[18F]FDG-PET/CT Radiomics for Prediction of Bone Marrow Involvement in Mantle Cell Lymphoma: A Retrospective Study in 97 Patients

 , ,
, ,  ,
,
Abstract
:1. Introduction
2. Results
2.1. Patient Characteristics
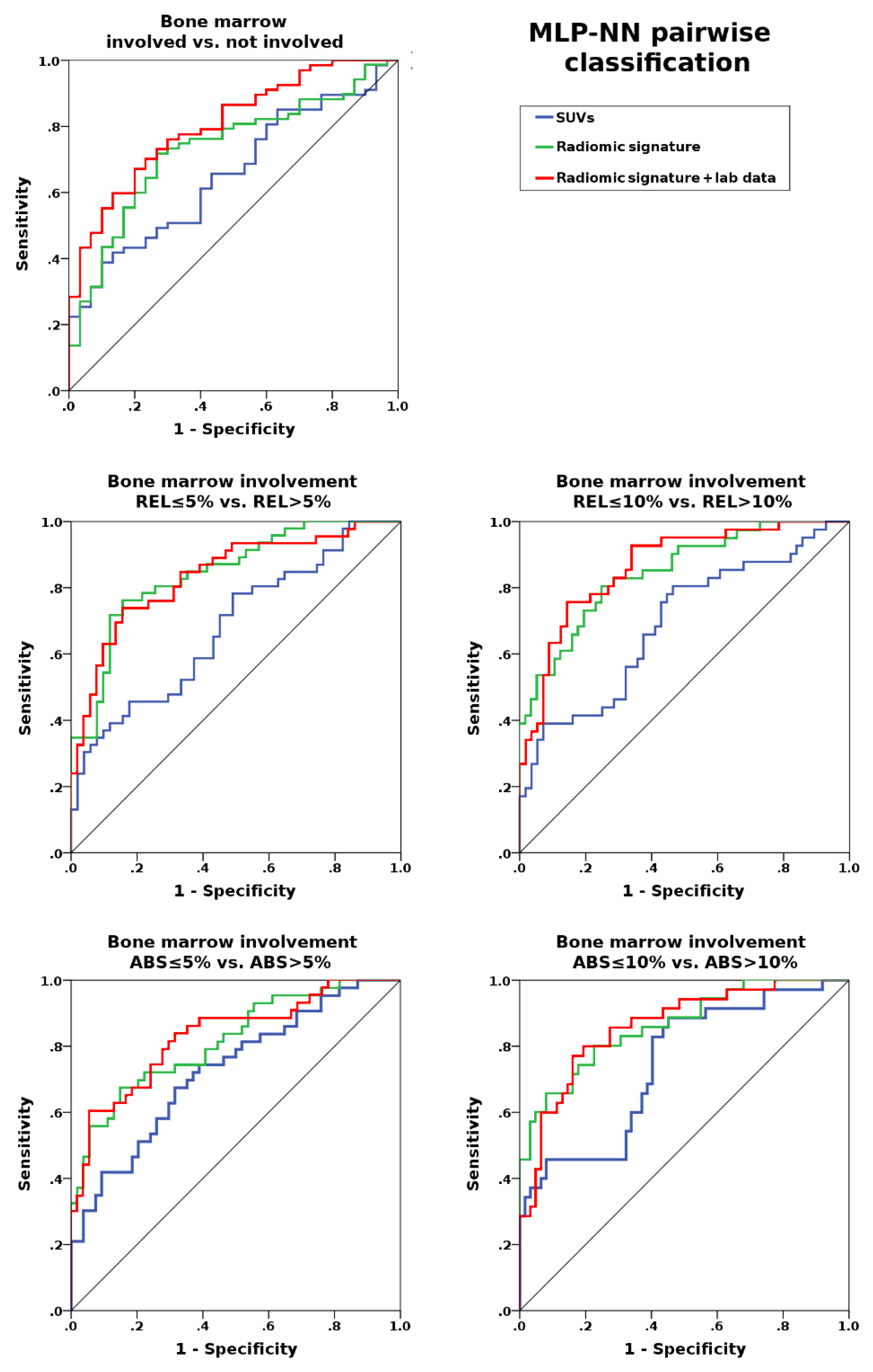
2.2. Prediction of Bone Marrow Involvement
3. Discussion
4. Materials and Methods
4.1. Patients and Design
4.2. Bone Marrow Histology—Percentage of Involvement
4.3. Imaging Protocol
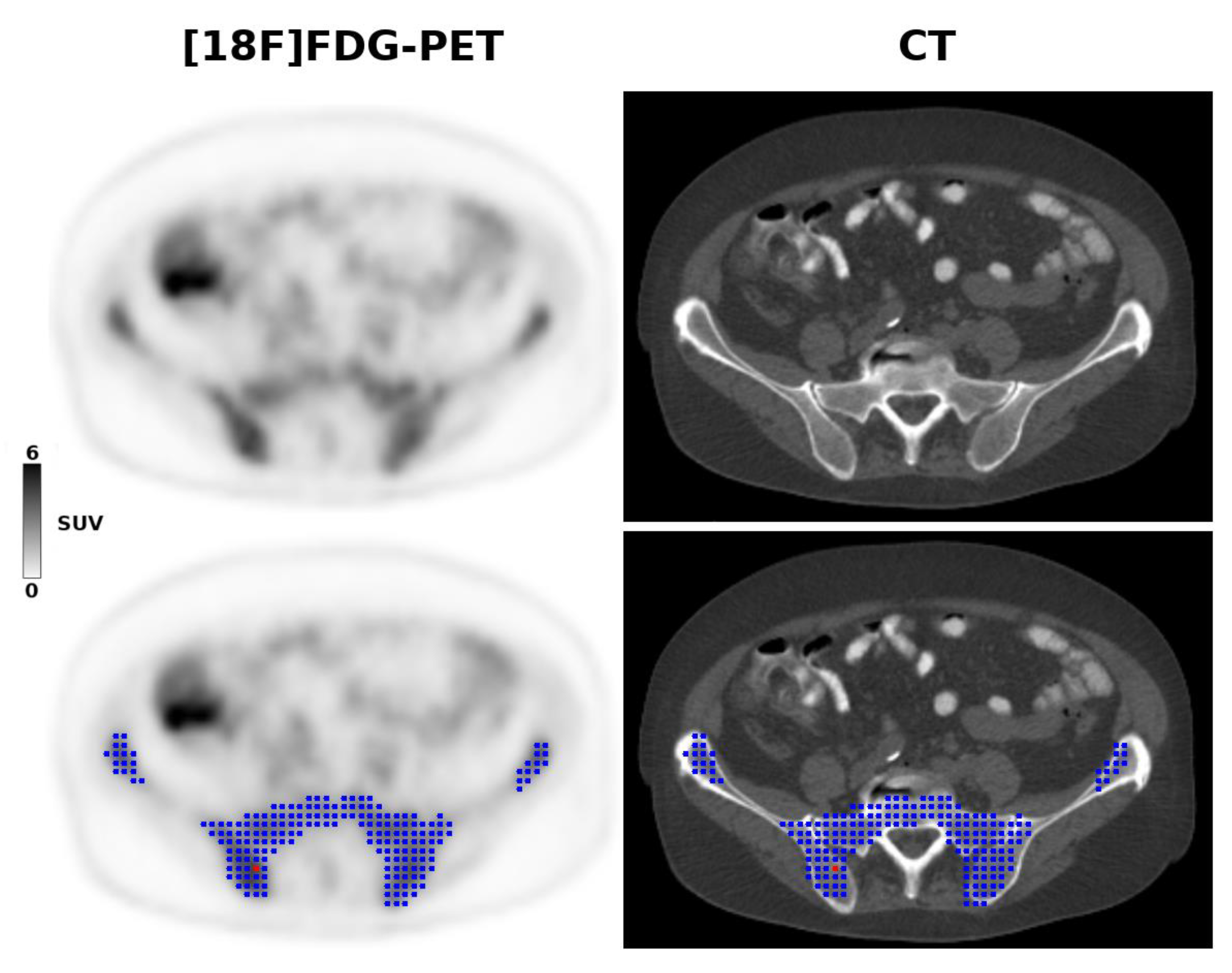
4.4. Image Analysis and Radiomic Feature Analysis
4.5. Image Analysis and Radiomic Feature Analysis
4.6. Machine Learning for Prediction of Bone Marrow Involvement
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cheson, B.D.; Fisher, R.I.; Barrington, S.F.; Cavalli, F.; Schwartz, L.H.; Zucca, E.; Lister, T.A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. JCO 2014, 32, 3059–3067. [Google Scholar] [CrossRef] [PubMed]
- El-Galaly, T.C.; d’Amore, F.; Mylam, K.J.; de Nully Brown, P.; Bøgsted, M.; Bukh, A.; Specht, L.; Loft, A.; Iyer, V.; Hjorthaug, K.; et al. Routine Bone Marrow Biopsy Has Little or No Therapeutic Consequence for Positron Emission Tomography/Computed Tomography–Staged Treatment-Naive Patients With Hodgkin Lymphoma. JCO 2012, 30, 4508–4514. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C.; de Keizer, B.; Fijnheer, R.; de Klerk, J.M.H.; Littooij, A.S.; Nievelstein, R.A.J. Systematic review and meta-analysis on the diagnostic performance of FDG-PET/CT in detecting bone marrow involvement in newly diagnosed Hodgkin lymphoma: Is bone marrow biopsy still necessary? Ann. Oncol. 2014, 25, 921–927. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.J.A.; Kwee, T.C.; de Keizer, B.; Fijnheer, R.; de Klerk, J.M.H.; Nievelstein, R.A.J. FDG PET/CT for the detection of bone marrow involvement in diffuse large B-cell lymphoma: Systematic review and meta-analysis. Eur. J. Nucl. Med. Mol. Imaging 2014, 41, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Younes, A.; Hilden, P.; Coiffier, B.; Hagenbeek, A.; Salles, G.; Wilson, W.; Seymour, J.F.; Kelly, K.; Gribben, J.; Pfreunschuh, M.; et al. International Working Group consensus response evaluation criteria in lymphoma (RECIL 2017). Ann. Oncol. 2017, 28, 1436–1447. [Google Scholar] [CrossRef] [PubMed]
