The Impact on Survival and Morbidity of Portal–Mesenteric Resection During Pancreaticoduodenectomy for Pancreatic Head Adenocarcinoma: A Systematic Review and Meta-Analysis of Comparative Studies

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Selection and Data Extraction
2.2. Inclusion Criteria and Assessment of Study Quality
2.3. Exclusion Criteria
2.4. Outcomes of Interest and Definitions
- Patients baseline characteristics: age, gender, American Society of Anesthesiologists Classification (ASA Class), number of patients receiving neoadjuvant chemotherapy, number of patients undergoing preoperative biliary drainage for obstructive jaundice.
- Tumor characteristics: stage according to AJCC, T stage according to the TNM, tumor size, grade of differentiation (well, moderate, and poor), and presence of lymphovascular invasion (LVI).
- Operation-related outcomes: type of vein resection/reconstruction performed, operative time, blood loss, rates of transfusion, status of resection margins (positive versus negative), rates of R0 and R1 resections, number of patients having venous infiltration at final histologic examination. Definition of resection margins varied among the included studies. Additionally, the definition of postoperative morbidity varied, although the main part of the complications were defined according to the International Study Group of Pancreatic Surgery [19,20,21].
- Duration of postoperative hospital stay.
- 30-day mortality, overall and specific postoperative morbidity: pancreatic fistula, bile leak, delayed gastric emptying (DGE), hemorrhage, rates of blood transfusions, rates of reoperations, number of patients receiving adjuvant chemotherapy.
- Duration of follow-up and survival outcomes including 1-, 3-, and 5- year overall survival (OS) in both the PD+VR and PD groups. Survival was defined as the number of months between the date of surgery and death.
2.5. Statistical Analysis
3. Results
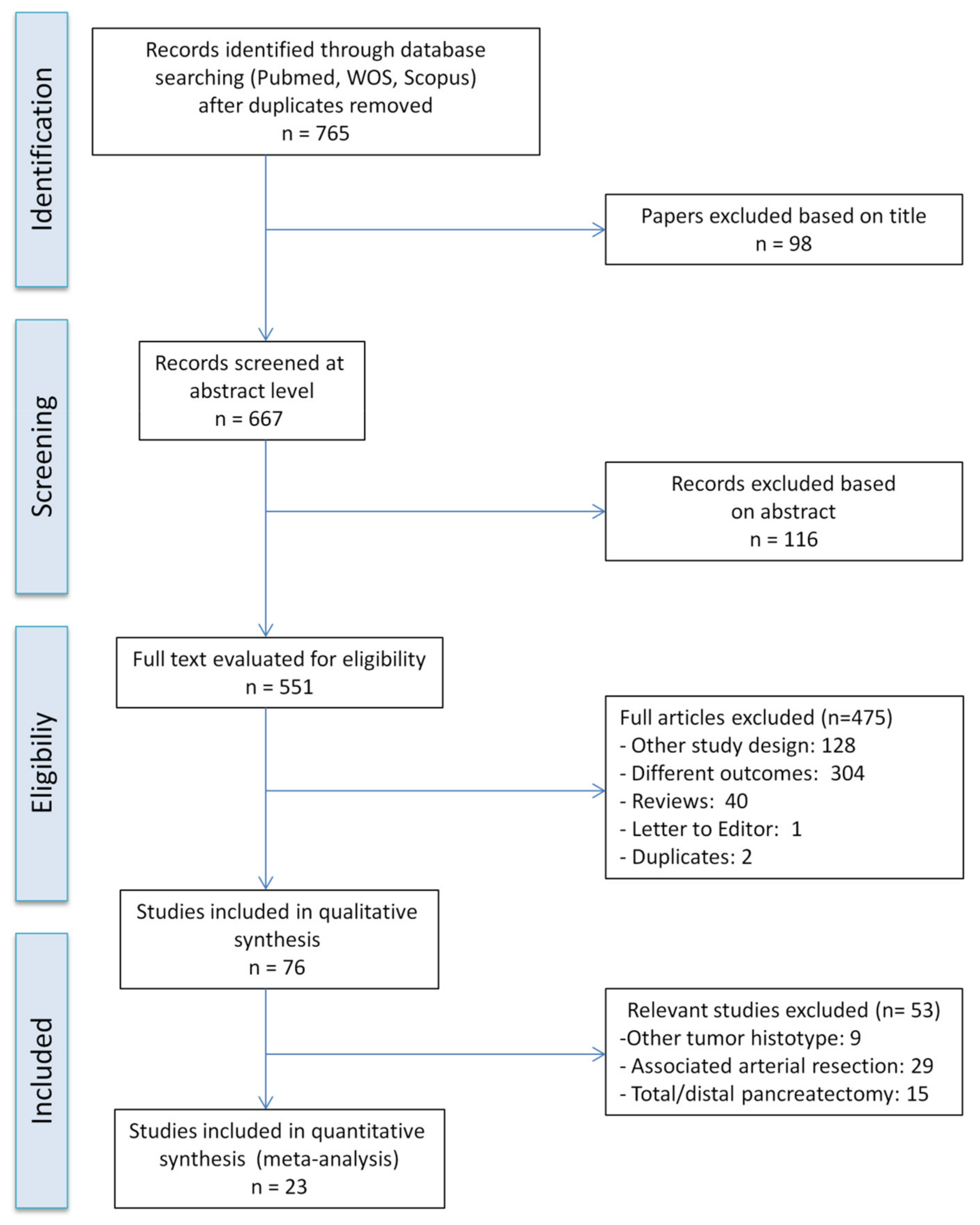
3.1. Included Studies
3.2. Patient and Tumor Characteristics
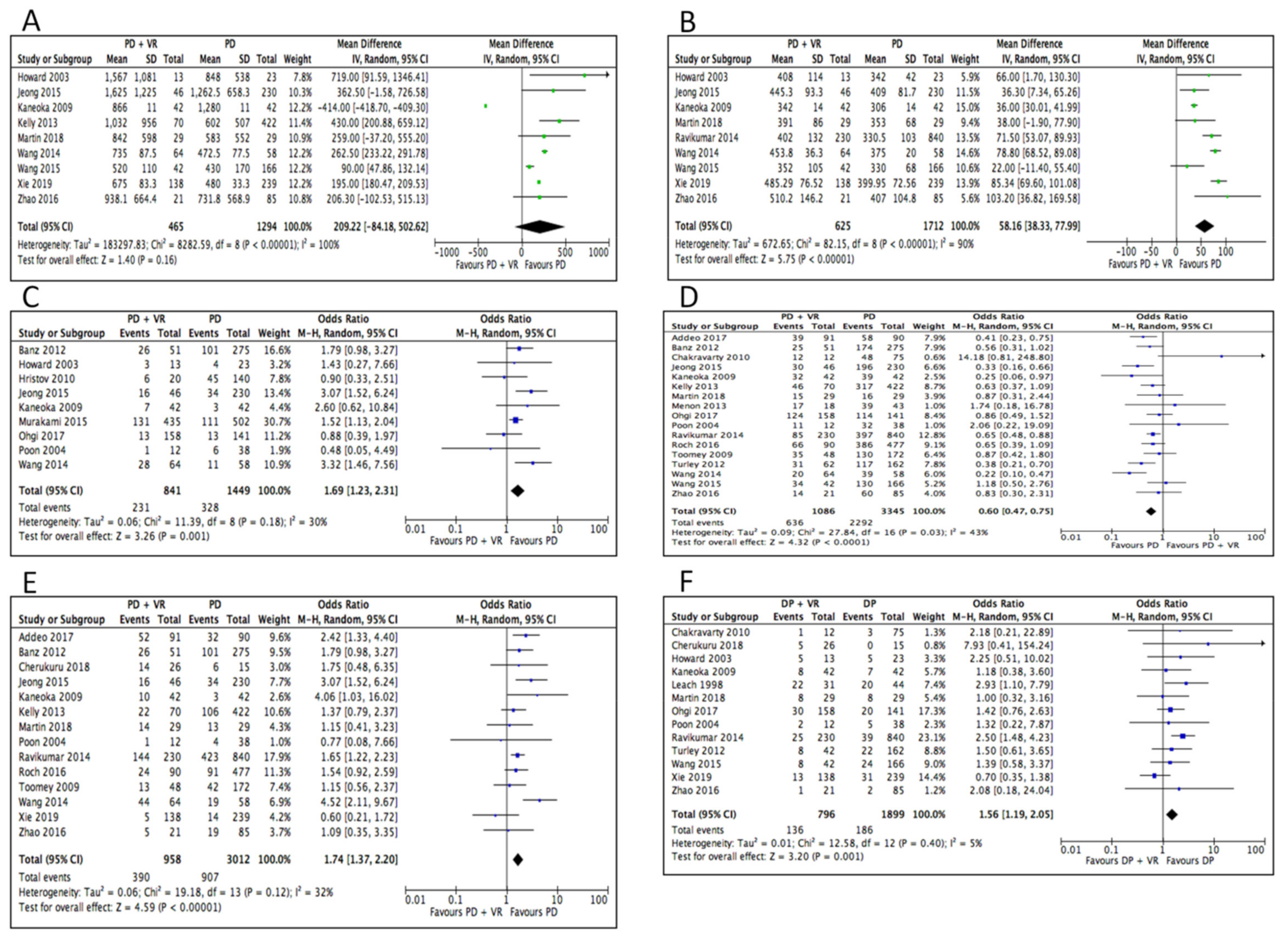
3.3. Operative Outcomes
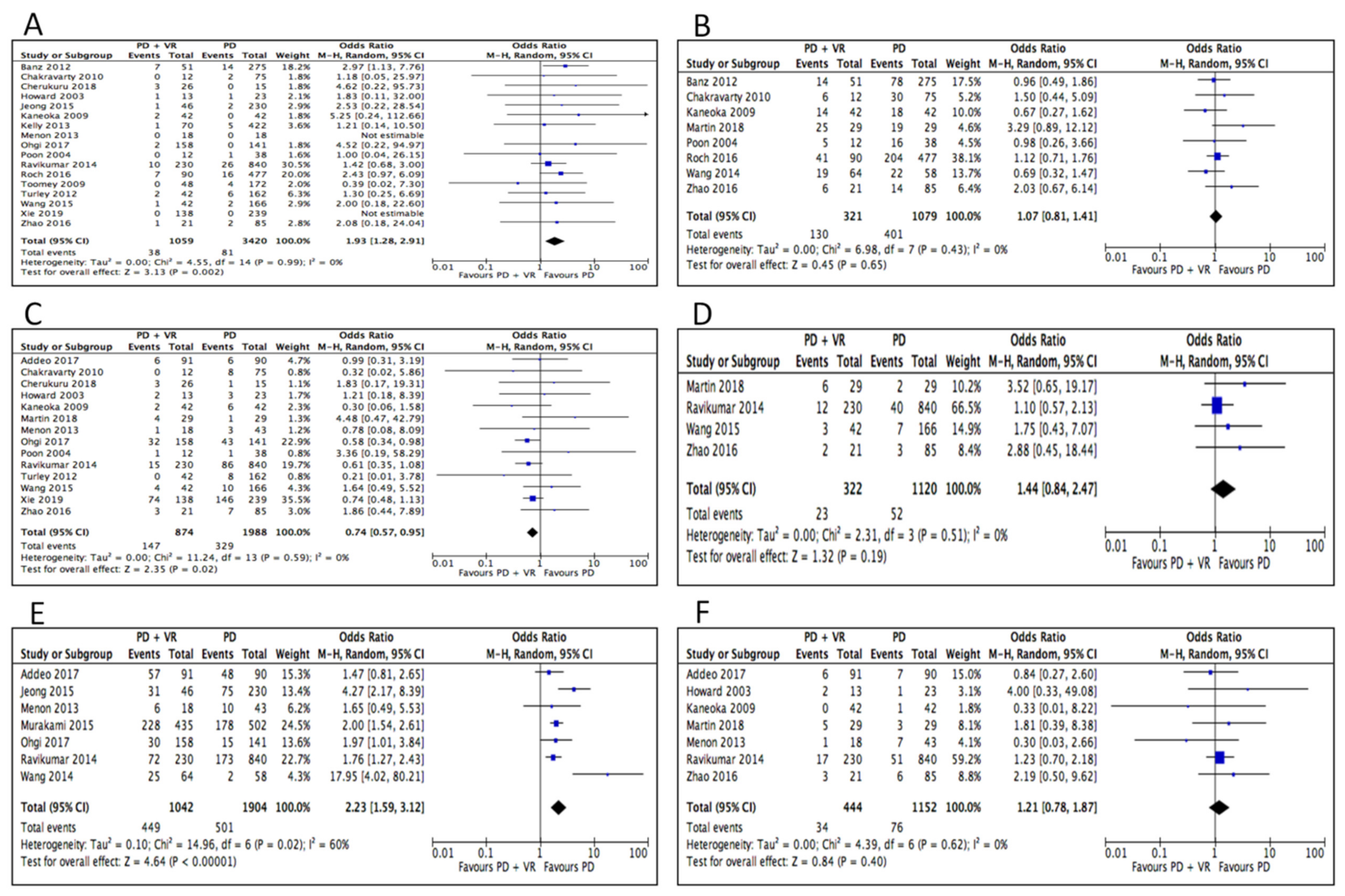
3.4. Postoperative Outcomes
