Concurrent TP53 and CDKN2A Gene Aberrations in Newly Diagnosed Mantle Cell Lymphoma Correlate with Chemoresistance and Call for Innovative Upfront Therapy

 , , ,
, , ,
Abstract
:1. Introduction
2. Patients and Methods
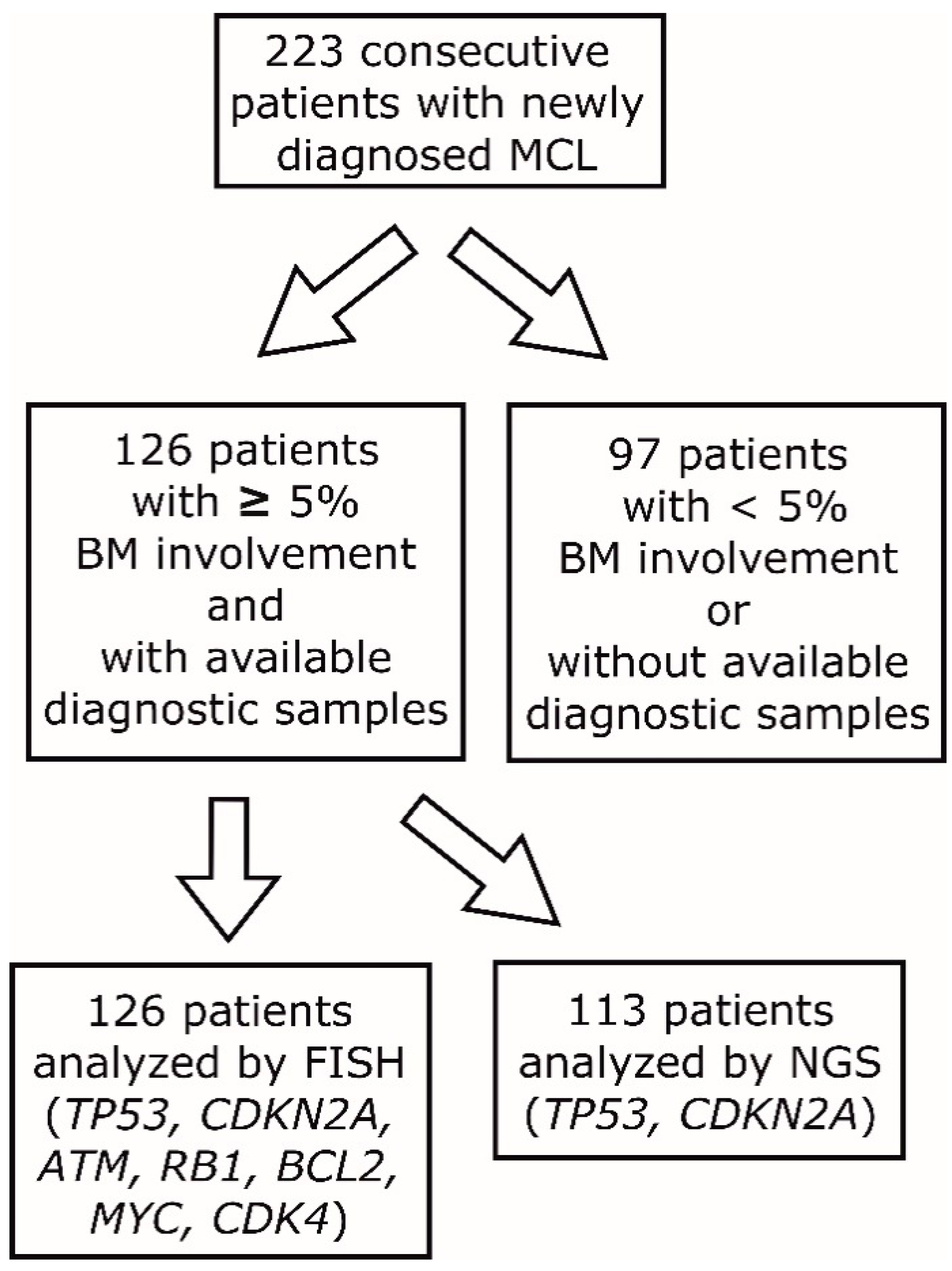
2.1. Patients’ Characteristics
2.2. Fluorescence in Situ Hybridization (FISH)
2.3. TP53 and CDKN2A Mutation Assessment by Next-Generation Sequencing (NGS)
2.4. Statistical Analysis
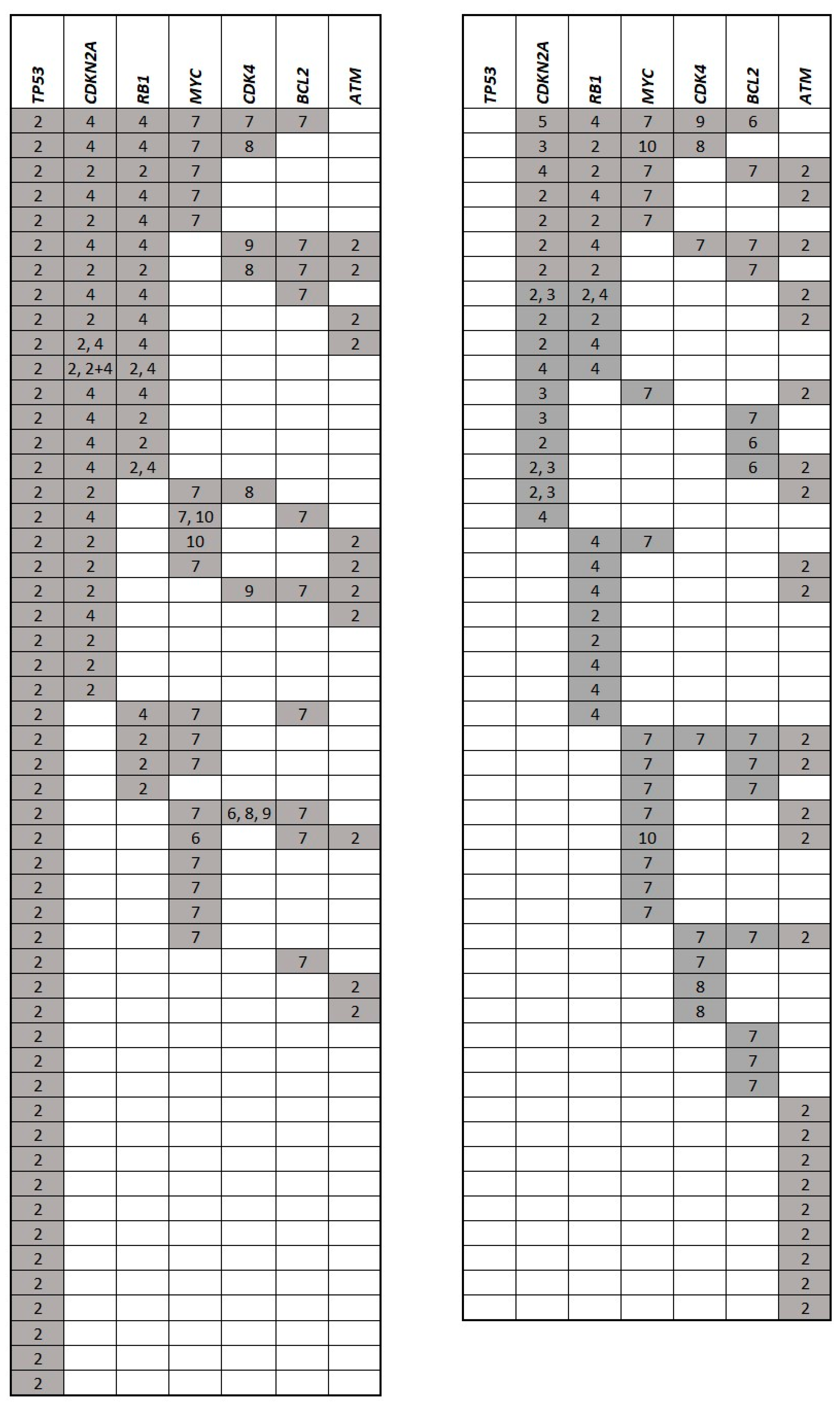
3. Results
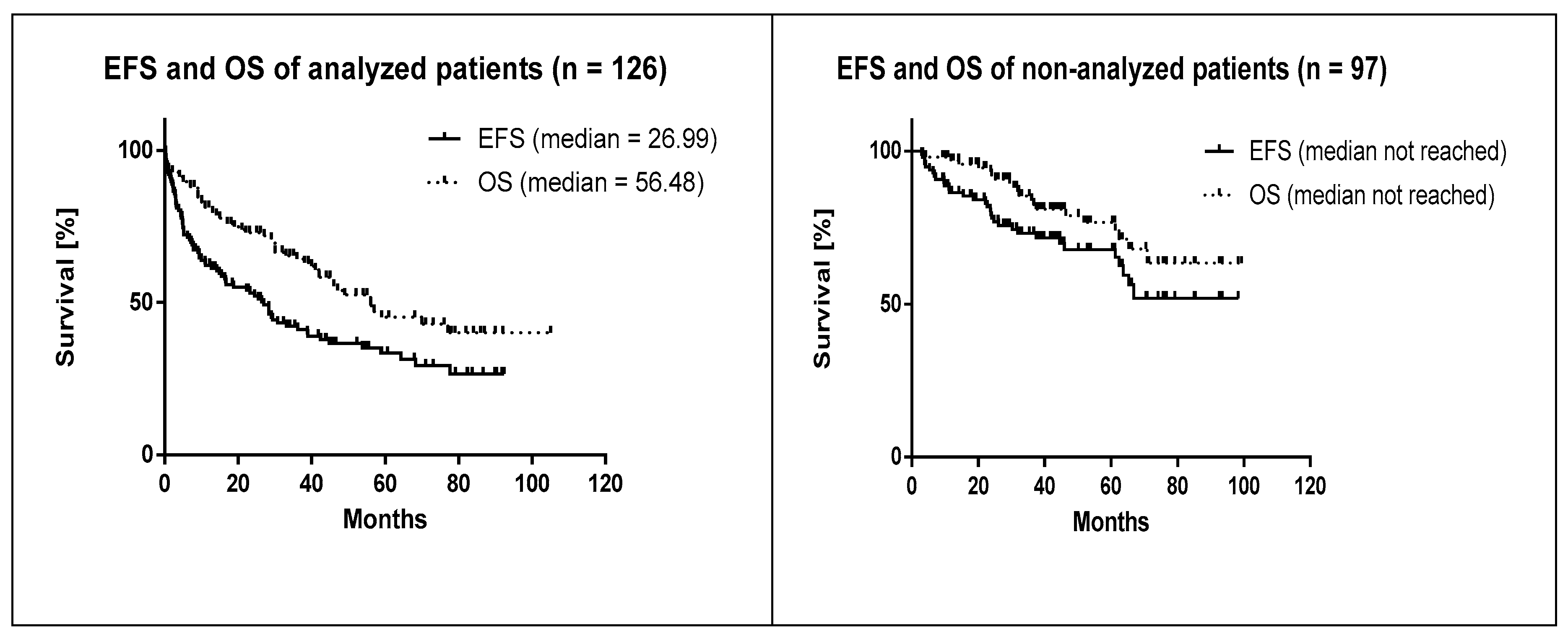
3.1. Baseline Characteristics of the Analyzed Patients
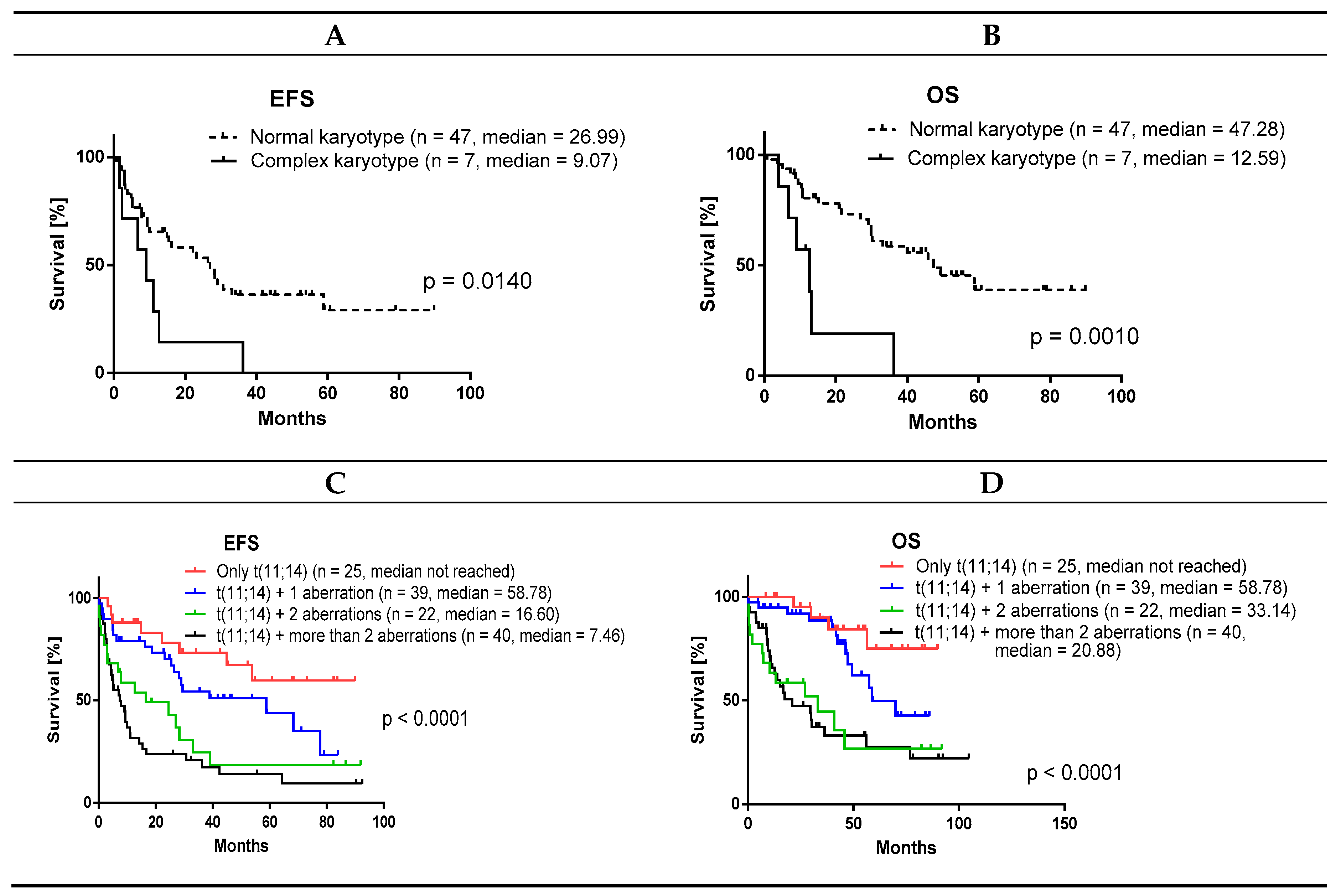
3.2. Correlation of Baseline Clinical and Histopathological Parameters on Survival in the Cohort of 126 Patients with ≥5% BM Involvement
4. Discussion
4.1. TP53 Deletions and Mutations
4.2. Survival Analysis
4.3. Concurrent Aberration of TP53 and Deletion of CDKN2A Is Associated with Chemoresistance
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Klener, P. Advances in Molecular Biology and Targeted Therapy of Mantle Cell Lymphoma. Int. J. Mol. Sci. 2019, 20, 4417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheah, C.Y.; Seymour, J.F.; Wang, M.L. Mantle Cell Lymphoma. J. Clin. Oncol. 2016, 34, 1256–1269. [Google Scholar] [CrossRef] [PubMed]
- Jain, P.; Wang, M. Mantle cell lymphoma: 2019 update on the diagnosis, pathogenesis, prognostication, and management. Am. J. Hematol. 2019, 94, 710–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maddocks, K. Update on mantle cell lymphoma. Blood 2018, 132, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Rule, S. The modern approach to mantle cell lymphoma. Hematol. Oncol. 