The Evolution of Care of Cancers of the Head and Neck Region: State of the Science in 2020

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Head and Neck Squamous Cell Carcinoma
2.1. Epidemiology, Prevention, and Surveillance
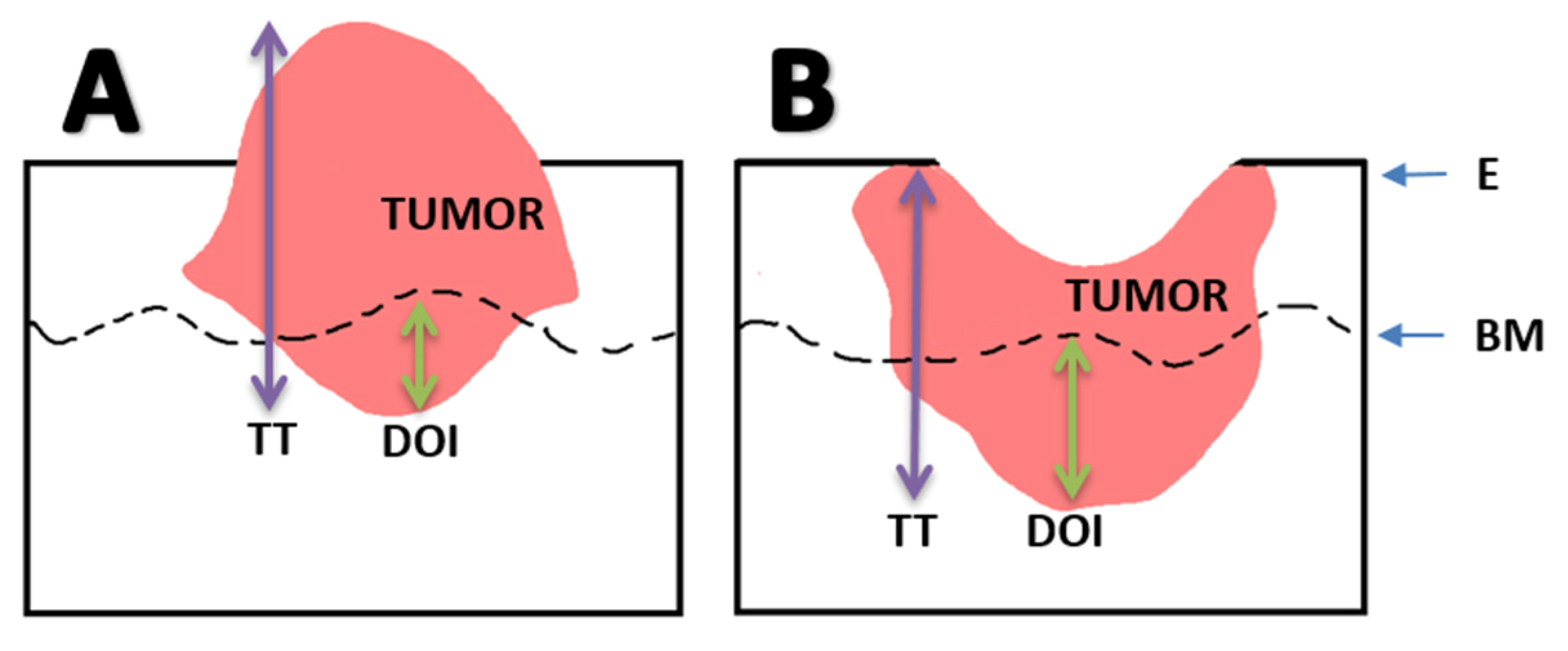
2.2. Updates from the 8th edition of the American Joint Committee on Cancer Staging System
2.3. Treatment
2.3.1. Robotic Surgery
2.3.2. Systemic Therapy
2.3.3. Treatment De-Intensification in HPV-Positive OPSCC
3. Skin Cancer
3.1. Basal Cell Carcinoma
3.2. Cutaneous Squamous Cell Carcinoma
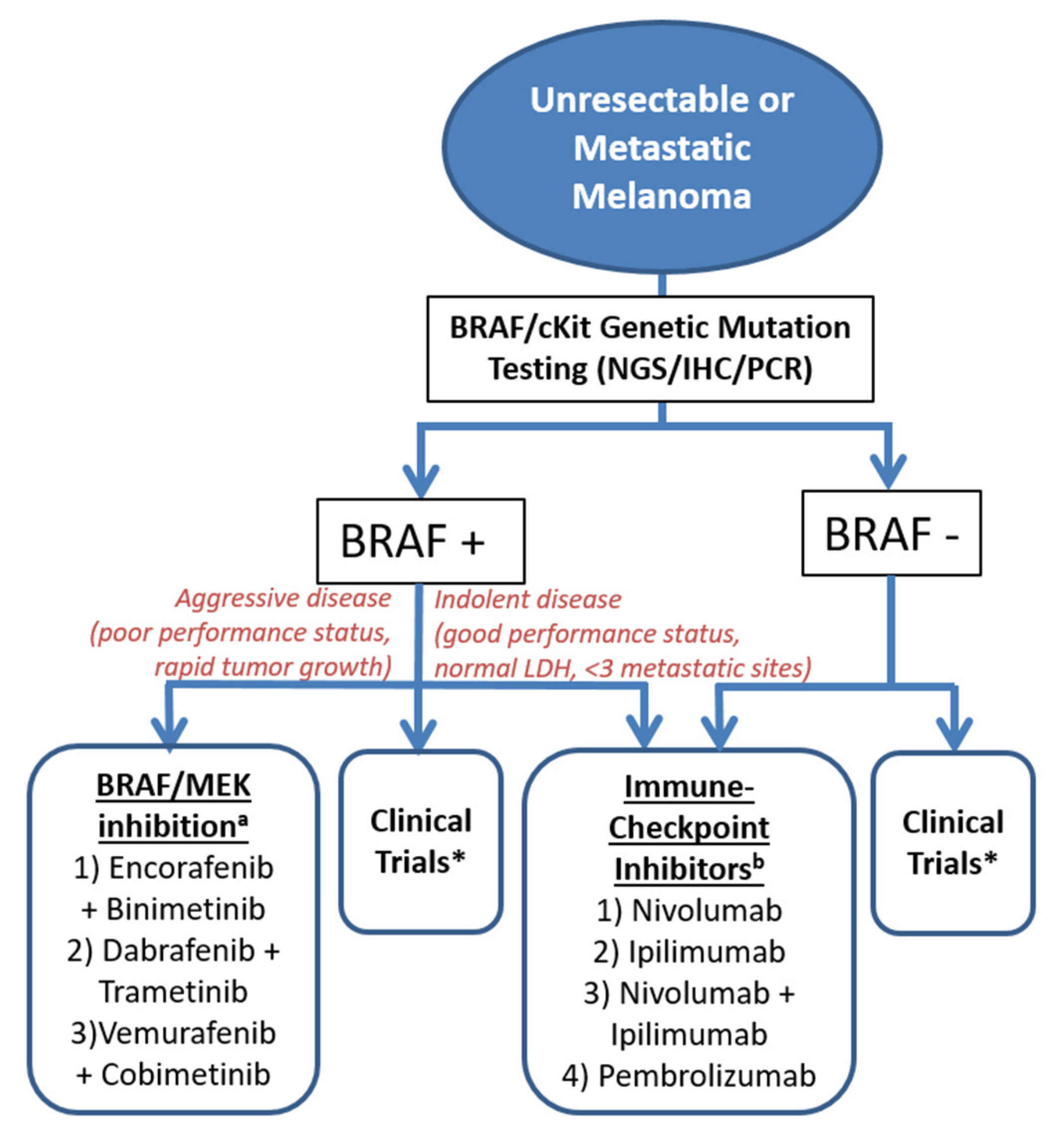
3.3. Cutaneous Melanoma
3.4. Merkel Cell Carcinoma
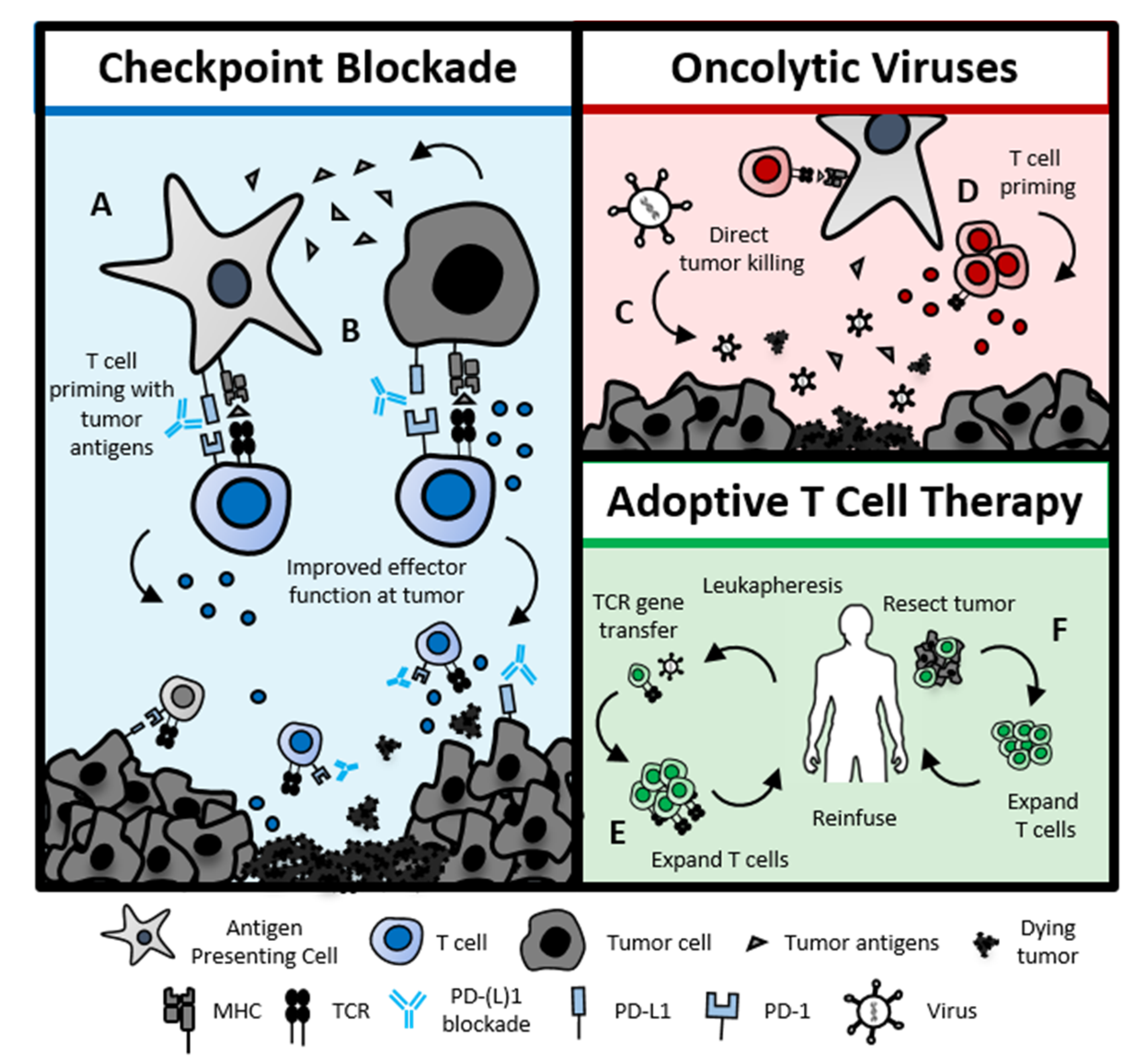
4. Emerging Developments—Immunotherapy
5. Emerging Developments: Radiation Therapy
6. Emerging Developments: Cancer Survivorship
7. Emerging Developments: Care during the COVID-19 Era
8. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Wu, Y.S.; Lin, P.Y.; Chien, C.Y.; Fang, F.M.; Chiu, N.M.; Hung, C.F.; Lee, Y.; Chong, M.Y. Anxiety and depression in patients with head and neck cancer: 6-month follow-up study. Neuropsychiatr. Dis. Treat. 2016, 12, 1029–1036. [Google Scholar] [CrossRef] [Green Version]
- List, M.A.; Stracks, J. Evaluation of quality of life in patients definitively treated for squamous carcinoma of the head and neck. Curr. Opin. Oncol. 2000, 12. [Google Scholar] [CrossRef] [PubMed]
- Hanna, E. How fragile we are. Head Neck 2020, 42, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- American Cancer Society. Cancer Statistics Center. Available online: https://cancerstatisticscenter.cancer.org (accessed on 23 January 2020).
- Cohen, N.; Fedewa, S.; Chen, A.Y. Epidemiology and Demographics of the Head and Neck Cancer Population. Oral Maxillofac. Surg. Clin. N. Am. 2018, 30, 381–395. [Google Scholar] [CrossRef] [PubMed]
- Sharma, D.; Sharma, N.; Sharma, V. Sinonasal Cancers: Diagnosis and Management. In Challenging Issues on Paranasal Sinuses; Wang, T., Ed.; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Chow, L.Q.M. Head and Neck Cancer. N. Engl. J. Med. 2020, 382, 60–72. [Google Scholar] [CrossRef]
- Chua, M.L.K.; Wee, J.T.S.; Hui, E.P.; Chan, A.T.C. Nasopharyngeal carcinoma. Lancet 2016, 387, 1012–1024. [Google Scholar] [CrossRef]
- Robbins, K.T.; Ferlito, A.; Silver, C.E.; Takes, R.P.; Strojan, P.; Snyderman, C.H.; de Bree, R.; Haigentz, M., Jr.; Langendijk, J.A.; Rinaldo, A.; et al. Contemporary management of sinonasal cancer. Head Neck 2011, 33, 1352–1365. [Google Scholar] [CrossRef]
- Tota, J.E.; Best, A.F.; Zumsteg, Z.S.; Gillison, M.L.; Rosenberg, P.S.; Chaturvedi, A.K. Evolution of the Oropharynx Cancer Epidemic in the United States: Moderation of Increasing Incidence in Younger Individuals and Shift in the Burden to Older Individuals. J. Clin. Oncol. 2019, 37, 1538–1546. [Google Scholar] [CrossRef]
- Mahal, B.A.; Catalano, P.J.; Haddad, R.I.; Hanna, G.J.; Kass, J.I.; Schoenfeld, J.D.; Tishler, R.B.; Margalit, D.N. Incidence and Demographic Burden of HPV-Associated Oropharyngeal Head and Neck Cancers in the United States. Cancer Epidemiol. Biomark. Prev. 2019, 28, 1660–1667. [Google Scholar] [CrossRef] [Green Version]
