [PubMed]
- Hiser, W.M.; Sangiorgio, V.; Bollito, E.; Esnakula, A.; Feely, M.; Falzarano, S.M. Tissue-based multigene expression tests for pretreatment prostate cancer risk assessment: Current status and future perspectives. Future Oncol. 2018, 14, 3073–3083. [Google Scholar] [CrossRef]
- Spratt, D.E.; Zhang, J.; Santiago-Jimenez, M.; Dess, R.T.; Davis, J.W.; Den, R.B.; Dicker, A.P.; Kane, C.J.; Pollack, A.; Stoyanova, R.; et al. Development and validation of a novel integrated clinical-genomic risk group classification for localized prostate cancer. J. Clin. Oncol. 2018, 36, 581–590. [Google Scholar] [CrossRef]
- Ross, A.E.; Johnson, M.H.; Yousefi, K.; Davicioni, E.; Netto, G.J.; Marchionni, L.; Fedor, H.L.; Glavaris, S.; Choeurng, V.; Buerki, C.; et al. Tissue-based genomics augments post-prostatectomy risk stratification in a natural history cohort of intermediate- and high-risk men. Eur. Urol. 2016, 69, 157–165. [Google Scholar] [CrossRef]
- Fine, N.D.; LaPolla, F.; Epstein, M.; Loeb, S.; Dani, H. Genomic classifiers for treatment selection in newly diagnosed prostate cancer. BJU Int. 2019, 124, 574–586. [Google Scholar] [CrossRef]
- Bell, E.H.; Kirste, S.; Fleming, J.L.; Stegmaier, P.; Drendel, V.; Mo, X.; Ling, S.; Fabian, D.; Manring, I.; Jilg, C.A.; et al. A novel miRNA-based predictive model for biochemical failure following post-prostatectomy salvage radiation therapy. PLoS ONE 2015, 10, e0118745. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Jung, M.; Stephan, C.; Honey, R.J.; Stewart, R.J.; Pace, K.T.; Erbersdobler, A.; Samaan, S.; Jung, K.; Yousef, G.M. miRNAs can predict prostate cancer biochemical relapse and are involved in tumor progression. Int. J. Oncol. 2011, 39, 1183–1192. [Google Scholar] [PubMed]
- Kristensen, H.; Thomsen, A.R.; Haldrup, C.; Dyrskjot, L.; Hoyer, S.; Borre, M.; Mouritzen, P.; Orntoft, T.F.; Sorensen, K.D. Novel diagnostic and prognostic classifiers for prostate cancer identified by genome-wide microRNA profiling. Oncotarget 2016, 7, 30760–30771. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.W.; Stephan, C.; Weickmann, S.; Jung, M.; Kristiansen, G.; Jung, K. Tissue-based microRNAs as predictors of biochemical recurrence after radical prostatectomy: What can we learn from past studies? Int. J. Mol. Sci. 2017, 18, 2023. [Google Scholar] [CrossRef]
- Karatas, O.F.; Guzel, E.; Suer, I.; Ekici, I.D.; Caskurlu, T.; Creighton, C.J.; Ittmann, M.; Ozen, M. miR-1 and miR-133b are differentially expressed in patients with recurrent prostate cancer. PLoS ONE 2014, 9, e98675. [Google Scholar] [CrossRef]
- Bovelstad, H.M.; Nygard, S.; Borgan, O. Survival prediction from clinico-genomic models—A comparative study. BMC Bioinform. 2009, 10, 413. [Google Scholar] [CrossRef]
- Cooperberg, M.R.; Davicioni, E.; Crisan, A.; Jenkins, R.B.; Ghadessi, M.; Karnes, R.J. Combined value of validated clinical and genomic risk stratification tools for predicting prostate cancer mortality in a high-risk prostatectomy cohort. Eur. Urol. 2015, 67, 326–333. [Google Scholar] [CrossRef]
- Nam, R.K.; Amemiya, Y.; Benatar, T.; Wallis, C.J.; Stojcic-Bendavid, J.; Bacopulos, S.; Sherman, C.; Sugar, L.; Naeim, M.; Yang, W.; et al. Five microRNA signature predictive of prostate cancer recurrence and metastasis: A cohort study. J. Cancer 2015, 6, 1160–1171. [Google Scholar] [CrossRef]
- Sauerbrei, W.; Taube, S.E.; McShane, L.M.; Cavenagh, M.M.; Altman, D.G. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): An abridged explanation and elaboration. J. Natl. Cancer Inst. 2018, 110, 803–811. [Google Scholar] [CrossRef]
- Wei, W.; Leng, J.; Shao, H.; Wang, W. MiR-1, a potential predictive biomarker for recurrence in prostate cancer after radical prostatectomy. Am. J. Med. Sci. 2017, 353, 315–319. [Google Scholar] [CrossRef]
- Hudson, R.S.; Yi, M.; Esposito, D.; Watkins, S.K.; Hurwitz, A.A.; Yfantis, H.G.; Lee, D.H.; Borin, J.F.; Naslund, M.J.; Alexander, R.B.; et al. MicroRNA-1 is a candidate tumor suppressor and prognostic marker in human prostate cancer. Nucleic Acids Res. 2012, 40, 3689–3703. [Google Scholar] [CrossRef] [PubMed]
- Leite, K.R.; Reis, S.T.; Viana, N.; Morais, D.R.; Moura, C.M.; Silva, I.A.; Pontes, J.; Katz, B.; Srougi, M. Controlling RECK miR21 promotes tumor cell invasion and is related to biochemical recurrence in prostate cancer. J. Cancer 2015, 6, 292–301. [Google Scholar] [CrossRef] [PubMed]
