
HER2 Expression Is Predictive of Survival in Cetuximab Treated Patients with RAS Wild Type Metastatic Colorectal Cancer

 ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Immunohistochemistry
2.2. Scoring Criteria
2.3. Statistical Analysis
3. Results
3.1. Clinicopathological Features
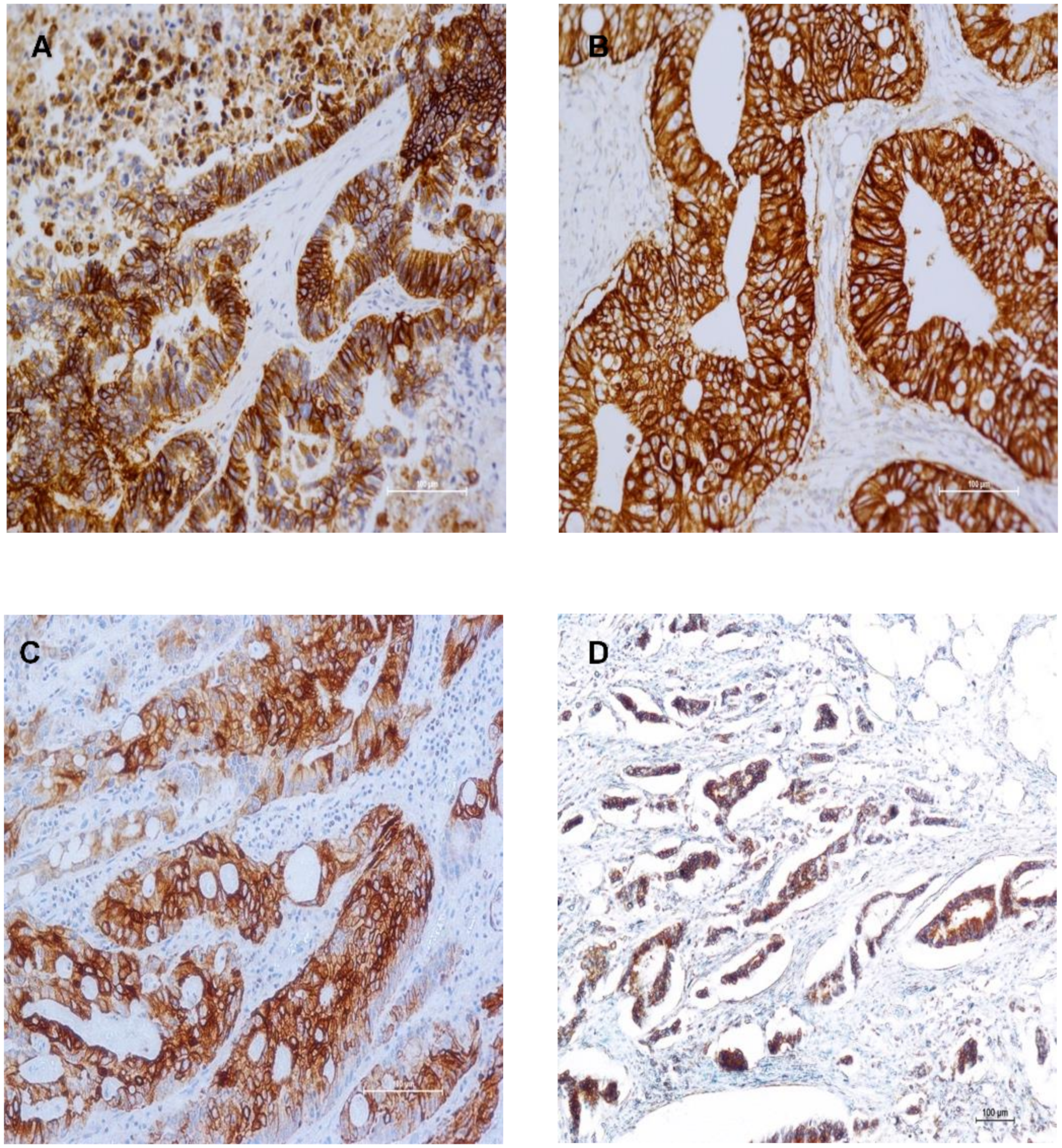
3.2. Immunohistochemical Expression of HER Family Members in Primary Tumours
3.3. HER Expression in Primary CRC and Their Corresponding Metastases
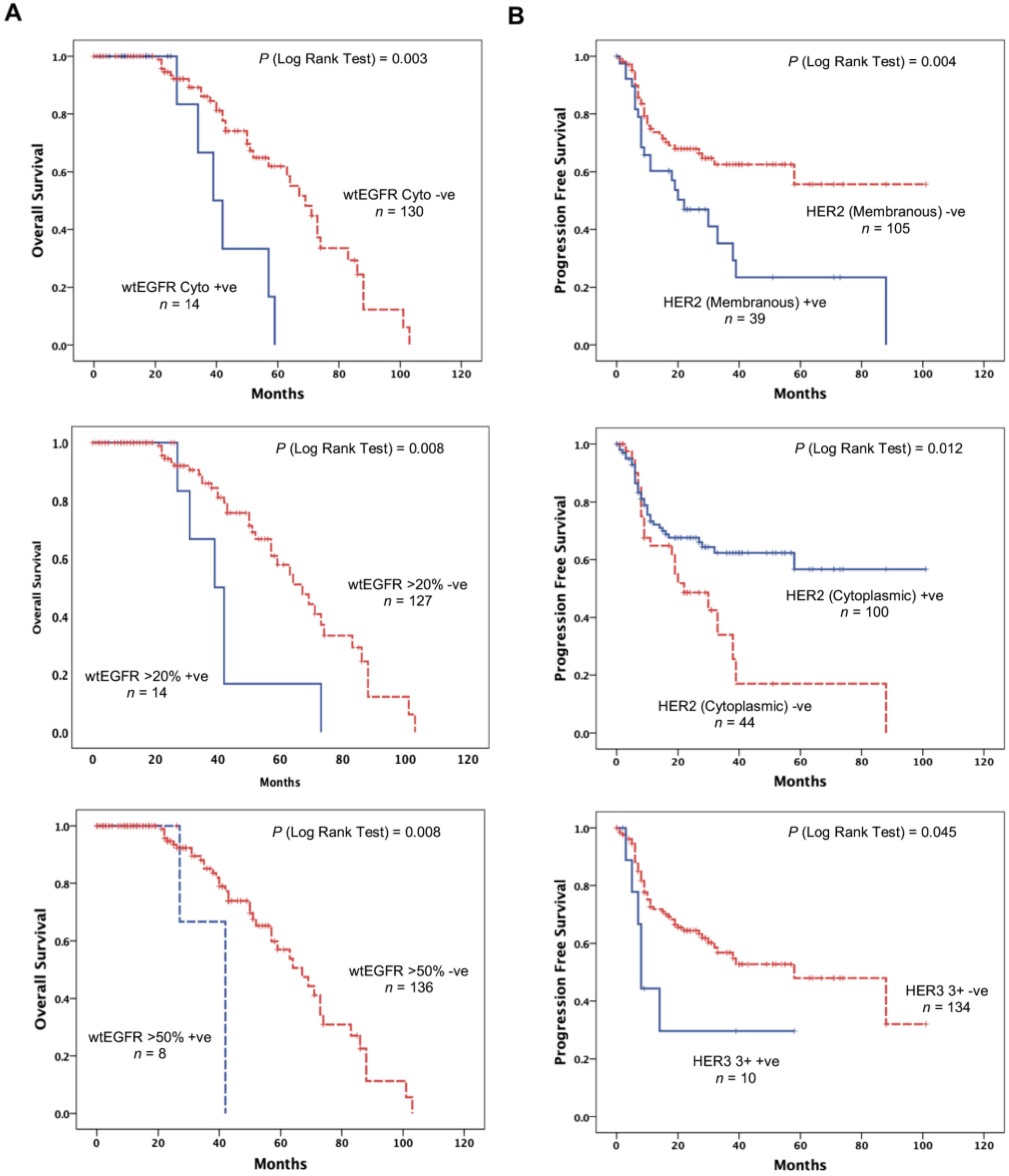
3.4. wtEGFR Expression is Significantly Associated with Adverse Overall Survival
3.5. HER2 and HER3 Expression Impacts Progression Free Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Arnold, D.; Seufferlein, T. Targeted treatments in colorectal cancer: State of the art and future perspectives. Gut 2010, 59, 838–858. [Google Scholar] [CrossRef]
- Khelwatty, S.A.; Essapen, S.; Seddon, A.M.; Modjtahedi, H. Prognostic significance and targeting of HER family in colorectal cancer. Front. Biosci. (Landmark Ed) 2013, 18, 394–421. [Google Scholar] [CrossRef] [Green Version]
- Wong, S.F. Cetuximab: An epidermal growth factor receptor monoclonal antibody for the treatment of colorectal cancer. Clin. Ther. 2005, 27, 684–694. [Google Scholar] [CrossRef]
- Shih, T.; Lindley, C. Bevacizumab: An angiogenesis inhibitor for the treatment of solid malignancies. Clin. Ther. 2006, 28, 1779–1802. [Google Scholar] [CrossRef]
- Wu, M.; Rivkin, A.; Pham, T. Panitumumab: Human monoclonal antibody against epidermal growth factor receptors for the treatment of metastatic colorectal cancer. Clin. Ther. 2008, 30, 14–30. [Google Scholar] [CrossRef]
- Tabernero, J.; Cohn, A.L.; Obermannova, R.; Bodoky, G.; Garcia-Carbonero, R.; Ciuleanu, T.-E.; Portnoy, D.C.; Cutsem, E.V.; Grothey, A.; Prausová, J.; et al. RAISE: A randomized, double-blind, multicenter phase III study of irinotecan, folinic acid, and 5-fluorouracil (FOLFIRI) plus ramucirumab (RAM) or placebo (PBO) in patients (pts) with metastatic colorectal carcinoma (CRC) progressive during or following first-line combination therapy with bevacizumab (bev), oxaliplatin (ox), and a fluoropyrimidine (fp). J. Clin. Oncol. 2015, 33, 512. [Google Scholar] [CrossRef]
- Golshani, G.; Zhang, Y. Advances in immunotherapy for colorectal cancer: A review. Ther. Adv. Gastroenterol. 2020, 13, 1756284820917527. [Google Scholar] [CrossRef]
- Akbarzadeh Khiavi, M.; Safary, A.; Somi, M.H. Recent advances in targeted therapy of colorectal cancer: Impacts of monoclonal antibodies nanoconjugates. Bioimpacts 2019, 9, 123–127. [Google Scholar] [CrossRef] [Green Version]