2019, 37, 66–69. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, J.; Jima, D.; Moffitt, A.B.; Liu, Q.; Czader, M.; Hsi, E.D.; Fedoriw, Y.; Dunphy, C.H.; Richards, K.L.; Gill, J.I.; et al. The genomic landscape of mantle cell lymphoma is related to the epigenetically determined chromatin state of normal B cells. Blood J. Am. Soc. Hematol. 2014, 123, 2988–2996. [Google Scholar] [CrossRef]
- Bea, S.; Valdes-Mas, R.; Navarro, A.; Salaverria, I.; Martín-Garcia, D.; Jares, P.; Giné, E.; Pinyol, M.; Royo, C.; Nadeu, F.; et al. Landscape of somatic mutations and clonal evolution in mantle cell lymphoma. Proc. Natl. Acad. Sci. USA 2013, 110, 18250–18255. [Google Scholar] [CrossRef] [Green Version]
- Yang, P.; Zhang, W.; Wang, J.; Liu, Y.; An, R.; Jing, H. Genomic landscape and prognostic analysis of mantle cell lymphoma. Cancer Gene Ther. 2018, 25, 129–140. [Google Scholar] [CrossRef]
- Ahmed, M.; Zhang, L.; Nomie, K.; Lam, L.; Wang, M. Gene mutations and actionable genetic lesions in mantle cell lymphoma. Oncotarget 2016, 7, 58638–58648. [Google Scholar] [CrossRef] [Green Version]
- Kridel, R.; Meissner, B.; Rogic, S.; Boyle, M.; Telenius, A.; Woolcock, B.; Gunawardana, J.; Jenkins, C.; Cochrane, C.; Ben-Neriah, S.; et al. Whole transcriptome sequencing reveals recurrent NOTCH1 mutations in mantle cell lymphoma. Blood 2012, 119, 1963–1971. [Google Scholar] [CrossRef]
- Wang, L.; Tang, G.; Medeiros, L.J.; Xu, J.; Huang, W.; Yin, C.C.; Wang, M.; Jain, P.; Lin, P.; Li, S. MYC rearrangement but not extra MYC copies is an independent prognostic factor in patients with mantle cell lymphoma. Haematologica 2020, 