Prophylactic Central Lymph Node Dissection Improves Disease-Free Survival in Patients with Intermediate and High Risk Differentiated Thyroid Carcinoma: A Retrospective Analysis on 399 Patients

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Outcome of the Study
2.2. Preoperative Evaluation
2.3. Surgical Treatment
2.4. Pathologic Examination
2.5. Postoperative Management and Follow-Up
2.6. Statistical Analysis
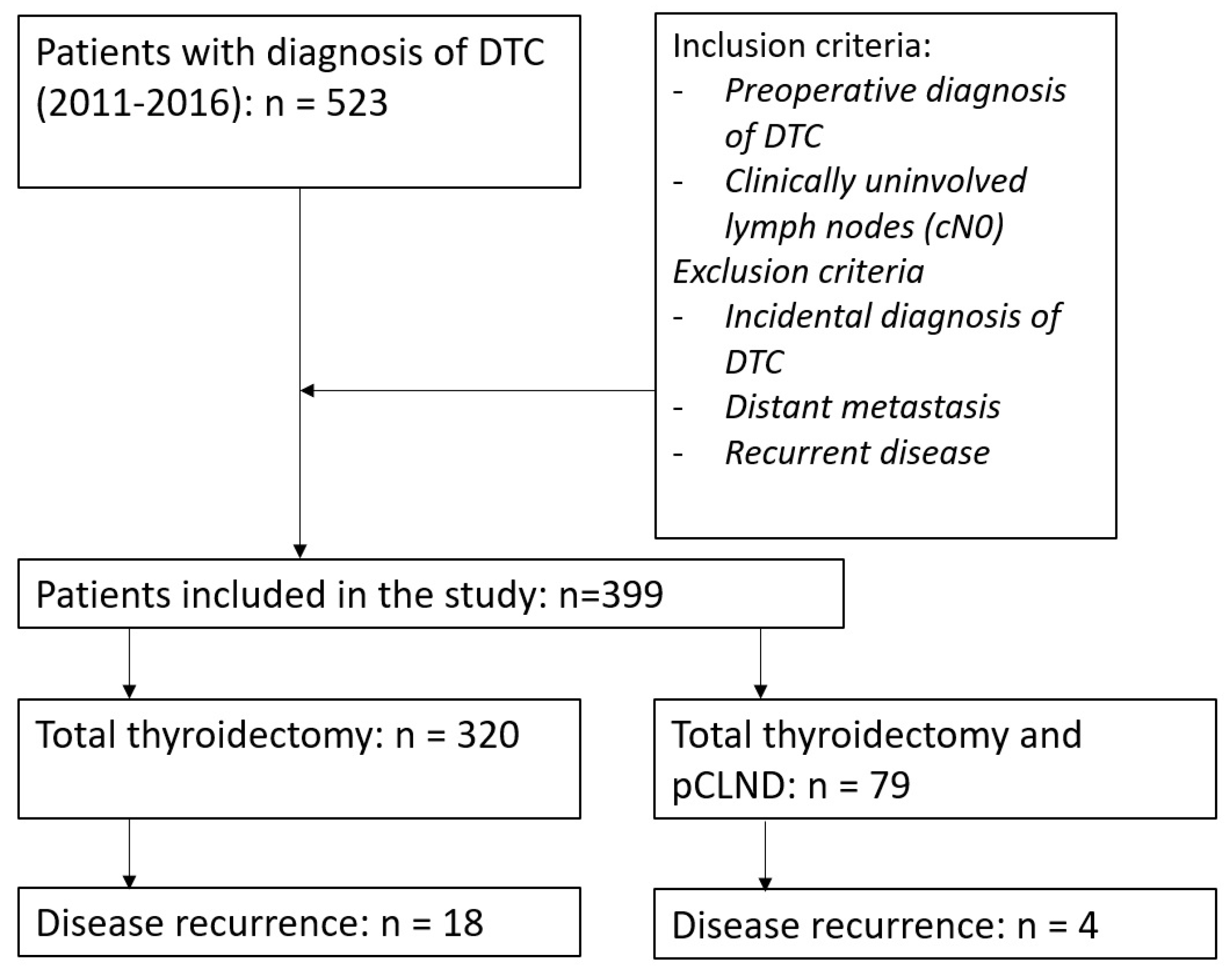
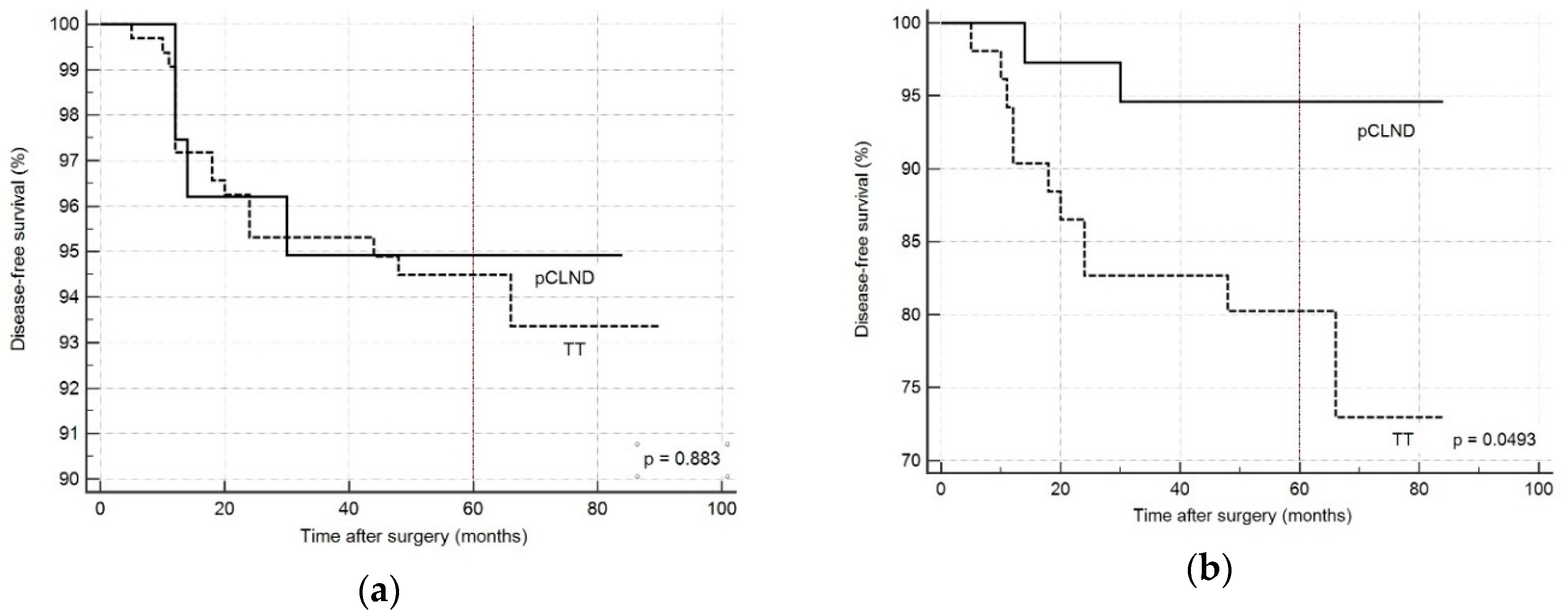
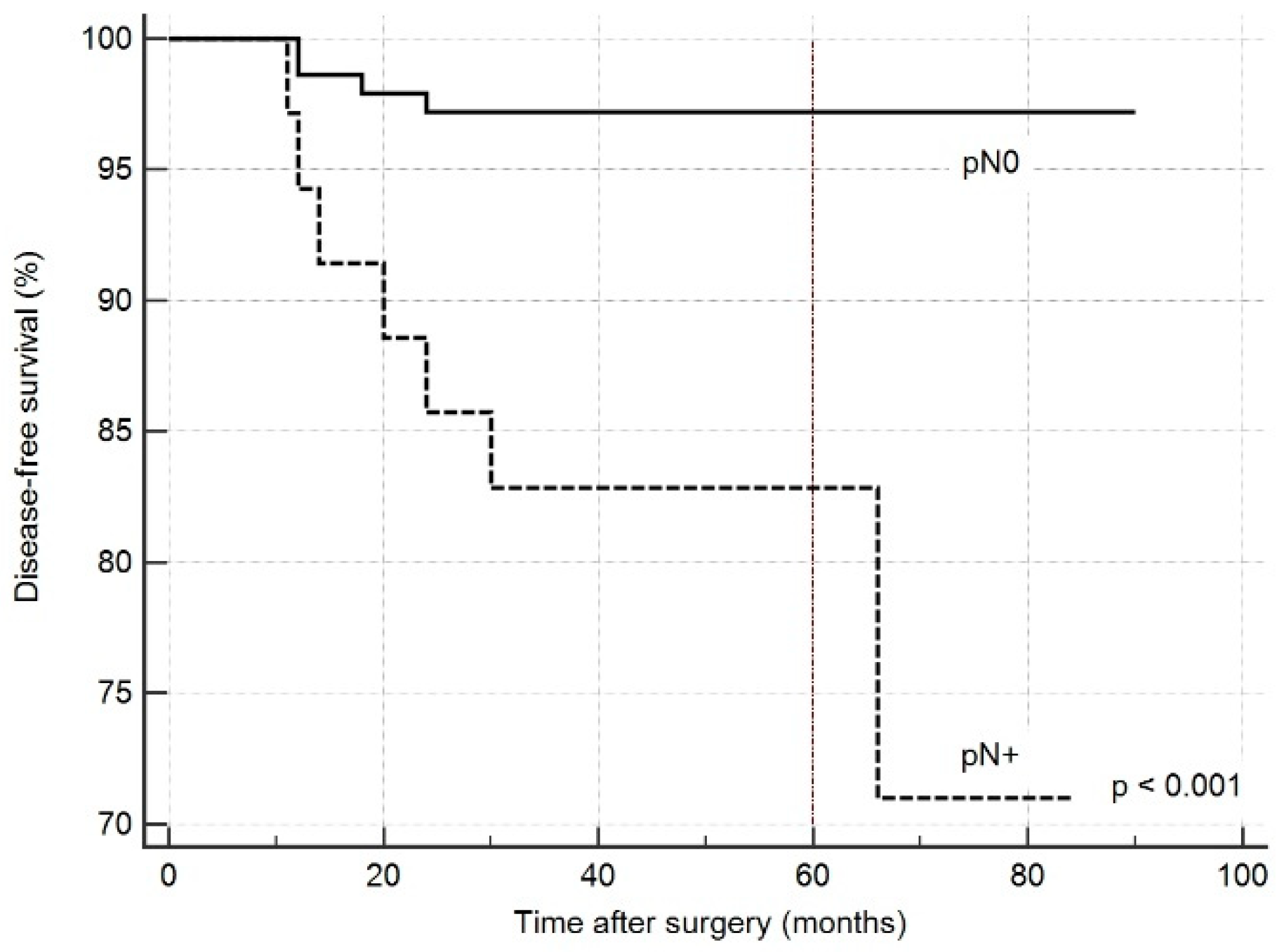
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barczyński, M.; Konturek, A.; Stopa, M.; Nowak, W. Prophylactic central neck dissection for papillary thyroid cancer. BJS 2013, 100, 410–418. [Google Scholar] [CrossRef] [PubMed]
- Calò, P.G.; Conzo, G.; Raffaelli, M.; Medas, F.; Gambardella, C.; De Crea, C.; Gordini, L.; Patrone, R.; Sessa, L.; Erdas, E.; et al. Total thyroidectomy alone versus ipsilateral versus bilateral prophylactic central neck dissection in clinically node-negative differentiated thyroid carcinoma. A retrospective multicenter study. Eur. J. Surg. Oncol. (EJSO) 2017, 43, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L.; Jhiang, S.M. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am. J. Med. 1994, 97, 418–428. [Google Scholar] [CrossRef]
- Otsuki, N.; Shimoda, H.; Morita, N.; Furukawa, T.; Teshima, M.; Shinomiya, H.; Nibu, K. Salvage surgery for structural local recurrence of papillary thyroid cancer: Recurrence patterns and surgical outcome. Endocr. J. 2020. [Google Scholar] [CrossRef]
- Kim, H.; Kim, T.H.; Choe, J.-H.; Kim, J.-H.; Kim, J.S.; Oh, Y.L.; Hahn, S.Y.; Shin, J.H.; Chi, S.A.; Jung, S.-H.; et al. Patterns of Initial Recurrence in Completely Resected Papillary Thyroid Carcinoma. Thyroid 2017, 27, 908–914. [Google Scholar] [CrossRef]
- Wang, L.Y.; Migliacci, J.C.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P.; Patel, S.G.; Ganly, I. Management and outcome of clinically evident neck recurrence in patients with papillary thyroid cancer. Clin. Endocrinol. 2017, 87, 566–571. [Google Scholar] [CrossRef]
