Effects of the Minimal Extrathyroidal Extension on Early Response Rates after (Adjuvant) Initial Radioactive Iodine Therapy in PTC Patients


Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
2.1. Group Analysis
2.1.1. Patient Characteristics
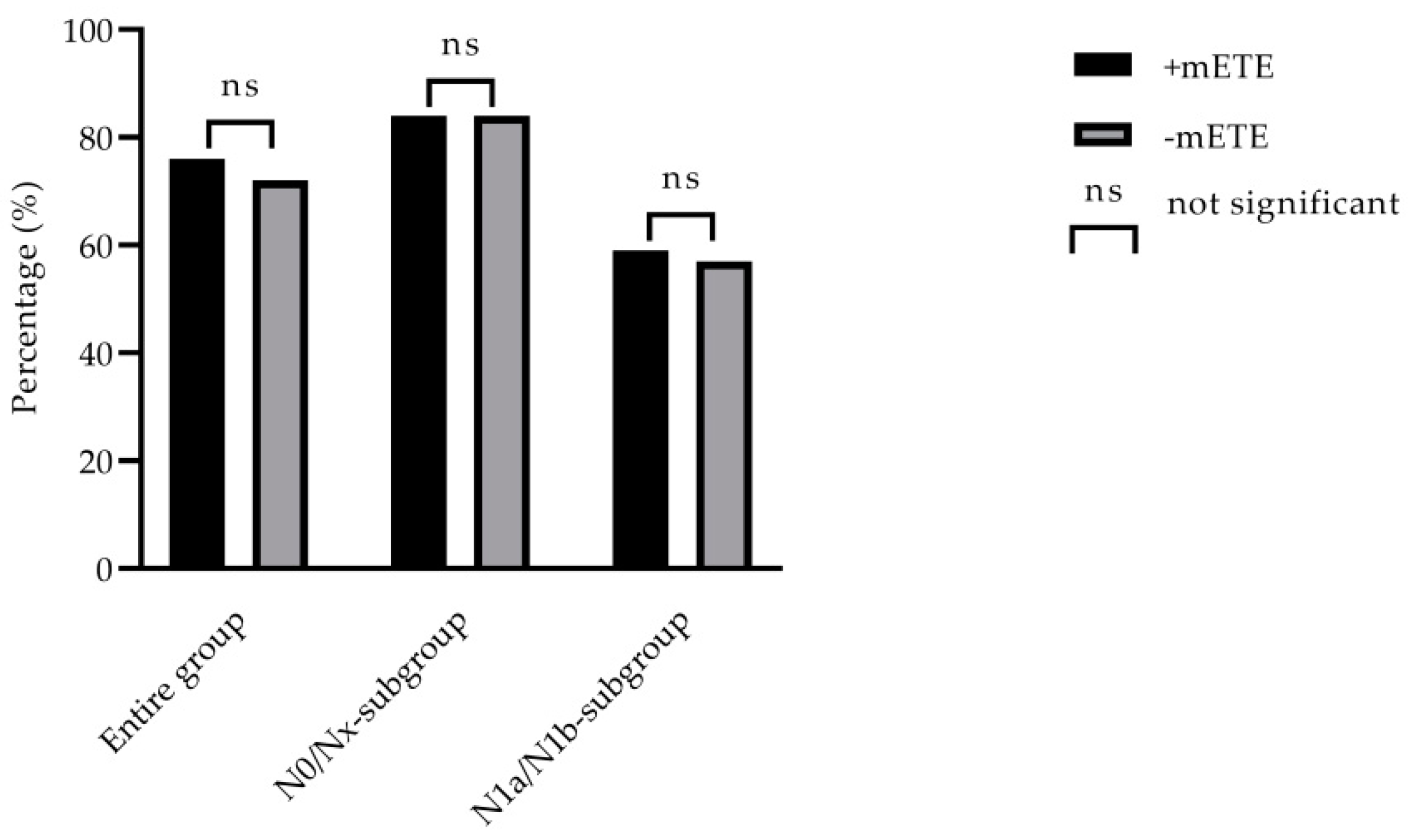
2.1.2. Outcome Analysis
2.2. Subgroup Analysis
2.2.1. N0/Nx-Subgroup Outcome Analysis
2.2.2. N1a/N1b-Subgroup Outcome Analysis
2.2.3. Uni- and Multivariate Analysis
3. Discussion
4. Materials and Methods
4.1. Study Population
4.2. Ethics Statement
4.3. Treatment
4.4. Follow-Up and Outcome
4.5. Subgroup Analysis
4.6. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Edge, S.B.; Compton, C.C. The American Joint Committee on Cancer: The 7th edition of the AJCC cancer staging manual and the future of TNM. Ann. Surg. Oncol. 2010, 17, 1471–1474. [Google Scholar] [CrossRef]
- Ito, Y.; Kudo, T.; Kobayashi, K.; Miya, A.; Ichihara, K.; Miyauchi, A. Prognostic factors for recurrence of papillary thyroid carcinoma in the lymph nodes, lung, and bone: Analysis of 5,768 patients with average 10-year follow-up. World J. Surg. 2012, 36, 1274–1278. [Google Scholar] [CrossRef] [PubMed]
- Verburg, F.A.; Mäder, U.; Tanase, K.; Thies, E.-D.; Diessl, S.; Buck, A.K.; Luster, M.; Reiners, C. Life expectancy is reduced in differentiated thyroid cancer patients >/= 45 years old with extensive local tumor invasion, lateral lymph node, or distant metastases at diagnosis and normal in all other DTC patients. J. Clin. Endocrinol. Metab. 2013, 98, 172–180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, P.E.; Kinsella, J.; Loree, T.R.; Shaha, A.R.; Shah, J.P. Differentiated carcinoma of the thyroid with extrathyroidal extension. Am. J. Surg. 1995, 170, 467–470. [Google Scholar] [CrossRef]
- Yin, D.-T.; Yu, K.; Lu, R.-Q.; Li, X.; Xu, J.; Lei, M. Prognostic impact of minimal extrathyroidal extension in papillary thyroid carcinoma. Medicine (Baltimore) 2016, 95, e5794. [Google Scholar] [CrossRef]
- Ito, Y.; Tomoda, C.; Uruno, T.; Takamura, Y.; Miya, A.; Kobayashi, K.; Matsuzuka, F.; Kuma, K.; Miyauchi, A. Prognostic significance of extrathyroid extension of papillary thyroid carcinoma: Massive but not minimal extension affects the relapse-free survival. World J. Surg. 2006, 30, 780–786. [Google Scholar] [CrossRef]
- Shin, J.H.; Haa, T.K.; Parka, H.K.; Ahna, M.S.; Kima, K.H.; Baea, K.B.; Kima, T.H.; Choia, C.S.; Kimb, T.K.; Baec, S.K.; et al. Implication of minimal extrathyroidal extension as a prognostic factor in papillary thyroid carcinoma. Int. J. Surg. 2013, 11, 944–947. [Google Scholar] [CrossRef] [Green Version]
- Al-Qurayshi, Z.; Shama, M.A.; Randolph, G.W.; Kandil, E. Minimal extrathyroidal extension does not affect survival of well-differentiated thyroid cancer. Endocr. Relat. Cancer 2017, 24, 221–226. [Google Scholar] [CrossRef]