105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferrero, S.; Rossi, D.; Rinaldi, A.; Bruscaggin, A.; Spina, V.; Eskelund, C.W.; Evangelista, A.; Moia, R.; Kwee, I.; Dahl, C. KMT2D mutations and TP53 disruptions are poor prognostic biomarkers in mantle cell lymphoma receiving high-dose therapy: A FIL study. Haematologica 2020, 105, 1604–1612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, H.A.; Qi, X.; Jain, P.; Nomie, K.; Wang, Y.; Zhou, S.; Wang, M.L. Genetic mutations and features of mantle cell lymphoma: A systematic review and meta-analysis. Blood Adv. 2020, 4, 2927–2938. [Google Scholar] [CrossRef] [PubMed]
- Hoster, E.; Dreyling, M.; Klapper, W.; Gisselbrecht, C.; Van Hoof, A.; Kluin-Nelemans, H.C.; Pfreundschuh, M.; Reiser, M.; Metzner, B.; Einsele, H.; et al. A new prognostic index (MIPI) for patients with advanced-stage mantle cell lymphoma. Blood 2008, 111, 558–565. [Google Scholar] [CrossRef]
- Hoster, E.; Rosenwald, A.; Berger, F.; Bernd, H.W.; Hartmann, S.; Loddenkemper, C.; Barth, T.F.; Brousse, N.; Pileri, S.; Rymkiewicz, G.; et al. Prognostic Value of Ki-67 Index, Cytology, and Growth Pattern in Mantle-Cell Lymphoma: Results from Randomized Trials of the European Mantle Cell Lymphoma Network. J. Clin. Oncol. 2016, 34, 1386–1394. [Google Scholar] [CrossRef]
- Eskelund, C.W.; Dahl, C.; Hansen, J.W.; Westman, M.; Kolstad, A.; Pedersen, L.B.; Montano-Almendras, C.P.; Husby, S.; Freiburghaus, C.; Ek, S.; et al. TP53 mutations identify younger mantle cell lymphoma patients who do not benefit from intensive chemoimmunotherapy. Blood J. Am. Soc. Hematol. 2017, 130, 1903–1910. [Google Scholar] [CrossRef] [Green Version]