- Lievre, A.; Bachet, J.-B.; Le Corre, D.; Boige, V.; Landi, B.; Emile, J.-F.; Cote, J.-F.; Tomasic, G.; Penna, C.; Ducreux, M.; et al. KRAS Mutation Status Is Predictive of Response to Cetuximab Therapy in Colorectal Cancer. Cancer Res. 2006, 66, 3992–3995. [Google Scholar] [CrossRef] [Green Version]
- Bardelli, A.; Siena, S. Molecular Mechanisms of Resistance to Cetuximab and Panitumumab in Colorectal Cancer. J. Clin. Oncol 2010, 28, 1254–1261. [Google Scholar] [CrossRef]
- Boussios, S.; Ozturk, M.A.; Moschetta, M.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Katsanos, K.H.; Christodoulou, D.K.; Pavlidis, N. The Developing Story of Predictive Biomarkers in Colorectal Cancer. J. Pers. Med. 2019, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Chung, K.Y.; Shia, J.; Kemeny, N.E. Cetuximab shows activity in colorectal cancer patients with tumours that do not express the epidermal growth factor receptor by immunohistochemistry. J. Clin. Oncol 2005, 23, 1803–1810. [Google Scholar] [CrossRef]
- Allegra, C.J.; Rumble, R.B.; Hamilton, S.R.; Mangu, P.B.; Roach, N.; Hantel, A.; Schilsky, R.L. Extended RAS Gene Mutation Testing in Metastatic Colorectal Carcinoma to Predict Response to Anti-Epidermal Growth Factor Receptor Monoclonal Antibody Therapy: American Society of Clinical Oncology Provisional Clinical Opinion Update 2015. J. Clin. Oncol. 2016, 34, 179–185. [Google Scholar] [CrossRef]
- Amado, R.G.; Wolf, M.; Peeters, M.; Van Cutsem, E.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Radinsky, R.; et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef]
- Tol, J.; Koopman, M.; Cats, A.; Rodenburg, C.J.; Creemers, G.J.; Schrama, J.G.; Erdkamp, F.L.; Vos, A.H.; van Groeningen, C.J.; Sinnige, H.A.; et al. Chemotherapy, bevacizumab, and cetuximab in metastatic colorectal cancer. N. Engl. J. Med. 2009, 360, 563–572. [Google Scholar] [CrossRef] [Green Version]
- Stintzing, S.; Fischer von Weikersthal, L.; Decker, T.; Vehling-Kaiser, U.; Jager, E.; Heintges, T.; Stoll, C.; Giessen, C.; Modest, D.P.; Neumann, J.; et al. FOLFIRI plus cetuximab versus FOLFIRI plus bevacizumab as first-line treatment for patients with metastatic colorectal cancer-subgroup analysis of patients with KRAS: Mutated tumours in the randomised German AIO study KRK-0306. Ann. Oncol. Off. J. Eur. Soc.Med. Oncol./ESMO 2012, 23, 1693–1699. [Google Scholar] [CrossRef]
- Baretti, M.; Personeni, N.; Destro, A.; Santoro, A.; Rimassa, L. Emergence of KRAS-mutation in liver metastases after an anti-EGFR treatment in patient with colorectal cancer: Are we aware of the therapeutic impact of intratumor heterogeneity? Cancer Biol. Ther. 2018, 19, 659–663. [Google Scholar] [CrossRef]