- Melbo-Jorgensen, C.; Ness, N.; Andersen, S.; Valkov, A.; Donnem, T.; Al-Saad, S.; Kiselev, Y.; Berg, T.; Nordby, Y.; Bremnes, R.M.; et al. Stromal expression of MiR-21 predicts biochemical failure in prostate cancer patients with Gleason score 6. PLoS ONE 2014, 9, e113039. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Li, R.S.; Li, Y.H.; Zhong, S.; Chen, Y.Y.; Zhang, C.M.; Hu, M.M.; Shen, Z.J. miR-21 as an independent biochemical recurrence predictor and potential therapeutic target for prostate cancer. J. Urol. 2012, 187, 1466–1472. [Google Scholar] [CrossRef]
- Zheng, Q.; Peskoe, S.B.; Ribas, J.; Rafiqi, F.; Kudrolli, T.; Meeker, A.K.; De Marzo, A.M.; Platz, E.A.; Lupold, S.E. Investigation of miR-21, miR-141, and miR-221 expression levels in prostate adenocarcinoma for associated risk of recurrence after radical prostatectomy. Prostate 2014, 74, 1655–1662. [Google Scholar] [CrossRef] [Green Version]
- Amankwah, E.K.; Anegbe, E.; Park, H.; Pow-Sang, J.; Hakam, A.; Park, J.Y. miR-21, miR-221 and miR-222 expression and prostate cancer recurrence among obese and non-obese cases. Asian J. Androl. 2013, 15, 226–230. [Google Scholar] [CrossRef] [Green Version]
- Lichner, Z.; Ding, Q.; Samaan, S.; Saleh, C.; Nasser, A.; Al-Haddad, S.; Samuel, J.N.; Fleshner, N.E.; Stephan, C.; Jung, K.; et al. miRNAs dysregulated in association with Gleason grade regulate extracellular matrix, cytoskeleton and androgen receptor pathways. J. Pathol. 2015, 237, 226–237. [Google Scholar] [CrossRef]
- Li, J.; Fu, F.; Wan, X.; Huang, S.; Wu, D.; Li, Y. Up-regulated miR-29c inhibits cell proliferation and glycolysis by inhibiting SLC2A3 expression in prostate cancer. Gene 2018, 665, 26–34. [Google Scholar] [CrossRef]
- Kato, M.; Kurozumi, A.; Goto, Y.; Matsushita, R.; Okato, A.; Nishikawa, R.; Fukumoto, I.; Koshizuka, K.; Ichikawa, T.; Seki, N. Regulation of metastasis-promoting LOXL2 gene expression by antitumor microRNAs in prostate cancer. J. Hum. Genet. 2017, 62, 123–132. [Google Scholar] [CrossRef]
- Ling, X.H.; Han, Z.D.; Xia, D.; He, H.C.; Jiang, F.N.; Lin, Z.Y.; Fu, X.; Deng, Y.H.; Dai, Q.S.; Cai, C.; et al. MicroRNA-30c serves as an independent biochemical recurrence predictor and potential tumor suppressor for prostate cancer. Mol. Biol. Rep. 2014, 41, 2779–2788. [Google Scholar] [CrossRef]
- Ling, X.H.; Chen, Z.Y.; Luo, H.W.; Liu, Z.Z.; Liang, Y.K.; Chen, G.X.; Jiang, F.N.; Zhong, W.D. BCL9, a coactivator for Wnt/-catenin transcription, is targeted by miR-30c and is associated with prostate cancer progression. Oncol. Lett. 2016, 11, 2001–2008. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Uemura, H.; Nagahama, K.; Okudela, K.; Furuya, M.; Ino, Y.; Ito, Y.; Hirano, H.; Inayama, Y.; Aoki, I.; et al. Identification of miR-30d as a novel prognostic maker of prostate cancer. Oncotarget 2012, 3, 1455–1471. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.Y.; Chen, G.; Zhang, Y.Q.; He, H.C.; Liang, Y.X.; Ye, J.H.; Liang, Y.K.; Mo, R.J.; Lu, J.M.; Zhuo, Y.J.; et al. MicroRNA-30d promotes angiogenesis and tumor growth via MYPT1/c-JUN/VEGFA pathway and predicts aggressive outcome in prostate cancer. Mol. Cancer 2017, 16, 48. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.; Jung, M.; Mollenkopf, H.-J.; Wagner, I.; Stephan, C.; Jentzmik, F.; Miller, K.; Lein, M.; Kristiansen, G.; Jung, K. Diagnostic and prognostic implications of microRNA profiling in prostate carcinoma. Int. J. Cancer 2010, 126, 1166–1176. [Google Scholar] [CrossRef]
- Daniunaite, K.; Dubikaityte, M.; Gibas, P.; Bakavicius, A.; Rimantas, L.J.; Ulys, A.; Jankevicius, F.; Jarmalaite, S. Clinical significance of miRNA host gene promoter methylation in prostate cancer. Hum. Mol. Genet. 2017, 26, 2451–2461. [Google Scholar] [CrossRef]
- Liu, X.; Luo, X.; Wu, Y.; Xia, D.; Chen, W.; Fang, Z.; Deng, J.; Hao, Y.; Yang, X.; Zhang, T.; et al. MicroRNA-34a attenuates paclitaxel resistance in prostate cancer cells via direct suppression of JAG1/Notch1 Axis. Cell Physiol. Biochem. 2018, 50, 261–276. [Google Scholar] [CrossRef]
- Song, C.J.; Chen, H.; Chen, L.Z.; Ru, G.M.; Guo, J.J.; Ding, Q.N. The potential of microRNAs as human prostate cancer biomarkers: A meta-analysis of related studies. J. Cell Biochem. 2018, 119, 2763–2786. [Google Scholar] [CrossRef]
- Avgeris, M.; Stravodimos, K.; Fragoulis, E.G.; Scorilas, A. The loss of the tumour-suppressor miR-145 results in the shorter disease-free survival of prostate cancer patients. Br. J. Cancer 2013, 108, 2573–2581. [Google Scholar] [CrossRef] [Green Version]