- Clot, G.; Jares, P.; Gine, E.; Navarro, A.; Royo, C.; Pinyol, M.; Martín-Garcia, D.; Demajo, S.; Espinet, B.; Salar, A.; et al. A gene signature that distinguishes conventional and leukemic nonnodal mantle cell lymphoma helps predict outcome. Blood 2018, 132, 413–422. [Google Scholar] [CrossRef] [Green Version]
- Delfau-Larue, M.H.; Klapper, W.; Berger, F.; Jardin, F.; Briere, J.; Salles, G.; Casasnovas, O.; Feugier, P.; Haioun, C.; Ribrag, V.; et al. High-Dose cytarabine does not overcome the adverse prognostic value of CDKN2A and TP53 deletions in mantle cell lymphoma. Blood J. Am. Soc. Hematol. 2015, 126, 604–611. [Google Scholar] [CrossRef] [Green Version]
- Obr, A.; Prochazka, V.; Jirkuvova, A.; Urbánková, H.; Kriegova, E.; Schneiderová, P.; Vatolíková, M.; Papajík, T. TP53 Mutation and Complex Karyotype Portends a Dismal Prognosis in Patients with Mantle Cell Lymphoma. Clin. Lymphoma Myeloma Leuk. 2018, 18, 762–768. [Google Scholar] [CrossRef]
- Petrackova, A.; Vasinek, M.; Sedlarikova, L.; Dyskova, T.; Schneiderova, P.; Novosad, T.; Papajik, T.; Kriegova, E. Standardization of Sequencing Coverage Depth in NGS: Recommendation for Detection of Clonal and Subclonal Mutations in Cancer Diagnostics. Front. Oncol. 2019, 9, 851. [Google Scholar] [CrossRef]
- Ishwaran, H.; Lu, M. Standard errors and confidence intervals for variable importance in random forest regression, classification, and survival. Stat. Med. 2019, 38, 558–582. [Google Scholar] [CrossRef] [PubMed]
- Cheson, B.D.; Horning, S.J.; Coiffier, B.; Shipp, M.A.; Fisher, R.I.; Connors, J.M.; Lister, T.A.; Vose, J.; Grillo-López, A.; Hagenbeek, A.; et al. Report of an international workshop to standardize response criteria for non-Hodgkin’s lymphomas. NCI Sponsored International Working Group. J. Clin. Oncol. 1999, 17, 1244. [Google Scholar] [CrossRef] [PubMed]