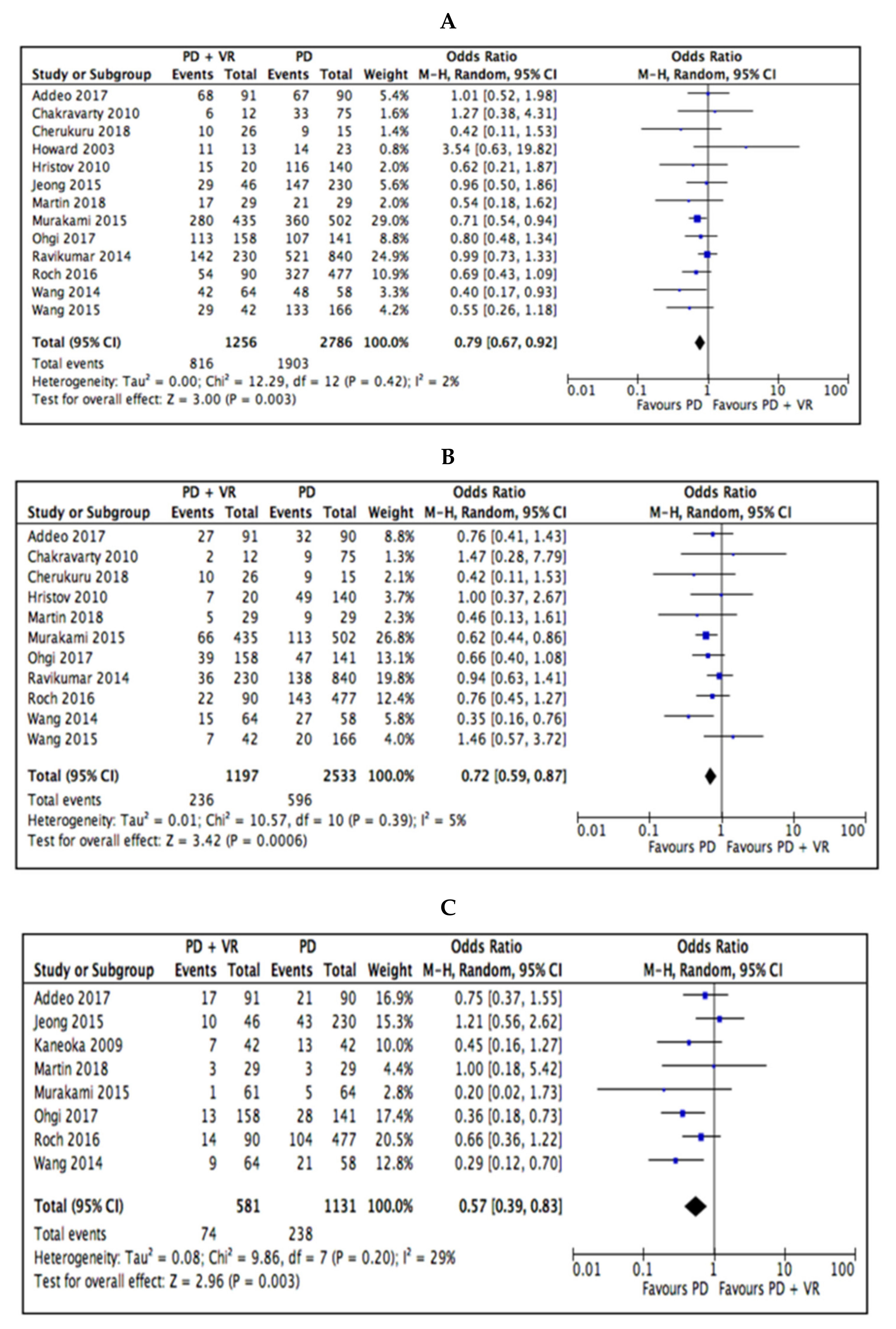
3.5. Survival Outcomes
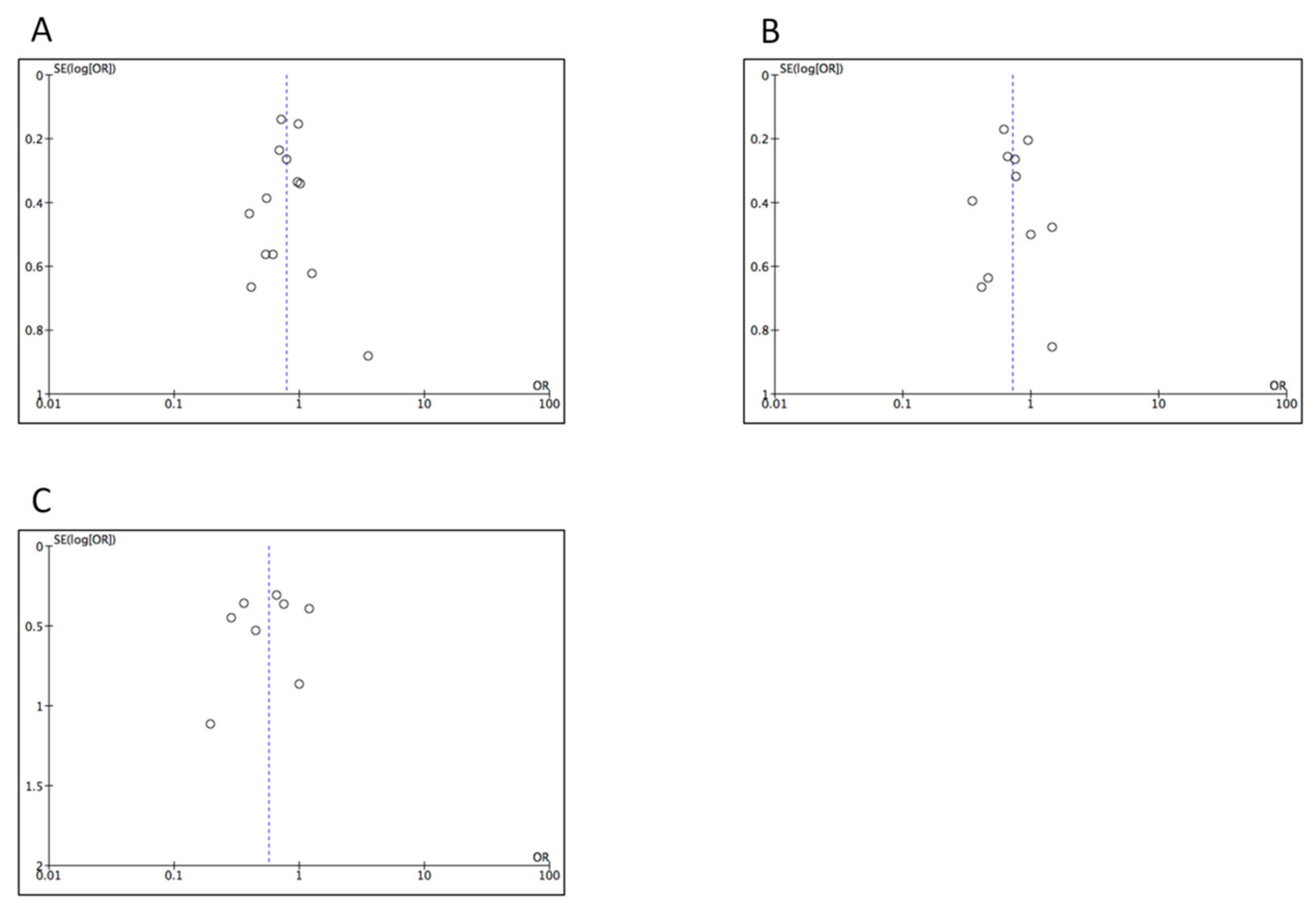
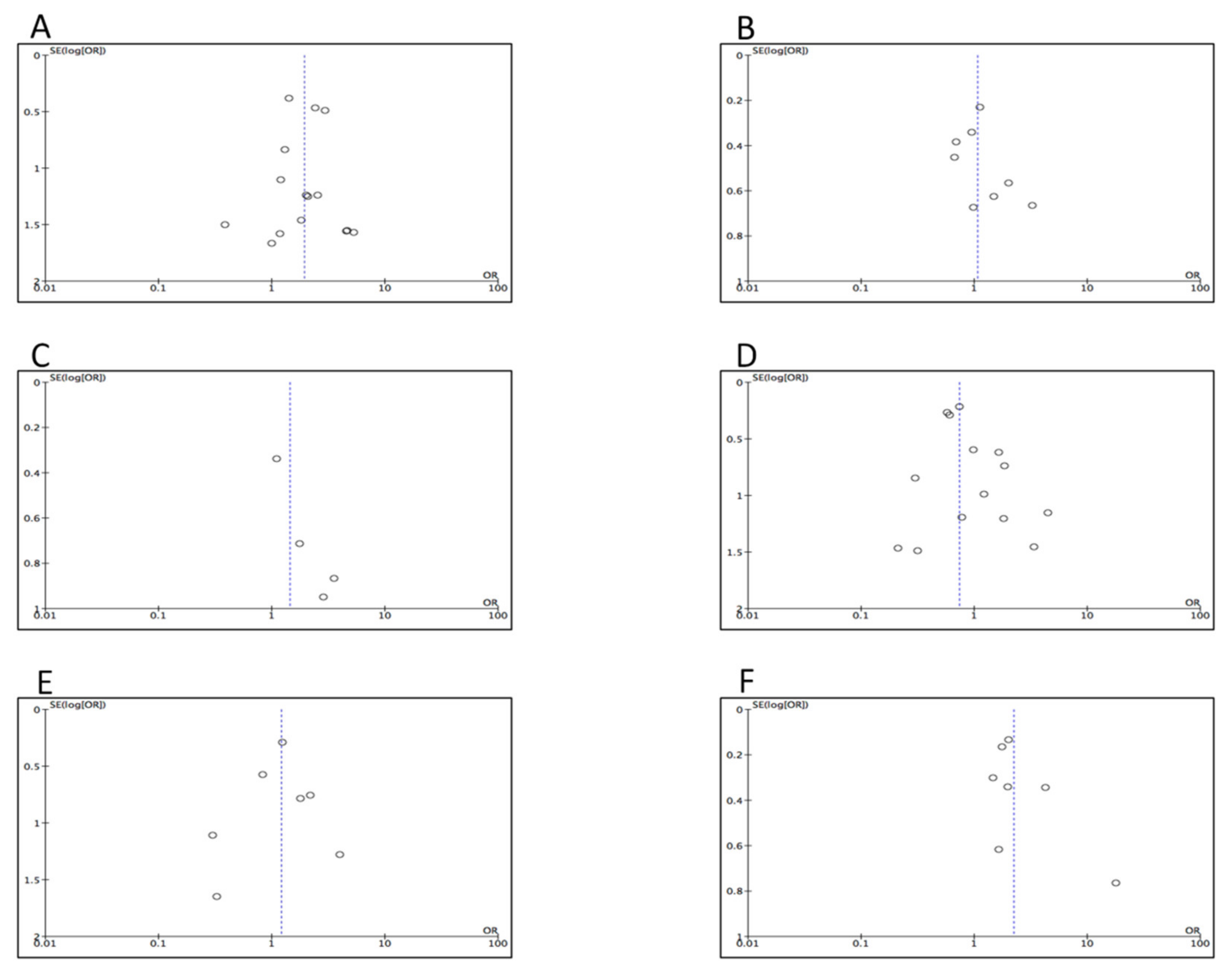
3.6. Assessment for Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawla, P.; Sunkara, T.; Gaduputi, V. Epidemiology of Pancreatic Cancer: Global Trends, Etiology and Risk Factors. World J. Oncol. 2019, 10, 10–27. [Google Scholar] [CrossRef]
- Pusceddu, C.; Melis, L.; Sotgia, B.; Fancellu, A.; Meloni, G.B. Computed Tomography-Guided Cryoablation of Local Recurrence after Primary Resection of Pancreatic Adenocarcinoma. Clin. Pract. 2015, 5, 741. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perysinakis, I.; Avlonitis, S.; Georgiadou, D.; Tsipras, H.; Margaris, I. Five-year actual survival after pancreatoduodenectomy for pancreatic head cancer. ANZ J. Surg. 2015, 85, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Yu, X.Z.; Li, J.; Fu, D.L.; Di, Y.; Yang, F.; Hao, S.J.; Jin, C. Benefit from synchronous portal-superior mesenteric vein resection during pancreaticoduodenectomy for cancer: A meta-analysis. Eur. J. Surg. Oncol. 