- Kang, S.G.; Ha, Y.R.; Kim, S.J.; Kang, S.H.; Park, H.S.; Lee, J.G.; Cheon, J.; Kim, C.H. Do microRNA 96, 145 and 221 expressions really aid in the prognosis of prostate carcinoma? Asian J. Androl. 2012, 14, 752–757. [Google Scholar] [CrossRef] [Green Version]
- Larne, O.; Martens-Uzunova, E.; Hagman, Z.; Edsjo, A.; Lippolis, G.; den Berg, M.S.; Bjartell, A.; Jenster, G.; Ceder, Y. miQ—A novel microRNA based diagnostic and prognostic tool for prostate cancer. Int. J. Cancer 2013, 132, 2867–2875. [Google Scholar] [CrossRef]
- Leite, K.R.; Tomiyama, A.; Reis, S.T.; Sousa-Canavez, J.M.; Sanudo, A.; Dall’Oglio, M.F.; Camara-Lopes, L.H.; Srougi, M. MicroRNA-100 expression is independently related to biochemical recurrence of prostate cancer. J. Urol. 2011, 185, 1118–1122. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.; Li, Z.; Zhang, L.; Xu, Z. MEF2 activated long noncoding RNA PCGEM1 promotes cell proliferation in hormonerefractory prostate cancer through downregulation of miR148a. Mol. Med. Rep. 2018, 18, 202–208. [Google Scholar] [PubMed]
- Guo, J.; Wang, M.; Liu, X. MicroRNA-195 suppresses tumor cell proliferation and metastasis by directly targeting BCOX1 in prostate carcinoma. J. Exp. Clin. Cancer Res. 2015, 34, 91. [Google Scholar] [CrossRef] [PubMed]
- Cai, C.; Chen, Q.B.; Han, Z.D.; Zhang, Y.Q.; He, H.C.; Chen, J.H.; Chen, Y.R.; Yang, S.B.; Wu, Y.D.; Zeng, Y.R.; et al. miR-195 inhibits tumor progression by targeting RPS6KB1 in human prostate cancer. Clin. Cancer Res. 2015, 21, 4922–4934. [Google Scholar] [CrossRef] [PubMed]
- Todorova, K.; Metodiev, M.V.; Metodieva, G.; Zasheva, D.; Mincheff, M.; Hayrabedyan, S. miR-204 is dysregulated in metastatic prostate cancer in vitro. Mol. Carcinog. 2016, 55, 131–147. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.; Chen, F.; Shen, L.; Tang, X.; Du, C.; Sun, Z.; Ding, H.; Chen, J.; Shen, B. Biomarker microRNAs for prostate cancer metastasis: Screened with a network vulnerability analysis model. J. Transl. Med. 2018, 16, 134. [Google Scholar] [CrossRef]
- Spahn, M.; Kneitz, S.; Scholz, C.J.; Stenger, N.; Rudiger, T.; Strobel, P.; Riedmiller, H.; Kneitz, B. Expression of microRNA-221 is progressively reduced in aggressive prostate cancer and metastasis and predicts clinical recurrence. Int. J. Cancer 2010, 127, 394–403. [Google Scholar]
- Lin, Z.Y.; Huang, Y.Q.; Zhang, Y.Q.; Han, Z.D.; He, H.C.; Ling, X.H.; Fu, X.; Dai, Q.S.; Cai, C.; Chen, J.H.; et al. MicroRNA-224 inhibits progression of human prostate cancer by downregulating TRIB1. Int. J. Cancer 2014, 135, 541–550. [Google Scholar] [CrossRef]
- Wan, Y.; Zeng, Z.C.; Xi, M.; Wan, S.; Hua, W.; Liu, Y.L.; Zhou, Y.L.; Luo, H.W.; Jiang, F.N.; Zhong, W.D. Dysregulated microRNA-224/apelin axis associated with aggressive progression and poor prognosis in patients with prostate cancer. Hum. Pathol. 2015, 46, 295–303. [Google Scholar] [CrossRef]
- Nam, R.K.; Benatar, T.; Wallis, C.J.; Amemiya, Y.; Yang, W.; Garbens, A.; Naeim, M.; Sherman, C.; Sugar, L.; Seth, A. MiR-301a regulates E-cadherin expression and is predictive of prostate cancer recurrence. Prostate 2016, 76, 869–884. [Google Scholar] [CrossRef]
- He, H.C.; Han, Z.D.; Dai, Q.S.; Ling, X.H.; Fu, X.; Lin, Z.Y.; Deng, Y.H.; Qin, G.Q.; Cai, C.; Chen, J.H.; et al. Global analysis of the differentially expressed miRNAs of prostate cancer in Chinese patients. BMC Genom. 2013, 14, 757. [Google Scholar] [CrossRef] [PubMed]
- Bian, H.; Zhou, Y.; Zhou, D.; Zhang, Y.; Shang, D.; Qi, J. The latest progress on miR-374 and its functional implications in physiological and pathological processes. J. Cell. Mol. Med. 2019, 23, 3063–3076. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Sun, C.; Wang, L.; Xu, M.; Zang, Y.; Zhou, Y.; Liu, X.; Tao, W.; Xue, B.; Shan, Y.; et al. Targeting survivin using a combination of miR494 and survivin shRNA has synergistic effects on the suppression of prostate cancer growth. Mol. Med. Rep. 2016, 13, 1602–1610. [Google Scholar] [CrossRef] [PubMed]
- Shen, P.F.; Chen, X.Q.; Liao, Y.C.; Chen, N.; Zhou, Q.; Wei, Q.; Li, X.; Wang, J.; Zeng, H. MicroRNA-494-3p targets CXCR4 to suppress the proliferation, invasion, and migration of prostate cancer. Prostate 2014, 74, 756–767. [Google Scholar] [CrossRef] [PubMed]
- Guo, K.; Liang, Z.; Li, F.; Wang, H. Comparison of miRNA and gene expression profiles between metastatic and primary prostate cancer. Oncol. Lett. 2017, 14, 6085–6090. [Google Scholar] [CrossRef] [PubMed]