- Rettig, E.M.; Zaidi, M.; Faraji, F.; Eisele, D.W.; El Asmar, M.; Fung, N.; D’Souza, G.; Fakhry, C. Oropharyngeal cancer is no longer a disease of younger patients and the prognostic advantage of Human Papillomavirus is attenuated among older patients: Analysis of the National Cancer Database. Oral. Oncol. 2018, 83, 147–153. [Google Scholar] [CrossRef]
- D’Souza, G.; Westra, W.H.; Wang, S.J.; van Zante, A.; Wentz, A.; Kluz, N.; Rettig, E.; Ryan, W.R.; Ha, P.K.; Kang, H.; et al. Differences in the Prevalence of Human Papillomavirus (HPV) in Head and Neck Squamous Cell Cancers by Sex, Race, Anatomic Tumor Site, and HPV Detection Method. JAMA Oncol. 2017, 3, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Faraji, F.; Rettig, E.M.; Tsai, H.-L.; El Asmar, M.; Fung, N.; Eisele, D.W.; Fakhry, C. The prevalence of human papillomavirus in oropharyngeal cancer is increasing regardless of sex or race, and the influence of sex and race on survival is modified by human papillomavirus tumor status. Cancer 2019, 125, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K.; Graubard, B.I.; Broutian, T.; Pickard, R.K.L.; Tong, Z.Y.; Xiao, W.; Kahle, L.; Gillison, M.L. Effect of Prophylactic Human Papillomavirus (HPV) Vaccination on Oral HPV Infections Among Young Adults in the United States. J. Clin. Oncol. 2018, 36, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Hadaya, J.; Schumm, M.; Livingston, E.H. Testing Individuals for Coronavirus Disease 2019 (COVID-19). JAMA 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control, Prevention (US). Epidemiology and Prevention of Vaccine-Preventable Diseases, 13th ed., Supplement ed.; Hamborsky, J., Kroger, A., Wolfe, C., Eds.; Public Health Foundation: Washington, DC, USA, 2017. [Google Scholar]
- Reagan-Steiner, S.; Yankey, D.; Jeyarajah, J.; Elam-Evans, L.D.; Curtis, C.R.; MacNeil, J.; Markowitz, L.E.; Singleton, J.A. National, Regional, State, and Selected Local Area Vaccination Coverage Among Adolescents Aged 13–17 Years—United States, 2015. Morb. Mortal. Wkly. Rep. 2016, 65, 850–858. [Google Scholar] [CrossRef]
- Trosman, S.J.; Koyfman, S.A.; Ward, M.C.; Al-Khudari, S.; Nwizu, T.; Greskovich, J.F.; Lamarre, E.D.; Scharpf, J.; Khan, M.J.; Lorenz, R.R.; et al. Effect of human papillomavirus on patterns of distant metastatic failure in oropharyngeal squamous cell carcinoma treated with chemoradiotherapy. JAMA Otolaryngol. Head Neck Surg. 2015, 141, 457–462. [Google Scholar] [CrossRef] [Green Version]
- Faraji, F.; Eisele, D.W.; Fakhry, C. Emerging insights into recurrent and metastatic human papillomavirus-related oropharyngeal squamous cell carcinoma. Laryngoscope Investig. Otolaryngol. 2017, 2, 10–18. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Blackford, A.L.; Neuner, G.; Xiao, W.; Jiang, B.; Agrawal, A.; Gillison, M.L. Association of Oral Human Papillomavirus DNA Persistence With Cancer Progression After Primary Treatment for Oral Cavity and Oropharyngeal Squamous Cell Carcinoma. JAMA Oncol. 2019, 5, 985–992. [Google Scholar] [CrossRef]
- Chera, B.S.; Kumar, S.; Shen, C.; Amdur, R.; Dagan, R.; Green, R.; Goldman, E.; Weiss, J.; Grilley-Olson, J.; Patel, S.; et al. Plasma Circulating Tumor HPV DNA for the Surveillance of Cancer Recurrence in HPV-Associated Oropharyngeal Cancer. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef]
- AJCC Cancer Staging Manual, 8th ed.; Springer International Publishing; American Joint Commission on Cancer: New York, NY, USA, 2017.