2014, 40, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Giovinazzo, F.; Turri, G.; Katz, M.H.; Heaton, N.; Ahmed, I. Meta-analysis of benefits of portal-superior mesenteric vein resection in pancreatic resection for ducal adenocarcinoma. Br. J. Surg. 2016, 103, 179–191. [Google Scholar] [CrossRef] [PubMed]
- Bell, R.; Ao, B.T.; Ironside, N.; Bartlett, A.; Windsor, J.A.; Pandanaboyana, S. Meta-analysis and cost effective analysis of portal-superior mesenteric vein resection during pancreatoduodenectomy: Impact on margin status and survival. Surg. Oncol. 2017, 26, 53–62. [Google Scholar] [CrossRef]
- Wang, W.L.; Ye, S.; Yan, S.; Shen, Y.; Zhang, M.; Wu, J.; Zheng, S.S. Pancreaticoduodenectomy with portal vein/superior mesenteric vein resection for patients with pancreatic cancer with venous invasion. Hepatobiliary Pancreat. Dis. Int. 2015, 14, 429–435. [Google Scholar] [CrossRef]
- NCCN Guidelines Version 1.2020 Pancreatic Adenocarcinoma. Available online: https://www.nccn.org/store/login/login.aspx?Returnurl=https://www.nccn.org/professionals/physician_gls/pdf/pancreatic.pdf (accessed on 15 April 2020).