- Baiocchi, G.; Lopes, A.; Coudry, R.A.; Rossi, B.M.; Soares, F.A.; Aguiar, S.; Guimaraes, G.C.; Ferreira, F.O.; Nakagawa, W.T. ErbB family immunohistochemical expression in colorectal cancer patients with higher risk of recurrence after radical surgery. Int. J. Colorectal Dis. 2009, 24, 1059–1068. [Google Scholar] [CrossRef]
- Khelwatty, S.A.; Essapen, S.; Bagwan, I.; Green, M.; Seddon, A.M.; Modjtahedi, H. Co-expression of HER family members in patients with Dukes’ C and D colon cancer and their impacts on patient prognosis and survival. PLoS ONE 2014, 9, e91139. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.C.; Wang, S.T.; Chow, N.H.; Yang, H.B. Investigation of the prognostic value of coexpressed erbB family members for the survival of colorectal cancer patients after curative surgery. Eur. J. Cancer 2002, 38, 1065–1071. [Google Scholar] [CrossRef]
- Ljuslinder, I.; Malmer, B.; Isaksson-Mettävainio, M.; Öberg, Å.; Henriksson, R.; Stenling, R.; Palmqvist, R. ErbB 1-4 expression alterations in primary colorectal cancers and their corresponding metastases. Anticancer Res. 2009, 29, 1489–1494. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Altman, D.G.; McShane, L.M.; Sauerbrei, W.; Taube, S.E. Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK): Explanation and elaboration. PLoS Med. 2012, 9, e1001216. [Google Scholar] [CrossRef] [Green Version]
- Khelwatty, S.; Essapen, S.; Bagwan, I.; Green, M.; Seddon, A.; Modjtahedi, H. The impact of co-expression of wild-type EGFR and its ligands determined by immunohistochemistry for response to treatment with cetuximab in patients with metastatic colorectal cancer. Oncotarget 2017, 8, 7666–7677. [Google Scholar] [CrossRef] [Green Version]
- Garnock-Jones, K.P. Necitumumab: First Global Approval. Drugs 2016, 76, 283–289. [Google Scholar] [CrossRef]
- Falzone, L.; Salomone, S.; Libra, M. Evolution of Cancer Pharmacological Treatments at the Turn of the Third Millennium. Front. Pharmacol 2018, 9, 1300. [Google Scholar] [CrossRef] [Green Version]
- Lieberman, R. Food and Drug Administration approval of cetuximab and a new KRAS genetic test for metastatic colorectal cancer: Major advance but just the tip of the biomarker iceberg. Am. J. Ther. 2012, 19, 395–396. [Google Scholar] [CrossRef]
- Ye, L.C.; Liu, T.S.; Ren, L.; Wei, Y.; Zhu, D.X.; Zai, S.Y.; Ye, Q.H.; Yu, Y.; Xu, B.; Qin, X.Y.; et al. Randomized controlled trial of cetuximab plus chemotherapy for patients with KRAS wild-type unresectable colorectal liver-limited metastases. J. Clin. Oncol 2013, 31, 1931–1938. [Google Scholar] [CrossRef] [Green Version]
- Chiorean, E.G.; Nandakumar, G.; Fadelu, T.; Temin, S.; Alarcon-Rozas, A.E.; Bejarano, S.; Croitoru, A.E.; Grover, S.; Lohar, P.V.; Odhiambo, A.; et al. Treatment of Patients With Late-Stage Colorectal Cancer: ASCO Resource-Stratified Guideline. JCO Glob. Oncol. 2020, 6, 414–438. [Google Scholar] [CrossRef]