- Ang, K.K.; Harris, J.; Wheeler, R.; Weber, R.; Rosenthal, D.I.; Nguyen-Tân, P.F.; Westra, W.H.; Chung, C.H.; Jordan, R.C.; Lu, C.; et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N. Engl. J. Med. 2010, 363, 24–35. [Google Scholar] [CrossRef] [Green Version]
- Fakhry, C.; Westra, W.H.; Li, S.; Cmelak, A.; Ridge, J.A.; Pinto, H.; Forastiere, A.; Gillison, M.L. Improved Survival of Patients With Human Papillomavirus–Positive Head and Neck Squamous Cell Carcinoma in a Prospective Clinical Trial. J. Natl. Cancer Inst. 2008, 100, 261–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lydiatt, W.M.; Patel, S.G.; O’Sullivan, B.; Brandwein, M.S.; Ridge, J.A.; Migliacci, J.C.; Loomis, A.M.; Shah, J.P. Head and Neck cancers-major changes in the American Joint Committee on cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 122–137. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Head and Neck Cancer (Version 3.2019). Available online: https://www.nccn.org/professionals/physician_gls/pdf/head-and-neck_blocks.pdf (accessed on 24 February 2020).
- Chernock, R.D.; Lewis, J.S. Approach to metastatic carcinoma of unknown primary in the head and neck: Squamous cell carcinoma and beyond. Head Neck Pathol. 2015, 9, 6–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maghami, E.; Ismaila, N.; Alvarez, A.; Chernock, R.; Duvvuri, U.; Geiger, J.; Gross, N.; Haughey, B.; Paul, D.; Rodriguez, C.; et al. Diagnosis and Management of Squamous Cell Carcinoma of Unknown Primary in the Head and Neck: ASCO Guideline. J. Clin. Oncol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Motz, K.; Qualliotine, J.R.; Rettig, E.; Richmon, J.D.; Eisele, D.W.; Fakhry, C. Changes in Unknown Primary Squamous Cell Carcinoma of the Head and Neck at Initial Presentation in the Era of Human Papillomavirus. JAMA Otolaryngol. Head Neck Surg. 2016, 142, 223–228. [Google Scholar] [CrossRef] [Green Version]
- Haas, I.; Hoffmann, T.K.; Engers, R.; Ganzer, U. Diagnostic strategies in cervical carcinoma of an unknown primary (CUP). Eur. Arch. Oto-Rhino-Laryngol. 2002, 259, 325–333. [Google Scholar] [CrossRef]
- Berdugo, J.; Thompson, L.D.R.; Purgina, B.; Sturgis, C.D.; Tuluc, M.; Seethala, R.; Chiosea, S.I. Measuring Depth of Invasion in Early Squamous Cell Carcinoma of the Oral Tongue: Positive Deep Margin, Extratumoral Perineural Invasion, and Other Challenges. Head Neck Pathol. 2019, 13, 154–161. [Google Scholar] [CrossRef]
- D’Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef]
- Pentenero, M.; Gandolfo, S.; Carrozzo, M. Importance of tumor thickness and depth of invasion in nodal involvement and prognosis of oral squamous cell carcinoma: A review of the literature. Head Neck 2005, 27, 1080–1091. [Google Scholar] [CrossRef]
- Almangush, A.; Salo, T. The 8th Edition of the American Joint Committee on Cancer (AJCC8) Staging Manual: Any improvement in the prognostication of oral tongue cancer? Chin. Clin. Oncol. 2019, 8, S8. [Google Scholar] [CrossRef] [Green Version]
- Mascitti, M.; Rubini, C.; De Michele, F.; Balercia, P.; Girotto, R.; Troiano, G.; Lo Muzio, L.; Santarelli, A. American Joint Committee on Cancer staging system 7th edition versus 8th edition: Any improvement for patients with squamous cell carcinoma of the tongue? Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Bigelow, E.O.; Seiwert, T.Y.; Fakhry, C. Deintensification of treatment for human papillomavirus-related oropharyngeal cancer: Current state and future directions. Oral Oncol. 2020, 105, 104652. [Google Scholar] [CrossRef] [PubMed]
- Golusiński, W. Functional Organ Preservation Surgery in Head and Neck Cancer: Transoral Robotic Surgery and Beyond. Front. Oncol. 2019, 9. [Google Scholar] [CrossRef] [PubMed]
- Evans, G.R.; Williams, J.Z.; Ainslie, N.B. Cutaneous nasal malignancies: Is primary reconstruction safe? Head Neck 1997, 19, 182–187. [Google Scholar] [CrossRef]
- Kelly, K.; Johnson-Obaseki, S.; Lumingu, J.; Corsten, M. Oncologic, functional and surgical outcomes of primary Transoral Robotic Surgery for early squamous cell cancer of the oropharynx: A systematic review. Oral Oncol. 2014, 50, 696–703. [Google Scholar] [CrossRef]
- De Almeida, J.R.; Byrd, J.K.; Wu, R.; Stucken, C.L.; Duvvuri, U.; Goldstein, D.P.; Miles, B.A.; Teng, M.S.; Gupta, V.; Genden, E.M. A systematic review of transoral robotic surgery and radiotherapy for early oropharynx cancer: A systematic review. Laryngoscope 2014, 124, 2096–2102. [Google Scholar] [CrossRef] [PubMed]
- Baskin, R.M.; Boyce, B.J.; Amdur, R.; Mendenhall, W.M.; Hitchcock, K.; Silver, N.; Dziegielewski, P.T. Transoral robotic surgery for oropharyngeal cancer: Patient selection and special considerations. Cancer Manag. Res. 2018, 10, 839–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeh, D.H.; Tam, S.; Fung, K.; MacNeil, S.D.; Yoo, J.; Winquist, E.; Palma, D.A.; Nichols, A.C. Transoral robotic surgery vs. radiotherapy for management of oropharyngeal squamous cell carcinoma—A systematic review of the literature. Eur. J. Surg. Oncol. (EJSO) 2015, 41, 1603–1614. [Google Scholar] [CrossRef] [PubMed]
- Nichols, A.C.; Theurer, J.; Prisman, E.; Read, N.; Berthelet, E.; Tran, E.; Fung, K.; de Almeida, J.R.; Bayley, A.; Goldstein, D.P.; et al. Radiotherapy versus transoral robotic surgery and neck dissection for oropharyngeal squamous cell carcinoma (ORATOR): An open-label, phase 2, randomised trial. Lancet Oncol. 2019, 20, 1349–1359. [Google Scholar] [CrossRef]
- Margalit, D.N.; Karam, S.D.; Chua, M.L.K.; Anderson, C.; Kimple, R.J. Four Influential Clinical Trials in Human Papilloma Virus-Associated Oropharynx Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 893–899. [Google Scholar] [CrossRef]
- Nichols, A.C.; Lang, P.; Prisman, E.; Berthelet, E.; Tran, E.; Hamilton, S.; Wu, J.; Fung, K.; de Almeida, J.R.; Bayley, A.; et al. Treatment de-escalation for HPV-associated oropharyngeal squamous cell carcinoma with radiotherapy vs. trans-oral surgery (ORATOR2): Study protocol for a randomized phase II trial. BMC Cancer 2020, 20, 125. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Noronha, V.; Joshi, A.; Patil, V.M.; Agarwal, J.; Ghosh-Laskar, S.; Budrukkar, A.; Murthy, V.; Gupta, T.; D’Cruz, A.K.; Banavali, S.; et al. Once-a-Week Versus Once-Every-3-Weeks Cisplatin Chemoradiation for Locally Advanced Head and Neck Cancer: A Phase III Randomized Noninferiority Trial. J. Clin. Oncol. 2018, 36, 1064–1072. [Google Scholar] [CrossRef]
- Rivera, F.; García-Castaño, A.; Vega, N.; Vega-Villegas, M.E.; Gutiérrez-Sanz, L. Cetuximab in metastatic or recurrent head and neck cancer: The EXTREME trial. Expert Rev. Anticancer Ther. 2009, 9, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Bonner, J.A.; Harari, P.M.; Giralt, J.; Azarnia, N.; Shin, D.M.; Cohen, R.B.; Jones, C.U.; Sur, R.; Raben, D.; Jassem, J.; et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 2006, 354, 567–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermorken, J.B.; Mesia, R.; Rivera, F.; Remenar, E.; Kawecki, A.; Rottey, S.; Erfan, J.; Zabolotnyy, D.; Kienzer, H.R.; Cupissol, D.; et al. Platinum-based chemotherapy plus cetuximab in head and neck cancer. N. Engl. J. Med. 2008, 359, 1116–1127. [Google Scholar] [CrossRef] [Green Version]
- Gillison, M.L.; Trotti, A.M.; Harris, J.; Eisbruch, A.; Harari, P.M.; Adelstein, D.J.; Jordan, R.C.K.; Zhao, W.; Sturgis, E.M.; Burtness, B.; et al. Radiotherapy plus cetuximab or cisplatin in human papillomavirus-positive oropharyngeal cancer (NRG Oncology RTOG 1016): A randomised, multicentre, non-inferiority trial. Lancet 2019, 393, 40–50. [Google Scholar] [CrossRef]