- Nigri, G.; Petrucciani, N.; Pinna, A.D.; Ravaioli, M.; Jovine, E.; Minni, F.; Grazi, G.L.; Chirletti, P.; Balzano, G.; Ferla, F.; et al. Evolution of pancreatectomy with en bloc venous resection for pancreatic cancer in Italy. Retrospective cohort study on 425 cases in 10 pancreatic referral units. Int. J. Surg. 2018, 55, 103–109. [Google Scholar] [CrossRef]
- Ramacciato, G.; Nigri, G.; Petrucciani, N.; Pinna, A.D.; Ravaioli, M.; Jovine, E.; Minni, F.; Grazi, G.L.; Chirletti, P.; Tisone, G.; et al. Pancreatectomy with Mesenteric and Portal Vein Resection for Borderline Resectable Pancreatic Cancer: Multicenter Study of 406 Patients. Ann. Surg. Oncol. 2016, 23, 2028–2037. [Google Scholar] [CrossRef]
- Addeo, P.; Velten, M.; Averous, G.; Faitot, F.; Nguimpi-Tambou, M.; Nappo, G.; Felli, E.; Fuchshuber, P.; Bachellier, P. Prognostic value of venous invasion in resected T3 pancreatic adenocarcinoma: Depth of invasion matters. Surgery 2017, 162, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Gilbert, J.W.; Wolpin, B.; Clancy, T.; Wang, J.; Mamon, H.; Shinagare, A.B.; Jagannathan, J.; Rosenthal, M. Borderline resectable pancreatic cancer: Conceptual evolution and current approach to image-based classification. Ann. Oncol. 2017, 28, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Gong, Y.; Zhang, L.; He, T.; Ding, J.; Zhang, H.; Chen, G.; Zhang, D.; Wu, Z.; Chen, Q.; Fan, H.; et al. Pancreaticoduodenectomy combined with vascular resection and reconstruction for patients with locally advanced pancreatic cancer: A multicenter; retrospective analysis. PLoS ONE 2013, 8, e70340. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lapshyn, H.; Bronsert, P.; Bolm, L.; Werner, M.; Hopt, U.T.; Makowiec, F.; Wittel, U.A.; Keck, T.; Wellner, U.F.; Bausch, D. Prognostic factors after pancreatoduodenectomy with en bloc portal venous resection for pancreatic cancer. Langenbecks Arch. Surg. 2016, 401, 63–69. [Google Scholar] [CrossRef]
- Flis, V.; Potrc, S.; Kobilica, N.; Ivanecz, A. Pancreaticoduodenectomy for ducal adenocarcinoma of the pancreatic head with venous resection. Radiol. Oncol. 2016, 50, 321–328. [Google Scholar] [CrossRef] [Green Version]
- Peng, C.; Zhou, D.; Meng, L.; Cao, Y.; Zhang, H.; Pan, Z.; Lin, C. The value of combined vein resection in pancreaticoduodenectomy for pancreatic head carcinoma: A meta-analysis. BMC Surg. 2019, 19, 84. [Google Scholar] [CrossRef] [Green Version]
- Wells, G.A.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 28 February 2020).
- Besselink, M.G.; van Rijssen, L.B.; Bassi, C.; Dervenis, C.; Montorsi, M.; Adham, M.; Asbun, H.J.; Bockhorn, M.; Strobel, O.; Büchler, M.W.; et al. Definition and classification of chyle leak after pancreatic operation: A consensus statement by the International Study Group on pancreatic surgery. Surgery 2017, 161, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.P.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 years after. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. BMJ 2009, 339, b2535. [Google Scholar] [CrossRef] [Green Version]
- Banz, V.M.; Croagh, D.; Coldham, C.; Tanière, P.; Buckels, J.; Isaac, J.; Mayer, D.; Muiesan, P.; Bramhall, S.; Mirza, D.F. Factors influencing outcome in patients undergoing portal vein resection for adenocarcinoma of the pancreas. Eur. J. Surg. Oncol. 2012, 38, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Chakravarty, K.D.; Hsu, J.T.; Liu, K.H.; Yeh, C.N.; Yeh, T.S.; Hwang, T.L.; Jan, Y.Y.; Chen, M.F. Prognosis and feasibility of en-bloc vascular resection in stage II pancreatic adenocarcinoma. World J. Gastroenterol. 2010, 16, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Cherukuru, R.; Govil, S.; Vij, M.; Rela, M. Vein resection in patients with adenocarcinoma of the head of pancreas adherent to the portomesenteric venous axis is beneficial despite a high rate of R1 resection. Ann. Hepatobiliary Pancreat. Surg. 2018, 22, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaneoka, Y.; Yamaguchi, A.; Isogai, M. Portal or superior mesenteric vein resection for pancreatic head adenocarcinoma: Prognostic value of the length of venous resection. Surgery 2009, 145, 417–425. [Google Scholar] [CrossRef]
- Kelly, K.J.; Winslow, E.; Kooby, D.; Lad, N.L.; Parikh, A.A.; Scoggins, C.R.; Ahmad, S.; Martin, R.C.; Maithel, S.K.; Kim, H.J.; et al. Vein involvement during pancreaticoduodenectomy: Is there a need for redefinition of "borderline resectable disease"? J. Gastrointest. Surg. 2013, 17, 1209–1217. [Google Scholar] [CrossRef]
- Hristov, B.; Reddy, S.; Lin, S.H.; Cameron, J.L.; Pawlik, T.M.; Hruban, R.H.; Swartz, M.J.; Edil, B.H.; Kemp, C.; Wolfgang, C.L.; et al. Outcomes of adjuvant chemoradiation after pancreaticoduodenectomy with mesenterico-portal vein resection for adenocarcinoma of the pancreas. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, 176–180. [Google Scholar] [CrossRef]
- Howard, T.J.; Villanustre, N.; Moore, S.A.; DeWitt, J.; LeBlanc, J.; Maglinte, D.; McHenry, L. Efficacy of venous reconstruction in patients with adenocarcinoma of the pancreatic head. J. Gastrointest. Surg. 2003, 7, 1089–1095. [Google Scholar] [CrossRef]
- Jeong, J.; Choi, D.W.; Choi, S.H.; Heo, J.S.; Jang, K.T. Long-term outcome of portomesenteric vein invasion and prognostic factors in pancreas head adenocarcinoma. ANZ J. Surg. 2015, 85, 264–269. [Google Scholar] [CrossRef]
- Leach, S.D.; Lee, J.E.; Charnsangavej, C.; Cleary, K.R.; Lowy, A.M.; Fenoglio, C.J.; Pisters, P.W.; Evans, D.B. Survival following pancreaticoduodenectomy with resection of the superior mesenteric-portal vein confluence for adenocarcinoma of the pancreatic head. Br. J. Surg. 1998, 85, 611–617. [Google Scholar] [CrossRef]