- Pashaei, E.; Pashaei, E.; Ahmady, M.; Ozen, M.; Aydin, N. Meta-analysis of miRNA expression profiles for prostate cancer recurrence following radical prostatectomy. PLoS ONE 2017, 12, e0179543. [Google Scholar] [CrossRef] [PubMed]
- Heagerty, P.J.; Zheng, Y. Survival model predictive accuracy and ROC curves. Biometrics 2005, 61, 92–105. [Google Scholar] [CrossRef]
- Steyerberg, E.W.; Pencina, M.J.; Lingsma, H.F.; Kattan, M.W.; Vickers, A.J.; Van, C.B. Assessing the incremental value of diagnostic and prognostic markers: A review and illustration. Eur. J. Clin. Investig. 2012, 42, 216–228. [Google Scholar] [CrossRef]
- Huang, Y.Q.; Ling, X.H.; Yuan, R.Q.; Chen, Z.Y.; Yang, S.B.; Huang, H.X.; Zhong, W.D.; Qiu, S.P. miR30c suppresses prostate cancer survival by targeting the ASF/SF2 splicing factor oncoprotein. Mol. Med. Rep. 2017, 16, 2431–2438. [Google Scholar] [CrossRef]
- Zhang, J.; Wang, X.; Wang, Y.; Peng, R.; Lin, Z.; Wang, Y.; Hu, B.; Wang, J.; Shi, G. Low expression of microRNA-30c promotes prostate cancer cells invasion involved in downregulation of KRAS protein. Oncol. Lett. 2017, 14, 363–368. [Google Scholar] [CrossRef]
- Zhang, Q.; Sun, M.; Zhou, S.; Guo, B. Class I HDAC inhibitor mocetinostat induces apoptosis by activation of miR-31 expression and suppression of E2F6. Cell Death Discov. 2016, 2, 16036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coarfa, C.; Fiskus, W.; Eedunuri, V.K.; Rajapakshe, K.; Foley, C.; Chew, S.A.; Shah, S.S.; Geng, C.; Shou, J.; Mohamed, J.S.; et al. Comprehensive proteomic profiling identifies the androgen receptor axis and other signaling pathways as targets of microRNAs suppressed in metastatic prostate cancer. Oncogene 2016, 35, 2345–2356. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Qi, M.; Feng, T.; Hu, J.; Wang, L.; Li, X.; Gao, W.; Liu, H.; Jiao, M.; Wu, Z.; et al. IDH1R132H promotes malignant transformation of benign prostatic epithelium by dysregulating microRNAs: Involvement of IGF1R-AKT/STAT3 signaling pathway. Neoplasia 2018, 20, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.; Wa, Q.; Pan, J.; Peng, X.; Ren, D.; Huang, Y.; Chen, X.; Tang, Y. Downregulation of miR-141-3p promotes bone metastasis via activating NF-kappaB signaling in prostate cancer. J. Exp. Clin. Cancer Res. 2017, 36, 173. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Z.; Li, J.; Wang, H.Q.; Li, X.; Wen, B.; Wang, Y.J. MiR-141-3p promotes prostate cancer cell proliferation through inhibiting kruppel-like factor-9 expression. Biochem. Biophys. Res. Commun. 2017, 482, 1381–1386. [Google Scholar] [CrossRef]
- Zhao, H.; Su, W.; Zhu, C.; Zeng, T.; Yang, S.; Wu, W.; Wang, D. Cell fate regulation by reticulon-4 in human prostate cancers. J. Cell. Physiol. 2019, 234, 10372–10385. [Google Scholar] [CrossRef]
- Murata, T.; Takayama, K.; Katayama, S.; Urano, T.; Horie-Inoue, K.; Ikeda, K.; Takahashi, S.; Kawazu, C.; Hasegawa, A.; Ouchi, Y.; et al. miR-148a is an androgen-responsive microRNA that promotes LNCaP prostate cell growth by repressing its target CAND1 expression. Prostate Cancer Prostatic Dis. 2010, 13, 356–361. [Google Scholar] [CrossRef]
- Fujita, Y.; Kojima, K.; Ohhashi, R.; Hamada, N.; Nozawa, Y.; Kitamoto, A.; Sato, A.; Kondo, S.; Kojima, T.; Deguchi, T.; et al. MiR-148a attenuates paclitaxel resistance of hormone-refractory, drug-resistant prostate cancer PC3 cells by regulating MSK1 expression. J. Biol. Chem. 2010, 285, 19076–19084. [Google Scholar] [CrossRef]
- Farina, N.H.; Zingiryan, A.; Akech, J.A.; Callahan, C.J.; Lu, H.; Stein, J.L.; Languino, L.R.; Stein, G.S.; Lian, J.B. A microRNA/Runx1/Runx2 network regulates prostate tumor progression from onset to adenocarcinoma in TRAMP mice. Oncotarget 2016, 7, 70462–70474. [Google Scholar] [CrossRef] [Green Version]
- Song, C.; Chen, H.; Wang, T.; Zhang, W.; Ru, G.; Lang, J. Expression profile analysis of microRNAs in prostate cancer by next-generation sequencing. Prostate 2015, 75, 500–516. [Google Scholar] [CrossRef]
- Klein, E.A.; Cooperberg, M.R.; Magi-Galluzzi, C.; Simko, J.P.; Falzarano, S.M.; Maddala, T.; Chan, J.M.; Li, J.; Cowan, J.E.; Tsiatis, A.C.; et al. A 17-gene assay to predict prostate cancer aggressiveness in the context of Gleason grade heterogeneity, tumor multifocality, and biopsy undersampling. Eur. Urol. 2014, 66, 550–560. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.W.; Devanarayan, V.; Barrett, Y.C.; Weiner, R.; Allinson, J.; Fountain, S.; Keller, S.; Weinryb, I.; Green, M.; Duan, L.; et al. Fit-for-purpose method development and validation for successful biomarker measurement. Pharm. Res. 2006, 23, 312–328. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Busch, J.; Jung, M.; Rabenhorst, S.; Ralla, B.; Kilic, E.; Mergemeier, S.; Budach, N.; Fendler, A.; Jung, K. Diagnostic and prognostic potential of circulating cell-free genomic and mitochondrial DNA fragments in clear cell renal cell carcinoma patients. Clin. Chim. Acta 2016, 452, 109–119. [Google Scholar] [CrossRef]