- Arora, N.; Turbendian, H.K.; Scognamiglio, T.; Wagner, P.L.; Goldsmith, S.J.; Zarnegar, R.; Fahey, T.J. Extrathyroidal extension is not all equal: Implications of macroscopic versus microscopic extent in papillary thyroid carcinoma. Surgery 2008, 144, 942–947. [Google Scholar] [CrossRef]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The Eighth Edition AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more "personalized" approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perrier, N.D.; Brierley, J.D.; Tuttle, R.M. Differentiated and anaplastic thyroid carcinoma: Major changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J. Clin. 2018, 68, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kluijfhout, W.P.; Pasternak, J.D.; Kwon, J.S.; Lim, J.; Shen, W.T.; Gosnell, J.E.; Khanafshar, E.; Duh, Q.-Y.; Suh, I. Microscopic Positive Tumor Margin Does Not Increase the Risk of Recurrence in Patients with T1-T2 Well-Differentiated Thyroid Cancer. Ann. Surg. Oncol. 2016, 23, 1446–1451. [Google Scholar] [CrossRef] [PubMed]
- Woo, C.G.; Sung, C.O.; Choi, Y.M.; Kim, W.G.; Kim, T.Y.; Shong, Y.K.; Kim, W.B.; Hong, S.J.; Song, D.E. Clinicopathological Significance of Minimal Extrathyroid Extension in Solitary Papillary Thyroid Carcinomas. Ann. Surg. Oncol. 2015, 22 (Suppl. 3), S728–S733. [Google Scholar] [CrossRef] [Green Version]
- Radowsky, J.S.; Howard, R.S.; Burch, H.B.; Stojadinovic, A. Impact of degree of extrathyroidal extension of disease on papillary thyroid cancer outcome. Thyroid 2014, 24, 241–244. [Google Scholar] [CrossRef]
- Santos, M.J.; Bugalho, M.J. Papillary thyroid carcinoma: Different clinical behavior among pT3 tumors. Endocrine 2016, 53, 754–760. [Google Scholar] [CrossRef]
- Youngwirth, L.M.; Adam, M.A.; Scheri, R.P.; Roman, S.A.; Sosa, J.A. Extrathyroidal Extension Is Associated with Compromised Survival in Patients with Thyroid Cancer. Thyroid 2017, 27, 626–631. [Google Scholar] [CrossRef]
- Nixon, I.J.; Ganly, I.; Patel, S.; Palmer, F.L.; Whitcher, M.M.; Tuttle, R.M.; Shaha, A.R.; Shah, J.P. The impact of microscopic extrathyroid extension on outcome in patients with clinical T1 and T2 well-differentiated thyroid cancer. Surgery 2011, 150, 1242–1249. [Google Scholar] [CrossRef] [Green Version]
- Hay, I.D.; Johnson, T.R.; Thompson, G.B.; Sebo, T.J.; Reinalda, M.S. Minimal extrathyroid extension in papillary thyroid carcinoma does not result in increased rates of either cause-specific mortality or postoperative tumor recurrence. Surgery 2016, 159, 11–19. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.W.; Roh, J.-L.; Gong, G.; Cho, K.-J.; Choi, S.-H.; Nam, S.Y.; Kim, S.Y. Extent of Extrathyroidal Extension as a Significant Predictor of Nodal Metastasis and Extranodal Extension in Patients with Papillary Thyroid Carcinoma. Ann. Surg. Oncol. 2017, 24, 460–468. [Google Scholar] [CrossRef]