- Mehanna, H.; Robinson, M.; Hartley, A.; Kong, A.; Foran, B.; Fulton-Lieuw, T.; Dalby, M.; Mistry, P.; Sen, M.; O’Toole, L.; et al. Radiotherapy plus cisplatin or cetuximab in low-risk human papillomavirus-positive oropharyngeal cancer (De-ESCALaTE HPV): An open-label randomised controlled phase 3 trial. Lancet 2019, 393, 51–60. [Google Scholar] [CrossRef] [Green Version]
- Siu, L.L.; Waldron, J.N.; Chen, B.E.; Winquist, E.; Wright, J.R.; Nabid, A.; Hay, J.H.; Ringash, J.; Liu, G.; Johnson, A.; et al. Effect of Standard Radiotherapy With Cisplatin vs Accelerated Radiotherapy With Panitumumab in Locoregionally Advanced Squamous Cell Head and Neck Carcinoma: A Randomized Clinical Trial. JAMA Oncol. 2017, 3, 220–226. [Google Scholar] [CrossRef]
- Ang, K.K.; Zhang, Q.; Rosenthal, D.I.; Nguyen-Tan, P.F.; Sherman, E.J.; Weber, R.S.; Galvin, J.M.; Bonner, J.A.; Harris, J.; El-Naggar, A.K.; et al. Randomized phase III trial of concurrent accelerated radiation plus cisplatin with or without cetuximab for stage III to IV head and neck carcinoma: RTOG 0522. J. Clin. Oncol. 2014, 32, 2940–2950. [Google Scholar] [CrossRef]
- Hargadon, K.M.; Johnson, C.E.; Williams, C.J. Immune checkpoint blockade therapy for cancer: An overview of FDA-approved immune checkpoint inhibitors. Int. Immunopharmacol. 2018, 62, 29–39. [Google Scholar] [CrossRef]
- Ferris, R.L.; Blumenschein, G., Jr.; Fayette, J.; Guigay, J.; Colevas, A.D.; Licitra, L.; Harrington, K.J.; Kasper, S.; Vokes, E.E.; Even, C.; et al. Nivolumab vs investigator’s choice in recurrent or metastatic squamous cell carcinoma of the head and neck: 2-year long-term survival update of CheckMate 141 with analyses by tumor PD-L1 expression. Oral Oncol. 2018, 81, 45–51. [Google Scholar] [CrossRef] [PubMed]
- Burtness, B.; Harrington, K.J.; Greil, R.; Soulières, D.; Tahara, M.; de Castro, G., Jr.; Psyrri, A.; Basté, N.; Neupane, P.; Bratland, Å.; et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): A randomised, open-label, phase 3 study. Lancet 2019, 394, 1915–1928. [Google Scholar] [CrossRef]
- Oliva, M.; Spreafico, A.; Taberna, M.; Alemany, L.; Coburn, B.; Mesia, R.; Siu, L.L. Immune biomarkers of response to immune-checkpoint inhibitors in head and neck squamous cell carcinoma. Ann. Oncol. 2019, 30, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Gomez Serrano, M.; Patel, S.; Harris, R.; Selvadurai, D. Initial surgical and clinical experience with the Nucleus CI532 slim modiolar electrode in the UK. Cochlear Implant. Int. 2019. [Google Scholar] [CrossRef]
- Troiano, G.; Caponio, V.C.A.; Zhurakivska, K.; Arena, C.; Pannone, G.; Mascitti, M.; Santarelli, A.; Lo Muzio, L. High PD-L1 expression in the tumour cells did not correlate with poor prognosis of patients suffering for oral squamous cells carcinoma: A meta-analysis of the literature. Cell Prolif. 2019, 52, e12537. [Google Scholar] [CrossRef] [Green Version]
- Hanna, G.J.; Lizotte, P.; Cavanaugh, M.; Kuo, F.C.; Shivdasani, P.; Frieden, A.; Chau, N.G.; Schoenfeld, J.D.; Lorch, J.H.; Uppaluri, R.M.; et al. Frameshift events predict anti-PD-1/L1 response in head and neck cancer. JCI Insight 2018, 3. [Google Scholar] [CrossRef] [Green Version]
- Scholfield, D.W.; Gujral, D.M.; Awad, Z. Transoral Robotic Surgery for Oropharyngeal Squamous Cell Carcinoma: Improving Function While Maintaining Oncologic Outcome. Otolaryngol. Head Neck Surg. 2020, 162, 267–268. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Huang, S.H.; Siu, L.L.; Waldron, J.; Zhao, H.; Perez-Ordonez, B.; Weinreb, I.; Kim, J.; Ringash, J.; Bayley, A.; et al. Deintensification candidate subgroups in human papillomavirus-related oropharyngeal cancer according to minimal risk of distant metastasis. J. Clin Oncol. 2013, 31, 543–550. [Google Scholar] [CrossRef]
- O’Sullivan, B.; Huang, S.H.; Perez-Ordonez, B.; Massey, C.; Siu, L.L.; Weinreb, I.; Hope, A.; Kim, J.; Bayley, A.J.; Cummings, B.; et al. Outcomes of HPV-related oropharyngeal cancer patients treated by radiotherapy alone using altered fractionation. Radiother. Oncol. 2012, 103, 49–56. [Google Scholar] [CrossRef]
- Villaflor, V.M.; Melotek, J.M.; Karrison, T.G.; Brisson, R.J.; Blair, E.A.; Portugal, L.; De Souza, J.A.; Ginat, D.T.; Stenson, K.M.; Langerman, A.; et al. Response-adapted volume de-escalation (RAVD) in locally advanced head and neck cancer. Ann. Oncol. 2016, 27, 908–913. [Google Scholar] [CrossRef]
- Chen, A.M.; Felix, C.; Wang, P.-C.; Hsu, S.; Basehart, V.; Garst, J.; Beron, P.; Wong, D.; Rosove, M.H.; Rao, S.; et al. Reduced-dose radiotherapy for human papillomavirus-associated squamous-cell carcinoma of the oropharynx: A single-arm, phase 2 study. Lancet Oncol. 2017, 18, 803–811. [Google Scholar] [CrossRef] [Green Version]
- Seiwert, T.Y.; Foster, C.C.; Blair, E.A.; Karrison, T.G.; Agrawal, N.; Melotek, J.M.; Portugal, L.; Brisson, R.J.; Dekker, A.; Kochanny, S.; et al. OPTIMA: A phase II dose and volume de-escalation trial for human papillomavirus-positive oropharyngeal cancer. Ann. Oncol. 2019, 30, 297–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misiukiewicz, K.; Gupta, V.; Miles, B.A.; Bakst, R.; Genden, E.; Selkridge, I.; Surgeon, J.T.; Rainey, H.; Camille, N.; Roy, E.; et al. Standard of care vs reduced-dose chemoradiation after induction chemotherapy in HPV+ oropharyngeal carcinoma patients: The Quarterback trial. Oral Oncol. 2019, 95, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Li, S.; Cmelak, A.J.; Gillison, M.L.; Zhao, W.J.; Ferris, R.L.; Westra, W.H.; Gilbert, J.; Bauman, J.E.; Wagner, L.I.; et al. E1308: Phase II Trial of Induction Chemotherapy Followed by Reduced-Dose Radiation and Weekly Cetuximab in Patients With HPV-Associated Resectable Squamous Cell Carcinoma of the Oropharynx—ECOG-ACRIN Cancer Research Group. J. Clin. Oncol. 2016, 35, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Ma, D.J.; Price, K.A.; Moore, E.J.; Patel, S.H.; Hinni, M.L.; Garcia, J.J.; Graner, D.E.; Foster, N.R.; Ginos, B.; Neben-Wittich, M.; et al. Phase II Evaluation of Aggressive Dose De-Escalation for Adjuvant Chemoradiotherapy in Human Papillomavirus–Associated Oropharynx Squamous Cell Carcinoma. J. Clin. Oncol. 2019, 37, 1909–1918. [Google Scholar] [CrossRef]
- Swisher-McClure, S.; Lukens, J.N.; Aggarwal, C.; Ahn, P.; Basu, D.; Bauml, J.M.; Brody, R.; Chalian, A.; Cohen, R.B.; Fotouhi-Ghiam, A.; et al. A Phase 2 Trial of Alternative Volumes of Oropharyngeal Irradiation for De-intensification (AVOID): Omission of the Resected Primary Tumor Bed After Transoral Robotic Surgery for Human Papilloma Virus–Related Squamous Cell Carcinoma of the Oropharynx. Int. J. Radiat. Oncol. Biol. Phys. 2020, 106, 725–732. [Google Scholar] [CrossRef]
- Chera, B.S.; Amdur, R.J.; Tepper, J.E.; Tan, X.; Weiss, J.; Grilley-Olson, J.E.; Hayes, D.N.; Zanation, A.; Hackman, T.G.; Patel, S.; et al. Mature results of a prospective study of deintensified chemoradiotherapy for low-risk human papillomavirus-associated oropharyngeal squamous cell carcinoma. Cancer 2018, 124, 2347–2354. [Google Scholar] [CrossRef] [Green Version]
- Chera, B.S.; Amdur, R.J.; Green, R.; Shen, C.; Gupta, G.; Tan, X.; Knowles, M.; Fried, D.; Hayes, N.; Weiss, J.; et al. Phase II Trial of De-Intensified Chemoradiotherapy for Human Papillomavirus–Associated Oropharyngeal Squamous Cell Carcinoma. J. Clin. Oncol. 2019, 37, 2661–2669. [Google Scholar] [CrossRef]
- Clinicaltrials.gov. De-intensified Radiation Therapy With Chemotherapy (Cisplatin) or Immunotherapy (Nivolumab) in Treating Patients With Early-Stage, HPV-Positive, Non-Smoking Associated Oropharyngeal Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03952585 (accessed on 27 April 2020).