- Bhatnagar, N.; Li, X.; Padi, S.K.; Zhang, Q.; Tang, M.S.; Guo, B. Downregulation of miR-205 and miR-31 confers resistance to chemotherapy-induced apoptosis in prostate cancer cells. Cell Death Dis. 2010, 1, e105. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, L.; Fredsoe, J.; Kristensen, H.; Strand, S.H.; Rasmussen, A.; Hoyer, S.; Borre, M.; Mouritzen, P.; Orntoft, T.; Sorensen, K.D. Training and validation of a novel 4-miRNA ratio model (MiCaP) for prediction of postoperative outcome in prostate cancer patients. Ann. Oncol. 2018, 29, 2003–2009. [Google Scholar] [CrossRef] [PubMed]
- Strand, S.H.; Bavafaye-Haghighi, E.; Kristensen, H.; Rasmussen, A.K.; Hoyer, S.; Borre, M.; Mouritzen, P.; Besenbacher, S.; Orntoft, T.F.; Sorensen, K.D. A novel combined miRNA and methylation marker panel (miMe) for prediction of prostate cancer outcome after radical prostatectomy. Int. J. Cancer 2019. [Google Scholar] [CrossRef] [PubMed]
- Nam, R.K.; Wallis, C.J.D.; Amemiya, Y.; Benatar, T.; Seth, A. Identification of a novel microRNA panel associated with metastasis following radical prostatectomy for prostate cancer. Anticancer Res. 2018, 38, 5027–5034. [Google Scholar] [CrossRef]
- Gerszten, R.E.; Wang, T.J. The search for new cardiovascular biomarkers. Nature 2008, 451, 949–952. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 479–505. [Google Scholar] [CrossRef] [Green Version]
- Loeb, S.; Ross, A.E. Genomic testing for localized prostate cancer: Where do we go from here? Curr. Opin. Urol. 2017, 27, 495–499. [Google Scholar] [CrossRef]
- Glass, A.G.; Leo, M.C.; Haddad, Z.; Yousefi, K.; du, P.M.; Chen, C.; Choeurng, V.; Abdollah, F.; Robbins, B.; Ra, S.; et al. Validation of a genomic classifier for predicting post-prostatectomy recurrence in a community based health care setting. J. Urol. 2016, 195, 1748–1753. [Google Scholar] [CrossRef] [PubMed]
- Tilki, D.; Evans, C.P. The Decipher Genomic Classifier independently improves prognostication for patients after prostatectomy. Eur. Urol. 2018, 73, 176–177. [Google Scholar] [CrossRef] [PubMed]
- Alam, S.; Tortora, J.; Staff, I.; McLaughlin, T.; Wagner, J. Prostate cancer genomics: Comparing results from three molecular assays. Can. J. Urol. 2019, 26, 9758–9762. [Google Scholar] [PubMed]
- Jung, M.; Schaefer, A.; Steiner, I.; Kempkensteffen, C.; Stephan, C.; Erbersdobler, A.; Jung, K. Robust microRNA stability in degraded RNA preparations from human tissue and cell samples. Clin. Chem. 2010, 56, 998–1006. [Google Scholar] [CrossRef] [PubMed]
- Littman, B.H.; Di, M.L.; Plebani, M.; Marincola, F.M. What’s next in translational medicine? Clin. Sci. Lond. 2007, 112, 217–227. [Google Scholar] [CrossRef] [PubMed]
- Fendler, A.; Stephan, C.; Yousef, G.M.; Jung, K. MicroRNAs as regulators of signal transduction in urological tumors. Clin. Chem. 2011, 57, 954–968. [Google Scholar] [CrossRef] [PubMed]
- Waltering, K.K.; Porkka, K.P.; Jalava, S.E.; Urbanucci, A.; Kohonen, P.J.; Latonen, L.M.; Kallioniemi, O.P.; Jenster, G.; Visakorpi, T. Androgen regulation of micro-RNAs in prostate cancer. Prostate 2011, 71, 604–614. [Google Scholar] [CrossRef]
- Salmena, L.; Poliseno, L.; Tay, Y.; Kats, L.; Pandolfi, P.P. A ceRNA hypothesis: The Rosetta Stone of a hidden RNA language? Cell 2011, 146, 353–358. [Google Scholar] [CrossRef]
- Burke, H.B. Predicting clinical outcomes using molecular biomarkers. Biomark. Cancer 2016, 8, 89–99. [Google Scholar] [CrossRef]
- Van den Broeck, T.; van den Bergh, R.C.N.; Briers, E.; Cornford, P.; Cumberbatch, M.; Tilki, D.; De, S.M.; Fanti, S.; Fossati, N.; Gillessen, S.; et al. Biochemical recurrence in prostate cancer: The European Association of Urology Prostate Cancer Guidelines Panel Recommendations. Eur. Urol. Focus 2019, in press. [Google Scholar] [CrossRef]