- Medas, F.; Canu, G.L.; Boi, F.; Lai, M.L.; Erdas, E.; Calò, P.G. Predictive Factors of Recurrence in Patients with Differentiated Thyroid Carcinoma: A Retrospective Analysis on 579 Patients. Cancers (Basel) 2019, 11, 1230. [Google Scholar] [CrossRef] [Green Version]
- Enumah, S.; Fingeret, A.; Parangi, S.; Dias-Santagata, D.; Sadow, P.M.; Lubitz, C.C. BRAFV600E Mutation is Associated with an Increased Risk of Papillary Thyroid Cancer Recurrence. World J. Surg. 2020. [Google Scholar] [CrossRef]
- Alvarado, R.; Sywak, M.S.; Delbridge, L.; Sidhu, S.B. Central lymph node dissection as a secondary procedure for papillary thyroid cancer: Is there added morbidity? Surgery 2009, 145, 514–518. [Google Scholar] [CrossRef]
- Calò, P.G.; Medas, F.; Pisano, G.; Boi, F.; Baghino, G.; Mariotti, S.; Nicolosi, A. Differentiated Thyroid Cancer: Indications and Extent of Central Neck Dissection—Our Experience. Available online: https://www.hindawi.com/journals/ijso/2013/625193/abs/ (accessed on 31 January 2019).
- Moreno, M.A.; Edeiken-Monroe, B.S.; Siegel, E.R.; Sherman, S.I.; Clayman, G.L. In papillary thyroid cancer, preoperative central neck ultrasound detects only macroscopic surgical disease, but negative findings predict excellent long-term regional control and survival. Thyroid 2012, 22, 347–355. [Google Scholar] [CrossRef] [Green Version]
- Ito, Y.; Tomoda, C.; Uruno, T.; Takamura, Y.; Miya, A.; Kobayashi, K.; Matsuzuka, F.; Kuma, K.; Miyauchi, A. Clinical significance of metastasis to the central compartment from papillary microcarcinoma of the thyroid. World J. Surg. 2006, 30, 91–99. [Google Scholar] [CrossRef]
- Ito, Y.; Tomoda, C.; Uruno, T.; Takamura, Y.; Miya, A.; Kobayashi, K.; Matsuzuka, F.; Kuma, K.; Miyauchi, A. Ultrasonographically and anatomopathologically detectable node metastases in the lateral compartment as indicators of worse relapse-free survival in patients with papillary thyroid carcinoma. World J. Surg. 2005, 29, 917–920. [Google Scholar] [CrossRef] [PubMed]
