
Stereotactic Body Radiotherapy for High-Risk Prostate Cancer: A Systematic Review

 , , , , , ,
, , , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
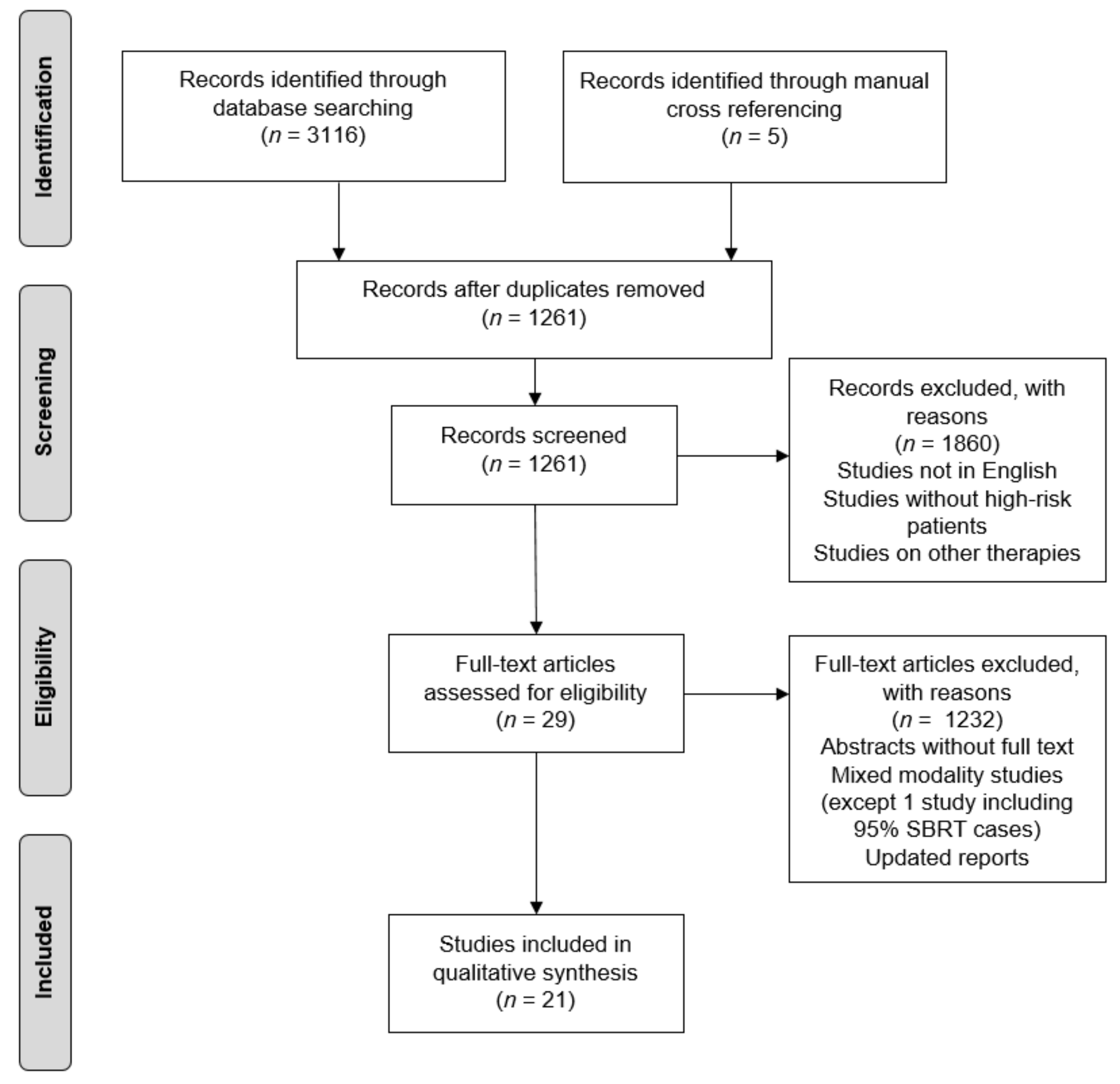
2.1. Selected Studies
2.2. Target Volume and Prescription Dose
2.2.1. Studies with Pelvic Lymph Node Irradiation
2.2.2. Studies without Pelvic Lymph Node Irradiation
2.3. Acute and Late Toxicity Rates
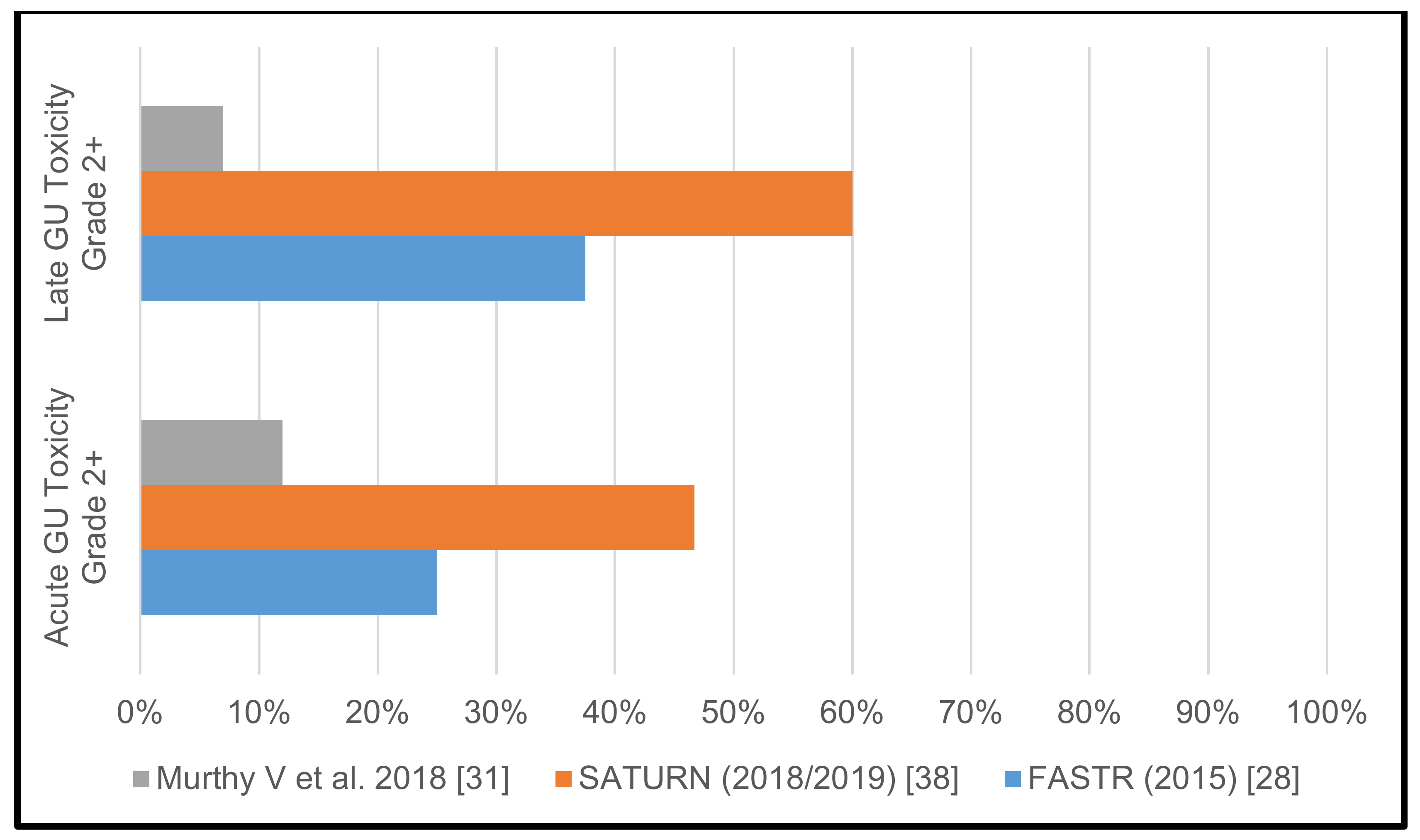
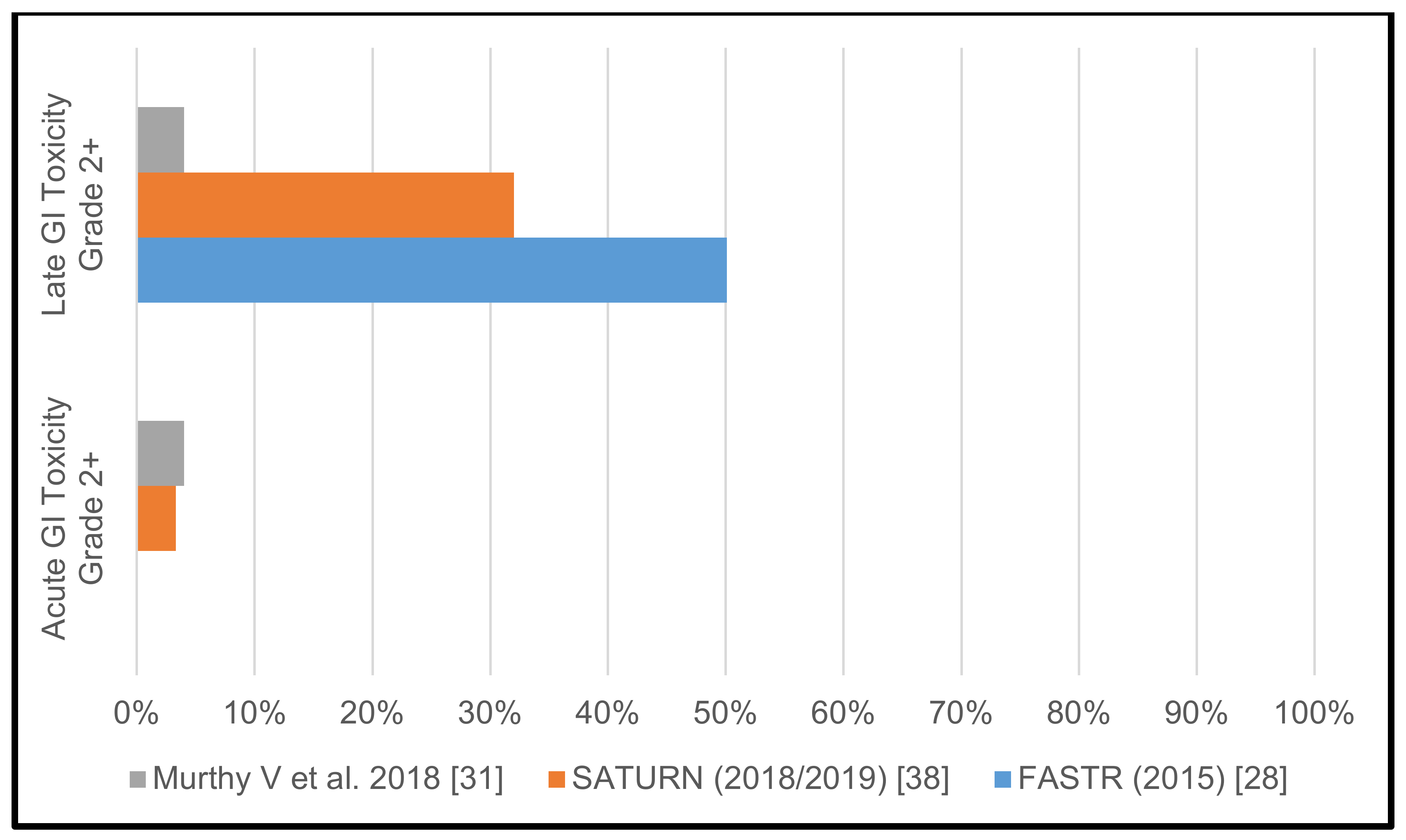
2.3.1. Studies with Pelvic Lymph Node Irradiation
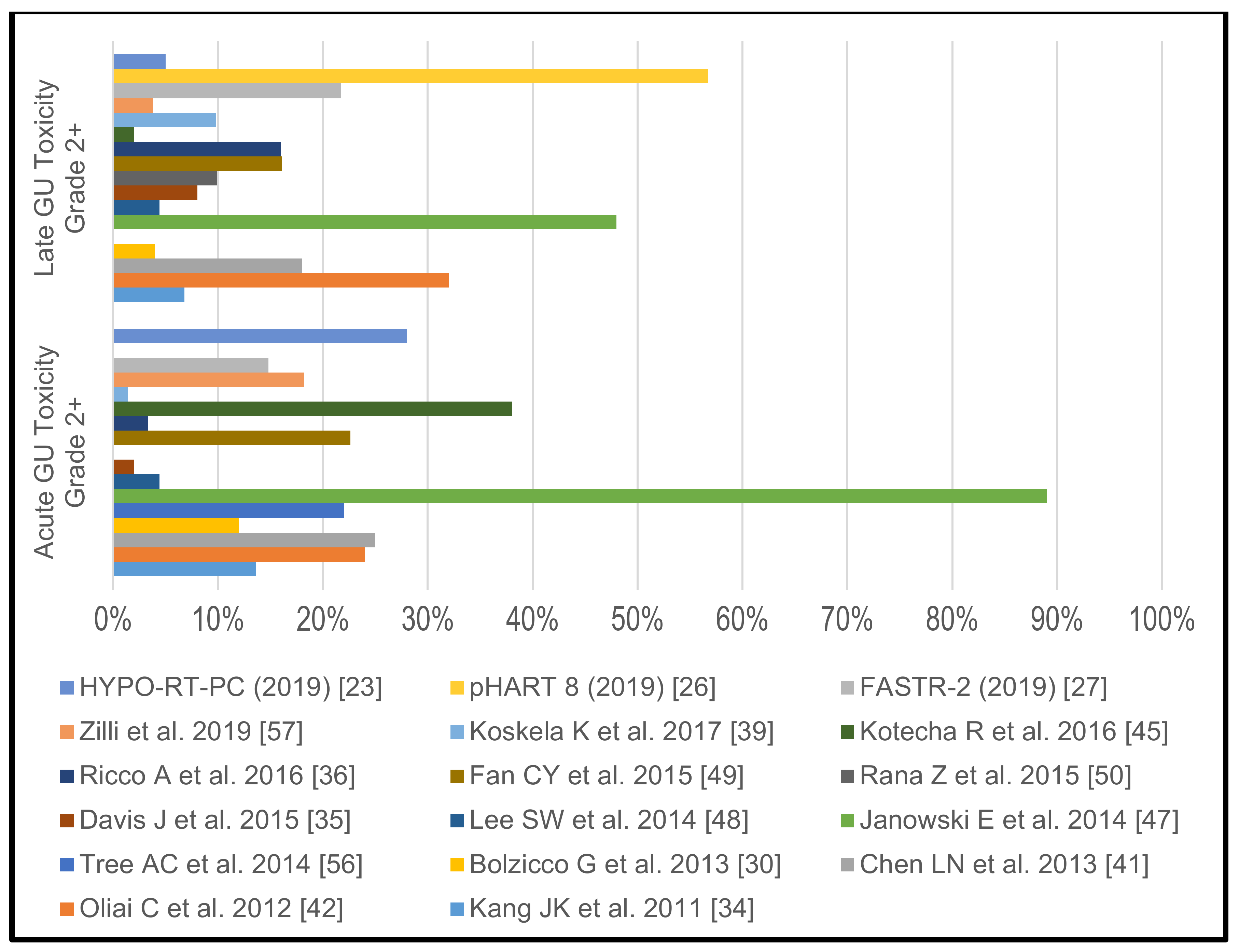