- Fend, F.; Kremer, M. Diagnosis and Classification of Malignant Lymphoma and Related Entities in the Bone Marrow Trephine Biopsy. Pathobiology 2007, 74, 133–143. [Google Scholar] [CrossRef]
- Dreyling, M.; Thieblemont, C.; Gallamini, A.; Arcaini, L.; Campo, E.; Hermine, O.; Kluin-Nelemans, J.C.; Ladetto, M.; Le Gouill, S.; Iannitto, E.; et al. ESMO Consensus conferences: Guidelines on malignant lymphoma. part 2: Marginal zone lymphoma, mantle cell lymphoma, peripheral T-cell lymphoma. Ann. Oncol. 2013, 24, 857–877. [Google Scholar] [CrossRef]
- Paes, F.M.; Kalkanis, D.G.; Sideras, P.A.; Serafini, A.N. FDG PET/CT of Extranodal Involvement in Non-Hodgkin Lymphoma and Hodgkin Disease. RadioGraphics 2010, 30, 269–291. [Google Scholar] [CrossRef]
- Hosein, P.J.; Pastorini, V.H.; Paes, F.M.; Eber, D.; Chapman, J.R.; Serafini, A.N.; Alizadeh, A.A.; Lossos, I.S. Utility of positron emission tomography scans in mantle cell lymphoma. Am. J. Hematol. 2011, 86, 841–845. [Google Scholar] [CrossRef]
- Bodet-Milin, C.; Touzeau, C.; Leux, C.; Sahin, M.; Moreau, A.; Maisonneuve, H.; Morineau, N.; Jardel, H.; Moreau, P.; Gallazini-Crépin, C.; et al. Prognostic impact of 18F-fluoro-deoxyglucose positron emission tomography in untreated mantle cell lymphoma: A retrospective study from the GOELAMS group. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 1633–1642. [Google Scholar] [CrossRef]
- Albano, D.; Ferro, P.; Bosio, G.; Fallanca, F.; Re, A.; Tucci, A.; Maria Ferreri, A.J.; Angelillo, P.; Gianolli, L.; Giubbini, R.; et al. Diagnostic and Clinical Impact of Staging 18F-FDG PET/CT in Mantle-Cell Lymphoma: A Two-Center Experience. Clin. Lymphoma Myeloma Leuk. 2019, 19, e457–e464. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Treglia, G.; Gazzilli, M.; Cerudelli, E.; Giubbini, R.; Bertagna, F. 18F-FDG PET or PET/CT in Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2020, S2152265020300653. [Google Scholar] [CrossRef] [PubMed]