- Cercek, A.; Braghiroli, M.I.; Chou, J.F.; Hechtman, J.F.; Kemeny, N.; Saltz, L.; Capanu, M.; Yaeger, R. Clinical Features and Outcomes of Patients with Colorectal Cancers Harboring NRAS Mutations. Clin. Cancer Res. 2017, 23, 4753–4760. [Google Scholar] [CrossRef] [Green Version]
- Khelwatty, S.A.; Essapen, S.; Bagwan, I.; Green, M.; Seddon, A.M.; Modjtahedi, H. Co-expression and prognostic significance of putative CSC markers CD44, CD133, wild-type EGFR and EGFRvIII in metastatic colorectal cancer. Oncotarget 2019, 10, 1704–1715. [Google Scholar] [CrossRef] [Green Version]
- Seo, Y.; Ishii, Y.; Ochiai, H.; Fukuda, K.; Akimoto, S.; Hayashida, T.; Okabayashi, K.; Tsuruta, M.; Hasegawa, H.; Kitagawa, Y. Cetuximab-mediated ADCC activity is correlated with the cell surface expression level of EGFR but not with the KRAS/BRAF mutational status in colorectal cancer. Oncol. Rep. 2014, 31, 2115–2122. [Google Scholar] [CrossRef] [Green Version]
- Sorkin, A.; Goh, L.K. Endocytosis and intracellular trafficking of ErbBs. Exp. Cell Res. 2009, 315, 683–696. [Google Scholar] [CrossRef] [Green Version]
- Madshus, I.H.; Stang, E. Internalization and intracellular sorting of the EGF receptor: A model for understanding the mechanisms of receptor trafficking. J. Cell Sci. 2009, 122, 3433–3439. [Google Scholar] [CrossRef] [Green Version]
- Khelwatty, S.A.; Essapen, S.; Seddon, A.M.; Fan, Z.; Modjtahedi, H. Acquired resistance to anti-EGFR mAb ICR62 in cancer cells is accompanied by an increased EGFR expression, HER2/HER3 signalling and sensitivity to pan HER blockers. Br. J. Cancer 2015, 113, 1010–1019. [Google Scholar] [CrossRef]
- Wang, G.; He, Y.; Sun, Y.; Wang, W.; Qian, X.; Yu, X.; Pan, Y. Prevalence, prognosis and predictive status of HER2 amplification in anti-EGFR-resistant metastatic colorectal cancer. Clin. Transl. Oncol. 2020, 22, 813–822. [Google Scholar] [CrossRef]
- Jeong, J.H.; Kim, J.; Hong, Y.S.; Kim, D.; Kim, J.E.; Kim, S.Y.; Kim, K.P.; Yoon, Y.K.; Kim, D.; Chun, S.M.; et al. HER2 Amplification and Cetuximab Efficacy in Patients With Metastatic Colorectal Cancer Harboring Wild-type RAS and BRAF. Clin. Colorectal Cancer 2017, 16, e147–e152. [Google Scholar] [CrossRef]
- Yao, Y.F.; Du, C.Z.; Chen, N.; Chen, P.; Gu, J. Expression of HER2 in rectal cancers treated with preoperative radiotherapy: A potential biomarker predictive of metastasis. Dis. Colon Rectum 2014, 57, 602–607. [Google Scholar] [CrossRef]
- Ciardiello, F.; Normanno, N. HER2 signaling and resistance to the anti-EGFR monoclonal antibody cetuximab: A further step toward personalized medicine for patients with colorectal cancer. Cancer Discov. 2011, 1, 472–474. [Google Scholar] [CrossRef] [Green Version]
