RNA Immune Signatures from Pan-Cancer Analysis Are Prognostic for High-Grade Serous Ovarian Cancer and Other Female Cancers

 ,
, 
Abstract
:1. Introduction
2. Results
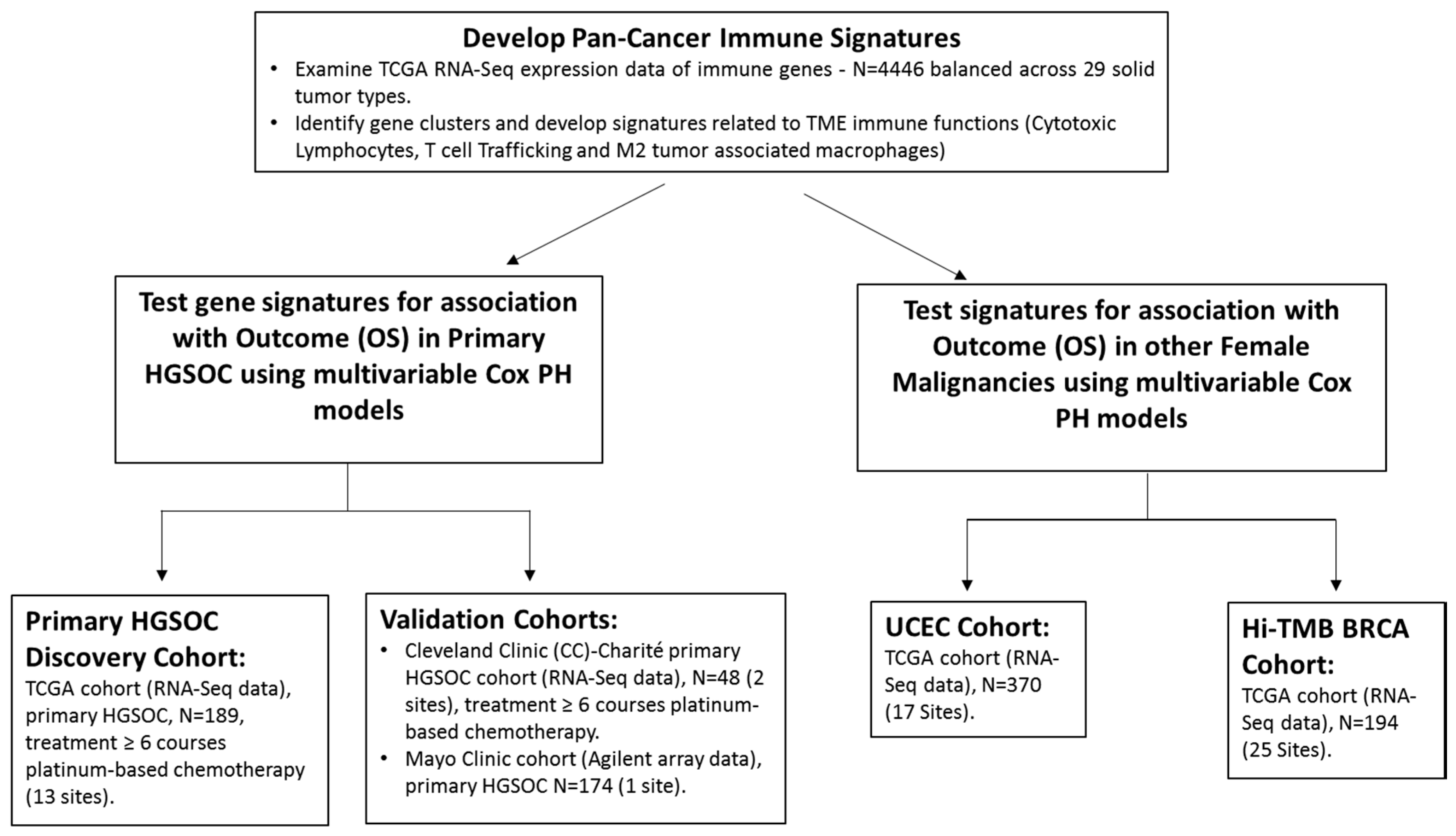
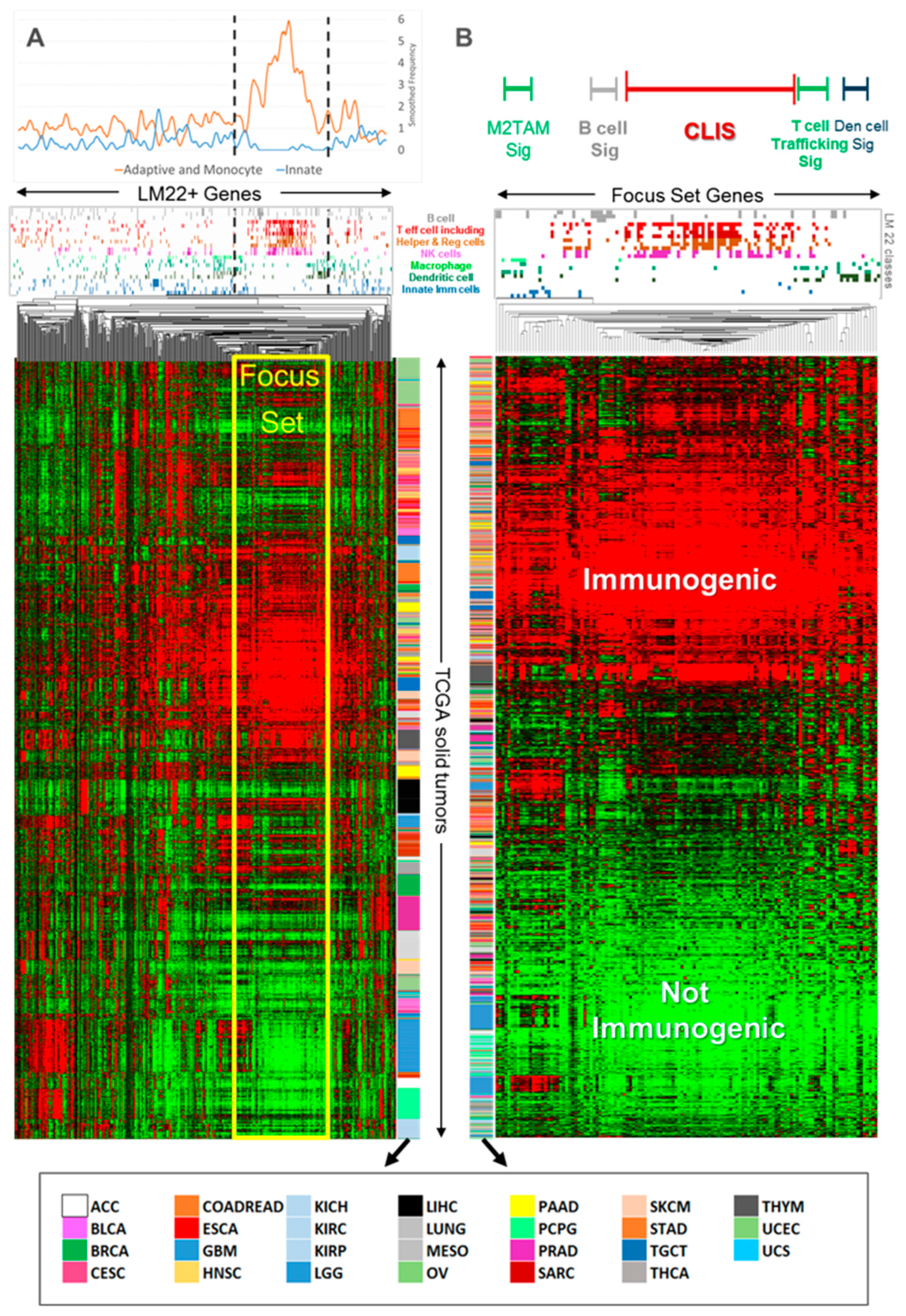
2.1. Pan-Cancer Analysis of TCGA RNA-Seq Data
2.2. Association of Pan-Cancer Derived Immune Signatures with Survival in HGSOC
2.3. Association of the Immune Signatures in the Presence of other Cofactors
2.4. Significance of Pan-Cancer-Based Immune Signature in other Cancers
3. Discussion
4. Materials and Methods
4.1. Pan-Cancer RNA-Seq Data Analysis for Derivation of Immune Signatures
4.2. Patient Cohorts
4.3. RNA-Seq and Microarray Analysis
4.4. Statistical and Survival Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Recurrence. Available online: https://ocrfa.org/patients/about-ovarian-cancer/recurrence/ (accessed on 6 February 2020).
