The Prognostic and Predictive Value of SOX2+ Cell Densities in Patients Treated for Colorectal Cancer

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
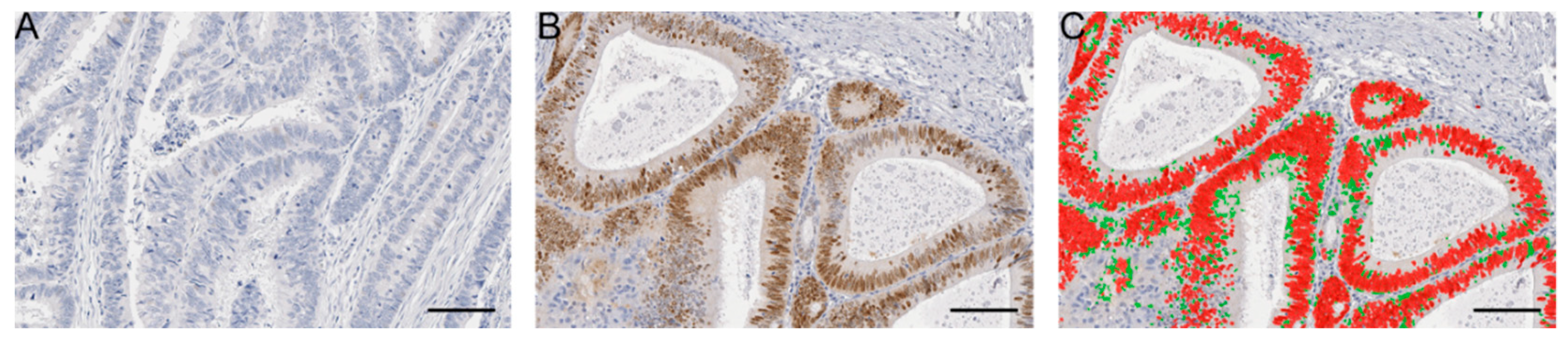
2.1. Patient Cohort and SOX2 Immunostaining
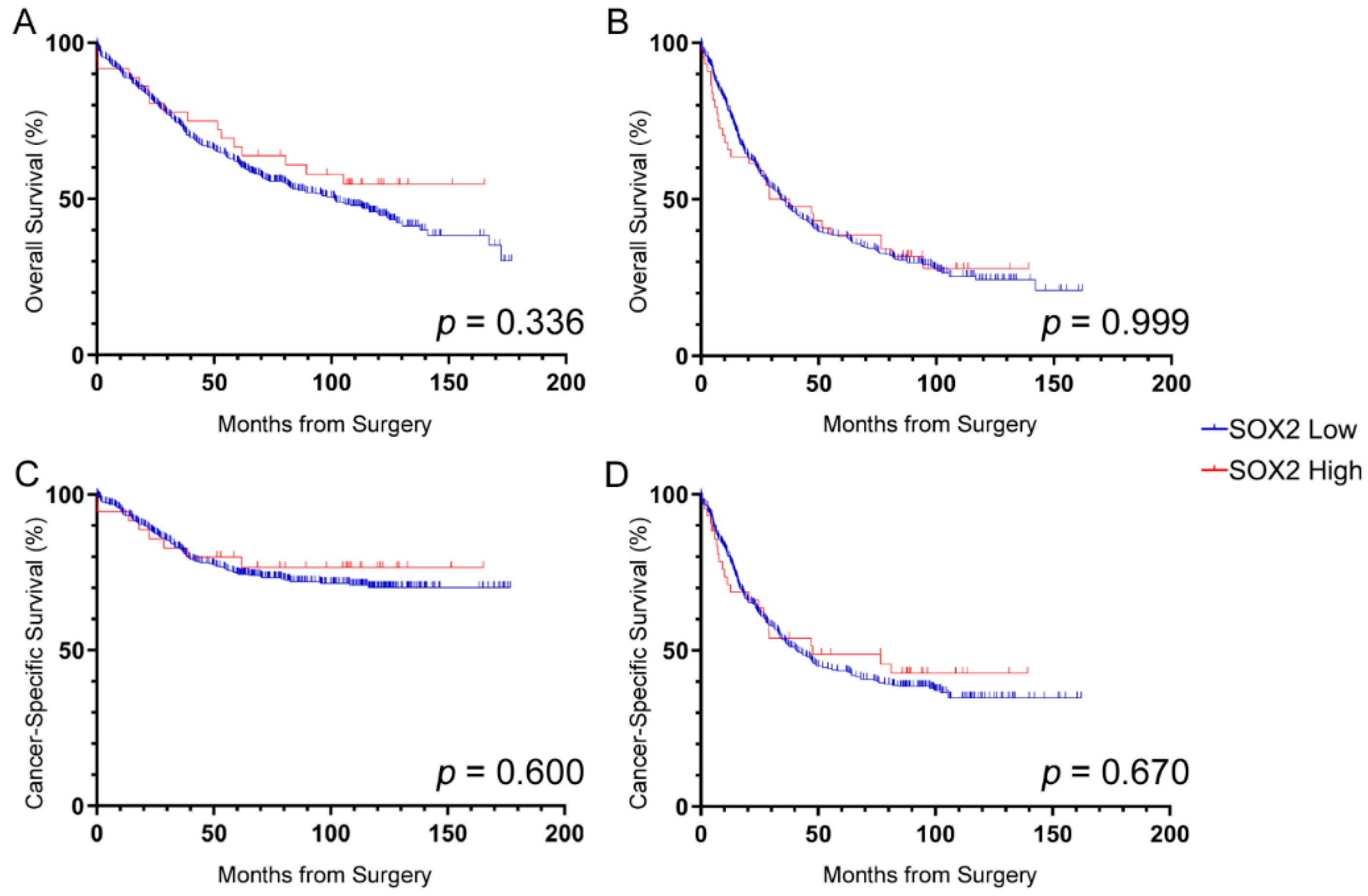
2.2. Prognosis
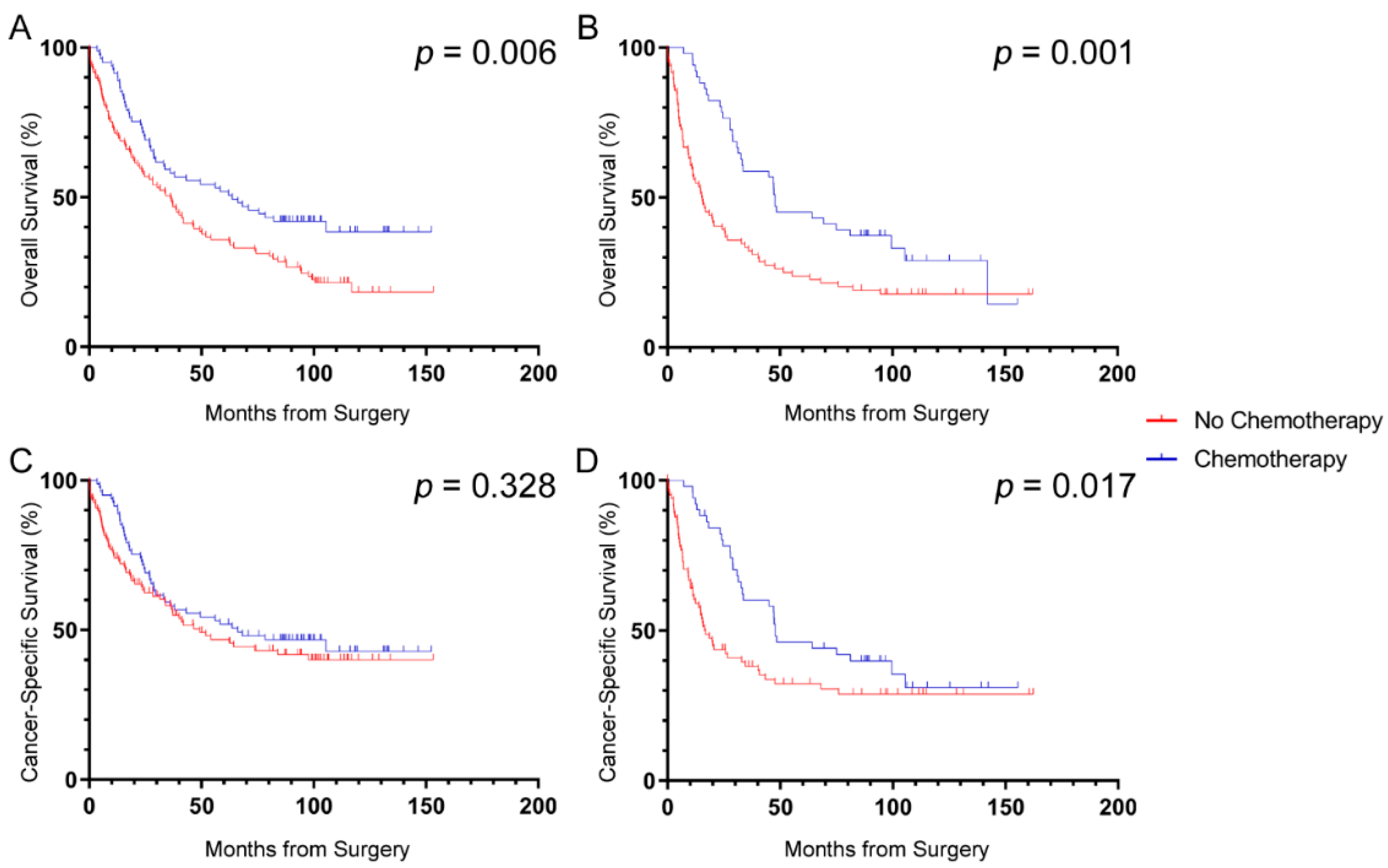
2.3. Survival Benefit from Chemotherapy
3. Discussion
4. Materials and Methods
4.1. Patients and Ethical Approval
4.2. Tissue Micro-Arrays
4.3. Immunostaining
4.4. Image Analysis and SOX2 Quantification
4.5. Statistical Analysis
4.6. Power Calculation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- American Cancer Society. Global Cancer Facts & Figures, 4th ed.; American Cancer Society: Atlanta, GA, USA, 2018. [Google Scholar]
- Kreso, A.; Dick, J.E. Evolution of the Cancer Stem Cell Model. Cell Stem Cell 2014, 14, 275–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, H.; Corbi, N.; Basilico, C.; Dailey, L. Developmental-specific activity of the FGF-4 enhancer requires the synergistic action of Sox2 and Oct-3. Genes Dev. 1995, 9, 2635–2645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Avilion, A.A.; Nicolis, S.K.; Pevny, L.H.; Perez, L.; Vivian, N.; Lovell-Badge, R. Multipotent cell lineages in early mouse development depend on SOX2 function. Genes Dev. 2003, 17, 126–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chew, J.L.; Loh, Y.H.; Zhang, W.; Chen, X.; Tam, W.L.; Yeap, L.S.; Li, P.; Ang, Y.S.; Lim, B.; Robson, P.; et al. Reciprocal transcriptional regulation of Pou5f1 and Sox2 via the Oct4/Sox2 complex in embryonic stem cells. Mol. Cell Biol. 2005, 25, 6031–6046. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sarkar, A.; Hochedlinger, K. The sox family of transcription factors: Versatile regulators of stem and progenitor cell fate. Cell Stem Cell 2013, 12, 15–30. [Google Scholar] [CrossRef] [Green Version]