- Albano, D.; Laudicella, R.; Ferro, P.; Allocca, M.; Abenavoli, E.; Buschiazzo, A.; Castellino, A.; Chiaravalloti, A.; Cuccaro, A.; Cuppari, L.; et al. The Role of 18F-FDG PET/CT in Staging and Prognostication of Mantle Cell Lymphoma: An Italian Multicentric Study. Cancers 2019, 11, 1831. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillies, R.J.; Kinahan, P.E.; Hricak, H. Radiomics: Images Are More than Pictures, They Are Data. Radiology 2016, 278, 563–577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailly, C.; Bodet-Milin, C.; Bourgeois, M.; Gouard, S.; Ansquer, C.; Barbaud, M.; Sébille, J.-C.; Chérel, M.; Kraeber-Bodéré, F.; Carlier, T. Exploring Tumor Heterogeneity Using PET Imaging: The Big Picture. Cancers 2019, 11, 1282. [Google Scholar] [CrossRef] [Green Version]
- Sala, E.; Mema, E.; Himoto, Y.; Veeraraghavan, H.; Brenton, J.D.; Snyder, A.; Weigelt, B.; Vargas, H.A. Unravelling tumour heterogeneity using next-generation imaging: Radiomics, radiogenomics, and habitat imaging. Clin. Radiol. 2017, 72, 3–10. [Google Scholar] [CrossRef] [Green Version]
- Moon, S.H.; Kim, J.; Joung, J.-G.; Cha, H.; Park, W.-Y.; Ahn, J.S.; Ahn, M.-J.; Park, K.; Choi, J.Y.; Lee, K.-H.; et al. Correlations between metabolic texture features, genetic heterogeneity, and mutation burden in patients with lung cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 446–454. [Google Scholar] [CrossRef]
- Choi, E.-R.; Lee, H.Y.; Jeong, J.Y.; Choi, Y.-L.; Kim, J.; Bae, J.; Lee, K.S.; Shim, Y.M. Quantitative image variables reflect the intratumoral pathologic heterogeneity of lung adenocarcinoma. Oncotarget 2016, 7, 67302. [Google Scholar] [CrossRef] [Green Version]
- Meyer, H.J.; Leifels, L.; Hamerla, G.; Höhn, A.K.; Surov, A. Histogram Analysis Parameters Derived from Conventional T1- and T2-Weighted Images Can Predict Different Histopathological Features Including Expression of Ki67, EGFR, VEGF, HIF-1α, and p53 and Cell Count in Head and Neck Squamous Cell Carcinoma. Mol. Imaging Biol. 2019, 21, 740–746. [Google Scholar] [CrossRef]
- Meyer, H.-J.; Schob, S.; Höhn, A.K.; Surov, A. MRI Texture Analysis Reflects Histopathology Parameters in Thyroid Cancer—A First Preliminary Study. Transl. Oncol. 2017, 10, 911–916. [Google Scholar] [CrossRef]