- Chitale, R. Monitoring ovarian cancer: CA125 trial stirs controversy. J. Natl. Cancer Inst. 2009, 101, 1233–1235. [Google Scholar] [CrossRef] [PubMed]
- Hoppenot, C.; Eckert, M.A.; Tienda, S.M.; Lengyel, E. Who are the long-term survivors of high grade serous ovarian cancer? Gynecol. Oncol. 2018, 148, 204–212. [Google Scholar] [CrossRef] [PubMed]
- Verhaak, R.G.; Tamayo, P.; Yang, J.Y.; Hubbard, D.; Zhang, H.; Creighton, C.J.; Fereday, S.; Lawrence, M.; Carter, S.L.; Mermel, C.H.; et al. Prognostically relevant gene signatures of high-grade serous ovarian carcinoma. J. Clin. Investig. 2012, 123, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Bristow, R.E.; Tomacruz, R.S.; Armstrong, D.K.; Trimble, E.L.; Montz, F.J. Survival effect of maximal cytoreductive surgery for advanced ovarian carcinoma during the platinum era: A meta-analysis. J. Clin. Oncol. 2002, 20, 1248–1259. [Google Scholar] [CrossRef] [PubMed]
- Aluloski, I.; Tanturovski, M.; Jovanovic, R.; Kostadinova-Kunovska, S.; Petrusevska, G.; Stojkovski, I.; Petreska, B. Survival of Advanced Stage High-Grade Serous Ovarian Cancer Patients in the Republic of Macedonia. Open Access Maced. J. Med Sci. 2017, 5, 904–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ovarian Tumor Tissue Analysis (OTTA) Consortium Goode, E.L.; Block, M.S.; Kalli, K.R.; Vierkant, R.A.; Chen, W.; Fogarty, Z.C.; Gentry-Maharaj, A.; Toloczko, A.; Hein, A.; Bouligny, A.L.; et al. Dose-response association of CD8+ tumor-infiltrating lymphocytes and survival time in high-grade serous ovarian cancer. JAMA Oncol. 2017, 3, e173290. [Google Scholar] [CrossRef] [Green Version]
- Cancer Genome Atlas Research Network. Integrated genomic analyses of ovarian carcinoma. Nature 2011, 474, 609–615. [Google Scholar] [CrossRef]
- Ledermann, J.; Harter, P.; Gourley, C.; Friedlander, M.; Vergote, I.G.; Rustin, G.; Scott, C.L.; Meier, W.; Shapira-Frommer, R.; Safra, T.; et al. Olaparib maintenance therapy in patients with platinum-sensitive relapsed serous ovarian cancer: A preplanned retrospective analysis of outcomes by BRCA status in a randomised phase 2 trial. Lancet Oncol. 2014, 15, 852–861. [Google Scholar] [CrossRef]
- Pujade-Lauraine, E.; Ledermann, J.A.; Selle, F.; Gebski, V.; Penson, R.T.; Oza, A.M.; Korach, J.; Huzarski, T.; Poveda, A.; Pignata, S.; et al. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): A double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017, 18, 1274–1284. [Google Scholar] [CrossRef] [Green Version]
- Zhang, L.; Conejo-Garcia, J.R.; Katsaros, D.; Gimotty, P.A.; Massobrio, M.; Regnani, M.; Makrigiannakis, A.; Gray, H.; Schlienger, K.; Liebman, M.N.; et al. Intratumoral T cells, recurrence, and survival in epithelial ovarian cancer. N. Engl. J. Med. 2003, 348, 203–213. [Google Scholar] [CrossRef] [Green Version]
