Stage I Squamous Cell Carcinoma of the Anus: Is Radiation Therapy Alone Sufficient Treatment?

 , , , ,
, , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
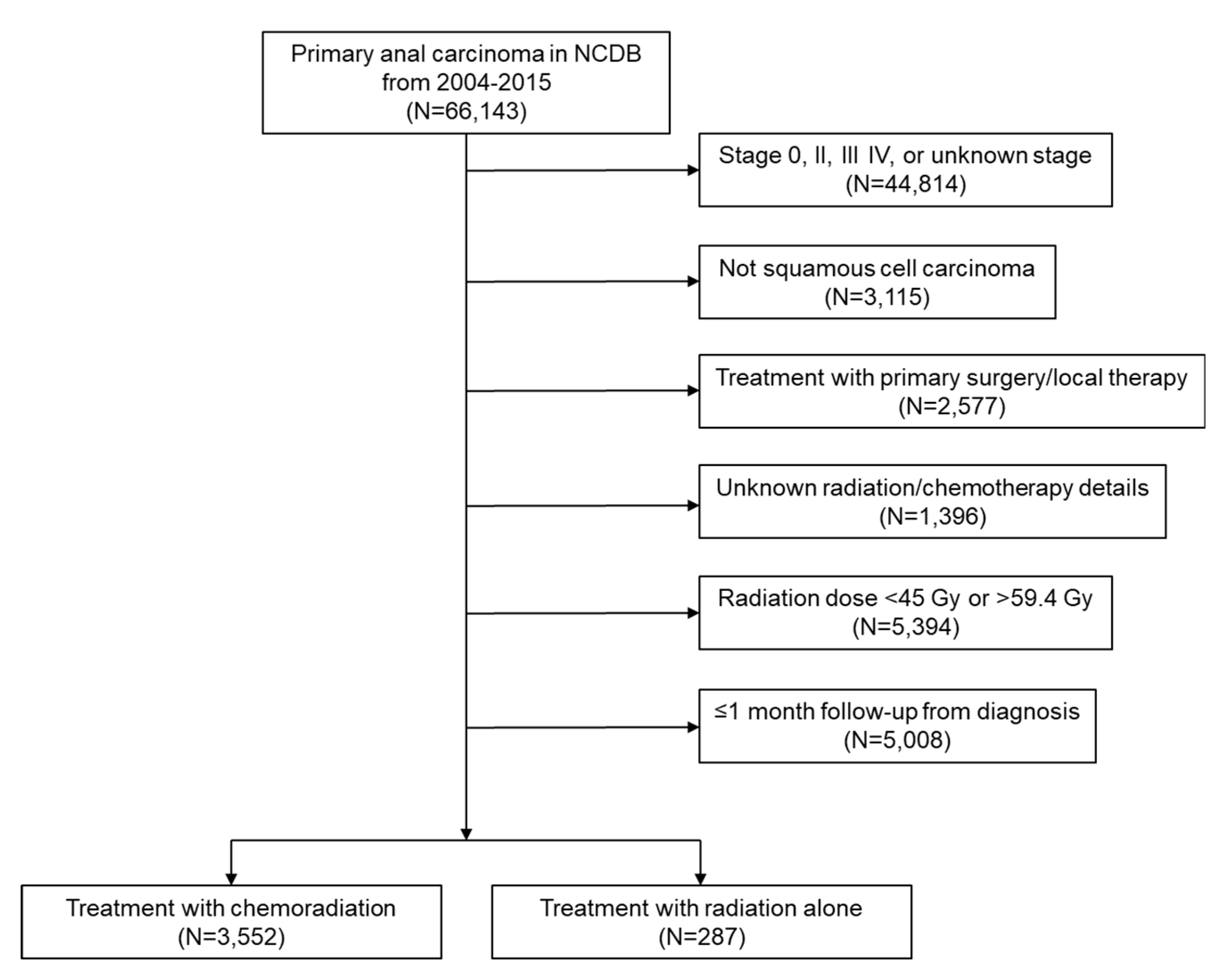
2.1. Baseline Characteristics
2.2. Factors Associated with RT Alone versus CRT
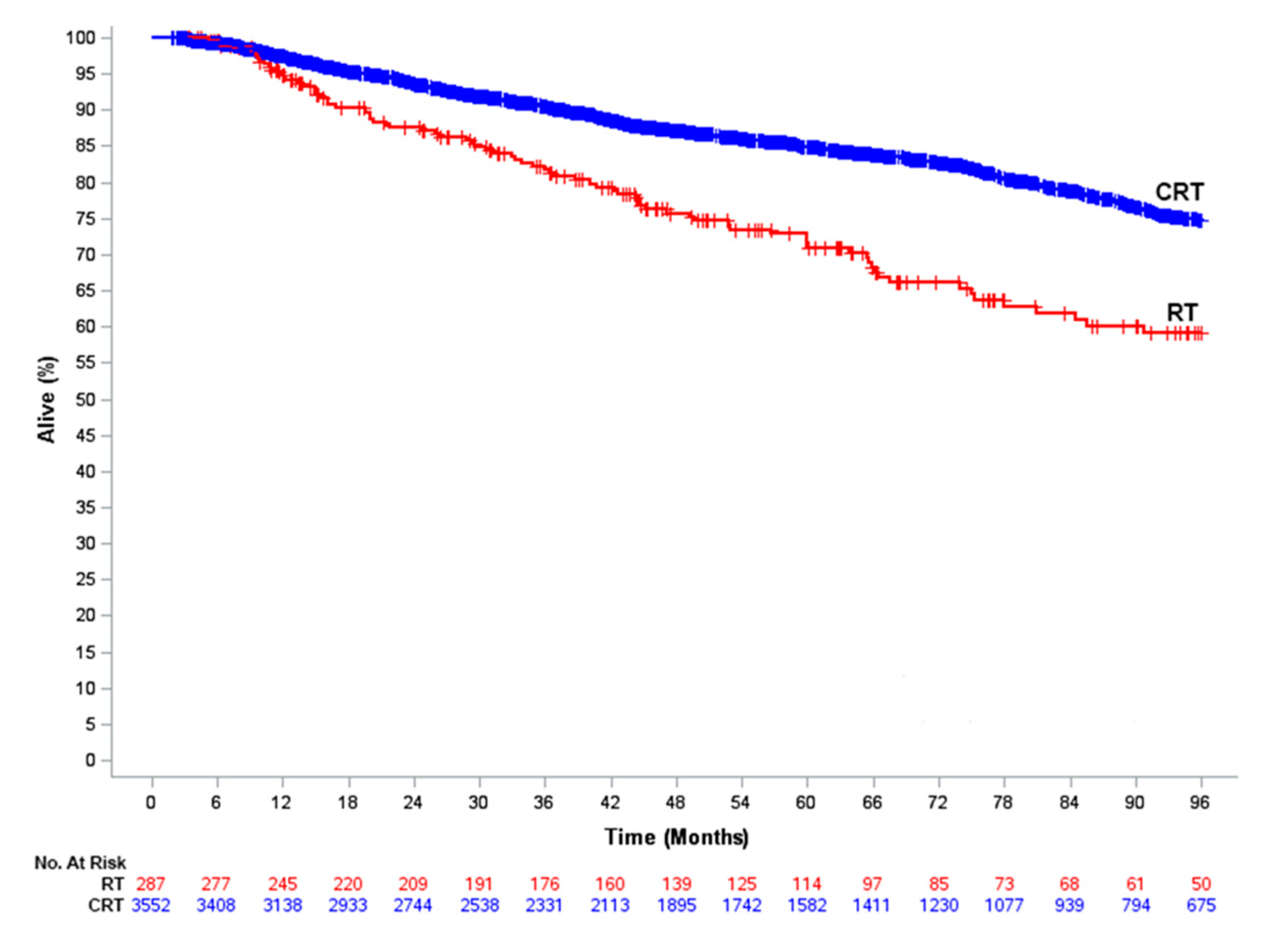
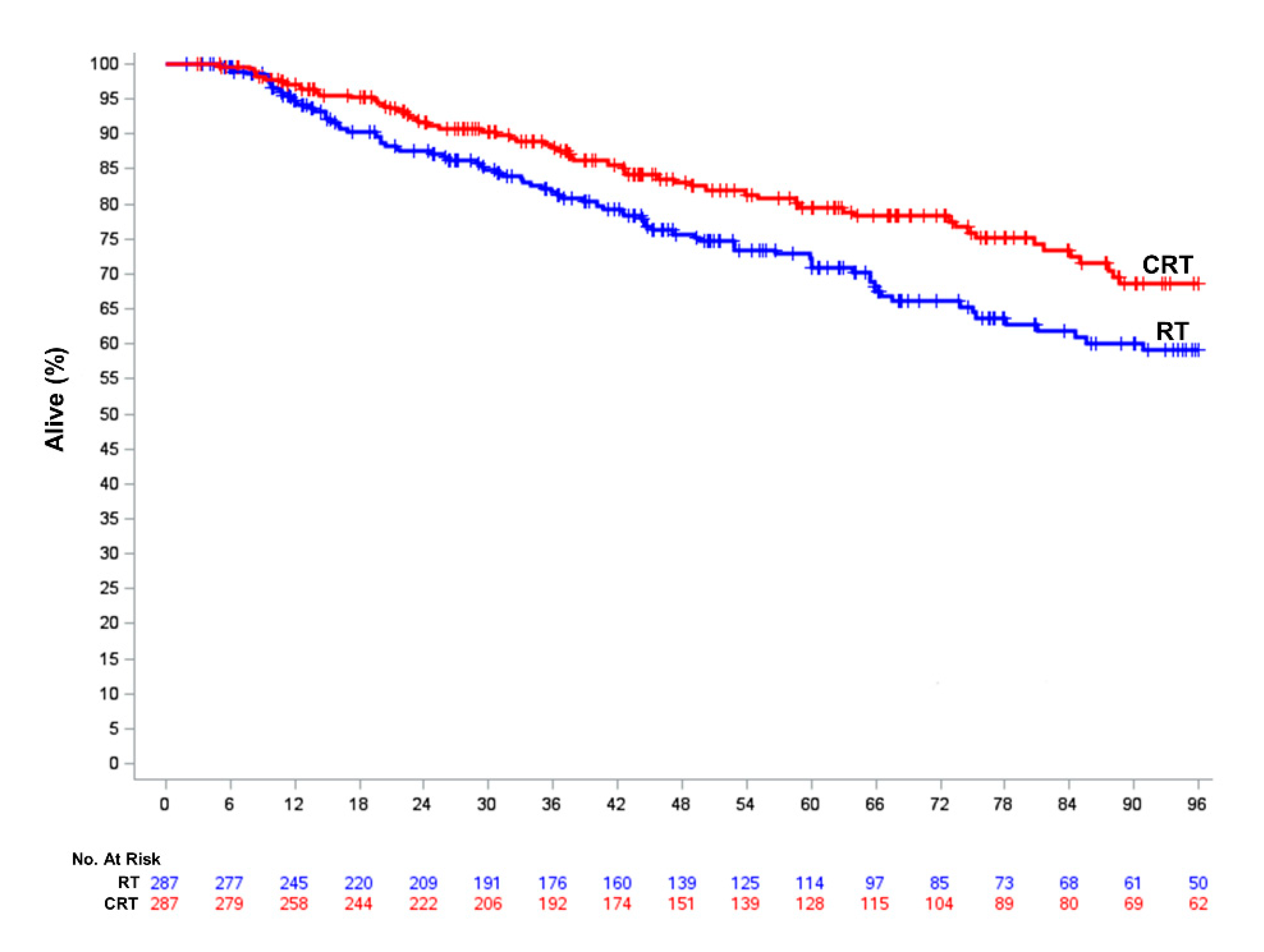
2.3. Overall Survival in CRT and RT Patients
3. Discussion
4. Materials and Methods
4.1. Treatment Definitions
4.2. Study Variables
4.3. Statistical Methods
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- UKCCCR Anal Cancer Trial Working Party. Epidermoid anal cancer: Results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 1996, 348, 1049–1054. [Google Scholar] [CrossRef]
- Bartelink, H.; Roelofsen, F.; Eschwege, F.; Rougier, P.; Bosset, J.F.; Gonzalez, D.G.; Peiffert, D.; van Glabbeke, M.; Pierart, M. Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: Results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J. Clin. Oncol. 1997, 15, 2040–2049. [Google Scholar] [CrossRef] [PubMed]
- Northover, J.; Glynne-Jones, R.; Sebag-Montefiore, D.; James, R.; Meadows, H.; Wan, S.; Jitlal, M.; Ledermann, J. Chemoradiation for the treatment of epidermoid anal cancer: 13-year follow-up of the first randomised UKCCCR Anal Cancer Trial (ACT I). Br. J. Cancer 2010, 102, 1123–1128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Garrido-Laguna, I.; et al. NCCN Clinical Practice Guidelines in Oncology: Anal Carcinoma. Version 2. 2020. Available online: https://www.nccn.org/professionals/physician_gls/pdf/anal.pdf (accessed on 24 July 2020).