- Cook, G.J.R.; Goh, V. What can artificial intelligence teach us about the molecular mechanisms underlying disease? Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2715–2721. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aide, N.; Talbot, M.; Fruchart, C.; Damaj, G.; Lasnon, C. Diagnostic and prognostic value of baseline FDG PET/CT skeletal textural features in diffuse large B cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 699–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lambin, P.; Leijenaar, R.T.H.; Deist, T.M.; Peerlings, J.; de Jong, E.E.C.; van Timmeren, J.; Sanduleanu, S.; Larue, R.T.H.M.; Even, A.J.G.; Jochems, A.; et al. Radiomics: The bridge between medical imaging and personalized medicine. Nat. Rev. Clin. Oncol. 2017, 14, 749–762. [Google Scholar] [CrossRef] [PubMed]
- Lidén, Y.; Landgren, O.; Arnér, S.; Sjölund, K.-F.; Johansson, E. Procedure-related pain among adult patients with hematologic malignancies. Acta Anaesthesiol. Scand. 2009, 53, 354–363. [Google Scholar] [CrossRef]
- Morgan, R.; Perry, M.; Kwak, J.; Jensen, A.; Kamdar, M. Positron Emission Tomography-based Analysis Can Accurately Predict Bone Marrow Involvement With Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2018, 18, 731–736. [Google Scholar] [CrossRef]
- Adams, H.J.A.; Kwee, T.C.; Fijnheer, R.; Dubois, S.V.; Blase, P.E.; Nievelstein, R.A.J.; de Klerk, J.M.H. Utility of quantitative FDG-PET/CT for the detection of bone marrow involvement in follicular lymphoma: A histopathological correlation study. Skelet. Radiol. 2014, 43, 1231–1236. [Google Scholar] [CrossRef]
- El-Najjar, I.; Montoto, S.; McDowell, A.; Matthews, J.; Gribben, J.; Szyszko, T.A. The value of semiquantitative analysis in identifying diffuse bone marrow involvement in follicular lymphoma. Nucl. Med. Commun. 2014, 35, 311–315. [Google Scholar] [CrossRef]
- Asenbaum, U.; Nolz, R.; Karanikas, G.; Furtner, J.; Woitek, R.; Simonitsch-Klupp, I.; Raderer, M.; Mayerhoefer, M.E. Bone Marrow Involvement in Malignant Lymphoma. Acad. Radiol. 2018, 25, 453–460. [Google Scholar] [CrossRef]
- Öner, A.O.; Sürer Budak, E.; Aydın, F.; Salim, O.; Yücel, O.K.; Akkaya, B.; Toptaş, T.; Boz, A.; Yıldız, A.; Güngör, F.; et al. Efficacy of 18F-2-fluoro-2-deoxy-D-glucose Positron Emission Tomography/Computerized Tomography for Bone Marrow Infiltration Assessment in the Initial Staging of Lymphoma. Mirt 2017, 26, 69–75. [Google Scholar] [CrossRef]