- Rizzino, A.; Wuebben, E.L. Sox2/Oct4: A delicately balanced partnership in pluripotent stem cells and embryogenesis. Biochim. Biophys. Acta 2016, 1859, 780–791. [Google Scholar] [CrossRef]
- Kondoh, H.; Kamachi, Y. SOX-partner code for cell specification: Regulatory target selection and underlying molecular mechanisms. Int. J. Biochem. Cell Biol. 2010, 42, 391–399. [Google Scholar] [CrossRef]
- Liu, X.F.; Yang, W.T.; Xu, R.; Liu, J.T.; Zheng, P.S. Cervical cancer cells with positive Sox2 expression exhibit the properties of cancer stem cells. PLoS ONE 2014, 9, e87092. [Google Scholar] [CrossRef]
- Vanner, R.J.; Remke, M.; Gallo, M.; Selvadurai, H.J.; Coutinho, F.; Lee, L.; Kushida, M.; Head, R.; Morrissy, S.; Zhu, X.; et al. Quiescent sox2(+) cells drive hierarchical growth and relapse in sonic hedgehog subgroup medulloblastoma. Cancer Cell 2014, 26, 33–47. [Google Scholar] [CrossRef] [Green Version]
- Weina, K.; Utikal, J. SOX2 and cancer: Current research and its implications in the clinic. Clin. Transl. Med. 2014, 3, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.G.; Koh, Y.W.; Sari, I.N.; Jun, N.; Lee, S.; Phi, L.T.H.; Kim, K.S.; Wijaya, Y.T.; Lee, S.H.; Baek, M.J.; et al. Interferon-induced transmembrane protein 1-mediated EGFR/SOX2 signaling axis is essential for progression of non-small cell lung cancer. Int. J. Cancer 2019, 144, 2020–2032. [Google Scholar] [CrossRef] [PubMed]
- Malladi, S.; Macalinao, D.G.; Jin, X.; He, L.; Basnet, H.; Zou, Y.; de Stanchina, E.; Massague, J. Metastatic Latency and Immune Evasion through Autocrine Inhibition of WNT. Cell 2016, 165, 45–60. [Google Scholar] [CrossRef] [Green Version]