- Clinicaltrials.gov. Major De-escalation to 30 Gy for Select Human Papillomavirus Associated Oropharyngeal Carcinoma (NCT03323463). Available online: https://clinicaltrials.gov/ct2/show/NCT03323463 (accessed on 25 April 2020).
- Clinicaltrials.gov. Individualized Adaptive De-escalated Radiotherapy for HPV-related Oropharynx Cancer (NCT03416153). Available online: https://clinicaltrials.gov/ct2/show/NCT03416153?term=NCT03416153&draw=2&rank=1 (accessed on 25 April 2020).
- Clinicaltrials.gov. Adaptive Treatment De-escalation in Favorable Risk HPV-Positive Oropharyngeal Carcinoma (NCT03215719). Available online: https://clinicaltrials.gov/ct2/show/NCT03215719?term=NCT03215719&draw=2&rank=1 (accessed on 25 April 2020).
- Clinicaltrials.gov. Trial of Magnetic Resonance Imaging Guided Radiotherapy Dose Adaptation in Human Papilloma Virus Positive Oropharyngeal Cancer (NCT03224000). Available online: https://clinicaltrials.gov/ct2/show/NCT03224000?term=NCT03224000&draw=2&rank=1 (accessed on 25 April 2020).
- Rubin, A.I.; Chen, E.H.; Ratner, D. Basal-cell carcinoma. N. Engl. J. Med. 2005, 353, 2262–2269. [Google Scholar] [CrossRef]
- Mydlarz, W.K.; Weber, R.S.; Kupferman, M.E. Cutaneous malignancy of the head and neck. Surg. Oncol. Clin. N. Am. 2015, 24, 593–613. [Google Scholar] [CrossRef]
- Silverman, M.K.; Kopf, A.W.; Bart, R.S.; Grin, C.M.; Levenstein, M.S. Recurrence Rates of Treated Basal Cell Carcinomas. J. Dermatol. Surg. Oncol. 1992, 18, 471–476. [Google Scholar] [CrossRef] [PubMed]
- Connolly, S.M.; Baker, D.R.; Coldiron, B.M.; Fazio, M.J.; Storrs, P.A.; Vidimos, A.T.; Zalla, M.J.; Brewer, J.D.; Smith Begolka, W.; Berger, T.G.; et al. AAD/ACMS/ASDSA/ASMS 2012 appropriate use criteria for Mohs micrographic surgery: A report of the American Academy of Dermatology, American College of Mohs Surgery, American Society for Dermatologic Surgery Association, and the American Society for Mohs Surgery. J. Am. Acad. Dermatol. 2012, 67, 531–550. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Squamous Cell Skin Cancer (Version 1.2020). Available online: https://www.nccn.org/professionals/physician_gls/pdf/squamous.pdf (accessed on 10 June 2020).
- Gantz, B.J.; McCabe, B.F.; Tyler, R.S. Use of multichannel cochlear implants in obstructed and obliterated cochleas. Otolaryngol. Head Neck Surg. 1988, 98, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Kronenberg, J.; Migirov, L. Is mastoidectomy indispensable in cochlear implant surgery? J. Otolaryngol. 2005, 34, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Sekulic, A.; Migden, M.R.; Lewis, K.; Hainsworth, J.D.; Solomon, J.A.; Yoo, S.; Arron, S.T.; Friedlander, P.A.; Marmur, E.; Rudin, C.M.; et al. Pivotal ERIVANCE basal cell carcinoma (BCC) study: 12-month update of efficacy and safety of vismodegib in advanced BCC. J. Am. Acad. Dermatol. 2015, 72, 1021–1026.e1028. [Google Scholar] [CrossRef]
- Basset-Seguin, N.; Hauschild, A.; Grob, J.J.; Kunstfeld, R.; Dreno, B.; Mortier, L.; Ascierto, P.A.; Licitra, L.; Dutriaux, C.; Thomas, L.; et al. Vismodegib in patients with advanced basal cell carcinoma (STEVIE): A pre-planned interim analysis of an international, open-label trial. Lancet. Oncol. 2015, 16, 729–736. [Google Scholar] [CrossRef]
- National Institute of Health. Topical Remetinostat in Treating Patient With Cutaneous Basal Cell Cancer. Available online: https://clinicaltrials.gov/ct2/show/NCT03180528?term=NCT03180528&draw=2&rank=1 (accessed on 22 April 2020).
- National Institute of Health. PD-1 in Patients With Advanced Basal Cell Carcinoma Who Experienced Progression of Disease on Hedgehog Pathway Inhibitor Therapy, or Were Intolerant of Prior Hedgehog Pathway Inhibitor Therapy. Available online: https://clinicaltrials.gov/ct2/show/NCT03132636?term=NCT03132636&draw=2&rank=1 (accessed on 22 April 2020).
- National Institute of Health. Nivolumab Alone or Plus Ipilimumab for Patients With Locally-Advanced Unresectable or Metastatic Basal Cell Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03521830?term=NCT03521830&draw=2&rank=1 (accessed on 22 April 2020).
- Bander, T.S.; Nehal, K.S.; Lee, E.H. Cutaneous Squamous Cell Carcinoma: Updates in Staging and Management. Dermatol. Clin. 2019, 37, 241–251. [Google Scholar] [CrossRef]
- Cañueto, J.; Burguillo, J.; Moyano-Bueno, D.; Viñolas-Cuadros, A.; Conde-Ferreirós, A.; Corchete-Sánchez, L.A.; Pérez-Losada, J.; Román-Curto, C. Comparing the eighth and the seventh editions of the American Joint Committee on Cancer staging system and the Brigham and Women’s Hospital alternative staging system for cutaneous squamous cell carcinoma: Implications for clinical practice. J. Am. Acad. Dermatol. 2019, 80, 106–113.e102. [Google Scholar] [CrossRef]
- Karia, P.S.; Jambusaria-Pahlajani, A.; Harrington, D.P.; Murphy, G.F.; Qureshi, A.A.; Schmults, C.D. Evaluation of American Joint Committee on Cancer, International Union Against Cancer, and Brigham and Women’s Hospital tumor staging for cutaneous squamous cell carcinoma. J. Clin. Oncol. 2014, 32, 327–334. [Google Scholar] [CrossRef] [Green Version]
- Ruiz, E.S.; Karia, P.S.; Besaw, R.; Schmults, C.D. Performance of the American Joint Committee on Cancer Staging Manual, 8th Edition vs the Brigham and Women’s Hospital Tumor Classification System for Cutaneous Squamous Cell Carcinoma. JAMA Dermatol. 2019, 155, 819–825. [Google Scholar] [CrossRef]
- Haksever, M.; Akduman, D.; Demir, M.; Aslan, S.; Yanılmaz, M.; Solmaz, F. The treatment of neck and parotid gland in cutaneous squamous cell carcinoma of face and forehead and the review of literature. Ann. Med. Surg. (Lond.) 2015, 4, 48–52. [Google Scholar] [CrossRef]
- Harris, B.N.; Pipkorn, P.; Nguyen, K.N.B.; Jackson, R.S.; Rao, S.; Moore, M.G.; Farwell, D.G.; Bewley, A.F. Association of Adjuvant Radiation Therapy With Survival in Patients With Advanced Cutaneous Squamous Cell Carcinoma of the Head and Neck. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 153–158. [Google Scholar] [CrossRef] [PubMed]
- Porceddu, S.V.; Bressel, M.; Poulsen, M.G.; Stoneley, A.; Veness, M.J.; Kenny, L.M.; Wratten, C.; Corry, J.; Cooper, S.; Fogarty, G.B.; et al. Postoperative Concurrent Chemoradiotherapy Versus Postoperative Radiotherapy in High-Risk Cutaneous Squamous Cell Carcinoma of the Head and Neck: The Randomized Phase III TROG 05.01 Trial. J. Clin. Oncol. 2018, 36, 1275–1283. [Google Scholar] [CrossRef] [PubMed]
- Lenarz, T.; Battmer, R.D.; Frohne, C.; Büchner, A.; Parker, J. The Nucleus Double Array cochlear implant for obliterated cochleae. Adv. Otorhinolaryngol. 2000, 57, 354–359. [Google Scholar] [CrossRef] [PubMed]
- Migden, M.R.; Rischin, D.; Schmults, C.D.; Guminski, A.; Hauschild, A.; Lewis, K.D.; Chung, C.H.; Hernandez-Aya, L.; Lim, A.M.; Chang, A.L.S.; et al. PD-1 Blockade with Cemiplimab in Advanced Cutaneous Squamous-Cell Carcinoma. N. Eng. J. Med. 2018, 379, 341–351. [Google Scholar] [CrossRef] [Green Version]
- National Institute of Health. Pembrolizumab Versus Placebo Following Surgery and Radiation in Participants With Locally Advanced Cutaneous Squamous Cell Carcinoma (MK-3475-630/KEYNOTE-630). Available online: https://clinicaltrials.gov/ct2/show/NCT03833167 (accessed on 24 April 2020).