- Gunderson, L.L.; Winter, K.A.; Ajani, J.A.; Pedersen, J.E.; Moughan, J.; Benson, A.B., 3rd; Thomas, C.R., Jr.; Mayer, R.J.; Haddock, M.G.; Rich, T.A.; et al. Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: Survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J. Clin. Oncol. 2012, 30, 4344–4351. [Google Scholar] [CrossRef]
- Flam, M.; John, M.; Pajak, T.F.; Petrelli, N.; Myerson, R.; Doggett, S.; Quivey, J.; Rotman, M.; Kerman, H.; Coia, L.; et al. Role of mitomycin in combination with fluorouracil and radiotherapy, and of salvage chemoradiation in the definitive nonsurgical treatment of epidermoid carcinoma of the anal canal: Results of a phase III randomized intergroup study. J. Clin. Oncol. 1996, 14, 2527–2539. [Google Scholar] [CrossRef] [PubMed]
- James, R.D.; Glynne-Jones, R.; Meadows, H.M.; Cunningham, D.; Myint, A.S.; Saunders, M.P.; Maughan, T.; McDonald, A.; Essapen, S.; Leslie, M.; et al. Mitomycin or cisplatin chemoradiation with or without maintenance chemotherapy for treatment of squamous-cell carcinoma of the anus (ACT II): A randomised, phase 3, open-label, 2 x 2 factorial trial. Lancet Oncol. 2013, 14, 516–524. [Google Scholar] [CrossRef]
- Northover, J.; Meadows, H.; Ryan, C.; Gray, R. Combined radiotherapy and chemotherapy for anal cancer-Reply. Lancet 1997, 349, 205–206. [Google Scholar] [CrossRef]
- Ortholan, C.; Ramaioli, A.; Peiffert, D.; Lusinchi, A.; Romestaing, P.; Chauveinc, L.; Touboul, E.; Peignaux, K.; Bruna, A.; de La Roche, G.; et al. Anal canal carcinoma: Early-stage tumors < or =10 mm (T1 or Tis): Therapeutic options and original pattern of local failure after radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2005, 62, 479–485. [Google Scholar] [CrossRef]
- Youssef, I.; Osborn, V.; Lee, A.; Katsoulakis, E.; Kavi, A.; Choi, K.; Safdieh, J.; Schreiber, D. Survival benefits and predictors of use of chemoradiation compared with radiation alone for early stage (T1-T2N0) anal squamous cell carcinoma. J. Gastrointest. Oncol. 2019, 10, 616–622. [Google Scholar] [CrossRef]
- Zilli, T.; Schick, U.; Ozsahin, M.; Gervaz, P.; Roth, A.D.; Allal, A.S. Node-negative T1-T2 anal cancer: Radiotherapy alone or concomitant chemoradiotherapy? Radiother. Oncol. 2012, 102, 62–67. [Google Scholar] [CrossRef]
- Chai, C.Y.; Tran Cao, H.S.; Awad, S.; Massarweh, N.N. Management of Stage I Squamous Cell Carcinoma of the Anal Canal. JAMA Surg. 2018, 153, 209–215. [Google Scholar] [CrossRef]
- Chakrabarti, S.; Jin, Z.; Huffman, B.M.; Yadav, S.; Graham, R.P.; Lam-Himlin, D.M.; Lightner, A.L.; Hallemeier, C.L.; Mahipal, A. Local excision for patients with stage I anal canal squamous cell carcinoma can be curative. J. Gastrointest. Oncol. 2019, 10, 171–178. [Google Scholar] [CrossRef]
- Kole, A.J.; Stahl, J.M.; Park, H.S.; Khan, S.A.; Johung, K.L. Predictors of Nonadherence to NCCN Guideline Recommendations for the Management of Stage I Anal Canal Cancer. J. Natl. Compr. Cancer Netw. 2017, 15, 355–362. [Google Scholar] [CrossRef] [Green Version]