- Lv, W.; Yuan, Q.; Wang, Q.; Ma, J.; Feng, Q.; Chen, W.; Rahmim, A.; Lu, L. Radiomics Analysis of PET and CT Components of PET/CT Imaging Integrated with Clinical Parameters: Application to Prognosis for Nasopharyngeal Carcinoma. Mol. Imaging Biol. 2019, 21, 954–964. [Google Scholar] [CrossRef]
- Mu, W.; Tunali, I.; Gray, J.E.; Qi, J.; Schabath, M.B.; Gillies, R.J. Radiomics of 18F-FDG PET/CT images predicts clinical benefit of advanced NSCLC patients to checkpoint blockade immunotherapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 47, 1168–1182. [Google Scholar] [CrossRef] [PubMed]
- Mayerhoefer, M.E.; Riedl, C.C.; Kumar, A.; Gibbs, P.; Weber, M.; Tal, I.; Schilksy, J.; Schöder, H. Radiomic features of glucose metabolism enable prediction of outcome in mantle cell lymphoma. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2760–2769. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoster, E.; Rosenwald, A.; Berger, F.; Bernd, H.-W.; Hartmann, S.; Loddenkemper, C.; Barth, T.F.E.; Brousse, N.; Pileri, S.; Rymkiewicz, G.; et al. Prognostic Value of Ki-67 Index, Cytology, and Growth Pattern in Mantle-Cell Lymphoma: Results From Randomized Trials of the European Mantle Cell Lymphoma Network. JCO 2016, 34, 1386–1394. [Google Scholar] [CrossRef] [PubMed]
- Zwanenburg, A.; Leger, S.; Vallières, M.; Löck, S. Image biomarker standardisation initiative. arXiv 2020, arXiv:1612.07003. [Google Scholar]
- Haubold, J.; Demircioglu, A.; Gratz, M.; Glas, M.; Wrede, K.; Sure, U.; Antoch, G.; Keyvani, K.; Nittka, M.; Kannengiesser, S.; et al. Non-invasive tumor decoding and phenotyping of cerebral gliomas utilizing multiparametric 18F-FET PET-MRI and MR Fingerprinting. Eur. J. Nucl. Med. Mol. Imaging 2019, 47, 1435–1445. [Google Scholar] [CrossRef] [PubMed]