- Mazzaferri, E.L. Long-term outcome of patients with differentiated thyroid carcinoma: Effect of therapy. Endocr. Pract. 2000, 6, 469–476. [Google Scholar] [CrossRef]
- Bhattacharyya, N. A population-based analysis of survival factors in differentiated and medullary thyroid carcinoma. Otolaryngol. Head Neck Surg. 2003, 128, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Steinmüller, T.; Klupp, J.; Rayes, N.; Ulrich, F.; Jonas, S.; Gräf, K.J.; Neuhaus, P. Prognostic factors in patients with differentiated thyroid carcinoma. Eur. J. Surg. 2000, 166, 29–33. [Google Scholar] [CrossRef]
- Kim, B.Y.; Choi, N.; Kim, S.W.; Jeong, H.-S.; Chung, M.K.; Son, Y.-I. Randomized trial of prophylactic ipsilateral central lymph node dissection in patients with clinically node negative papillary thyroid microcarcinoma. Eur. Arch. Otorhinolaryngol. 2020, 277, 569–576. [Google Scholar] [CrossRef] [PubMed]
- Shaha, A.R. Thyroid cancer: Extent of thyroidectomy. Cancer Control 2000, 7, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Beasley, N.J.P.; Lee, J.; Eski, S.; Walfish, P.; Witterick, I.; Freeman, J.L. Impact of nodal metastases on prognosis in patients with well-differentiated thyroid cancer. Arch. Otolaryngol. Head Neck Surg. 2002, 128, 825–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rotstein, L. The role of lymphadenectomy in the management of papillary carcinoma of the thyroid. J. Surg. Oncol. 2009, 99, 186–188. [Google Scholar] [CrossRef]
- Yazıcı, D.; Çolakoğlu, B.; Sağlam, B.; Sezer, H.; Kapran, Y.; Aydın, Ö.; Demirkol, M.O.; Alagöl, F.; Terzioğlu, T. Effect of prophylactic central neck dissection on the surgical outcomes in papillary thyroid cancer: Experience in a single center. Eur. Arch. Otorhinolaryngol. 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Li, Y.; Mao, Y. Local lymph node recurrence after central neck dissection in papillary thyroid cancers: A meta analysis. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2019, 136, 481–487. [Google Scholar] [CrossRef] [PubMed]