- Sato, E.; Olson, S.H.; Ahn, J.; Bundy, B.; Nishikawa, H.; Qian, F.; Jungbluth, A.A.; Frosina, D.; Gnjatic, S.; Ambrosone, C.; et al. Intraepithelial CD8+ tumor-infiltrating lymphocytes and a high CD8+/regulatory T cell ratio are associated with favorable prognosis in ovarian cancer. Proc. Natl. Acad. Sci. USA 2005, 102, 18538–18543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kandalaft, L.E.; Odunsi, K.; Coukos, G. Immunotherapy in Ovarian Cancer: Are We There Yet? J. Clin. Oncol. 2019, 37, 2460–2471. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; He, Y.; Sun, X.; Li, Q.; Wang, W.; Zhao, A.; Di, W. A high M1/M2 ratio of tumor-associated macrophages is associated with extended survival in ovarian cancer patients. J. Ovarian Res. 2014, 7, 1–16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Taub, D.D.; Lloyd, A.R.; Conlon, K.; Wang, J.M.; Ortaldo, J.R.; Harada, A.; Matsushima, K.; Kelvin, D.J.; Oppenheim, J.J. Recombinant human interferon-inducible protein 10 is a chemoattractant for human monocytes and T lymphocytes and promotes T cell adhesion to endothelial cells. J. Exp. Med. 1993, 177, 1809–1814. [Google Scholar] [CrossRef]
- Groom, J.R.; Luster, A.D. CXCR3 in T cell function. Exp. Cell Res. 2011, 317, 620–631. [Google Scholar] [CrossRef]
- Slaney, C.Y.; Kershaw, M.H.; Darcy, P.K. Trafficking of T cells into tumors. Cancer Res. 2014, 74, 7168–7174. [Google Scholar] [CrossRef] [Green Version]
- Abron, J.D.; Singh, N.P.; Murphy, A.E.; Mishra, M.K.; Price, R.L.; Nagarkatti, M.; Nagarkatti, P.S.; Singh, U.P. Differential role of CXCR3 in inflammation and colorectal cancer. Oncotarget 2018, 9, 17928–17936. [Google Scholar] [CrossRef] [Green Version]
- Bronger, H.; Singer, J.; Windmüller, C.; Reuning, U.; Zech, D.; Delbridge, C.; Dorn, J.; Kiechle, M.; Schmalfeldt, B.; Schmitt, M.; et al. CXCL9 and CXCL10 predict survival and are regulated by cyclooxygenase inhibition in advanced serous ovarian cancer. Br. J. Cancer 2016, 115, 553–563. [Google Scholar] [CrossRef] [Green Version]
- Lieber, S.; Reinartz, S.; Raifer, H.; Finkernagel, F.; Dreyer, T.; Bronger, H.; Jansen, J.M.; Wagner, U.; Worzfeld, T.; Muller, R.; et al. Prognosis of ovarian cancer is associated with effector memory CD8+ T cell accumulation in ascites, CXCL9 levels and activation-triggered signal transduction in T cells. Oncoimmunology 2018, 7, e1424672. [Google Scholar] [CrossRef] [Green Version]
- Iglesia, M.D.; Parker, J.S.; Hoadley, K.A.; Serody, J.S.; Perou, C.M.; Vincent, B.G. Genomic analysis of immune cell infiltrates across 11 tumor types. JNCI: J. Natl. Cancer Inst. 2016, 108, djw144. [Google Scholar] [CrossRef]
- Konecny, G.E.; Wang, C.; Hamidi, H.; Winterhoff, B.; Kalli, K.R.; Dering, J.; Ginther, C.; Chen, H.-W.; Dowdy, S.; Cliby, W.; et al. Prognostic andtherapeutic relevance of molecular subtypes in high-grade serous ovarian cancer. JNCI: J. Natl. Cancer Inst. 2014, 106, dju249. [Google Scholar] [CrossRef] [PubMed]