- Fendler, A.; Jung, M.; Stephan, C.; Erbersdobler, A.; Jung, K.; Yousef, G.M. The antiapoptotic function of miR-96 in prostate cancer by inhibition of FOXO1. PLoS ONE 2013, 8, e80807. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.; Jung, M.; Stephan, C.; Miller, K.; Lein, M.; Kristiansen, G.; Erbersdobler, A.; Jung, K. Suitable reference genes for relative quantification of miRNA expression in prostate cancer. Exp. Mol. Med. 2010, 42, 749–758. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; et al. The MIQE guidelines: Minimum information for publication of quantitative real-time PCR experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Stephan, C.; Jung, K.; Semjonow, A.; Schulze-Forster, K.; Cammann, H.; Hu, X.; Meyer, H.A.; Bogemann, M.; Miller, K.; Friedersdorff, F. Comparative assessment of urinary prostate cancer antigen 3 and TMPRSS2:ERG gene fusion with the serum [−2] proprostate-specific antigen-based prostate health index for detection of prostate cancer. Clin. Chem. 2013, 59, 280–288. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | Patients with Biochemical Recurrence | Patients without Biochemical Recurrence | p-value a |
|---|---|---|---|---|
| Patients, no. (%) | 206 (100) | 98 (48) | 108 (52) | |
| Age, median years (range) | 63 (47–74) | 64 (51–74) | 62 (47–73) | 0.014 |
| PSA, median µg/L (range) | 8.4 (1.3–50.6) | 9.3 (1.4–50.6) | 7.5 (1.3–32.9) | 0.003 |
| Prostate volume, median cm3 (range) | 33 (14–130) | 33 (15–130) | 32 (14–120) | 0.465 |
| DRE, no. (%) | 0.260 | |||
| Non-suspicious | 122 (59) | 54 (55) | 68 (63) | |
| Suspicious | 84 (41) | 44 (45) | 40 (37) | |
| pT status, no. (%) | <0.0001 | |||
| pT2a | 18 (9) | 5 (5) | 13 (12) | |
| pT2b | 28 (14) | 6 (6) | 22 (20) | |
| pT2c | 76 (37) | 31 (32) | 45 (42) | |
| pT3a | 62 (30) | 40 (41) | 22 (20) | |
| pT3b | 21 (10) | 15 (15) | 6 (6) | |
| pT4 | 1 (0.5) | 1 (1) | 0 | |
| ISUP Grade groups, no. (%) | ||||
| 1 | 52 (25) | 14 (14) | 38 (35) | 0.0003 |
| 2 | 68 (33) | 30 (31) | 38 (35) | |
| 3 | 27 (13) | 19 (19) | 8 (7) | |
| 4 | 29 (14) | 16 (16) | 13 (12) | |
| 5 | 30 (15) | 19 (19) | 11 (10) | |
| pN status, no. (%) b | ||||
| pN0 | 113 (55) | 57 (58) | 56 (52) | 0.207 |
| pN1 | 10 (5) | 7 (7) | 3 (3) | |
| pNx | 83 (40) | 34 (35) | 49 (45) | |
| Surgical margin, no. (%) | ||||
| Negative | 133 (65) | 54 (55) | 79 (73) | 0.009 |
| Positive | 73 (35) | 44 (45) | 29 (27) | |
| Follow-up after surgery | ||||
| Median months (range) | 108 (17–180) | 101 (19–160) | 121 (17–180) | <0.0001 |
| Recurrence free survival | ||||
| Median months (95% CI) | 52 (46–60) | 16 (11-21) | 80 (75–93) | <0.0001 |
| miRBase ID Release 22 | miRBase Accession No. a | Reference to BCR-Related miRNA | Differential Expression: Tumor vs. Normal Tissue b | Differential Expression: Recurrence vs. Non-Recurrence c |
|---|---|---|---|---|
| hsa-miR-1-3p | MIMAT0000416 | [35,40,41] | n.s., p = 0.177 | ↓, p = 0.0004 |
| hsa-miR-21-5p | MIMAT0000076 | [42,43,44,45,46] | ↑, p = 0.006 | n.s., p = 0.271 |
| hsa-miR-29c-3p | MIMAT0000681 | [47,48,49] | n.s., p = 0.272 | n.s., p = 0.390 |
| hsa-miR-30c-5p | MIMAT0000244 | [50,51] | ↑, p = 0.011 | n.s., p = 0.056 |
| hsa-miR-30d-5p | MIMAT0000245 | [52,53] | ↑, p < 0.0001 | n.s., p = 0.297 |
| hsa-miR-31-5p | MIMAT0000089 | [54,55] | ↓, p < 0.0001 | ↓, p = 0.0007 |
| hsa-miR-34a-5p | MIMAT0000255 | [47,56,57] | n.s., p = 0.155 | ↓, p = 0.0004 |
| hsa-miR-141-3p | MIMAT0000432 | [45,47] | n.s., p = 0.219 | n.s., p = 0.099 |
| hsa-miR-145-5p | MIMAT0000437 | [58,59,60,61] | ↓, p = 0.011 | ↓, p = 0.0004 |
| hsa-miR-148a-3p | MIMAT0000243 | [47,62] | ↑, p = 0.018 | n.s., p = 0.809 |
| hsa-miR-185-5p | MIMAT0000455 | [33] | ↑, p = 0.015 | n.s., p = 0.420 |
| hsa-miR-195-5p | MIMAT0000461 | [63,64] | ↑, p < 0.0001 | n.s., p = 0.559 |
| hsa-miR-204-5p | MIMAT0000265 | [65,66] | ↓, p = 0.0001 | ↓, p = 0.045 |
| hsa-miR-221-3p | MIMAT0000278 | [33,45,59,60,67] | ↓, p < 0.0001 | ↓, p = 0.0001 |
| hsa-miR-224-5p d | MIMAT0000281 | [68,69] | ↓, p < 0.0001 | ↓, p = 0.0001 |
| hsa-miR-301a-3p | MIMAT0000688 | [38,70] | ↑, p = 0.0002 | n.s., p = 0.674 |
| hsa-miR-326 | MIMAT0000756 | [33] | ↑, p = 0.009 | ↓, p = 0.033 |
| hsa-miR-374b-5p | MIMAT0004955 | [71,72] | ↑, p < 0.0001 | n.s., p = 0.141 |
| hsa-miR-494-3p | MIMAT0002816 | [73,74,75] | n.s., p = 0.721 | n.s., p = 0.821 |
| hsa-miR-939-5p | MIMAT0004982 | [76] | ↑, p = 0.028 | n.s., p = 0.784 |
| (A) miR-1 to miR-1 to miR148a | |||||||||||
| miR-1 | miR-21 | miR-29c | miR-30c | miR-30d | miR-31 | miR-34a | miR-141 | miR-145 | miR-148a | ||
| Age | rs | −0.059 | −0.087 | 0.104 | 0.009 | 0.073 | −0.094 | 0.070 | 0.095 | −0.036 | 0.042 |
| p-value | 0.403 | 0.214 | 0.139 | 0.901 | 0.294 | 0.178 | 0.318 | 0.174 | 0.604 | 0.546 | |