- Conzo, G.; Calò, P.G.; Sinisi, A.A.; De Bellis, A.; Pasquali, D.; Iorio, S.; Tartaglia, E.; Mauriello, C.; Gambardella, C.; Cavallo, F.; et al. Impact of prophylactic central compartment neck dissection on locoregional recurrence of differentiated thyroid cancer in clinically node-negative patients: A retrospective study of a large clinical series. Surgery 2014, 155, 998–1005. [Google Scholar] [CrossRef]
- Scherl, S.; Mehra, S.; Clain, J.; Dos Reis, L.L.; Persky, M.; Turk, A.; Wenig, B.; Husaini, H.; Urken, M.L. The effect of surgeon experience on the detection of metastatic lymph nodes in the central compartment and the pathologic features of clinically unapparent metastatic lymph nodes: What are we missing when we don’t perform a prophylactic dissection of central compartment lymph nodes in papillary thyroid cancer? Thyroid 2014, 24, 1282–1288. [Google Scholar] [CrossRef]
- Calò, P.; Pisano, G.; Medas, F.; Marcialis, J.; Gordini, L.; Erdas, E.; Nicolosi, A. Total thyroidectomy without prophylactic central neck dissection in clinically node-negative papillary thyroid cancer: Is it an adequate treatment? World J. Surg. Oncol. 2014, 12, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haddad, R.I.; Kandeel, F.; Scheri, R.P. NCCN Guidelines Index Table of Contents Discussion. J. Natl. Compr. Cancer Netw. 2018, 16, 1429–1440. [Google Scholar] [CrossRef] [Green Version]
- Takami, H.; Ito, Y.; Okamoto, T.; Onoda, N.; Noguchi, H.; Yoshida, A. Revisiting the Guidelines Issued by the Japanese Society of Thyroid Surgeons and Japan Association of Endocrine Surgeons: A Gradual Move Towards Consensus Between Japanese and Western Practice in the Management of Thyroid Carcinoma. World J. Surg. 2014, 38, 2002–2010. [Google Scholar] [CrossRef]
- Ganly, I.; Ibrahimpasic, T.; Rivera, M.; Nixon, I.; Palmer, F.; Patel, S.G.; Tuttle, R.M.; Shah, J.P.; Ghossein, R. Prognostic implications of papillary thyroid carcinoma with tall-cell features. Thyroid 2014, 24, 662–670. [Google Scholar] [CrossRef]