- National Institute of Health. Study of Adjuvant Cemiplimab Versus Placebo After Surgery and Radiation Therapy in Patients With High Risk Cutaneous Squamous Cell Carcinoma. Available online: https://clinicaltrials.gov/ct2/show/NCT03969004 (accessed on 24 April 2020).
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA: Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2017, 67, 472–492. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gershenwald, J.E.; Morton, D.L.; Thompson, J.F.; Kirkwood, J.M.; Soong, S.; Balch, C.M.; Eggermont, A.M.; Sondak, V.K.; Johnson, M.M.; Warneke, C. Staging and prognostic factors for stage IV melanoma: Initial results of an American Joint Committee on Cancer (AJCC) international evidence-based assessment of 4,895 melanoma patients. J. Clin. Oncol. 2008, 26, 9035. [Google Scholar] [CrossRef]
- Phan, K.; Onggo, J.; Loya, A. Mohs micrographic surgery versus wide local excision for head and neck melanoma-in-situ. J. Dermatol. Treat. 2019, 1–4. [Google Scholar] [CrossRef]
- Hanson, J.; Demer, A.; Liszewski, W.; Foman, N.; Maher, I. Improved overall survival of melanoma of the head and neck treated with Mohs micrographic surgery versus wide local excision. J. Am. Acad. Dermatol. 2020, 82, 149–155. [Google Scholar] [CrossRef]
- Nosrati, A.; Berliner, J.G.; Goel, S.; McGuire, J.; Morhenn, V.; de Souza, J.R.; Yeniay, Y.; Singh, R.; Lee, K.; Nakamura, M.; et al. Outcomes of Melanoma In Situ Treated With Mohs Micrographic Surgery Compared With Wide Local Excision. JAMA Dermatol. 2017, 153, 436–441. [Google Scholar] [CrossRef] [PubMed]
- Wong, S.L.; Faries, M.B.; Kennedy, E.B.; Agarwala, S.S.; Akhurst, T.J.; Ariyan, C.; Balch, C.M.; Berman, B.S.; Cochran, A.; Delman, K.A.; et al. Sentinel Lymph Node Biopsy and Management of Regional Lymph Nodes in Melanoma: American Society of Clinical Oncology and Society of Surgical Oncology Clinical Practice Guideline Update. Ann. Surg. Oncol. 2018, 25, 356–377. [Google Scholar] [CrossRef] [PubMed]
- Cordeiro, E.; Gervais, M.-K.; Shah, P.S.; Look Hong, N.J.; Wright, F.C. Sentinel Lymph Node Biopsy in Thin Cutaneous Melanoma: A Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2016, 23, 4178–4188. [Google Scholar] [CrossRef] [PubMed]
- Balch, C.M.; Thompson, J.F.; Gershenwald, J.E.; Soong, S.-j.; Ding, S.; McMasters, K.M.; Coit, D.G.; Eggermont, A.M.M.; Gimotty, P.A.; Johnson, T.M.; et al. Age as a Predictor of Sentinel Node Metastasis among Patients with Localized Melanoma: An Inverse Correlation of Melanoma Mortality and Incidence of Sentinel Node Metastasis Among Young and Old Patients. Ann. Surg. Oncol. 2014, 21, 1075–1081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartlett, E.K.; Peters, M.G.; Blair, A.; Etherington, M.S.; Elder, D.E.; Xu, X.G.; Guerry, D.; Ming, M.E.; Fraker, D.L.; Czerniecki, B.J.; et al. Identification of Patients with Intermediate Thickness Melanoma at Low Risk for Sentinel Lymph Node Positivity. Ann. Surg. Oncol. 2016, 23, 250–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Volpe, V.O.; Klufas, D.M.; Hegde, U.; Grant-Kels, J.M. The new paradigm of systemic therapies for metastatic melanoma. J. Am. Acad. Dermatol. 2017, 77, 356–368. [Google Scholar] [CrossRef]
- Coit, D.G.; Thompson, J.A.; Albertini, M.R.; Barker, C.; Carson, W.E.; Contreras, C.; Daniels, G.A.; DiMaio, D.; Fields, R.C.; Fleming, M.D.; et al. Cutaneous Melanoma, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 367–402. [Google Scholar] [CrossRef] [Green Version]
- Sumi, M.; Nakamura, T. Extranodal spread in the neck: MRI detection on the basis of pixel-based time-signal intensity curve analysis. J. Magn. Reson. Imaging: JMRI 2011, 33, 830–838. [Google Scholar] [CrossRef]
- Hoffman La Roche. ZELBORAF (Vemurafenib) [package insert]. U.S. Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/202429s016lbl.pdf (accessed on 15 January 2020).
- Novartis. MEKINIST (Trametinib). U.S. Food and Drug Aministration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/204114s012lbl.pdf (accessed on 15 January 2020).
- Genetech Inc. COTELLIC (Cobimetinib Fumarate). U.S. Food and Drug Administration. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/206192s002lbl.pdf (accessed on 15 January 2020).