- Schiano, C.; Franzese, M.; Pane, K.; Garbino, N.; Soricelli, A.; Salvatore, M.; de Nigris, F.; Napoli, C. Hybrid 18F-FDG-PET/MRI Measurement of Standardized Uptake Value Coupled with Yin Yang 1 Signature in Metastatic Breast Cancer. A Preliminary Study. Cancers 2019, 11, 1444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baiocco, S.; Sah, B.-R.; Mallia, A.; Kelly-Morland, C.; Neji, R.; Stirling, J.J.; Jeljeli, S.; Bevilacqua, A.; Cook, G.J.R.; Goh, V. Exploratory radiomic features from integrated 18F-fluorodeoxyglucose positron emission tomography/magnetic resonance imaging are associated with contemporaneous metastases in oesophageal/gastroesophageal cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1478–1484. [Google Scholar] [CrossRef] [Green Version]
- Giannini, V.; Mazzetti, S.; Bertotto, I.; Chiarenza, C.; Cauda, S.; Delmastro, E.; Bracco, C.; Di Dia, A.; Leone, F.; Medico, E.; et al. Predicting locally advanced rectal cancer response to neoadjuvant therapy with 18F-FDG PET and MRI radiomics features. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 878–888. [Google Scholar] [CrossRef]
- Berthet, L.; Cochet, A.; Kanoun, S.; Berriolo-Riedinger, A.; Humbert, O.; Toubeau, M.; Dygai-Cochet, I.; Legouge, C.; Casasnovas, O.; Brunotte, F. In Newly Diagnosed Diffuse Large B-Cell Lymphoma, Determination of Bone Marrow Involvement with 18F-FDG PET/CT Provides Better Diagnostic Performance and Prognostic Stratification Than Does Biopsy. J. Nucl. Med. 2013, 54, 1244–1250. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, R.; Nishio, M.; Do, R.K.G.; Togashi, K. Convolutional neural networks: An overview and application in radiology. Insights Imaging 2018, 9, 611–629. [Google Scholar] [CrossRef] [Green Version]
- Swerdlow, S.H.; Campo, E.; Pileri, S.A.; Harris, N.L.; Stein, H.; Siebert, R.; Advani, R.; Ghielmini, M.; Salles, G.A.; Zelenetz, A.D.; et al. The 2016 revision of the World Health Organization classification of lymphoid neoplasms. Blood 2016, 127, 2375–2390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanoun, S.; Tal, I.; Berriolo-Riedinger, A.; Rossi, C.; Riedinger, J.-M.; Vrigneaud, J.