- Bernstein, J.; Virk, R.K.; Hui, P.; Prasad, A.; Westra, W.H.; Tallini, G.; Adeniran, A.J.; Udelsman, R.; Sasaki, C.T.; Roman, S.A.; et al. Tall cell variant of papillary thyroid microcarcinoma: Clinicopathologic features with BRAF(V600E) mutational analysis. Thyroid 2013, 23, 1525–1531. [Google Scholar] [CrossRef]
- Axelsson, T.A.; Hrafnkelsson, J.; Olafsdottir, E.J.; Jonasson, J.G. Tall cell variant of papillary thyroid carcinoma: A population-based study in Iceland. Thyroid 2015, 25, 216–220. [Google Scholar] [CrossRef]
- Raffaelli, M.; De Crea, C.; Sessa, L.; Giustacchini, P.; Revelli, L.; Bellantone, C.; Lombardi, C.P. Prospective evaluation of total thyroidectomy versus ipsilateral versus bilateral central neck dissection in patients with clinically node–negative papillary thyroid carcinoma. Surgery 2012, 152, 957–964. [Google Scholar] [CrossRef] [PubMed]
- Sadowski, B.M.; Snyder, S.K.; Lairmore, T.C. Routine bilateral central lymph node clearance for papillary thyroid cancer. Surgery 2009, 146, 696–705. [Google Scholar] [CrossRef] [PubMed]
- Zhao, W.; Luo, H.; Zhou, Y.; Dai, W.; Zhu, J. Evaluating the effectiveness of prophylactic central neck dissection with total thyroidectomy for cN0 papillary thyroid carcinoma: An updated meta-analysis. Eur. J. Surg. Oncol. 2017, 43, 1989–2000. [Google Scholar] [CrossRef] [PubMed]
- Ahn, S.-H.; Kim, W.S. The effect of prophylactic central neck dissection during hemithyroidectomy on locoregional recurrence in patients with papillary thyroid carcinoma: A meta-analysis. Clin. Exp. Otorhinolaryngol. 2020, 13, 194. [Google Scholar] [CrossRef]
- Zhao, H.; Li, H. Meta-analysis of ultrasound for cervical lymph nodes in papillary thyroid cancer: Diagnosis of central and lateral compartment nodal metastases. Eur. J. Radiol. 2019, 112, 14–21. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Patients (n = 399) | TT Group (n = 320) | pCLND Group (n = 79) | p | |
|---|---|---|---|---|
| Sex | 0.1493 | |||
| Male | 101 (25.3%) | 86 (26.9%) | 15 (19.0%) | |
| Female | 298 (74.7%) | 234 (73.1%) | 64 (81.0%) | |
| Age, years | 50.5 ± 14.4 (15–83) | 52.4 + 14.0 | 42.6 ± 13.5 | p < 0.001 |
| Hyperthyroidism | 28 (7%) | 25 (7.8%) | 3 (3.8%) | 0.314 |