| PSA | rs | −0.218 | 0.007 | 0.030 | −0.107 | 0.019 | −0.086 | −0.119 | 0.156 | −0.211 | 0.068 |
| p-value | 0.002 | 0.922 | 0.668 | 0.125 | 0.783 | 0.220 | 0.090 | 0.025 | 0.002 | 0.334 | |
| DRE | rs | −0.119 | 0.132 | −0.035 | −0.127 | 0.021 | −0.053 | −0.031 | −0.022 | −0.062 | 0.005 |
| p-value | 0.087 | 0.059 | 0.622 | 0.068 | 0.765 | 0.446 | 0.657 | 0.757 | 0.376 | 0.945 | |
| Margin | rs | −0.146 | −0.129 | 0.056 | −0.139 | −0.064 | −0.198 | −0.114 | 0.112 | −0.184 | 0.184 |
| p-value | 0.037 | 0.065 | 0.425 | 0.047 | 0.358 | 0.004 | 0.102 | 0.108 | 0.008 | 0.008 | |
| pN status | rs | −0.110 | 0.022 | −0.147 | −0.122 | −0.091 | −0.129 | −0.142 | −0.046 | −0.110 | 0.005 |
| p-value | 0.116 | 0.753 | 0.035 | 0.080 | 0.194 | 0.064 | 0.041 | 0.508 | 0.114 | 0.946 | |
| pT stage | rs | −0.218 | 0.146 | 0.029 | −0.086 | 0.015 | −0.085 | −0.061 | 0.153 | −0.179 | 0.144 |
| p-value | 0.002 | 0.036 | 0.677 | 0.222 | 0.828 | 0.225 | 0.385 | 0.028 | 0.010 | 0.038 | |
| ISUP | rs | −0.351 | 0.198 | 0.188 | −0.080 | 0.095 | −0.232 | −0.014 | 0.298 | −0.265 | 0.249 |
| p-value | 0.0001 | 0.004 | 0.007 | 0.256 | 0.173 | 0.001 | 0.844 | 0.0001 | 0.0001 | 0.0003 | |
| (B) miR-185 to miR-939 | |||||||||||
| miR-185 | miR-195 | miR-204 | miR-221 | miR-224 | miR-301a | miR-326 | miR-374b | miR-494 | miR-939 | ||
| Age | rs | −0.002 | 0.011 | 0.119 | 0.001 | −0.088 | −0.044 | 0.045 | −0.036 | 0.038 | 0.000 |
| p-value | 0.976 | 0.870 | 0.090 | 0.983 | 0.208 | 0.528 | 0.517 | 0.611 | 0.584 | 0.999 | |
| PSA | rs | 0.063 | −0.137 | −0.220 | −0.080 | −0.137 | −0.030 | 0.048 | −0.063 | 0.005 | −0.027 |
| p-value | 0.371 | 0.050 | 0.002 | 0.253 | 0.049 | 0.670 | 0.495 | 0.367 | 0.945 | 0.702 | |
| DRE | rs | 0.012 | 0.033 | −0.062 | −0.082 | −0.038 | 0.001 | 0.000 | −0.034 | 0.071 | −0.003 |
| p-value | 0.860 | 0.634 | 0.373 | 0.244 | 0.588 | 0.990 | 0.994 | 0.632 | 0.311 | 0.966 | |
| Margin | rs | −0.096 | −0.214 | −0.124 | −0.032 | −0.175 | −0.080 | −0.092 | −0.096 | 0.127 | −0.030 |
| p-value | 0.169 | 0.002 | 0.076 | 0.652 | 0.012 | 0.254 | 0.186 | 0.168 | 0.069 | 0.672 | |
| pN status | rs | −0.020 | 0.031 | −0.110 | −0.048 | −0.106 | 0.034 | −0.080 | −0.097 | −0.031 | −0.130 |
| p-value | 0.774 | 0.659 | 0.116 | 0.496 | 0.131 | 0.631 | 0.256 | 0.166 | 0.659 | 0.062 | |
| pT stage | rs | 0.088 | 0.032 | −0.100 | −0.083 | −0.166 | 0.121 | −0.023 | −0.064 | −0.049 | −0.065 |
| p-value | 0.211 | 0.648 | 0.154 | 0.235 | 0.017 | 0.084 | 0.738 | 0.361 | 0.485 | 0.352 | |
| ISUP | rs | 0.092 | −0.042 | −0.256 | −0.015 | −0.146 | 0.051 | 0.066 | −0.059 | 0.056 | −0.069 |
| p-value | 0.186 | 0.551 | 0.0002 | 0.825 | 0.036 | 0.467 | 0.346 | 0.402 | 0.423 | 0.323 | |
| miRNA | Univariate Cox Regression for All miRs | Multivariate Cox Regression with Significant Univariate miRs b | ||||
|---|---|---|---|---|---|---|
| Full Model | Backward Elimination | |||||
| HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| miR-1-3p | 0.67 (0.52–0.87) | 0.003 | 0.82 (0.58–1.16) | 0.262 | ||
| miR-21-5p | 1.12 (1.01–1.24) | 0.049 | 1.35 (0.86–2.12) | 0.188 | ||
| miR-29c-3p | 1.06 (0.81–1.39) | 0.660 | ||||
| miR-30c-5p | 0.56 (0.34–0.92) | 0.023 | 0.46 (0.23–0.93) | 0.031 | 0.49 (0.28–0.85) | 0.011 |
| miR-30d-5p | 1.22 (1.05–1.42) | 0.009 | 1.79 (1.12–2.85) | 0.015 | 1.27 (0.98–1.66) | 0.075 |
| miR-31-5p | 0.78 (0.68–0.90) | 0.001 | 0.83 (0.69–0.98) | 0.030 | 0.78 (0.67–0.91) | 0.001 |
| miR-34a-5p | 1.09 (0.96–1.23) | 0.174 | 0.61 (0.36–1.03) | 0.063 | ||
| miR-141-3p | 1.25 (1.10–1.41) | 0.001 | 1.96 (1.25–3.07) | 0.003 | 1.92 (1.32–2.79) | 0.001 |
| miR-145-5p | 0.68 (0.51–0.90) | 0.008 | 1.17 (0.65–2.11) | 0.604 | ||
| miR-148a-3p | 1.15 (0.99–1.34) | 0.064 | 0.58 (0.35–0.95) | 0.031 | 0.60 (0.44–0.81) | 0.001 |
| miR-185-5p | 1.06 (1.01–1.12) | 0.024 | 0.99 (0.68–1.43) | 0.955 | ||
| miR-195-5p | 0.91 (0.68–1.23) | 0.553 | ||||
| miR-204-5p | 0.76 (0.59–0.98) | 0.033 | 1.31 (0.92–1.88) | 0.138 | ||
| miR-221-3p | 0.81 (0.67–0.98) | 0.033 | 0.67 (0.48-0.95) | 0.024 | 0.74 (0.61–0.90) | 0.002 |
| miR-224-5p | 0.67 (0.50–0.89) | 0.006 | 0.79 (0.51–1.22) | 0.280 | ||
| miR-301a-3p | 0.83 (0.61–1.14) | 0.241 | ||||
| miR-326 | 1.03 (1.01–1.05) | 0.008 | 0.97 (0.80–1.18) | 0.749 | ||
| miR-374b-5p | 0.85 (0.52–1,38) | 0.509 | ||||
| miR-494-3p | 1.00 (1.00–1.01) | 0.023 | 1.01 (0.99–1.04) | 0.447 | ||
| miR-939-5p | 1.02 (1.00–1.05) | 0.021 | 0.98 (0.80–1.21) | 0.869 | ||
| miRNA Panel | All Samples (n = 206) | Training Set (n = 140) | Test Set (n = 66) | p-value a |