- Diker-Cohen, T.; Hirsch, D.; Shimon, I.; Bachar, G.; Akirov, A.; Duskin-Bitan, H.; Robenshtok, E. Impact of Minimal Extra-Thyroid Extension in Differentiated Thyroid Cancer: Systematic Review and Meta-analysis. J. Clin. Endocrinol. Metab. 2018. [Google Scholar] [CrossRef] [PubMed]
- Seo, M.; Kim, Y.S.; Lee, J.C.; Han, M.W.; Kim, E.S.; Kim, K.B.; Park, S.H. Low-Dose Radioactive Iodine Ablation Is Sufficient in Patients With Small Papillary Thyroid Cancer Having Minor Extrathyroidal Extension and Central Lymph Node Metastasis (T3 N1a). Clin. Nucl. Med. 2017, 42, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Hughes, C.J.; Shaha, A.R.; Shah, J.P.; Loree, T.R. Impact of lymph node metastasis in differentiated carcinoma of the thyroid: A matched-pair analysis. Head Neck. 1996, 18, 127–132. [Google Scholar] [CrossRef]
- Mallick, U.; Harmer, C.; Yap, B.; Wadsley, J.; Clarke, S.; Moss, L.; Nicol, A.; Clark, P.M.; Farnell, K.; McCready, R.; et al. Ablation with low-dose radioiodine and thyrotropin alfa in thyroid cancer. N. Engl. J. Med. 2012, 366, 1674–1685. [Google Scholar] [CrossRef] [Green Version]
- Schlumberger, M.; Catargi, B.; Borget, I.; Pharm, D.; Deandreis, D.; Zerdoud, S.; Bridji, B.; Bardet, S.; Leenhardt, L.; Bastie, D.; et al. Strategies of radioiodine ablation in patients with low-risk thyroid cancer. N. Engl. J. Med. 2012, 366, 1663–1673. [Google Scholar] [CrossRef] [Green Version]
- Henke, L.E.; Pfeifer, J.D.; Baranski, T.J.; DeWees, T.; Grigsby, P.W. Long-term outcomes of follicular variant vs. classic papillary thyroid carcinoma. Endocr. Connect. 2018, 7, 1226–1235. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.-M.; Schneider, D.F.; Leverson, G.; Chen, H.; Rebecca, S. Follicular variant of papillary thyroid carcinoma is a unique clinical entity: A population-based study of 10,740 cases. Thyroid 2013, 23, 1263–1268. [Google Scholar] [CrossRef] [Green Version]
- Robinson, T.J.; Thomas, S.; Dinan, M.A.; Roman, S.; Sosa, J.A.; Hyslop, T. How Many Lymph Nodes Are Enough? Assessing the Adequacy of Lymph Node Yield for Papillary Thyroid Cancer. J. Clin. Oncol. 2016, 34, 3434–3439. [Google Scholar] [CrossRef]
- Ruel, E.; Thomas, S.; Dinan, M.; Perkins, J.M.; Roman, S.A.; Sosa, J.A. Adjuvant radioactive iodine therapy is associated with improved survival for patients with intermediate-risk papillary thyroid cancer. J. Clin. Endocrinol. Metab. 2015, 100, 1529–1536. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| n = 455 (100%) | T1/2 +mETE n = 138 (30%) | T1/2 −mETE n = 317 (70%) | p Value |
|---|---|---|---|
| Patient characteristics | |||
| Age (years) | 57 ± 16 | 55 ± 14 | 0.054 ┼ |
| Female sex–no. (%) | 95 (69%) | 234 (74%) | 0.276 ╪ |
| Tumor size (mm) | 14.9 ± 8.4 | 14.4 ± 8.7 | 0.551 ┼ |
| Classical PTC | 103 (75%) | 197 (62%) | 0.010 ╪ |
| N1a/N1b-stage–no. (%) | 63 (46%) | 91 (29%) | 0.001 ╪ |