- Ganapathi, M.K.; Jones, W.D.; Sehouli, J.; Michener, C.M.; Braicu, I.E.; Norris, E.J.; Biscotti, C.V.; Vaziri, S.A.J.; Ganapathi, R.N. Expression profile of COL2A1 and the pseudogene SLC6A10P predicts tumor recurrence in high-grade serous ovarian cancer. Int. J. Cancer 2016, 138, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Thomas, A.; Routh, E.D.; Pullikuth, A.; Jin, G.; Su, J.; Chou, J.W.; Hoadley, K.A.; Print, C.; Knowlton, N.; Black, M.A.; et al. Tumor mutational burden is a determinant of immune-mediated survival in breast cancer. Oncoimmunology 2018, 7, e1490854. [Google Scholar] [CrossRef] [PubMed]
- Ellrott, K.; Bailey, M.H.; Saksena, G.; Covington, K.R.; Kandoth, C.; Stewart, C.; Hess, J.; Ma, S.; Chiotti, K.E.; McLellan, M.; et al. Scalable open science approach for mutation calling of tumor exomes using multiple genomic pipelines. Cell Syst. 2018, 6, 271–281. [Google Scholar] [CrossRef] [Green Version]
- Krishnan, V.; Berek, J.S.; Dorigo, O. Immunotherapy in ovarian cancer. Curr. Probl. Cancer 2017, 41, 48–63. [Google Scholar] [CrossRef]
- Peranzoni, E.; Lemoine, J.; Vimeux, L.; Feuillet, V.; Barrin, S.; Kantari-Mimoun, C.; Bercovici, N.; Guérin, M.; Biton, J.; Ouakrim, H.; et al. Macrophages impede CD8 T cells from reaching tumor cells and limit the efficacy of anti–PD- 1 treatment. Proc. Natl. Acad. Sci. USA 2018, 115, e4041–e4050. [Google Scholar] [CrossRef] [Green Version]
- Powerful combination therapies (editorial). Nat. Biomed. Eng. 2018, 2, 555–556. [CrossRef]
- Böhm, S.; Montfort, A.; Pearce, O.M.; Topping, J.; Chakravarty, P.; Everitt, G.L.; Clear, A.; McDermott, J.R.; Ennis, D.; Dowe, T.; et al. Neoadjuvant chemotherapy modulates the immune microenvironment in metastases of tubo-ovarian high-grade serous carcinoma. Clin. Cancer Res. 2016, 22, 3025–3036. [Google Scholar] [CrossRef] [Green Version]
- Lo, C.S.; Sanii, S.; Kroeger, D.R.; Milne, K.; Talhouk, A.; Chiu, D.S.; Rahimi, K.; Shaw, P.A.; Clarke, B.A.; Nelson, B.H. Neoadjuvant chemotherapy of ovarian cancer results in three patterns of tumor-infiltrating lymphocyte response with distinct implications for immunotherapy. Clin. Cancer Res. 2017, 23, 925–934. [Google Scholar] [CrossRef] [Green Version]
- Thorsson, V.; Gibbs, D.L.; Brown, S.D.; Wolf, D.; Bortone, D.S.; Yang, T.H.; Porta-Pardo, E.; Gao, G.F.; Plaiser, C.L.; Eddy, J.A.; et al. The immune landscape of cancer. Immunity 2018, 48, 812–830. [Google Scholar] [CrossRef] [Green Version]
- Aran, D.; Hu, Z.; Butte, A.J. xCell: Digitally portraying the tissue cellular heterogeneity landscape. Genome Biol. 2017, 18, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bastaki, S.; Irandoust, M.; Ahmadi, A.; Hojjat-Farsangi, M.; Ambrose, P.; Hallaj, S.; Edalati, M.; Ghalamfarsa, G.; Azizi, G.; Yousefi, M.; et al. PD-L1/PD-1 axis as a potent therapeutic target in breast cancer. Life Sci. 2020, 247, 117437. [Google Scholar] [CrossRef] [PubMed]