| Autoimmune thyroiditis | 146 (36.6%) | 97 (30.3%) | 49 (62.0%) | p < 0.001 |
| US findings | ||||
| Multinodular disease | 250 (62.7%) | 204 (63.8%) | 46 (58.2%) | 0.436 |
| Peri- and intra-vascularization of the nodule | 243 (60.9%) | 195 (60.9%) | 48 (60.8%) | 0.920 |
| Hypoechoic nodule | 70 (17.6%) | 48 (15%) | 22 (27.8%) | 0.011 |
| Microcalcification | 34 (8.5%) | 29 (9.1%) | 5 (6.3%) | 0.579 |
| FNAC | <0.001 | |||
| Tir1-2 | 73 (18.3%) | 66 (20.6%) | 7 (8.9%) | |
| Tir3 | 148 (37.1%) | 131 (40.9%) | 17 (21.5%) | |
| Tir4-5 | 178 (44.6%) | 123 (38.4%) | 55 (69.6%) | |
| Operative time, minutes | 94.4 ± 22.2 | 92.5 ± 22.6 | 102.3 ± 18.9 | p < 0.001 |
| Postoperative stay, days | 2.8 ± 1.1 | 2.8 ± 1.0 | 3.0 ± 1.3 | 0.068 |
| Transient hypoparathyroidism | 136 (34.1%) | 102 (31.9%) | 34 (43.0%) | 0.081 |
| Permanent hypoparathyroidism | 39 (9.8%) | 27 (8.4%) | 12 (15.2%) | 0.109 |
| Transient RLN injury | 10 (2.5%) | 7 (2.2%) | 3 (3.8%) | 0.675 |
| Permanent RLN injury | 3 (0.8%) | 2 (0.6%) | 1 (1.3%) | 0.891 |
| Postoperative bleeding | 5 (1.3%) | 4 (1.3%) | 1 (1.3%) | 0.580 |
| RAI therapy | 331 (82.9%) | 258 (80.6%) | 73 (92.4%) | 0.019 |
| Follow-up, months | 55.4 ± 15.9 | 56.1 ± 16.1 | 52.6 ± 15.2 | 0.087 |
| Recurrent disease | 22 (5.5%) | 18 (5.6%) | 4 (5.1%) | 0.936 |
| Patients (n = 399) | TT Group (n = 320) | pCLND Group (n = 79) | p | |
|---|---|---|---|---|
| Nodule size (mm) | 16.8 ± 10.9 | 16.9 ± 11.1 | 16.3 ± 9.8 | 0.681 |
| Thyroid weight (gr) | 26.7 ± 22.5 | 27.4 ± 24.2 | 24.1 ± 13.3 | 0.252 |
| Histotype | <0.0001 | |||
| PTC | 151 | 115 (35.9%) | 36 (45.6%) | |
| FV-PTC | 133 | 120 (37.5%) | 13 (16.5%) | |
| TCV-PTC | 40 | 20 (6.3%) | 20 (25.3%) | |
| FTC | 53 | 47 (14.7%) | 6 (7.6%) | |
| HCC | 21 | 18 (5.6%) | 3 (3.8%) | |
| Low differentiated carcinoma | 1 | 0 | 1 (1.3%) | |
| Microcarcinoma | 109 (27.3%) | 87 (27.2%) | 22 (27.8%) | 0.981 |
| Multicentricity | 151 (37.8%) | 117 (36.6%) | 34 (43%) | 0.350 |
| Angioinvasivity | 15 (3.8%) | 13 (4.1%) | 2 (2.5%) | 0.756 |
| Extrathyroidal extension | 27 (6.8%) | 23 (7.2%) | 4 (5.1%) | 0.672 |