- Han, K.; Cummings, B.J.; Lindsay, P.; Skliarenko, J.; Craig, T.; Le, L.W.; Brierley, J.; Wong, R.; Dinniwell, R.; Bayley, A.J.; et al. Prospective evaluation of acute toxicity and quality of life after IMRT and concurrent chemotherapy for anal canal and perianal cancer. Int. J. Radiat. Oncol. Biol. Phys. 2014, 90, 587–594. [Google Scholar] [CrossRef]
- Bentzen, A.G.; Balteskard, L.; Wanderas, E.H.; Frykholm, G.; Wilsgaard, T.; Dahl, O.; Guren, M.G. Impaired health-related quality of life after chemoradiotherapy for anal cancer: Late effects in a national cohort of 128 survivors. Acta Oncol. 2013, 52, 736–744. [Google Scholar] [CrossRef] [Green Version]
- Das, P.; Cantor, S.B.; Parker, C.L.; Zampieri, J.B.; Baschnagel, A.; Eng, C.; Delclos, M.E.; Krishnan, S.; Janjan, N.A.; Crane, C.H. Long-term quality of life after radiotherapy for the treatment of anal cancer. Cancer 2010, 116, 822–829. [Google Scholar] [CrossRef]
- Koerber, S.A.; Seither, B.; Slynko, A.; Haefner, M.F.; Krug, D.; Liermann, J.; Adeberg, S.; Herfarth, K.; Debus, J.; Sterzing, F. Chemoradiation in female patients with anal cancer: Patient-reported outcome of acute and chronic side effects. Tumori 2019, 105, 174–180. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.B.; Maeda, Y.; Wilson, A.; Glynne-Jones, R.; Vaizey, C.J. Late gastrointestinal toxicity after radiotherapy for anal cancer: A systematic literature review. Acta Oncol. 2018, 57, 1427–1437. [Google Scholar] [CrossRef]
- Franco, P.; Arcadipane, F.; Ragona, R.; Mistrangelo, M.; Cassoni, P.; Rondi, N.; Morino, M.; Racca, P.; Ricardi, U. Early-stage Node-negative (T1-T2N0) Anal Cancer Treated with Simultaneous Integrated Boost Radiotherapy and Concurrent Chemotherapy. Anticancer Res. 2016, 36, 1943–1948. [Google Scholar]
- White, E.C.; Goldman, K.; Aleshin, A.; Lien, W.W.; Rao, A.R. Chemoradiotherapy for squamous cell carcinoma of the anal canal: Comparison of one versus two cycles mitomycin-C. Radiother. Oncol. 2015, 117, 240–245. [Google Scholar] [CrossRef] [PubMed]
- Goodman, K.A.; Julie, D.; Cercek, A.; Cambridge, L.; Woo, K.M.; Zhang, Z.; Wu, A.J.; Reidy, D.L.; Segal, N.H.; Stadler, Z.K.; et al. Capecitabine With Mitomycin Reduces Acute Hematologic Toxicity and Treatment Delays in Patients Undergoing Definitive Chemoradiation Using Intensity Modulated Radiation Therapy for Anal Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 1087–1095. [Google Scholar] [CrossRef] [PubMed]
- Crowley, C.; Winship, A.Z.; Hawkins, M.A.; Morris, S.L.; Leslie, M.D. Size does matter: Can we reduce the radiotherapy field size for selected cases of anal canal cancer undergoing chemoradiation? Clin. Oncol. 2009, 21, 376–379. [Google Scholar] [CrossRef]
- Kim, H.; Park, H.C.; Yu, J.I.; Choi, D.H.; Ahn, Y.C.; Kim, S.T.; Park, J.O.; Park, Y.S.; Kim, H.C. Can we omit prophylactic inguinal nodal irradiation in anal cancer patients? Radiat. Oncol. J. 2015, 33, 83–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Charnley, N.; Choudhury, A.; Chesser, P.; Cooper, R.A.; Sebag-Montefiore, D. Effective treatment of anal cancer in the elderly with low-dose chemoradiotherapy. Br. J. Cancer 2005, 92, 1221–1225. [Google Scholar] [CrossRef] [Green Version]