- Vonderheid, E.C.; Tan, E.T.; Kantor, A.F.; Shrager, L.; Micaily, B.; Van Scott, E.J. Long-term efficacy, curative potential, and carcinogenicity of topical mechlorethamine chemotherapy in cutaneous T cell lymphoma. J. Am. Acad. Dermatol. 1989, 20, 416–428. [Google Scholar] [CrossRef]
- Lewin, J.S.; Cleary, K.R.; Eicher, S.A. An unusual metastasis to the thumb in a laryngectomized tracheoesophageal speaker. Arch. Otolaryngol. Head Neck Surg. 1997, 123, 1007–1009. [Google Scholar] [CrossRef]
- Url, C.; Schartinger, V.H.; Riechelmann, H.; Gluckert, R.; Maier, H.; Trumpp, M.; Widmann, G. Radiological detection of extracapsular spread in head and neck squamous cell carcinoma (HNSCC) cervical metastases. Eur. J. Radiol. 2013, 82, 1783–1787. [Google Scholar] [CrossRef] [PubMed]
- Craig, M.; Lavy, J. How I do it/short communication: The middle temporal artery flap for coverage of an exposed cochlear implant cable in the mastoid cavity. Cochlear Implants Int. 2006, 7, 214–218. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, M.; Goto, T.; Kashio, A.; Yasui, T.; Sakamoto, T.; Ito, K.; Yamasoba, T. Preservation of vestibular function after scala vestibuli cochlear implantation. Auris Nasus Larynx 2011, 38, 638–642. [Google Scholar] [CrossRef] [PubMed]
- Young, K.; Minchom, A.; Larkin, J. BRIM-1, -2 and -3 trials: Improved survival with vemurafenib in metastatic melanoma patients with a BRAF(V600E) mutation. Future Oncol. (Lond., Eng.) 2012, 8, 499–507. [Google Scholar] [CrossRef]
- Hodi, F.S.; Corless, C.L.; Giobbie-Hurder, A.; Fletcher, J.A.; Zhu, M.; Marino-Enriquez, A.; Friedlander, P.; Gonzalez, R.; Weber, J.S.; Gajewski, T.F.; et al. Imatinib for melanomas harboring mutationally activated or amplified KIT arising on mucosal, acral, and chronically sun-damaged skin. J. Clin. Oncol. 2013, 31, 3182–3190. [Google Scholar] [CrossRef] [Green Version]
- Hu-Lieskovan, S.; Robert, L.; Homet Moreno, B.; Ribas, A. Combining targeted therapy with immunotherapy in BRAF-mutant melanoma: Promise and challenges. J. Clin. Oncol. 2014, 32, 2248–2254. [Google Scholar] [CrossRef] [Green Version]
- Pitale, M.; Sessions, R.B.; Husain, S. An analysis of prognostic factors in cutaneous neuroendocrine carcinoma. Laryngoscope 1992, 102, 244–249. [Google Scholar] [CrossRef]
- Medina-Franco, H.; Urist, M.M.; Fiveash, J.; Heslin, M.J.; Bland, K.I.; Beenken, S.W. Multimodality treatment of Merkel cell carcinoma: Case series and literature review of 1024 cases. Ann. Surg. Oncol. 2001, 8, 204–208. [Google Scholar] [CrossRef]
- Coggshall, K.; Tello, T.L.; North, J.P.; Yu, S.S. Merkel cell carcinoma: An update and review: Pathogenesis, diagnosis, and staging. J. Am. Acad. Dermatol. 2018, 78, 433–442. [Google Scholar] [CrossRef] [Green Version]
- Allen, P.J.; Bowne, W.B.; Jaques, D.P.; Brennan, M.F.; Busam, K.; Coit, D.G. Merkel cell carcinoma: Prognosis and treatment of patients from a single institution. J. Clin. Oncol. 2005, 23, 2300–2309. [Google Scholar] [CrossRef] [Green Version]
- Lemos, B.; Nghiem, P. Merkel Cell Carcinoma: More Deaths but Still No Pathway to Blame. J. Investig. Dermatol. 2007, 127, 2100–2103. [Google Scholar] [CrossRef] [PubMed]
- Moshiri, A.S.; Doumani, R.; Yelistratova, L.; Blom, A.; Lachance, K.; Shinohara, M.M.; Delaney, M.; Chang, O.; McArdle, S.; Thomas, H.; et al. Polyomavirus-Negative Merkel Cell Carcinoma: A More Aggressive Subtype Based on Analysis of 282 Cases Using Multimodal Tumor Virus Detection. J. Investig. Dermatol. 2017, 137, 819–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sihto, H.; Kukko, H.; Koljonen, V.; Sankila, R.; Böhling, T.; Joensuu, H. Clinical Factors Associated With Merkel Cell Polyomavirus Infection in Merkel Cell Carcinoma. JNCI: J. Natl. Cancer Inst. 2009, 101, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Tetzlaff, M.T.; Harms, P.W. Danger is only skin deep: Aggressive epidermal carcinomas. An overview of the diagnosis, demographics, molecular-genetics, staging, prognostic biomarkers, and therapeutic advances in Merkel cell carcinoma. Mod. Pathol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Tello, T.L.; Coggshall, K.; Yom, S.S.; Yu, S.S. Merkel cell carcinoma: An update and review: Current and future therapy. J. Am. Acad. Dermatol. 2018, 78, 445–454. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Merkel Cell Carcinoma (Version 1.2020). Available online: http://mdanderson.libanswers.com/faq/26180 (accessed on 15 January 2020).
- Balkany, T.; Gantz, B.J.; Steenerson, R.L.; Cohen, N.L. Systematic approach to electrode insertion in the ossified cochlea. Otolaryngol. Head Neck Surg. 1996, 114, 4–11. [Google Scholar] [CrossRef]
- National Institute of Health. Pembrolizumab Compared to Standard of Care Observation in Treating Patients With Completely Resected Stage I-III Merkel Cell Cancer, STAMP Study. Available online: https://clinicaltrials.gov/ct2/show/NCT03712605 (accessed on 24 April 2020).
- Cohen, E.E.W.; Bell, R.B.; Bifulco, C.B.; Burtness, B.; Gillison, M.L.; Harrington, K.J.; Le, Q.-T.; Lee, N.Y.; Leidner, R.; Lewis, R.L.; et al. The Society for Immunotherapy of Cancer consensus statement on immunotherapy for the treatment of squamous cell carcinoma of the head and neck (HNSCC). J. Immunother. Cancer 2019, 7, 184. [Google Scholar] [CrossRef] [Green Version]
- Harrington, K.J.; Kong, A.H.; Mach, N.; Rordorf, T.; Jaime, J.C.; Espeli, V.; Treichel, S.; Gumuscu, B.; Kim, J.J.; Chesney, J.A. Safety and preliminary efficacy of talimogene laherparepvec (T-VEC) in combination (combo) with pembrobrolizumab (Pembro) in patients (pts) with recurrent or metastatic squamous cell carcinoma of the head and neck (R/M HNSCC): A multicenter, phase 1b study (MASTERKEY-232). J. Clin. Oncol. 2018, 36, 6036. [Google Scholar] [CrossRef]
- Cohen, E.E.W.; Nabell, L.; Wong, D.J.L.; Day, T.A.; Daniels, G.A.; Milhem, M.M.; Deva, S.; Jameson, M.B.; Guntinas-Lichius, O.; Almubarak, M.; et al. Phase 1b/2, open label, multicenter study of intratumoral SD-101 in combination with pembrolizumab in anti-PD-1 treatment naïve patients with recurrent or metastatic head and neck squamous cell carcinoma (HNSCC). J. Clin. Oncol. 2019, 37, 6039. [Google Scholar] [CrossRef]
- Jazaeri, A.A.; Edwards, R.P.; Wenham, R.M.; Matsuo, K.; Fleming, G.F.; O’Malley, D.M.; Slomovitz, B.M.; Monk, B.J.; Brown, R.J.; Suzuki, S.; et al. A phase 2, multicenter study to evaluate the efficacy and safety using autologous tumor infiltrating lymphocytes (LN-145) in patients with recurrent, metastatic, or persistent cervical carcinoma. J. Clin. Oncol. 2018, 36, TPS5604. [Google Scholar] [CrossRef]
- Doran, S.L.; Stevanovic, S.; Adhikary, S.; Gartner, J.J.; Jia, L.; Kwong, M.L.M.; Faquin, W.C.; Feldman, S.; Somerville, R.; Sherry, R.M.; et al. Genetically engineered T-cell therapy for HPV-associated epithelial cancers: A first in human, phase I/II clinical trial. J. Clin. Oncol. 2018, 36, 3019. [Google Scholar] [CrossRef]
- National Institute of Health. E7 TCR T Cells for Human Papillomavirus-Associated Cancers. Available online: https://clinicaltrials.gov/ct2/show/NCT02858310 (accessed on 22 April 2020).
- Alterio, D.; Marvaso, G.; Ferrari, A.; Volpe, S.; Orecchia, R.; Jereczek-Fossa, B.A. Modern radiotherapy for head and neck cancer. Semin. Oncol. 2019, 46, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Morgan, H.E.; Sher, D.J. Adaptive radiotherapy for head and neck cancer. Cancers Head Neck 2020, 5, 1. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.; Daly, M.E.; Cui, J.; Mathai, M.; Benedict, S.; Purdy, J.A. Clinical outcomes among patients with head and neck cancer treated by intensity-modulated radiotherapy with and without adaptive replanning. Head Neck 2014, 36, 1541–1546. [Google Scholar] [CrossRef]
- Luo, Y.; Qin, Y.; Lang, J. Effect of adaptive replanning in patients with locally advanced nasopharyngeal carcinoma treated by intensity-modulated radiotherapy: A propensity score matched analysis. Clin. Transl. Oncol. 2017, 19, 470–476. [Google Scholar] [CrossRef] [PubMed]
- Cohen, E.E.; LaMonte, S.J.; Erb, N.L.; Beckman, K.L.; Sadeghi, N.; Hutcheson, K.A.; Stubblefield, M.D.; Abbott, D.M.; Fisher, P.S.; Stein, K.D.; et al. American Cancer Society Head and Neck Cancer Survivorship Care Guideline. CA Cancer J. Clin. 2016, 66, 203–239. [Google Scholar] [CrossRef]
- Windon, M.J.; D’Souza, G.; Rettig, E.M.; Westra, W.H.; van Zante, A.; Wang, S.J.; Ryan, W.R.; Mydlarz, W.K.; Ha, P.K.; Miles, B.A.; et al. Increasing prevalence of human papillomavirus–positive oropharyngeal cancers among older adults. Cancer 2018, 124, 2993–2999. [Google Scholar] [CrossRef] [Green Version]
- Windon, M.J.; Fakhry, C.; Faraji, F.; Troy, T.; Gourin, C.G.; Kiess, A.P.; Koch, W.; Eisele, D.W.; D’Souza, G. Priorities of human papillomavirus-associated oropharyngeal cancer patients at diagnosis and after treatment. Oral Oncol. 2019, 95, 11–15. [Google Scholar] [CrossRef]
- Cella, D.; Hahn, E.; Jensen, S.; Zeeshan, B.; Nowinski, C.J.; Rothrock, N.; Lohr, K.N. Patient-Rep. Outcomes Perform. Meas.; RI Press: Research Triangle Park, NC, USA, 2015. [Google Scholar]
- Lowe, D.; Rogers, S. University of Washington Quality of Life Questionnaire (UW-QOL v4 and v4.1). Available online: http://www.headandneckcancer.co.uk/sites/default/files/assets/pages/UW-QOL-update-2018.pdf (accessed on 10 June 2020).