- Martin, D.; Petermann, D.; Fontanella, S.; Pu, Y.; Halkic, N.; Demartines, N.; Schäfer, M. Pancreatic adenocarcinoma with histologically proven portal vein infiltration: What is the outcome? Eur. J. Gastroenterol. Hepatol. 2018, 30, 1507–1513. [Google Scholar] [CrossRef]
- Menon, V.G.; Puri, V.C.; Annamalai, A.A.; Tuli, R.; Nissen, N.N. Outcomes of vascular resection in pancreaticoduodenectomy: Single-surgeon experience. Am. Surg. 2013, 79, 1064–1067. [Google Scholar] [CrossRef] [PubMed]
- Murakami, Y.; Satoi, S.; Motoi, F.; Sho, M.; Kawai, M.; Matsumoto, I.; Honda, G.; Multicentre Study Group of Pancreatobiliary Surgery (MSG-PBS). Portal or superior mesenteric vein resection in pancreatoduodenectomy for pancreatic head carcinoma. Br. J. Surg. 2015, 102, 837–846. [Google Scholar] [CrossRef] [PubMed]
- Ohgi, K.; Yamamoto, Y.; Sugiura, T.; Okamura, Y.; Ito, T.; Ashida, R.; Aramaki, T.; Uesaka, K. Is Pancreatic Head Cancer with Portal Venous Involvement Really Borderline Resectable? Appraisal of an Upfront Surgery Series. Ann. Surg. Oncol. 2017, 24, 2752–2761. [Google Scholar] [CrossRef] [PubMed]
- Poon, R.T.; Fan, S.T.; Lo, C.M.; Liu, C.L.; Lam, C.M.; Yuen, W.K.; Yeung, C.; Wong, J. Pancreaticoduodenectomy with en bloc portal vein resection for pancreatic carcinoma with suspected portal vein involvement. World J. Surg. 2004, 28, 602–608. [Google Scholar] [CrossRef]
- Ravikumar, R.; Sabin, C.; Abu Hilal, M.; Bramhall, S.; White, S.; Wigmore, S.; Imber, C.J.; Fusai, G.; UK Vascular Resection in Pancreatic Cancer Study Group. Portal vein resection in borderline resectable pancreatic cancer: A United Kingdom multicenter study. J. Am. Coll. Surg. 2014, 218, 401–411. [Google Scholar]
- Roch, A.M.; House, M.G.; Cioffi, J.; Ceppa, E.P.; Zyromski, N.J.; Nakeeb, A.; Schmidt, C.M. Significance of Portal Vein Invasion and Extent of Invasion in Patients Undergoing Pancreatoduodenectomy for Pancreatic Adenocarcinoma. J. Gastrointest. Surg. 2016, 20, 479–487. [Google Scholar] [CrossRef]
- Toomey, P.; Hernandez, J.; Morton, C.; Duce, L.; Farrior, T.; Villadolid, D.; Ross, S.; Rosemurgy, A. Resection of portovenous structures to obtain microscopically negative margins during pancreaticoduodenectomy for pancreatic adenocarcinoma is worthwhile. Am. Surg. 2009, 75, 804–809. [Google Scholar]
- Turley, R.S.; Peterson, K.; Barbas, A.S.; Ceppa, E.P.; Paulson, E.K.; Blazer, D.G., 3rd; Clary, B.M.; Pappas, T.N.; Tyler, D.S.; McCann, R.L.; et al. Vascular surgery collaboration during pancreaticoduodenectomy with vascular reconstruction. Ann. Vasc. Surg. 2012, 26, 685–692. [Google Scholar] [CrossRef]
- Wang, F.; Gill, A.J.; Neale, M.; Puttaswamy, V.; Gananadha, S.; Pavlakis, N.; Clarke, S.; Hugh, T.J.; Samra, J.S. Adverse tumor biology associated with mesenterico-portal vein resection influences survival in patients with pancreatic ductal adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 1937–1947. [Google Scholar] [CrossRef]
- Xie, Z.B.; Li, J.; Gu, J.C.; Jin, C.; Zou, C.F.; Fu, D.L. Pancreatoduodenectomy with portal vein resection favors the survival time of patients with pancreatic ductal adenocarcinoma: A propensity score matching analysis. Oncol. Lett. 2019, 18, 4563–4572. [Google Scholar] [CrossRef] [Green Version]
- Zhao, X.; Li, L.X.; Fan, H.; Kou, J.T.; Li, X.L.; Lang, R.; He, Q. Segmental portal/superior mesenteric vein resection and reconstruction with the iliac vein after pancreatoduodenectomy. J. Int. Med. Res. 2016, 44, 1339–1348. [Google Scholar] [CrossRef] [PubMed]
- Zettervall, S.L.; Ju, T.; Holzmacher, J.L.; Huysman, B.; Werba, G.; Sidawy, A.; Lin, P.; Vaziri, K. Arterial, but Not Venous; Reconstruction Increases 30-Day Morbidity and Mortality in Pancreaticoduodenectomy. J. Gastrointest. Surg. 2020, 24, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Kasumova, G.G.; Conway, W.C.; Tseng, J.F. The Role of Venous and Arterial Resection in Pancreatic Cancer Surgery. Ann. Surg. Oncol. 2018, 25, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Siriwardana, H.P.P.; Siriwardena, A.K. Systematic review of outcome of synchronous portal-superior mesenteric vein resection during pancreatectomy for cancer. Br. J. Surg. 2006, 93, 662–673. [Google Scholar] [CrossRef]
- Delpero, J.R.; Boher, J.M.; Sauvanet, A.; Le Treut, Y.P.; Sa-Cunha, A.; Mabrut, J.Y.; Chiche, L.; Turrini, O.; Bachellier, P.; Paye, F. Pancreatic adenocarcinoma with venous involvement: Is up-front synchronous portal-superior mesenteric vein resection still justified? A survey of the Association Française de Chirurgie. Ann. Surg. Oncol. 2015, 22, 1874–1883. [Google Scholar] [CrossRef]
- Nakao, A.; Kanzaki, A.; Fujii, T.; Kodera, Y.; Yamada, S.; Sugimoto, H.; Nomoto, S.; Nakamura, S.; Morita, S.; Takeda, S. Correlation between radiographic classification and pathological grade of portal vein wall invasion in pancreatic head cancer. Ann. Surg. 2012, 255, 103–108. [Google Scholar] [CrossRef]
- Tummala, P.; Howard, T.; Agarwal, B. Dramatic Survival Benefit Related to R0 Resection of Pancreatic Adenocarcinoma in Patients With Tumor ≤25 mm in Size and ≤1 Involved Lymph Nodes. Clin. Transl. Gastroenterol. 2013, 4, e33. [Google Scholar] [CrossRef]
- Konstantinidis, I.T.; Warshaw, A.L.; Allen, J.N.; Blaszkowsky, L.S.; Castillo, C.F.; Deshpande, V.; Hong, T.S.; Kwak, E.L.; Lauwers, G.Y.; Ryan, D.P.; et al. Pancreatic ductal adenocarcinoma: Is there a survival difference for R1 resections versus locally advanced unresectable tumors? What is a "true" R0 resection? Ann. Surg. 2013, 257, 731–736. [Google Scholar] [CrossRef]