- Hatfield, P.; Cooper, R.; Sebag-Montefiore, D. Involved-field, low-dose chemoradiotherapy for early-stage anal carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 2008, 70, 419–424. [Google Scholar] [CrossRef]
- Smith, D.E.; Shah, K.H.; Rao, A.R.; Frost, D.B.; Latino, F.; Anderson, P.J.; Peddada, A.V.; Kagan, A.R. Cancer of the anal canal: Treatment with chemotherapy and low-dose radiation therapy. Radiology 1994, 191, 569–572. [Google Scholar] [CrossRef]
- Bilimoria, K.Y.; Stewart, A.K.; Winchester, D.P.; Ko, C.Y. The National Cancer Data Base: A powerful initiative to improve cancer care in the United States. Ann. Surg. Oncol. 2008, 15, 683–690. [Google Scholar] [CrossRef] [Green Version]
- Coca-Perraillon, M. Local and global optimal propensity score matching. In Proceedings of the SAS Global Forum 2007 Conference, Orlando, FL, USA, 16–19 April 2007. [Google Scholar]
- Rosenbaum, P.R.; Rubin, D.B. Constructing a Control-Group Using Multivariate Matched Sampling Methods That Incorporate the Propensity Score. Am. Stat. 1985, 39, 33–38. [Google Scholar] [CrossRef]
- Lanehart, R.E.; Rodriguez de Gil, P.; Kim, E.S.; Bellara, A.P.; Kromrey, J.D.; Lee, R.S. Propensity score analysis and assessment of propensity score approaches using SAS procedures. In Proceedings of the SAS Global Forum 2012 Conference, Orlando, FL, USA, 22–25 April 2012. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Chemoradiation (N = 3552), Number (%) | Radiation Therapy Alone (N = 287), Number (%) | p-Value |
|---|---|---|---|
| Age (years) | <0.001 | ||
| <50 | 642 (18.1) | 59 (20.6) | |
| 50–59 | 1196 (33.7) | 68 (23.7) | |
| 60–69 | 1013 (28.5) | 65 (22.6) | |
| ≥70 | 701 (19.7) | 95 (33.1) | |
| Gender | <0.001 | ||
| Female | 2522 (71.0) | 181 (63.1) | |
| Male | 1030 (29.0) | 106 (36.9) | |
| Race | 0.054 | ||
| White | 3229 (90.9) | 251 (87.5) | |
| Non–white | 323 (9.1) | 36 (12.5) | |
| Charlson–Deyo score | 0.164 | ||
| 0 | 2938 (82.7) | 232 (80.8) | |
| 1 2–3 | 403 (11.4) 211 (5.9) | 30 (10.5) 25 (8.7) | |
| Median income | 0.145 | ||
| ≥$46,000 | 1405 (39.6) | 101 (35.2) | |
| <$46,000 | 2147 (60.4) | 186 (64.8) | |
| Insurance Status | 0.775 | ||
| Insured | 3451 (97.2) | 278 (96.9) | |
| Uninsured | 101 (2.8) | 9 (3.1) | |
| Distance to facility, mi. | 23.5 (SD = 102.3) | 19.8 (SD = 38.5) | 0.550 |
| Facility type | 0.459 | ||
| Academic | 1004 (28.3) | 87 (30.3) | |
| Non–academic | 2548 (71.7) | 200 (69.7) | |
| Tumor Size | 0.009 | ||
| ≤1 cm | 821 (23.1) | 77 (26.8) | |
| >1–2 cm | 1914 (53.9) | 128 (44.6) | |
| Unknown size | 817 (23.0) | 82 (28.6) |
| RT Alone vs. CRT | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| Variable | OR | 95% CI | p-Value | OR | 95% CI | p-Value |
| Age (years) | ||||||
| <50 | 1.62 | 1.13–2.32 | 0.009 | 1.42 | 0.98–2.05 | 0.064 |
| 50–59 | Ref | Ref | Ref | Ref | Ref | Ref |
| 60–69 | 1.13 | 0.80–1.60 | 0.498 | 1.15 | 0.81–1.63 | 0.437 |
| ≥70 | 2.38 | 1.72–3.30 | <0.001 | 2.45 | 1.76–3.39 | <0.001 |