- Essapen, S.; Thomas, H.; Green, M.; De Vries, C.; Cook, M.G.; Marks, C.; Topham, C.; Modjtahedi, H. The expression and prognostic significance of HER2 in colorectal cancer and its relationship with clinicopathological parameters. Int. J. Oncol. 2004, 24, 241–248. [Google Scholar] [PubMed]
- Ellebaek, S.; Brix, S.; Grandal, M.; Lantto, J.; Horak, I.D.; Kragh, M.; Poulsen, T.T. Pan-HER-An antibody mixture targeting EGFR, HER2 and HER3 abrogates preformed and ligand-induced EGFR homo- and heterodimers. Int. J. Cancer 2016, 139, 2095–2105. [Google Scholar] [CrossRef] [Green Version]
- Alimandi, M.; Romano, A.; Curia, M.C.; Muraro, R.; Fedi, P.; Aaronson, S.A.; Di Fiore, P.P.; Kraus, M.H. Cooperative signaling of ErbB3 and ErbB2 in neoplastic transformation and human mammary carcinomas. Oncogene 1995, 10, 1813–1821. [Google Scholar]
- Cleary, J.M.; McRee, A.J.; Shapiro, G.I.; Tolaney, S.M.; O’Neil, B.H.; Kearns, J.D.; Mathews, S.; Nering, R.; MacBeath, G.; Czibere, A.; et al. A phase 1 study combining the HER3 antibody seribantumab (MM-121) and cetuximab with and without irinotecan. Investig. New Drugs 2017, 35, 68–78. [Google Scholar] [CrossRef]
- Styczen, H.; Nagelmeier, I.; Beissbarth, T.; Nietert, M.; Homayounfar, K.; Sprenger, T.; Boczek, U.; Stanek, K.; Kitz, J.; Wolff, H.A.; et al. HER2 and HER3 expression in liver metastases of patients with colorectal cancer. Oncotarget 2015, 6, 15065–15076. [Google Scholar] [CrossRef] [Green Version]
- Marshall, J.; Shapiro, G.I.; Uttenreuther-Fischer, M.; Ould-Kaci, M.; Stopfer, P.; Gordon, M.S. Phase I dose-escalation study of afatinib, an ErbB family blocker, plus docetaxel in patients with advanced cancer. Future Oncol. 2013, 9, 271–281. [Google Scholar] [CrossRef]
- Siena, S.; Bartolomeo, M.D.; Raghav, K.P.S.; Masuishi, T.; Loupakis, F.; Kawakami, H.; Yamaguchi, K.; Nishina, T.; Fakih, M.; Elez, E.; et al. A phase II, multicenter, open-label study of trastuzumab deruxtecan (T-DXd; DS-8201) in patients (pts) with HER2-expressing metastatic colorectal cancer (mCRC): DESTINY-CRC01. J. Clin. Oncol. 2020, 38, 4000. [Google Scholar] [CrossRef]
- Desai, M.D.; Saroya, B.S.; Lockhart, A.C. Investigational therapies targeting the ErbB (EGFR, HER2, HER3, HER4) family in GI cancers. Expert Opin. Investig. Drugs 2013, 22, 341–356. [Google Scholar] [CrossRef]
- Kountourakis, P.; Pavlakis, K.; Psyrri, A.; Rontogianni, D.; Xiros, N.; Patsouris, E.; Pectasides, D.; Economopoulos, T. Prognostic significance of HER3 and HER4 protein expression in colorectal adenocarcinomas. BMC Cancer 2006, 6, 46. [Google Scholar] [CrossRef] [Green Version]