| LN yield | 5.1 ± 5.3 | 2.1 ± 1.1 | 8.9 ± 6.0 | p < 0.001 |
| LN metastasis | 35 (8.8%) | 15 (4.7%) | 20 (25.3%) | p < 0.001 |
| Number of positive LN | 0.5 ± 1.3 | 0.2 ± 0.7 | 0.8 ± 1.7 | 0.006 |
| LN ratio | 0.5 ± 0.3 | 0.6 ± 0.2 | 0.3 ± 0.3 | 0.004 |
| ATA risk class of disease recurrence | p < 0.001 | |||
| Low | 310 (77.7%) | 268 (83.8%) | 42 (53.2%) | |
| Medium | 64 (16%) | 30 (9.4%) | 34 (43.0%) | |
| High | 25 (6.3%) | 22 (6.9%) | 3 (3.8%) |
| ATA Risk | Low | Medium–High | ||||
|---|---|---|---|---|---|---|
| TT | pCLND | Total | TT | pCLND | Total | |
| Patients | 268 | 42 | 310 | 52 | 37 | 89 |
| Recurrent disease | 7 (2.6%) | 2 (4.8%) | 9 (2.9%) | 11 (21.2%) | 2 (5.4%) | 13 (14.6%) |
| p (TT vs. CLND) | 0.441 | 0.0392 | ||||
| pNx | pN0 | pN+ | |
|---|---|---|---|
| Patients | 221 | 143 | 35 |
| Disease recurrence | 11 (5%) | 4 (2.8%) | 7 (20%) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Medas, F.; Canu, G.L.; Cappellacci, F.; Anedda, G.; Conzo, G.; Erdas, E.; Calò, P.G. Prophylactic Central Lymph Node Dissection Improves Disease-Free Survival in Patients with Intermediate and High Risk Differentiated Thyroid Carcinoma: A Retrospective Analysis on 399 Patients. Cancers 2020, 12, 1658. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061658
Medas F, Canu GL, Cappellacci F, Anedda G, Conzo G, Erdas E, Calò PG. Prophylactic Central Lymph Node Dissection Improves Disease-Free Survival in Patients with Intermediate and High Risk Differentiated Thyroid Carcinoma: A Retrospective Analysis on 399 Patients. Cancers. 2020; 12(6):1658. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061658
Chicago/Turabian StyleMedas, Fabio, Gian Luigi Canu, Federico Cappellacci, Giacomo Anedda, Giovanni Conzo, Enrico Erdas, and Pietro Giorgio Calò. 2020. "Prophylactic Central Lymph Node Dissection Improves Disease-Free Survival in Patients with Intermediate and High Risk Differentiated Thyroid Carcinoma: A Retrospective Analysis on 399 Patients" Cancers 12, no. 6: 1658. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12061658