2.3.2. Studies without Pelvic Lymph Node Irradiation
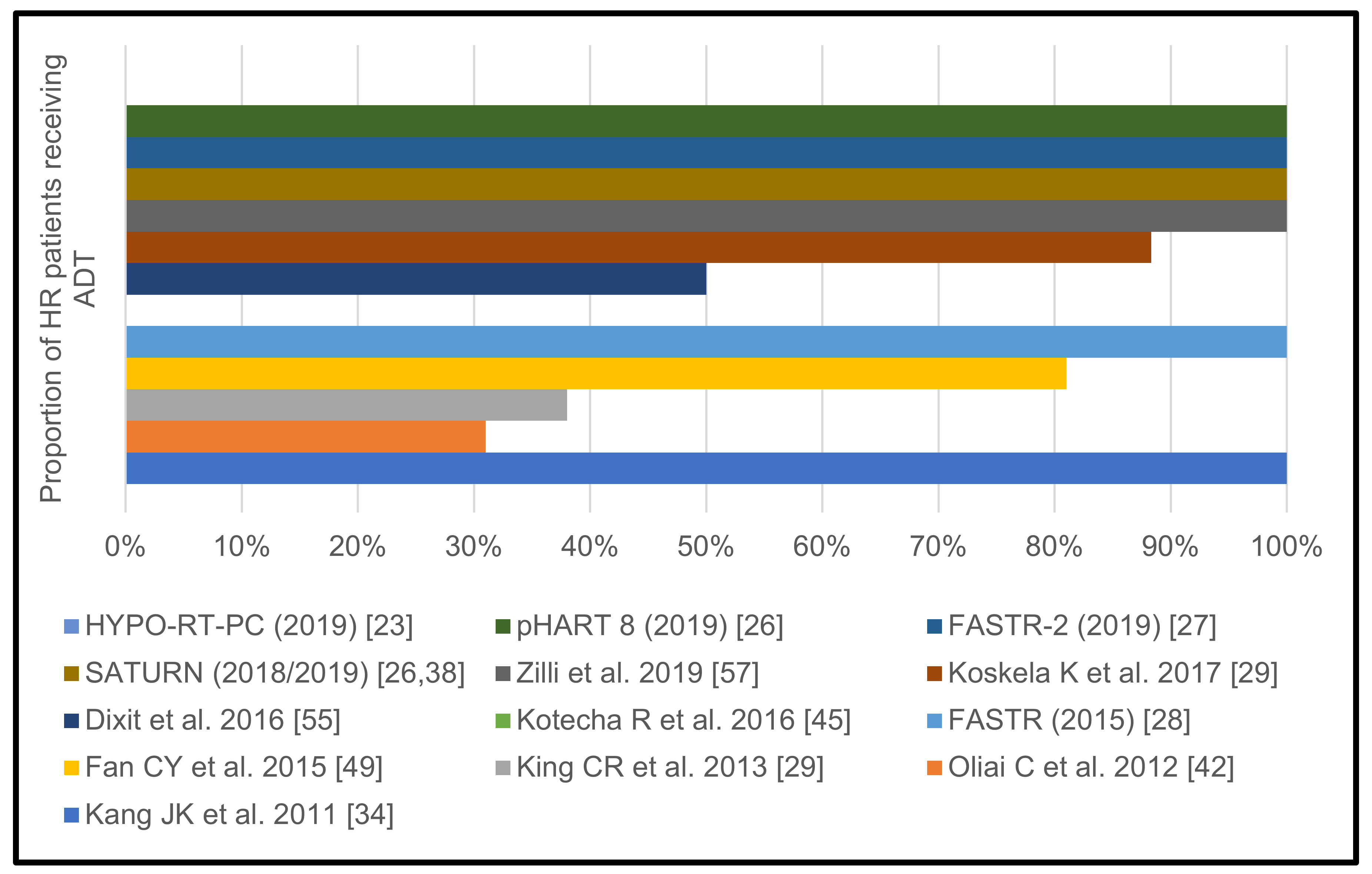
2.4. Androgen Deprivation Therapy
2.4.1. Studies with Pelvic Lymph Node Irradiation
2.4.2. Studies without Pelvic Lymph Node Irradiation
2.5. Biochemical Control
2.5.1. Studies with Pelvic Lymph Node Irradiation
2.5.2. Studies without Pelvic Lymph Node Irradiation
3. Discussion
4. Materials and Methods
4.1. Study Search and Selection Process
4.2. Data Extraction Process
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rawla, P. Epidemiology of Prostate Cancer. World J. Oncol. 