- Jia, X.; Wang, H.; Li, Z.; Yan, J.; Guo, Y.; Zhao, W.; Gao, L.; Wang, B.; Jia, Y. HER4 promotes the progression of colorectal cancer by promoting epithelialmesenchymal transition. Mol. Med. Rep. 2020, 21, 1779–1788. [Google Scholar] [CrossRef]
- Meropol, N.J. Epidermal growth factor receptor inhibitors in colorectal cancer: It’s time to get back on target. J. Clin. Oncol. 2005, 23, 1791–1793. [Google Scholar] [CrossRef]
- Modjtahedi, H.; Essapen, S. Epidermal growth factor receptor inhibitors in cancer treatment: Advances, challenges and opportunities. Anticancer Drugs 2009, 20, 851–855. [Google Scholar] [CrossRef]
- Bridgewater, J.A.; Pugh, S.A.; Maishman, T.; Eminton, Z.; Mellor, J.; Whitehead, A.; Stanton, L.; Radford, M.; Corkhill, A.; Griffiths, G.O.; et al. Systemic chemotherapy with or without cetuximab in patients with resectable colorectal liver metastasis (New EPOC): Long-term results of a multicentre, randomised, controlled, phase 3 trial. Lancet Oncol. 2020, 21, 398–411. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Number of Patients (%) | PFS in Months (Mean ± SE) | 95% CI | p-Value | OS in Months (Mean ± SE) | 95% CI | p-Value |
|---|---|---|---|---|---|---|---|
| Age in years | NS | NS | |||||
| ≤70 | 85 (59) | 53.7 ± 5.8 | 42.3–65.1 | 61.5 ± 4.6 | 52.5–70.6 | ||
| >70 | 59 (41) | 55.5 ± 5.6 | 44.4–66.5 | 67.6 ± 4.7 | 58.3–76.9 | ||
| Gender | NS | NS | |||||
| Male | 101 (70) | 47.1 ± 4.4 | 38.5–55.6 | 63.8 ± 3.2 | 57.4–70.1 | ||
| Female | 43 (30) | 71.9 ± 7.0 | 58.1–85.6 | 59.4 ± 6.6 | 46.4–72.4 | ||
| Tumour Type | NS | NS | |||||
| Resection | 76 (53) | 52.9 ± 6.0 | 41.2–64.6 | 63.2 ± 4.1 | 55.1–71.3 | ||
| Liver Metastasis | 11 (8) | 39.14 ± 8.7 | 22.4–56.1 | 64.1 ± 5.5 | 53.3–74.9 | ||
| Biopsy | 57 (39) | 48.4 ± 4.8 | 39.0–57.8 | 61.4 ± 6.5 | 48.5–74.2 | ||
| T stage * | NS | NS | |||||
| <T4 | 46 (32) | 51.2 ± 6.9 | 37.5–64.9 | 63.8 ± 4.9 | 54.2–73.4 | ||
| T4 | 33 (23) | 38.8 ± 4.2 | 30.6–47.0 | 61.7 ± 6.6 | 48.9–74.6 | ||
| N Stage * | NS | NS | |||||
| <N2 | 41 (29) | 50.5 ± 6.4 | 38.1–62.9 | 63.9 ± 4.3 | 55.6–72.3 | ||
| N2 | 38 (26) | 63.3 ± 7.8 | 48.0–78.5 | 65.1 ± 11.3 | 43.0–87.2 | ||
| M Stage * | NS | NS | |||||
| Mx/M0 | 70 (49) | 53.6 ± 6.1 | 41.5–65.6 | 64.7 ± 4.1 | 56.6–72.8 | ||
| M1 | 11 (8) | 25.8 ± 4.1 | 17.8–33.8 | 34.8 ± 3.0 | 28.9–40.7 | ||
| Vascular Invasion * | NS | NS | |||||
| V0 | 30 (21) | 49.7 ± 7.6 | 34.8–64.7 | 63.6 ± 5.7 | 52.3–74.8 | ||
| V1 | 49 (34) | 54.7 ± 7.1 | 40.8–68.7 | 65.5 ± 5.9 | 53.9–77.0 | ||
| LVI * | NS | NS | |||||
| Yes | 39 (27) | 55.5 ± 7.8 | 40.2–70.7 | 64.6 ± 4.9 | 54.8–74.4 | ||
| No | 39 (27) | 50.1 ± 6.7 | 37.1–63.2 | 63.6 ± 6.4 | 51.1–76.1 | ||
| Grade * | 0.022 | NS | |||||
| G1&G2 | 78 (54) | 61.3 ± 6.1 | 49.4–73.1 | 63.0 ± 4.1 | 54.9–71.1 | ||
| G3 | 32 (22) | 31.9 ± 6.4 | 19.4–44.6 | 57.7 ± 6.2 | 45.4–69.9 | ||