- Boumahdi, S.; Driessens, G.; Lapouge, G.; Rorive, S.; Nassar, D.; Le Mercier, M.; Delatte, B.; Caauwe, A.; Lenglez, S.; Nkusi, E.; et al. SOX2 controls tumour initiation and cancer stem-cell functions in squamous-cell carcinoma. Nature 2014, 511, 246–250. [Google Scholar] [CrossRef]
- Miller, T.J.; McCoy, M.J.; Hemmings, C.; Bulsara, M.K.; Iacopetta, B.; Platell, C.F. The prognostic value of cancer stem-like cell markers SOX2 and CD133 in stage III colon cancer is modified by expression of the immune-related markers FoxP3, PD-L1 and CD3. Pathology 2017, 49, 721–730. [Google Scholar] [CrossRef] [PubMed]
- Andre, T.; Boni, C.; Mounedji-Boudiaf, L.; Navarro, M.; Tabernero, J.; Hickish, T.; Topham, C.; Zaninelli, M.; Clingan, P.; Bridgewater, J.; et al. Multicenter International Study of Oxaliplatin/5-Fluorouracil/Leucovorin in the Adjuvant Treatment of Colon Cancer, I. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N. Engl. J. Med. 2004, 350, 2343–2351. [Google Scholar] [CrossRef] [Green Version]
- Ng, L.; Wan, T.; Chow, A.; Iyer, D.; Man, J.; Chen, G.H.; Yau, T.C.C.; Lo, O.; Foo, C.C.; Poon, J.T.C.; et al. Osteopontin Overexpression Induced Tumor Progression and Chemoresistance to Oxaliplatin through Induction of Stem-Like Properties in Human Colorectal Cancer. Stem Cells Int. 2015, 2015, 247892. [Google Scholar] [CrossRef] [Green Version]
- Lundberg, I.V.; Burstrom, A.L.; Edin, S.; Eklof, V.; Oberg, A.; Stenling, R.; Palmqvist, R.; Wikberg, M.L. SOX2 Expression Is Regulated by BRAF and Contributes to Poor Patient Prognosis in Colorectal Cancer. PLoS ONE 2014, 9, e101957. [Google Scholar] [CrossRef] [Green Version]