- Bockhorn, M.; Uzunoglu, F.G.; Adham, M.; Imrie, C.; Milicevic, M.; Sandberg, A.A.; Asbun, H.J.; Bassi, C.; Büchler, M.; Charnley, R.M.; et al. Borderline resectable pancreatic cancer: A consensus statement by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2014, 155, 977–988. [Google Scholar] [CrossRef]
- Artinyan, A.; Anaya, D.A.; McKenzie, S.; Ellenhorn, J.D.; Kim, J. Neoadjuvant therapy is associated with improved survival in resectable pancreatic adenocarcinoma. Cancer 2010, 117, 2044–2049. [Google Scholar] [CrossRef]
- Ducreux, M.; Cuhna, A.S.; Caramella, C.; Hollebecque, A.; Burtin, P.; Goéré, D.; Seufferlein, T.; Haustermans, K.; Van Laethem, J.L.; Conroy, T.; et al. Cancer of the pancreas: ESMO Clinical Practice Guidelines for diagnosis; treatment and follow-up. Ann. Oncol. 2015, 26((Suppl. 5)), v56–v68. [Google Scholar] [CrossRef]
- Jang, J.Y.; Han, Y.; Lee, H.; Kim, S.W.; Kwon, W.; Lee, K.H.; Oh, D.Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological Benefits of Neoadjuvant Chemoradiation With Gemcitabine Versus Upfront Surgery in Patients With Borderline Resectable Pancreatic Cancer: A Prospective, Randomized, Open-label, Multicenter Phase 2/3 Trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- D’Angelo, F.; Antolino, L.; Farcomeni, A.; Sirimarco, D.; Kazemi Nava, A.; De Siena, M.; Petrucciani, N.; Nigri, G.; Valabrega, S.; Aurello, P.; et al. Neoadjuvant treatment in pancreatic cancer: Evidence-based medicine? A systematic review and meta-analysis. Med. Oncol. 2017, 34, 85. [Google Scholar] [CrossRef] [PubMed]
- Versteijne, E.; Suker, M.; Groothuis, K.; Akkermans-Vogelaar, J.M.; Besselink, M.G.; Bonsing, B.A.; Buijsen, J.; Busch, O.R.; Creemers, G.M.; van Dam, R.M.; et al. Preoperative Chemoradiotherapy Versus Immediate Surgery for Resectable and Borderline Resectable Pancreatic Cancer: Results of the Dutch Randomized Phase III PREOPANC Trial. J. Clin. Oncol. 2020, 38, 1763–1773. [Google Scholar] [CrossRef] [PubMed]
- Ravikumar, R.; Sabin, C.; Abu Hilal, M.; Al-Hilli, A.; Aroori, S.; Bond-Smith, G.; Bramhall, S.; Coldham, C.; Hammond, J.; Hutchins, R.; et al. Impact of portal vein infiltration and type of venous reconstruction in surgery for borderline resectable pancreatic cancer. Br. J. Surg. 2017, 104, 1539–1548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malleo, G.; Maggino, L.; Marchegiani, G.; Feriani, G.; Esposito, A.; Landoni, L.; Casetti, L.; Paiella, S.; Baggio, E.; Lipari, G.; et al. Pancreatectomy with venous resection for pT3 head adenocarcinoma: Perioperative outcomes; recurrence pattern and prognostic implications of histologically confirmed vascular infiltration. Pancreatology 2017, 17, 847–857. [Google Scholar] [CrossRef] [PubMed]
- Tseng, J.F.; Raut, C.P.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Abdalla, E.K.; Gomez, H.F.; Sun, C.C.; Crane, C.H.; Wolff, R.A.; et al. Pancreaticoduodenectomy with vascular resection: Margin status and survival duration. J. Gastrointest. Surg. 2004, 8, 935–950. [Google Scholar] [CrossRef]
- Yekebas, E.F.; Bogoevski, D.; Cataldegirmen, G.; Kunze, C.; Marx, A.; Vashist, Y.K.; Schurr, P.G.; Liebl, L.; Thieltges, S.; Gawad, K.A.; et al. En bloc vascular resection for locally advanced pancreatic malignancies infiltrating major blood vessels: Perioperative outcome and long-term survival in 136 patients. Ann. Surg. 2008, 247, 300–309. [Google Scholar] [CrossRef]
- Kaissis, G.A.; Lohöfer, F.K.; Ziegelmayer, S.; Danner, J.; Jäger, C.; Schirren, R.; Ankerst, D.; Ceyhan, G.O.; Friess, H.; Rummeny, E.J.; et al. Borderline-resectable pancreatic adenocarcinoma: Contour irregularity of the venous confluence in pre-operative computed tomography predicts histopathological infiltration. PLoS ONE 2019, 14, e0208717. [Google Scholar] [CrossRef]
- Fang, J.Z.; Lu, C.D.; Wu, S.D.; Huang, J.; Zhou, J. Portal vein/superior mesenteric vein resection in pancreatic cancer treatment in the elderly. Medicine 2017, 96, e7335. [Google Scholar] [CrossRef]
- Castleberry, A.W.; White, R.R.; De La Fuente, S.G.; Clary, B.M.; Blazer, D.G., 3rd; McCann, R.L.; Pappas, T.N.; Tyler, D.S.; Scarborough, J.E. The impact of vascular resection on early postoperative outcomes after pancreaticoduodenectomy: An analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Ann. Surg. Oncol. 2012, 19, 4068–4077. [Google Scholar] [CrossRef] [PubMed]
- Worni, M.; Castleberry, A.W.; Clary, B.M.; Gloor, B.; Carvalho, E.; Jacobs, D.O.; Pietrobon, R.; Scarborough, J.E.; White, R.R. Concomitant vascular reconstruction during pancreatectomy for malignant disease: A propensity score-adjusted; population-based trend analysis involving10;206 patients. JAMA Surg. 2013, 148, 331–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramacciato, G.; Mercantini, P.; Petrucciani, N.; Nigri, G.R.; Kazemi, A.; Muroni, M.; Del Gaudio, M.; Balesh, A.; Cescon, M.; Cucchetti, A.; et al. Risk factors of pancreatic fistula after pancreaticoduodenectomy: A collective review. Am. Surg. 2011, 77, 257–269. [Google Scholar]
- Nigri, G.R.; Rosman, A.S.; Petrucciani, N.; Fancellu, A.; Pisano, M.; Zorcolo, L.; Ramacciato, G.; Melis, M. Metaanalysis of trials comparing minimally invasive and open distal pancreatectomies. Surg. Endosc. 2011, 25, 1642–1651. [Google Scholar] [CrossRef] [PubMed]
- Fancellu, A.; Ginesu, G.C.; Feo, C.F.; Cossu, M.L.; Puledda, M.; Pinna, A.; Porcu, A. Pancreatic head excavation for tissue diagnosis may reduce unnecessary pancreaticoduodenectomies in the setting of chronic pancreatitis. Hepatobiliary Pancreat. Dis. Int. 2017, 16, 315–322. [Google Scholar] [CrossRef]
- Carrère, N.; Sauvanet, A.; Goere, D.; Kianmanesh, R.; Vullierme, M.P.; Couvelard, A.; Ruszniewski, P.; Belghiti, J. Pancreaticoduodenectomy with mesenteric portal vein resection for adenocarcinoma of the pancreatic head. World J. Surg. 2006, 30, 1526–1535. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Year | Country | Time Frame | PD+VR | PD | Age | Stage | Survival Outcomes |