- Zenz, T.; Krober, A.; Scherer, K.; Häbe, S.; Bühler, A.; Benner, A.; Denzel, T.; Winkler, D.; Edelmann, J.; Schwänen, C.; et al. Monoallelic TP53 inactivation is associated with poor prognosis in chronic lymphocytic leukemia: Results from a detailed genetic characterization with long-term follow-up. Blood J. Am. Soc. Hematol. 2008, 112, 3322–3329. [Google Scholar] [CrossRef] [PubMed]
- Streich, L.; Sukhanova, M.; Lu, X.; Chen, Y.H.; Venkataraman, G.; Mathews, S.; Zhang, S.; Kelemen, K.; Segal, J.; Gao, J.; et al. Aggressive morphologic variants of mantle cell lymphoma characterized with high genomic instability showing frequent chromothripsis, CDKN2A/B loss, and TP53 mutations: A multi-institutional study. Genes Chromosomes Cancer 2020, 59, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Beato, M.; Saez, A.I.; Navas, I.C.; Algara, P.; Mateo, M.S.; Villuendas, R.; Camacho, F.; Sánchez-Aguilera, A.; Sánchez, E.; Piris, M.A. Overall survival in aggressive B-Cell lymphomas is dependent on the accumulation of alterations in p53, p16, and p27. Am. J. Pathol. 2001, 159, 205–213. [Google Scholar] [CrossRef] [Green Version]
- Lopez, C.; Kleinheinz, K.; Aukema, S.M.; Rohde, M.; Bernhart, S.H.; Hübschmann, D.; Wagener, R.; Toprak, U.H.; Raimondi, F.; Kreuz, M.; et al. Genomic and transcriptomic changes complement each other in the pathogenesis of sporadic Burkitt lymphoma. Nat. Commun. 2019, 10, 1459. [Google Scholar] [CrossRef] [Green Version]