- Plate, J.D.J.; Borggreve, A.S.; van Hillegersberg, R.; Peelen, L.M. Post Hoc Power Calculation: Observing the Expected. Ann. Surg. 2019, 269, e11. [Google Scholar] [CrossRef]
- Song, K.; Hao, J.; Ge, Z.; Chen, P. Clinical and Survival Impact of Sex-Determining Region Y-Box 2 in Colorectal Cancer: An Integrated Analysis of the Immunohistochemical Study and Bioinformatics Analysis. J. Oncol. 2020, 2020, 3761535. [Google Scholar] [CrossRef]
- Chai, S.M.; Zeps, N.; Shearwood, A.-M.; Grieu, F.; Charles, A.; Harvey, J.; Goldblatt, J.; Joseph, D.; Iacopetta, B. Screening for defective DNA mismatch repair in stage II and III colorectal cancer patients. Clin. Gastroenterol. Hepatol. 2004, 2, 1017–1025. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variable | AJCC Stage II | AJCC Stage III |
|---|---|---|
| n = 445 | n = 352 | |
| Age, median (IQR) | 72.3 (64.6, 79.0) | 68.3 (59.3, 76.9) |
| T Stage, n (%) | ||
| T1 | - | 1 (0.3) |
| T2 | - | 11 (3.1) |
| T3 | 419 (94.2) | 331 (94.0) |
| T4 | 26 (5.8) | 9 (2.6) |
| Localization, n (%) | ||
| Proximal colon | 199 (44.7) | 140 (39.8) |
| Distal colon | 117 (26.3) | 110 (31.3) |
| Rectum | 113 (25.4) | 102 (29.0) |
| Not Reported | 16 (3.6) | 0 (0.0) |
| Vascular Invasion, n (%) | ||
| Present | 69 (15.5) | 160 (45.5) |
| Absent | 361 (81.1) | 192 (54.6) |
| Not Reported | 15 (3.4) | 0 (0.0) |
| PNI, n (%) | ||
| Present | 18 (4.0) | 39 (11.1) |
| Absent | 407 (91.5) | 313 (88.9) |
| Not Reported | 20 (4.5) | 0 (0.0) |
| Grade, n (%) | ||
| High | 45 (10.1) | 36 (10.2) |
| Low | 395 (88.8) | 314 (89.2) |
| Not Reported | 5 (1.1) | 2 (0.6) |
| Mucinous, n (%) | ||
| Yes | 72 (16.2) | 25 (7.1) |
| No | 74 (16.6) | 26 (7.4) |
| Not Reported | 299 (67.2) | 301 (85.6) |