- Fan, C.A.; Reader, J.; Roque, D.M. Review of Immune Therapies Targeting Ovarian Cancer. Curr. Treat. Options Oncol. 2018, 19, 74. [Google Scholar] [CrossRef] [PubMed]
- Puzzoni, M.; Silvestris, N.; Leone, F.; Giampieri, R.; Faloppi, L.; Demurtas, L.; Dell’Aquila, E.; Marino, D.; Brunetti, O.; Garattini, S.K.; et al. The immune revolution in gastrointestinal tumours: Leading the way or just following? Target. Oncol. 2016, 11, 593–603. [Google Scholar] [CrossRef]
- Newman, A.M.; Liu, C.L.; Green, M.R.; Gentles, A.J.; Feng, W.; Xu, Y.; Hoang, C.D.; Diehn, M.; Alizadeh, A.A. Robust enumeration of cell subsets from tissue expression profiles. Nat. Methods 2015, 12, 453–457. [Google Scholar] [CrossRef] [Green Version]
- Rőszer, T. Understanding the mysterious M2 macrophage through activation markers and effector mechanisms. Mediat. Inflammatio 2015, 816460. [Google Scholar] [CrossRef] [Green Version]
- Bindea, G.; Mlecnik, B.; Tosolini, M.; Kirilovsky, A.; Waldner, M.; Obenauf, A.C.; Angell, H.; Fredriksen, T.; Lafontaine, L.; Berger, A.; et al. Spatiotemporal dynamics of intratumoral immune cells reveal the immune landscape in human cancer. Immunity 2013, 39, 782–795. [Google Scholar] [CrossRef] [Green Version]
- Li, B.; Dewey, C.N. RSEM: accurate transcript quantification from RNA-Seq data with or without a reference genome. BMC bioinformatics 2011, 12, 323. [Google Scholar] [CrossRef] [Green Version]
- Broad Institute TCGA Genome Data Analysis Center: Analysis-ready standardized TCGA data from Broad GDAC Firehose 2016_01_28 run. Broad Institute of MIT and Harvard. Dataset 2016. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cohort Characteristics | TCGA | Cleveland Clinic-Charité | Mayo Clinic |
|---|---|---|---|
| No. of patients (n) a | 189 | 48 | 174 |
| n with t ≤ 1-year (censored) b | 26 (24) | 4 (0) | 24 (0) |
| n with 1 year < t ≤ 5-year (censored) b | 123 (32) | 24 (6) | 99 (2) |
| n with t > 5- year (censored) b | 40 (19) | 20 (14) | 51 (19) |
| % patients w/censored survival | 40% | 42% | 12% |
| Minimum % with ≥ 5-year survival | 21% | 42% | 29% |
| Stage ≤ 2 | 12 (6%) | 6 (13%) | 8 (5%) |
| Stage 3 | 154 (81%) | 38 (79%) | 125 (72%) |
| Stage 4 | 23 (12%) | 4 (8%) | 41 (24%) |
| Primary Surgical Cytoreduction Status: Opt. – Subopt. – Unknown c | 130-12-47 | 34-14-0 | 128-48-3 |
| Median Age (years) | 57 | 61 | 64 |
| Interquartile Range of Age (years) | (51, 67) | (49, 70) | (55, 72) |
| RNA measurement platform | RNA-Seq | RNA-Seq | Agilent |
| Multivariable. Cox PH Models a | TCGA | Cleveland Clinic-Charité | Mayo Clinic | ||||||
|---|---|---|---|---|---|---|---|---|---|
| p-Value | HR b Est. | HR 95% Wald CI | p-Value | HRb Est. | HR 95% Wald CI | p-Value | HRb Est. | HR 95% Wald CI | |