| Female vs. male | 0.70 | 0.54–0.90 | 0.005 | 0.76 | 0.58–0.98 | 0.036 |
| Charlson–Deyo score | ||||||
| 0 | Ref | Ref | Ref | Ref | Ref | Ref |
| 1 | 0.94 | 0.64–1.40 | 0.769 | 0.86 | 0.58–1.29 | 0.476 |
| 2–3 | 1.50 | 0.97–2.32 | 0.068 | 1.26 | 0.80–1.99 | 0.315 |
| White vs. non–white | 0.70 | 0.48–1.01 | 0.055 | 0.72 | 0.49–1.05 | 0.089 |
| Academic vs. non–academic | 1.10 | 0.85–1.44 | 0.460 | –––– | –––– | –––– |
| Uninsured vs. insured | 1.11 | 0.55–2.21 | 0.775 | –––– | –––– | –––– |
| Median income (<$46 K/yr vs. ≥$46 K/yr) | 1.21 | 0.94–1.55 | 0.146 | 1.15 | 0.89–1.49 | 0.276 |
| Tumor Size | ||||||
| ≤1 cm | Ref | Ref | Ref | Ref | Ref | Ref |
| 1–2 cm | 0.71 | 0.53–0.96 | 0.024 | 0.69 | 0.51–0.93 | 0.014 |
| Unknown | 1.07 | 0.77–1.48 | 0.683 | 1.01 | 0.72–1.40 | 0.975 |
| Distance (per mile) | 1.00 | 1.00–1.00 | 0.544 | –––– | –––– | –––– |
| Variable | Univariate Analysis | Multivariate Analysis | ||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| CRT vs. RT | 0.54 | 0.43–0.68 | <0.001 | 0.65 | 0.52–0.82 | <0.001 |
| Age (years) | ||||||
| <50 | 1.21 | 0.94–1.56 | 0.148 | 0.96 | 0.74–1.25 | 0.757 |
| 50–59 | Ref | Ref | Ref | Ref | Ref | Ref |
| 60–69 | 1.57 | 1.25–1.96 | <0.001 | 1.53 | 1.22–1.91 | <0.001 |
| ≥70 | 3.89 | 3.17–4.76 | <0.001 | 3.65 | 2.97–4.48 | <0.001 |
| Female vs. male | 0.65 | 0.55–0.75 | <0.001 | 0.69 | 0.59–0.81 | <0.001 |
| Charlson–Deyo score | ||||||
| 0 | Ref | Ref | Ref | Ref | Ref | Ref |
| 1 | 1.82 | 1.49–2.23 | <0.001 | 1.50 | 1.22–1.84 | <0.001 |
| 2–3 | 2.99 | 2.35–3.81 | <0.001 | 2.77 | 2.15–3.56 | <0.001 |
| White vs. non–white | 0.81 | 0.64–1.04 | 0.099 | 0.84 | 0.65–1.07 | 0.317 |
| Academic vs. non–academic | 0.82 | 0.69–0.98 | 0.025 | 0.85 | 0.72–1.02 | 0.065 |
| Uninsured vs. insured | 1.01 | 0.66–1.54 | 0.982 | –––– | –––– | –––– |
| Median income (<$46 K/yr vs. ≥$46 K/yr) | 1.41 | 1.21–1.66 | <0.001 | 1.27 | 1.08–1.50 | 0.003 |
| Tumor Size ≤1 cm 1–2 cm Unknown | Ref 0.96 1.29 | Ref 0.79–1.16 1.04–1.58 | Ref 0.669 0.018 | Ref 0.91 1.16 | Ref 0.75–1.10 0.95–1.43 | Ref 0.322 0.154 |
| Distance (per mile) | 1.00 | 1.00–1.00 | 0.471 | –––– | –––– | –––– |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miller, E.; Nalin, A.; Diaz Pardo, D.; Arnett, A.; Abushahin, L.; Husain, S.; Jin, N.; Williams, T.; Bazan, J. Stage I Squamous Cell Carcinoma of the Anus: Is Radiation Therapy Alone Sufficient Treatment? Cancers 2020, 12, 3248. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113248
Miller E, Nalin A, Diaz Pardo D, Arnett A, Abushahin L, Husain S, Jin N, Williams T, Bazan J. Stage I Squamous Cell Carcinoma of the Anus: Is Radiation Therapy Alone Sufficient Treatment? Cancers. 2020; 12(11):3248. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113248
Chicago/Turabian StyleMiller, Eric, Ansel Nalin, Dayssy Diaz Pardo, Andrea Arnett, Laith Abushahin, Syed Husain, Ning Jin, Terence Williams, and Jose Bazan. 2020. "Stage I Squamous Cell Carcinoma of the Anus: Is Radiation Therapy Alone Sufficient Treatment?" Cancers 12, no. 11: 3248. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113248