-M.; Legrand, L.; Humbert, O.; Casasnovas, O.; Brunotte, F.; et al. Influence of Software Tool and Methodological Aspects of Total Metabolic Tumor Volume Calculation on Baseline [18F]FDG PET to Predict Survival in Hodgkin Lymphoma. PLoS ONE 2015, 10, e0140830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boellaard, R.; O’Doherty, M.J.; Weber, W.A.; Mottaghy, F.M.; Lonsdale, M.N.; Stroobants, S.G.; Oyen, W.J.G.; Kotzerke, J.; Hoekstra, O.S.; Pruim, J.; et al. FDG PET and PET/CT: EANM procedure guidelines for tumour PET imaging: Version 1.0. Eur. J. Nucl. Med. Mol. Imaging 2010, 37, 181–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haralick, R.M.; Shanmugam, K.; Dinstein, I. Textural Features for Image Classification. IEEE Trans. Syst. ManCybern. 1973, SMC-3, 610–621. [Google Scholar] [CrossRef] [Green Version]
- Orlhac, F.; Boughdad, S.; Philippe, C.; Stalla-Bourdillon, H.; Nioche, C.; Champion, L.; Soussan, M.; Frouin, F.; Frouin, V.; Buvat, I. A Postreconstruction Harmonization Method for Multicenter Radiomic Studies in PET. J. Nucl. Med. 2018, 59, 1321–1328. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteritsic | Entire Population (97 Patients) | Training Cohort (68 Patients) | Test Cohort (29 Patients) |
|---|---|---|---|
| Age | 63.5 ± 12.5 | 64.3 ± 12.8 | 61.6 ± 11.8 |
| Female | 31/97 (32.0%) | 20/68 (29.4%) | 11/29 (37.9%) |
| Ann Arbor Stage | |||
| I–II | 14/97 (14.4%) | 12/68 (17.6%) | 2/29 (6.9%) |
| II–IV | 83/97 (85.6%) | 56/68 (82.4%) | 27/29 (93.1%) |
| Blastoid differentiation | 21/97 (21.6%) | 15/68 (22.1%) | 6/29 (20.7%) |
| Blastic | 18/97 (18.6%) | 12/68 (17.6%) | 6/29 (20.7%) |
| Pleomorphic | 3/97 (3.1%) | 3/68 (4.4%) | 0/29 (0%) |
| WBC (×109/L) | 10.5 ± 11.9 | 10.2 ± 12.4 | 10.7 ± 11.0 |
| LDH (U/L) | 232.3 ± 86.0 | 236.4 ± 97.2 | 222.4 ± 51.4 |
| ECOG ≥ 2 | 9/97 (9.3%) | 6/68 (8.8%) | 3/29 (10.3%) |
| Bone marrow involvement | 67/97 (69.1%) | 47/67 (70.1%) | 20/29 (70.0%) |
| REL | 33.0 ± 29.1% | 33.0 ± 29.6% | 32.9 ± 28.6% |
| ABS | 22.6 ± 23.6% | 24.5 ± 22.6% | 21.8 ± 22.0% |
| Ki-67 | 28.9 ± 23.7% | 29.3 ± 24.6% | 28.0 ± 22.0% |
| Metrics | Training Accuracy Median (Range) % | Test Accuracy Median (Range) % | AUC Median (Range) % |
|---|---|---|---|
| SUVs: | |||
| BMB pos. vs. BMB neg. | 69.1 (69.1–70.6) | 69.0 (69.0–69-0) | 0.61 (0.60–0.66) |
| REL ≤ 5% vs. REL > 5% | 54.4 (51.5–58.8) | 72.4 (69.0–72.4) | 0.68 (0.68–0.68) |
| REL ≤ 10% vs. REL > 10% | 69.1 (61.8–70.6) | 69.0 (65.5–72.4) | 0.69 (0.68–0.69) |