| Apical Node * | NS | NS | |||||
| Negative | 67 (47) | 53.4 ± 6.2 | 41.2–65.5 | 65.5 ± 4.1 | 56.4–72.7 | ||
| Positive | 12 (8) | 30.4 ± 4.4 | 21.9–38.9 | 36.7 ± 2.6 | 31.6–41.7 | ||
| Chemotherapy | NS | 0.007 | |||||
| FOLFOX + cetuximab | 25 (17) | 45.8 ± 5.9 | 34.2–57.6 | 47.6 ± 6.5 | 34.8–60.5 | ||
| FOLFIRI + cetuximAb | 78 (54) | 36.4 ± 3.7 | 29.1–43.6 | 65.5 ± 3.6 | 58.5–72.5 |
| Variables | No. of Positive Tumours (%) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| % Positive Tumour Cells | Intensity | Location | |||||||||
| >5 | >10 | >20 | >50 | 1+ | 2+ | 3+ | Mem | Cyto | Nuc | ||
| EGFR | 36 | 28 | 17 | 8 | 26 | 15 | 2 | 31 | 14 | - | |
| (25) | (19) | (12) | (6) | (18) | (10) | (1) | (22) | (10) | |||
| HER2 | 139 | 125 | 103 | 89 | 90 | 37 | 8 | 39 | 100 | - | |
| (97) | (87) | (72) | (62) | (63) | (26) | (6) | (27) | (69) | |||
| HER3 | 114 | 79 | 55 | 29 | 67 | 38 | 10 | 70 | 43 | - | |
| (79) | (55) | (38) | (20) | (47) | (26) | (7) | (49) | (30) | |||
| HER4 | 69 | 59 | 34 | 14 | 67 | 2 | 0 | 4 | 27 | 38 | |
| (48) | (41) | (24) | (10) | (47) | (1) | (0) | (3) | (19) | (26) | ||
| Co-expression of HER family (%) | |||||||||||
| EGFR | EGFR | EGFR | HER2 | HER2 | HER3 | EGFR | EGFR | EGFR | HER2 | EGFRHER2 | |
| HER2 | HER3 | HER4 | HER3 | HER4 | HER4 | HER2HER3 | HER2HER4 | HER3HER4 | HER3HER4 | HER3HER4 | |
| 34 | 29 | 17 | 109 | 68 | 57 | 27 | 15 | 18 | 56 | 15 | |
| (24) | (20) | (12) | (76) | (47) | (40) | (19) | (10) | (13) | (39) | (10) | |
| Case | Sex | Age | Type of Metastasis | wtEGFR 1° Met | HER2 1° Met | HER3 1° Met | HER4 1° Met | Overall Change in Expression | Response | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Female | 64 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | −ve | +ve | Yes | Yes |
| 2 | Female | 52 | Metachronous | +ve | −ve | −ve | −ve | +ve | −ve | −ve | +ve | Yes | Yes |
| 3 | Male | 52 | Synchronous | −ve | −ve | −ve | −ve | +ve | +ve | +ve | +ve | No | Yes |
| 4 | Male | 60 | Synchronous | +ve | +ve | +ve | −ve | +ve | +ve | +ve | −ve | Yes | No |
| 5 | Male | 88 | Metachronous | +ve | −ve | −ve | −ve | +ve | +ve | +ve | −ve | Yes | No |
| 6 | Male | 61 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | +ve | −ve | Yes | Yes |
| 7 | Female | 49 | Synchronous | −ve | +ve | −ve | +ve | +ve | +ve | +ve | +ve | Yes | No |
| 8 | Female | 69 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | +ve | +ve | No | No |
| 9 | Male | 65 | Metachronous | −ve | +ve | −ve | −ve | +ve | +ve | +ve | −ve | Yes | No |
| 10 | Female | 50 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | +ve | +ve | No | No |
| 11 | Male | 56 | Metachronous | +ve | −ve | −ve | −ve | +ve | +ve | +ve | −ve | Yes | Yes |