- Bolen, C.R.; Klanova, M.; Trneny, M.; Sehn, L.H.; He, J.; Tong, J.; Paulson, J.N.; Kim, E.; Vitolo, U.; Di Rocco, A.; et al. Prognostic impact of somatic mutations in diffuse large B-Cell lymphoma and relationship to cell-of-origin: Data from the phase III GOYA study. Haematologica 2019, 105, 227892. [Google Scholar] [CrossRef] [Green Version]
- Rossi, D.; Spina, V.; Gaidano, G. Biology and treatment of Richter syndrome. Blood 2018, 131, 2761–2772. [Google Scholar] [CrossRef] [Green Version]
- Chigrinova, E.; Rinaldi, A.; Kwee, I.; Rossi, D.; Rancoita, P.M.; Strefford, J.C.; Oscier, D.; Stamatopoulos, K.; Papadaki, T.; Berger, F.; et al. Two main genetic pathways lead to the transformation of chronic lymphocytic leukemia to Richter syndrome. Blood J. Am. Soc. Hematol. 2013, 122, 2673–2682. [Google Scholar] [CrossRef] [Green Version]
- Kwiecinska, A.; Ichimura, K.; Berglund, M.; Dinets, A.; Sulaiman, L.; Collins, V.P.; Larsson, C.; Porwit, A.; Lagercrantz, S.B. Amplification of 2p as a genomic marker for transformation in lymphoma. Genes Chromosomes Cancer 2014, 53, 750–768. [Google Scholar] [CrossRef] [Green Version]
- Pasqualucci, L.; Khiabanian, H.; Fangazio, M.; Vasishtha, M.; Messina, M.; Holmes, A.B.; Ouillette, P.; Trifonov, V.; Rossi, D.; Tabbò, F.; et al. Genetics of follicular lymphoma transformation. Cell Rep. 2014, 6, 130–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cohort | 126 Patients with Bone Marrow Involvement ≥5% | 97 Patients with No Available Diagnostic Samples | ||
|---|---|---|---|---|
| Numbers (N) or percentages (%) | N | % | N | % |
| All patients | 126 | 57 | 97 | 43 |
| M | 88 | 70 | 73 | 75 |
| F | 38 | 30 | 24 | 25 |
| Age (median; years) | 68 | 66 | ||
| Age (range; years) | 29–82 | 40–87 | ||