| CLIS | 0.038 | 0.807 | (0.659,0.989) | 0.048 | 0.670 | (0.451,0.996) | 0.003 | 0.767 | (0.643,0.915) |
| Age | 0.088 | 1.016 | (0.998,1.034) | 0.286 | 1.018 | (0.985,1.053) | 0.058 | 1.016 | (0.999,1.030) |
| Stage | 0.659 | 0.019 | 0.006 | ||||||
| Primary surgical cytoreduction c | Not significant | Not significant | <0.000001 | 0.400 | (0.277,0.579) | ||||
| TCT | 0.014 | 0.795 | (0.662,0.954) | 0.014 | 0.587 | (0.384,0.897) | 0.0002 | 0.716 | (0.601,0.852) |
| Age | 0.112 | 1.015 | (0.997,1.033) | 0.350 | 1.019 | (0.980,1.059) | 0.074 | 1.014 | (0.999,1.029) |
| Stage | 0.886 | 0.120 | 0.008 | ||||||
| Primary surgical cytoreduction c | Not significant | 0.059 | 0.443 | (0.190,1.031) | <0.000001 | 0.382 | (0.263,0.554) | ||
| TCT:M2TAMd | <0.000001 | 0.603 | (0.482,0.754) | 0.067 | 0.660 | (0.422,1.030) | <0.000001 | 0.570 | (0.458,0.710) |
| Age | 0.228 | 1.011 | (0.993,1.030) | 0.539 | 1.012 | (0.974,1.051) | 0.073 | 1.013 | (0.999,1.028) |
| Stage | 0.783 | 0.208 | 0.059 | ||||||
| Primary surgical cytoreduction c | Not significant | 0.047 | 0.427 | (0.185,0.987) | 0.00002 | 0.419 | (0.290,0.604) | ||
| Multivariable Cox. Proportional Hazards Models b | TCGA UCEC Cohort | TCGA Hi-TMB c BRCA Cohort | ||||
|---|---|---|---|---|---|---|
| (OS e, n = 370) | (OS e, n = 194) | |||||
| p-Value | HR d Est. | HR 95% CI | p-Value | HR d Est. | HR 95% CI | |
| CLIS | 0.001 | 0.633 | (0.480,0.836) | 0.002 | 0.397 | (0.224,0.705) |
| Age | 0.002 | 1.043 | (1.016,1.071) | 0.004 | 1.055 | (1.017,1.094) |
| Stage | <0.00001 | 0.00001 | ||||
| PR Status | N/A | 0.011 | 3.375 | (1.350,10.437) | ||
| TCT | 0.036 | 0.733 | (0.548,0.980) | 0.032 | 0.521 | (0.287,0.944) |
| Age | 0.0005 | 1.047 | (1.020,1.074) | 0.005 | 1.055 | (1.016,1.094) |
| Stage | <0.00001 | 0.00001 | ||||
| PR Status | N/A | 0.017 | 3.344 | (1.241,9.016) | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jones, W.D.; Michener, C.M.; Biscotti, C.; Braicu, I.; Sehouli, J.; Ganapathi, M.K.; Ganapathi, R.N. RNA Immune Signatures from Pan-Cancer Analysis Are Prognostic for High-Grade Serous Ovarian Cancer and Other Female Cancers. Cancers 2020, 12, 620. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030620
Jones WD, Michener CM, Biscotti C, Braicu I, Sehouli J, Ganapathi MK, Ganapathi RN. RNA Immune Signatures from Pan-Cancer Analysis Are Prognostic for High-Grade Serous Ovarian Cancer and Other Female Cancers. Cancers. 2020; 12(3):620. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030620
Chicago/Turabian StyleJones, Wendell D., Chad M. Michener, Charles Biscotti, Iona Braicu, Jalid Sehouli, Mahrukh K. Ganapathi, and Ram N. Ganapathi. 2020. "RNA Immune Signatures from Pan-Cancer Analysis Are Prognostic for High-Grade Serous Ovarian Cancer and Other Female Cancers" Cancers 12, no. 3: 620. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12030620