|---|---|---|---|---|
| AUC (SE) | AUC (SE) | AUC (SE) | ||
| five-miR-panel | 0.774 (0.040) | 0.735 (0.069) | 0.625 | |
| 0.745 (0.034) | ||||
| six-miR-panel | 0.779 (0.040) | 0.741 (0.058) | 0.587 | |
| 0.749 (0.034) | ||||
| p-value b | 0.623 | 0.930 | 0.947 |
| Variable a | Univariate Cox Regression | Multivariate Cox Regression with Significant Variables | ||||
|---|---|---|---|---|---|---|
| Full Model b | Reduced Model after Backward Elimination c | |||||
| HR (95% CI) | p-value | HR (95% CI) | p-value | HR (95% CI) | p-value | |
| Age | 1.04 (1.00–1.08) | 0.029 | 1.02 (0.98–1.07) | 0.231 | ||
| PSA | 1.04 (1.01–1.07) | 0.004 | 1.02 (0.99–1.05) | 0.207 | ||
| DRE | 1.24 (0.83–1.95) | 0.286 | ||||
| Margin | 1.72 (1.16–2.56) | 0.008 | 1.42 (0.64–3.11) | 0.548 | ||
| pN status | 2.66 (0.88–4.10) | 0.103 | 1.14 (0.74–1.75) | 0.396 | ||
| pT stage | 1.12 (1.08–1.17) | <0.0001 | 1.08 (1.03–1.14) | 0.002 | 1.10 (1.04–1.15) | 0.001 |
| ISUP Group | 1.37 (1.19–1.57) | <0.0001 | 1.19 (1.02–1.40) | 0.027 | 1.23 (1.06–1.43) | 0.007 |
| Prediction Tool | Clinicopathological-Based Tool | Clinicopathological-Based Tool Combined with the five-miR-Panel | p-value |
|---|---|---|---|
| AUC (95% CI) | AUC (95% CI) | ||
| Reference models | |||
| D’Amico et al. [15] | 0.590 (0.519–0.657) | 0.759 (0.695–0.816) | <0.0001 |
| CAPRAS | 0.692 (0.624–0.754) | 0.769 (0.706–0.825) | 0.008 |
| NCCN | 0.642 (0.572–0.707) | 0.757 (0.693–0.814) | 0.0005 |
| Stephenson et al. [17] | 0.664 (0.595–0.728) | 0.747 (0.682–0.805) | 0.017 |
| Present study | |||
| Full model | 0.723 (0.657–0.783) | 0.793 (0.731–0.8465) | 0.007 |
| Reduced model | 0.712 (0.638–0.677) | 0.783 (0.720–0.837) | 0.007 |
| miRNA [Reference] | Tumor Suppressor Oncogene | Target Gene | Molecular Mechanism | |
|---|---|---|---|---|
| miR-30c-5p [79] | Tumor suppressor | ASF/SF2 | Inhibition of tumor cell proliferation, promotion of apoptosis through the inhibition of ASF/SF2 | |
| [80] | Tumor suppressor | KRAS | Inhibition of tumor cell proliferation, migration, and invasion | |
| [51] | Tumor suppressor | BCL9 | Correlation of disease progression via BCL9/Wingles-type signaling | |
| miR-31-5p [81] | Tumor suppressor | E2F6 | Promotion of apoptosis, reduced prostate cancer growth | |
| [82] | Tumor suppressor | Androgen receptor | Inhibition of cell proliferation and cell cycle | |
| miR-141-3p [83] | Tumor suppressor | IGF1R | inhibit malignant transformation of benign prostate epithelial cell via IGF1R-AKT/STAT3 signaling pathway | |
| [84] | Tumor suppressor | TRAF5, TRAF6 | Suppression of invasion and migration of PCa cells via inhibiting activation of NF-kB | |
| [85] | Oncogene | KLF9 | Regulation of proliferation, spheroid formation, and expression of the stemness factors OCT-4, SOX9, and CCND1 | |
| miR-148a-3p [86] | Tumor suppressor | RTN4 | Inhibition of cell proliferation and cell cycle blocked in G2/M phase | |
| [87] | Oncogene | CAND1 | Increased cell proliferation | |
| [88] | Tumor suppressor | MSK1 | Inhibition of cell growth, migration, and invasion | |
| miR-221-3p [89] | Tumor suppressor | Runx1, Runx2 | Inhibition of prostate tumorigenesis | |
| [82] | Tumor suppressor | Androgen receptor and its receptor coactivators | Inhibition of cell proliferation and targeted key oncogenic pathways, including cell cycle | |
| [90] | Oncogene | PI3K/AKT, P53 | Associated with signal transduction and cell communication | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhao, Z.; Weickmann, S.; Jung, M.; Lein, M.; Kilic, E.; Stephan, C.; Erbersdobler, A.; Fendler, A.; Jung, K. A Novel Predictor Tool of Biochemical Recurrence after Radical Prostatectomy Based on a Five-MicroRNA Tissue Signature. Cancers 2019, 11, 1603. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101603
Zhao Z, Weickmann S, Jung M, Lein M, Kilic E, Stephan C, Erbersdobler A, Fendler A, Jung K. A Novel Predictor Tool of Biochemical Recurrence after Radical Prostatectomy Based on a Five-MicroRNA Tissue Signature. Cancers. 2019; 11(10):1603. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101603
Chicago/Turabian StyleZhao, Zhongwei, Sabine Weickmann, Monika Jung, Michael Lein, Ergin Kilic, Carsten Stephan, Andreas Erbersdobler, Annika Fendler, and Klaus Jung. 2019. "A Novel Predictor Tool of Biochemical Recurrence after Radical Prostatectomy Based on a Five-MicroRNA Tissue Signature" Cancers 11, no. 10: 1603. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers11101603