| <65 years | 47 | 37 | 44 | 45 |
| ≥65 years | 79 | 63 | 53 | 55 |
| Stage I–II | 0 | 0 | 7 | 7 |
| Stage III | 0 | 0 | 13 | 13 |
| Stage IV | 126 | 100 | 77 | 79 |
| Ki-67 ≥ 30% * | 36 | 47 | 38 | 48 |
| MIPI 1 | 19 | 15 | 25 | 26 |
| MIPI 2 | 29 | 23 | 34 | 35 |
| MIPI 3 | 78 | 62 | 38 | 39 |
| B-symptoms | 52 | 41 | 32 | 33 |
| BM infiltration | 126 | 100 | 73 | 75 |
| BM infiltration ≥5% | 126 | 100 | 25 | 26 |
| Nodal involvement | 108 | 86 | 88 | 91 |
| Splenomegaly | 89 | 71 | 46 | 47 |
| Extra-hematological involvement | 50 | 40 | 47 | 48 |
| Bulky disease (≥5 cm) | 45 | 36 | 27 | 28 |
| CNS involvement ** | 17 | 13 | 7 | 7 |
| Intensified therapy | 37 | 29 | 50 | 52 |
| R-CHOP-like therapy | 71 | 56 | 38 | 39 |
| Palliative therapy | 8 | 6 | 7 | 7 |
| Watch and wait | 7 | 6 | 1 | 1 |
| Died before initiation of therapy | 3 | 2 | 0 | 0 |
| Died during induction | 9 | 7 | 0 | 0 |
| ORR (CR/PR) | 90 | 71 | 92 | 95 |
| CR | 61 | 48 | 73 | 75 |
| PR | 29 | 23 | 19 | 20 |
| SD | 4 | 3 | 3 | 3 |
| PD | 15 | 12 | 0 | 0 |
| Event | 78 | 62 | 32 | 33 |
| Relapse | 48 | 38 | 18 | 19 |
| Death ** | 55 | 44 | 21 | 22 |
| CDK4 | RB1 | BCL2 | ATM | TP53 | CDKN2A | MYC | |
|---|---|---|---|---|---|---|---|
| CDK4 | 1 | 0.138 | <0.001 | 0.260 | 0.651 | 0.016 | 0.055 |
| RB1 | 1 | 0.384 | 0.847 | 0.191 | <0.001 | 0.074 | |
| BCL2 | 1 | 0.091 | 0.965 | 0.012 | 0.055 | ||
| ATM | 1 | 0.164 | 0.05 | 0.706 | |||
| TP53 | 1 | 0.006 | 0.071 | ||||
| CDKN2A | 1 | 0.065 | |||||
| MYC | 1 |
| A. Event-Free Survival | B. Overall Survival | ||||||
|---|---|---|---|---|---|---|---|
| Gene | HR | 95% CI | p | Gene | HR | 95% CI | p |