| ABS ≤ 5% vs. ABS > 5% | 61.8 (61.8–66.2) | 72.4 (69.0–75.9) | 0.70 (0.69–0.73) |
| ABS ≤ 10% vs. ABS > 10% | 69.1 (67.6–70.6) | 89.7 (86.2–89.7) | 0.75 (0.74–0.75) |
| Radiomics signature: | |||
| BMB pos. vs. BMB neg. | 70.6 (69.1–72.1) | 72.4 (69.0–72.4) | 0.68 (0.61–0.73) |
| REL ≤5 % vs. REL > 5% | 70.6 (66.2–76.5) | 79.3 (79.3–82.8) | 0.77 (0.75–0.84) |
| REL ≤ 10% vs. REL > 10% | 76.5 (72.1–76.5) | 75.9 (72.4–79.3) | 0.80 (0.79–0.85) |
| ABS ≤ 5% vs. ABS > 5% | 73.5 (67.6–73.5) | 72.4 (69.0–79.3) | 0.81 (0.77–0.82) |
| ABS ≤ 10% vs. ABS > 10% | 79.4 (77.8–82.4) | 82.8 (79.3–86.2) | 0.85 (0.83–0.86) |
| Radiomics + Laboratory: | |||
| BMB pos. vs. BMB neg. | 76.5 (71.2–82.4) | 72.4 (69.0–75.9) | 0.76 (0.71–0.81) |
| REL ≤ 5% vs. REL > 5% | 70.6 (67.6–72.1) | 82.8 (79.3–93.1) | 0.82 (0.81–0.84) |
| REL ≤ 10% vs. REL > 10% | 77.9 (71.1–80.9) | 75.9 (72.4–79.3) | 0.84 (0.82–0.87) |
| ABS ≤ 5% vs. ABS > 5% | 75.0 (70.6–79.4) | 75.9 (72.4–79.3) | 0.81 (0.79–0.83) |
| ABS ≤ 10% vs. ABS > 10% | 79.4 (72.1–80.9) | 79.3 (75.0–82.8) | 0.84 (0.82–0.86) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mayerhoefer, M.E.; Riedl, C.C.; Kumar, A.; Dogan, A.; Gibbs, P.; Weber, M.; Staber, P.B.; Huicochea Castellanos, S.; Schöder, H. [18F]FDG-PET/CT Radiomics for Prediction of Bone Marrow Involvement in Mantle Cell Lymphoma: A Retrospective Study in 97 Patients. Cancers 2020, 12, 1138. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051138
Mayerhoefer ME, Riedl CC, Kumar A, Dogan A, Gibbs P, Weber M, Staber PB, Huicochea Castellanos S, Schöder H. [18F]FDG-PET/CT Radiomics for Prediction of Bone Marrow Involvement in Mantle Cell Lymphoma: A Retrospective Study in 97 Patients. Cancers. 2020; 12(5):1138. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051138
Chicago/Turabian StyleMayerhoefer, Marius E., Christopher C. Riedl, Anita Kumar, Ahmet Dogan, Peter Gibbs, Michael Weber, Philipp B. Staber, Sandra Huicochea Castellanos, and Heiko Schöder. 2020. "[18F]FDG-PET/CT Radiomics for Prediction of Bone Marrow Involvement in Mantle Cell Lymphoma: A Retrospective Study in 97 Patients" Cancers 12, no. 5: 1138. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12051138