|---|---|---|---|---|---|---|---|---|
| Addeo P [12] | 2017 | France | 2006–2014 | 91 | 90 | PD+VR: 66 PD: 67 | NR | Median OS 27 vs. 22 months (p = 0.28) |
| Banz VM [23] | 2011 | UK | 1997–2009 | 51 | 275 | PD+VR: 67 PD 65: | IB: 3 (0.9%) IIA: 54 (16.6%) IIB: 268 (82.2%) IV: 1 (0.3%) | Median OS 14.8 vs. 14.5 months (p = 0.41) |
| Chakravarty K [24] | 2010 | Taiwan | 1996–2006 | 12 | 75 | PD+VR: 62.9 PD: 62.9 | IIA: 14 (16.1%) IIB: 3 (3.4%) | 5-year OS 16.7 vs. 12.2 (p = 0.9) |
| Cherukuru R [25] | 2018 | India | 2010–2016 | 26 | 15 | 59 * | NR | Median OS 14 vs. 17 months (p = 0.9) |
| Howard TJ [29] | 2003 | USA | NR | 13 | 23 | PD+VR: 68 PD: 67.8 | I: 6 (16.7%) II: 9 (25%) III: 21 (58.3%) | Median OS 12 vs. 13 months (p < 0.05) |
| Hristov B [28] | 2010 | USA | 1993–2005 | 20 | 140 | PD+VR: 63.5 PD: 54 | NR | Median OS 20.8 vs. 21.4 months (p < 0.05) |
| Jeong J [30] | 2015 | South Korea | 1995–2009 | 46 | 230 | PD+VR: 60.5 PD: 61.5 | NR | Median OS 16 vs. 12 months (p = 0.08) |
| Kaneoka Y [26] | 2009 | Japan | 1993–2006 | 42 | 42 | PD+VR: 66 PD: 65 | IA: 6 (6.9%) IB: 6 (6.9%) IIA: 30 (34.5%) IIB: 38 (43.7%) III: 2 (2.3%) IV: 5 (5.7%) | Median OS 26 vs. 12 months (p = 0.04) |
| Kelly KJ [27] | 2013 | USA | 2000–2007 | 70 | 422 | PD+VR: 66.8 PD: 65 | NR | Median OS 19.3 vs. 15.6 months (p = 0.05) |
| Leach SD [31] | 1998 | USA | 1990–1995 | 31 | 44 | PD+VR: 66 PD: 64 | NR | Median OS 20 vs. 22 months (p = 0.25) |
| Martin D [32] | 2018 | Switzerland | 2008–2013 | 29 | 29 | PD+VR: 69 PD: 66 | NR | Median OS 12.9 vs. 20.3 months (p = 0.13) |
| Menon VG [33] | 2013 | USA | 2007–2012 | 18 | 43 | PD+VR: 67.2 PR: 69 | IIB: 41 (67.2%) | Median OS 31 vs. 31 months (p = 0.9) |
| Murakami Y [34] | 2015 | Japan | 2001–2012 | 435 | 502 | 68 * | IA-I: 58 (6.2%) IIA-IIB-III-IV: 879 (93.8%) | Median OS 18.5 vs. 25.8 months (p < 0.01) |
| Ohgi K [35] | 2017 | Japan | 2002–2014 | 158 | 141 | PD+VR: 68 PD: 67 | NR | Median OS 20.7 vs. 18.6 months (p = 0.8) |
| Poon RT [36] | 2004 | China | 1998–2002 | 12 | 38 | PD+VR: 61.5 PD: 62.5 | I: 17 (34%) II: 7 (14%) III: 18 (36%) IV: 8 (16%) | Median OS 19.5 vs 20.7 months (p = 0.8) |
| Ravikumar R [37] | 2014 | UK | 1998–2011 | 230 | 840 | PD+VR: 65 PD: 66 | NR | Median OS 18 vs. 18.2 months (p NR) |
| Roch AM [38] | 2016 | USA | 2000–2014 | 90 | 477 | PD+VR: 66.4 PD: 66.3 | NR | Median OS 14 vs. 21 months (p = 0.08) |
| Toomey P [39] | 2009 | USA | NR | 48 | 172 | PD+VR: 67 PD: 68 | IA: 10 (4.5%) IA: 40 (18.2%) IIA: 43 (19.6%) IIB: 127 (57.7%) | Median OS 18 vs. 17 months (p = 0.84) |
| Turley RS [40] | 2012 | USA | 1997–2008 | 42 | 162 | PD+VR: 63.5 PD: 66 | NR | Median OS 21 vs. 20 months (p = 0.9) |
| Wang F [41] | 2014 | Australia | 2004–2012 | 64 | 58 | PD+VR: 66 PD: 67 | IA: 1 (0.8%) IB: 3 (2.5%) IIA: 27 (22.5%) IIB: 75 (62.5%) III: 9 (7.5%) IV: 5 (4.2%) | Median OS 18 vs. 31 months (p = 0.02) |
| Wang WL [8] | 2015 | China | 2009–2013 | 42 | 166 | PD+VR: 59.4 PD: 60.5 | NR | Median OS 20 vs 26 months (p = 0.2) |
| Xie ZB [42] | 2019 | China | 2011–2013 | 138 | 239 | PD+VR: 62.75 PD: 61.54 | I: 136 (36.1%) II: 210 (55.7%) III: 31 (8.2%) | Median OS 25.1 vs. 29.3 months (p = 0.04) |
| Zhao X [43] | 2016 | China | 2014–2016 | 21 | 85 | PD+VR: 63 PD: 63.5 | IA: 17 (16%) IB: 18 (17%) IIA: 6 (5.7%) IIB: 65 (61.3%) | Median OS 15 vs. 19 months (p < 0.05) |
| Variables | No. of Pooled Studies | Mean PD+VR | Mean PD | Difference or Odds Ratio | 95% LLCI | 95% ULCI |
|---|---|---|---|---|---|---|
| Blood loss (ml) | 9 | 977.8 | 743.31 | 209.22 | −84.18 | 502.62 |
| Operative time (min) | 9 | 421.1 | 361.4 | 58.16 | 38.3 | 77.9 |
| Positive margin status | 9 | 0.27 | 0.22 | 1.69 | 1.23 | 2.31 |
| R0 resection | 17 | 0.58 | 0.68 | 0.6 | 0.47 | 0.75 |
| Delayed gastric emptying | 13 | 0.17 | 0.09 | 1.56 | 1.19 | 2.05 |
| Mortality | 17 | 0.03 | 0.02 | 1.93 | 1.28 | 2.91 |
| Overall complications | 8 | 0.4 | 0.4 | 1.07 | 0.81 | 1.41 |
| Pancreatic fistula | 14 | 0.2 | 0.2 | 0.74 | 0.57 | 0.95 |
| Postoperative Hemorrage | 4 | 0.1 | 0.04 | 1.44 | 0.84 | 2.47 |
| Reoperations | 7 | 0.1 | 0.1 | 1.21 | 0.78 | 1.87 |
| 1-yr OS | 13 | 0.6 | 0.7 | 0.79 | 0.67 | 0.92 |
| 3-yr OS | 11 | 0.2 | 0.2 | 0.72 | 0.59 | 0.87 |
| 5-yr OS | 8 | 0.1 | 0.2 | 0.57 | 0.39 | 0.83 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fancellu, A.; Petrucciani, N.; Porcu, A.; Deiana, G.; Sanna, V.; Ninniri, C.; Perra, T.; Celoria, V.; Nigri, G. The Impact on Survival and Morbidity of Portal–Mesenteric Resection During Pancreaticoduodenectomy for Pancreatic Head Adenocarcinoma: A Systematic Review and Meta-Analysis of Comparative Studies. Cancers 2020, 12, 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071976
Fancellu A, Petrucciani N, Porcu A, Deiana G, Sanna V, Ninniri C, Perra T, Celoria V, Nigri G. The Impact on Survival and Morbidity of Portal–Mesenteric Resection During Pancreaticoduodenectomy for Pancreatic Head Adenocarcinoma: A Systematic Review and Meta-Analysis of Comparative Studies. Cancers. 2020; 12(7):1976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071976
Chicago/Turabian StyleFancellu, Alessandro, Niccolò Petrucciani, Alberto Porcu, Giulia Deiana, Valeria Sanna, Chiara Ninniri, Teresa Perra, Valentina Celoria, and Giuseppe Nigri. 2020. "The Impact on Survival and Morbidity of Portal–Mesenteric Resection During Pancreaticoduodenectomy for Pancreatic Head Adenocarcinoma: A Systematic Review and Meta-Analysis of Comparative Studies" Cancers 12, no. 7: 1976. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12071976