| CDK4 | 1.6 | 0.8–3.1 | 0.218 | CDK4 | 1.7 | 0.8–3.7 | 0.205 |
| RB1 | 0.9 | 0.5–1.6 | 0.803 | RB1 | 1.2 | 0.6–2.2 | 0.645 |
| BCL2 | 1.5 | 0.8–2.5 | 0.287 | BCL2 | 2.6 | 1.4–4.8 | 0.004 |
| ATM | 1.1 | 0.7–1.9 | 0.667 | ATM | 1.0 | 0.6–2.0 | 0.921 |
| TP53 | 2.3 | 1.4–3.6 | 0.001 | TP53 | 2.2 | 1.2–3.8 | 0.008 |
| CDKN2A | 2.6 | 1.5–4.7 | 0.001 | CDKN2A | 2.5 | 1.2–4.9 | 0.011 |
| MYC | 1.6 | 1.0–2.6 | 0.06 | MYC | 1.2 | 0.7–2.2 | 0.507 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malarikova, D.; Berkova, A.; Obr, A.; Blahovcova, P.; Svaton, M.; Forsterova, K.; Kriegova, E.; Prihodova, E.; Pavlistova, L.; Petrackova, A.; et al. Concurrent TP53 and CDKN2A Gene Aberrations in Newly Diagnosed Mantle Cell Lymphoma Correlate with Chemoresistance and Call for Innovative Upfront Therapy. Cancers 2020, 12, 2120. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082120
Malarikova D, Berkova A, Obr A, Blahovcova P, Svaton M, Forsterova K, Kriegova E, Prihodova E, Pavlistova L, Petrackova A, et al. Concurrent TP53 and CDKN2A Gene Aberrations in Newly Diagnosed Mantle Cell Lymphoma Correlate with Chemoresistance and Call for Innovative Upfront Therapy. Cancers. 2020; 12(8):2120. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082120
Chicago/Turabian StyleMalarikova, Diana, Adela Berkova, Ales Obr, Petra Blahovcova, Michael Svaton, Kristina Forsterova, Eva Kriegova, Eva Prihodova, Lenka Pavlistova, Anna Petrackova, and et al. 2020. "Concurrent TP53 and CDKN2A Gene Aberrations in Newly Diagnosed Mantle Cell Lymphoma Correlate with Chemoresistance and Call for Innovative Upfront Therapy" Cancers 12, no. 8: 2120. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12082120