| 12 | Male | 70 | Synchronous | +ve | +ve | −ve | −ve | +ve | +ve | +ve | +ve | No | Yes |
| 13 | Female | 76 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | +ve | +ve | No | Yes |
| 14 | Male | 62 | Synchronous | +ve | −ve | +ve | −ve | +ve | +ve | −ve | +ve | Yes | Yes |
| 15 | Female | 58 | Metachronous | −ve | +ve | −ve | +ve | +ve | +ve | −ve | +ve | Yes | Yes |
| 16 | Male | 65 | Synchronous | +ve | +ve | −ve | −ve | +ve | +ve | +ve | +ve | No | Yes |
| 17 | Male | 69 | Metachronous | +ve | −ve | −ve | −ve | +ve | +ve | +ve | −ve | Yes | Yes |
| 18 | Male | 74 | Metachronous | −ve | −ve | −ve | −ve | +ve | +ve | −ve | +ve | Yes | Yes |
| 19 | Male | 69 | Metachronous | +ve | −ve | −ve | −ve | −ve | +ve | +ve | +ve | Yes | Yes |
| 20 | Male | 35 | Synchronous | −ve | −ve | −ve | −ve | +ve | −ve | +ve | +ve | Yes | No |
| 21 | Male | 34 | Metachronous | −ve | +ve | −ve | −ve | +ve | +ve | +ve | +ve | Yes | Yes |
| Variables | Progression Free Survival (PFS) | |||||
|---|---|---|---|---|---|---|
| Univariate | Multivariate | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| HER2 (Membranous) | 2.097 | 1.242–3.542 | 0.006 | 2.560 | 1.295–5.059 | 0.007 |
| HER2 (Cytoplasmic) | 0.518 | 0.305–0.879 | 0.015 | 0.367 | 0.185–0.728 | 0.004 |
| HER3 (3+) | 2.307 | 0.986–5.398 | 0.054 | - | - | NS |
| Overall Survival (OS) | ||||||
| Univariate | Multivariate | |||||
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| wtEGFR (Cytoplasmic) | 3.584 | 1.455–8.826 | 0.006 | 3.822 | 1.446–10.103 | 0.007 |
| wtEGFR (>20%) | 3.084 | 1.274–7.464 | 0.013 | 2.914 | 1.064–7.986 | 0.038 |
| wtEGFR (>50%) | 4.473 | 1.309–15.287 | 0.017 | 4.810 | 1.320–17.524 | 0.017 |
| HER2 | 0.213 | 0.62–0.734 | 0.014 | - | - | NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khelwatty, S.A.; Puvanenthiran, S.; Essapen, S.; Bagwan, I.; Seddon, A.M.; Modjtahedi, H. HER2 Expression Is Predictive of Survival in Cetuximab Treated Patients with RAS Wild Type Metastatic Colorectal Cancer. Cancers 2021, 13, 638. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040638
Khelwatty SA, Puvanenthiran S, Essapen S, Bagwan I, Seddon AM, Modjtahedi H. HER2 Expression Is Predictive of Survival in Cetuximab Treated Patients with RAS Wild Type Metastatic Colorectal Cancer. Cancers. 2021; 13(4):638. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040638
Chicago/Turabian StyleKhelwatty, Said A., Soozana Puvanenthiran, Sharadah Essapen, Izhar Bagwan, Alan M. Seddon, and Helmout Modjtahedi. 2021. "HER2 Expression Is Predictive of Survival in Cetuximab Treated Patients with RAS Wild Type Metastatic Colorectal Cancer" Cancers 13, no. 4: 638. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040638