| Mean initial RAI activity (GBq) | 4.6 ± 2.1 | 3.3 ± 1.0 | 0.001 ┼ |
| Outcome analysis | |||
| Tg-level < 0.5 ng/mL after TSH-stimulation | 106 (77%) | 258 (81%) | 0.262 ╪ |
| No pathological uptake in WBS–no. (%) | 128 (93%) | 291 (92%) | 0.729 ╪ |
| Unremarkable neck ultrasonography | 134 (97%) | 313 (99%) | 0.241 ╪ |
| Responder rates–no. (%) | 100 (76%) | 242 (72%) | 0.379 ╪ |
| ╪ χ2 ┼ t-test | |||
| Outcome Parameters | N0/Nx n = 301 | p Value | N1a/1b n = 154 | p Value | ||
|---|---|---|---|---|---|---|
| +mETE n = 75 (25%) | −mETE n = 226 (75%) | +mETE n = 63 (41%) | −mETE n = 91 (59%) | |||
| Outcome analysis | ||||||
| Tg-level < 0.5 ng/mL after TSH-stimulation | 67 (89%) | 199 (88%) | 0.764 ╪ | 39 (62%) | 59 (65%) | 0.710 ╪ |
| No pathological uptake in WBS–no. (%) | 70 (93%) | 212 (94%) | 0.884 ╪ | 58 (92%) | 79 (87%) | 0.307 ╪ |
| Responder rates–no. (%) | 63 (84%) | 190 (84%) | 0.0.988 ╪ | 37 (59%) | 52 (57%) | 0.845 ╪ |
| ╪ χ2 ┼ t-test | ||||||
| Covariate | Level | Response Rate (Univariate Analysis) | Response Rate (Multivariate Analysis) | ||
|---|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | ||
| Gender | Female Male | Ref 10.675 (6.752–14.577) | 0.104 | ||
| Age (years) | <55 ≥55 | Ref 7.605 (7.220–7.989) | 0.006 | Ref 1.003 (0.995–1.012) | 0.405 |
| Histology | Classical PTC Follicular variant PTC | Ref 8.123 (7.451–8.796) | 0.746 | ||
| T-stage | T 1>T1 | Ref 8.837 (7.081–10.592) | 0.251 | ||
| N-stage | N0, Nx N1a, N1b | Ref 10.737 (6.917–14.557) | < 0.001 | Ref 0.716 (0.536–0.956) | 0.024 |
| mETE | −mETE +mETE | Ref 9.556 (6.757–12.355) | 0.256 | ||
| Mean initial RAI dose (GBq) | ≤3.7 ≥7.4 | Ref 14.028 (5.044–23.012) | 0.026 | Ref 0.915 (0.605–1.383) | 0.672 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahmaddy, F.; Wenter, V.; Ilhan, H.; Wacker, D.; Unterrainer, M.; Knösel, T.; Bartenstein, P.; Spitzweg, C.; Lehner, S.; Todica, A. Effects of the Minimal Extrathyroidal Extension on Early Response Rates after (Adjuvant) Initial Radioactive Iodine Therapy in PTC Patients. Cancers 2020, 12, 3357. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113357
Ahmaddy F, Wenter V, Ilhan H, Wacker D, Unterrainer M, Knösel T, Bartenstein P, Spitzweg C, Lehner S, Todica A. Effects of the Minimal Extrathyroidal Extension on Early Response Rates after (Adjuvant) Initial Radioactive Iodine Therapy in PTC Patients. Cancers. 2020; 12(11):3357. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113357
Chicago/Turabian StyleAhmaddy, Freba, Vera Wenter, Harun Ilhan, Daniel Wacker, Marcus Unterrainer, Thomas Knösel, Peter Bartenstein, Christine Spitzweg, Sebastian Lehner, and Andrei Todica. 2020. "Effects of the Minimal Extrathyroidal Extension on Early Response Rates after (Adjuvant) Initial Radioactive Iodine Therapy in PTC Patients" Cancers 12, no. 11: 3357. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers12113357