- Chen, A.Y.; Frankowski, R.; Bishop-Leone, J.; Hebert, T.; Leyk, S.; Lewin, J.; Goepfert, H. The Development and Validation of a Dysphagia-Specific Quality-of-Life Questionnaire for Patients With Head and Neck Cancer: The M. D. Anderson Dysphagia Inventory. Arch. Otolaryngol. Head Neck Surg. 2001, 127, 870–876. [Google Scholar] [CrossRef]
- Basch, E.; Deal, A.M.; Dueck, A.C.; Scher, H.I.; Kris, M.G.; Hudis, C.; Schrag, D. Overall Survival Results of a Trial Assessing Patient-Reported Outcomes for Symptom Monitoring During Routine Cancer Treatment. JAMA 2017, 318, 197–198. [Google Scholar] [CrossRef] [Green Version]
- Zeller, J.L. High suicide risk found for patients with head and neck cancer. JAMA 2006, 296, 1716–1717. [Google Scholar] [CrossRef]
- Osazuwa-Peters, N.; Simpson, M.C.; Zhao, L.; Boakye, E.A.; Olomukoro, S.I.; Deshields, T.; Loux, T.M.; Varvares, M.A.; Schootman, M. Suicide risk among cancer survivors: Head and neck versus other cancers. Cancer 2018, 124, 4072–4079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhong, B.; Li, L.K.; Deng, D.; Du, J.T.; Liu, Y.F.; Liu, F.; Liu, S.X. Effect of High-Intensity Focused Ultrasound Versus Plasma Radiofrequency Ablation on Recurrent Allergic Rhinitis. Med. Sci. Monit. 2019, 25, 6775–6781. [Google Scholar] [CrossRef] [PubMed]
- Graboyes, E.M.; Hill, E.G.; Marsh, C.H.; Maurer, S.; Day, T.A.; Hornig, J.D.; Lentsch, E.J.; Neskey, D.M.; Skoner, J.; Sterba, K.R. Temporal Trajectory of Body Image Disturbance in Patients with Surgically Treated Head and Neck Cancer. Otolaryngol. Head Neck Surg. 2020, 162, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Health Alliance of Northern California. Survivorship Symposium. Available online: https://www.headandneck.org/symposium/ (accessed on 10 June 2020).
- Worldometer. COVID-19 Coronavirus Pandemic. Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 3 June 2020).
- Yuen, E.; Fote, G.; Horwich, P.; Nguyen, S.A.; Patel, R.; Davies, J.; Houlton, J.; Nathan, C.-A.; St. John, M.; Day, T. Head and Neck Cancer Care in the COVID-19 Pandemic: A Brief Update. Oral Oncol. 2020, 104738. [Google Scholar] [CrossRef] [PubMed]
- Houlton, J.J. Defining Optimal Treatment Times in Head and Neck Cancer Care: What Are We Waiting For? JAMA Otolaryngol. Head Neck Surg. 2019, 145, 177–178. [Google Scholar] [CrossRef] [PubMed]
- Graboyes, E.M.; Kompelli, A.R.; Neskey, D.M.; Brennan, E.; Nguyen, S.; Sterba, K.R.; Warren, G.W.; Hughes-Halbert, C.; Nussenbaum, B.; Day, T.A. Association of Treatment Delays With Survival for Patients With Head and Neck Cancer: A Systematic Review. JAMA Otolaryngol. Head Neck Surg. 2019, 145, 166–177. [Google Scholar] [CrossRef] [PubMed]
- Topf, M.C.; Shenson, J.A.; Holsinger, F.C.; Wald, S.H.; Cianfichi, L.J.; Rosenthal, E.L.; Sunwoo, J.B. A Framework for Prioritizing Head and Neck Surgery during the COVID-19 Pandemic. Head Neck 2020. [Google Scholar] [CrossRef] [PubMed]
- Ranasinghe, V.; Mady, L.J.; Kim, S.; Ferris, R.L.; Duvvuri, U.; Johnson, J.T.; Solari, M.G.; Sridharan, S.; Kubik, M. Major head and neck reconstruction during the COVID-19 pandemic: The University of Pittsburgh approach. Head Neck 2020, 42, 1243–1247. [Google Scholar] [CrossRef] [PubMed]
- Givi, B.; Schiff, B.A.; Chinn, S.B.; Clayburgh, D.; Iyer, N.G.; Jalisi, S.; Moore, M.G.; Nathan, C.-A.; Orloff, L.A.; O’Neill, J.P.; et al. Safety Recommendations for Evaluation and Surgery of the Head and Neck During the COVID-19 Pandemic. JAMA Otolaryngol. Head Neck Surg. 2020. [Google Scholar] [CrossRef] [Green Version]
- Mady, L.J.; Kubik, M.W.; Baddour, K.; Snyderman, C.H.; Rowan, N.R. Consideration of povidone-iodine as a public health intervention for COVID-19: Utilization as “Personal Protective Equipment” for frontline providers exposed in high-risk head and neck and skull base oncology care. Oral Oncol. 2020, 104724. [Google Scholar] [CrossRef] [PubMed]
- Eggers, M.; Koburger-Janssen, T.; Eickmann, M.; Zorn, J. In Vitro Bactericidal and Virucidal Efficacy of Povidone-Iodine Gargle/Mouthwash Against Respiratory and Oral Tract Pathogens. Infect. Dis. Ther. 2018, 7, 249–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abbasi, J. The Promise and Peril of Antibody Testing for COVID-19. JAMA 2020. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| T-Classification | Tumor Size and Depth of Invasion (DOI) |
|---|---|
| T1 | ≤ 2 cm and DOI ≤ 5 mm |
| T2 | ≤ 2 cm and 5 < DOI ≤ 10 mm OR >2 and ≤ 4 cm and DOI ≤ 10 mm |
| T3 | >2 and ≤ 4 cm and DOI > 10 mm OR > 4 cm and 0 < DOI ≤ 10mm |
| T4a | > 4 cm and DOI > 10 mm OR Moderately Advanced Local Disease * |
| T4b | Very Advanced Local Disease * |
| Cancer | Immunotherapy | Indication | Required Diagnostic Testing |
|---|---|---|---|
| HNSCC | Pembrolizumab (Anti-PD-1 Mab) | 1st line with FU/platinum-based therapy for treatment naïve R/M | None |
| 1st line for R/M with PD-L1 [CPS ≥1] expression | PD-L1 (+) Expression with CPS ≥ 1% | ||
| 2nd line for R/M after progression on platinum-based therapy | None | ||
| Nivolumab (Anti-PD-1 Mab) | 2nd line for R/M after progression on platinum-based therapy | ||
| MCC | Pembrolizumab (Anti-PD-1 Mab) | 1st line for R/M | |
| Avelumab (Anti-PD-L1 Mab) | 1st line for M | ||
| cSCC | Cemiplimab-rwlc (Anti-PD-1 Mab) | 1st line for LA/M | |
| Melanoma | Nivolumab (Anti-PD1 Mab) | 1st line for LA/M BRAF-WT and BRAF-MT | |
| Adjuvant tx for LN mets/M after primary resection | |||
| Nivolumab (Anti-PD1 Mab) +Ipilimumab (Anti-CTLA-4 Mab) | 1st line for LA/M BRAF-WT or BRAF-MT | ||
| Ipilimumab (Anti-CTLA-4 Mab) | 1st line for LA/M | ||
| Adjuvant tx for LN mets after primary resection and lymphadenectomy | |||
| Pembrolizumab (Anti-PD-1 Mab) | 1st line for LA/M melanoma | ||
| Adjuvant tx for LN mets after complete resection |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yan, F.; Knochelmann, H.M.; Morgan, P.F.; Kaczmar, J.M.; Neskey, D.M.; Graboyes, E.M.; Nguyen, S.A.; Ogretmen, B.; Sharma, A.K.; Day, T.A. The Evolution of Care of Cancers of the Head and Neck Region: State of the Science in 2020. Cancers 2020, 12, 1543. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061543
Yan F, Knochelmann HM, Morgan PF, Kaczmar JM, Neskey DM, Graboyes EM, Nguyen SA, Ogretmen B, Sharma AK, Day TA. The Evolution of Care of Cancers of the Head and Neck Region: State of the Science in 2020. Cancers. 2020; 12(6):1543. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061543
Chicago/Turabian StyleYan, Flora, Hannah M. Knochelmann, Patrick F. Morgan, John M. Kaczmar, David M. Neskey, Evan M. Graboyes, Shaun A. Nguyen, Besim Ogretmen, Anand K. Sharma, and Terry A. Day. 2020. "The Evolution of Care of Cancers of the Head and Neck Region: State of the Science in 2020" Cancers 12, no. 6: 1543. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061543