| TILs, n (%) | ||
| Present | 58 (13.0) | 11 (3.1) |
| Absent | 87 (19.6) | 37 (10.5) |
| Not Reported | 300 (67.4) | 304 (86.4) |
| MMR, n (%) | ||
| Deficient | 63 (14.2) | 21 (6.0) |
| Proficient | 374 (84.0) | 323 (91.8) |
| Not Reported | 8 (1.8) | 8 (2.3) |
| SOX2, n (%) 1 | ||
| Low | 409 (91.9) | 308 (87.5) |
| High | 36 (8.1) | 44 (12.5) |
| Adjuvant Chemotherapy, n (%) | ||
| Yes | 22 (4.9) | 132 (37.5) |
| No | 167 (37.5) | 193 (54.8) |
| Not Reported | 256 (57.5) | 27 (7.7) |
| 5-Year OS, n (%) | ||
| Alive | 277 (62.2) | 135 (38.4) |
| Died | 168 (37.8) | 217 (61.6) |
| 5-Year CSS | ||
| Alive/Died from other cause | 343 (77.1) | 164 (46.6) |
| Died from CRC | 102 (22.9) | 188 (53.4) |
| Follow-up time, median 2 | 173.7 months | 166.1 months |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, T.J.; McCoy, M.J.; Lee-Pullen, T.F.; Anyaegbu, C.C.; Hemmings, C.; Bulsara, M.K.; Platell, C.F. The Prognostic and Predictive Value of SOX2+ Cell Densities in Patients Treated for Colorectal Cancer. Cancers 2020, 12, 1110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051110
Miller TJ, McCoy MJ, Lee-Pullen TF, Anyaegbu CC, Hemmings C, Bulsara MK, Platell CF. The Prognostic and Predictive Value of SOX2+ Cell Densities in Patients Treated for Colorectal Cancer. Cancers. 2020; 12(5):1110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051110
Chicago/Turabian StyleMiller, Tim J., Melanie J. McCoy, Tracey F. Lee-Pullen, Chidozie C. Anyaegbu, Christine Hemmings, Max K. Bulsara, and Cameron F. Platell. 2020. "The Prognostic and Predictive Value of SOX2+ Cell Densities in Patients Treated for Colorectal Cancer" Cancers 12, no. 5: 1110. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051110