2019, 10, 63–89. [Google Scholar] [CrossRef] [Green Version]
- Warde, P.; Mason, M.; Ding, K.; Kirkbride, P.; Brundage, M.; Cowan, R.; Gospodarowicz, M.; Sanders, K.; Kostashuk, E.; Swanson, G.; et al. Combined androgen deprivation therapy and radiation therapy for locally advanced prostate cancer: A randomised, phase 3 trial. Lancet 2011, 378, 2104–2111. [Google Scholar] [CrossRef] [Green Version]
- Bolla, M.; Van Tienhoven, G.; Warde, P.; Dubois, J.B.; Mirimanoff, R.O.; Storme, G.; Bernier, J.; Kuten, A.; Sternberg, C.; Billiet, I.; et al. External irradiation with or without long-term androgen suppression for prostate cancer with high metastatic risk: 10-year results of an EORTC randomised study. Lancet Oncol. 2010, 11, 1066–1073. [Google Scholar] [CrossRef]
- Widmark, A.; Klepp, O.; Solberg, A.; Damber, J.E.; Angelsen, A.; Fransson, P.; Lund, J.A.; Tasdemir, I.; Hoyer, M.; Wiklund, F.; et al. Endocrine treatment, with or without radiotherapy, in locally advanced prostate cancer (SPCG-7/SFUO-3): An open randomised phase III trial. Lancet 2009, 373, 301–308. [Google Scholar] [CrossRef] [Green Version]
- Shipley, W.U.; Verhey, L.J.; Munzenrider, J.E.; Suit, H.D.; Urie, M.M.; McManus, P.L.; Young, R.H.; Shipley, J.W.; Zietman, A.L.; Biggs, P.J.; et al. Advanced prostate cancer: The results of a randomized comparative trial of high dose irradiation boosting with conformal protons compared with conventional dose irradiation using photons alone. Int. J. Radiat. Oncol. Biol. Phys. 1995, 32, 3–12. [Google Scholar] [CrossRef]
- Zietman, A.L.; DeSilvio, M.L.; Slater, J.D.; Rossi, C.J., Jr.; Miller, D.W.; Adams, J.A.; Shipley, W.U. Comparison of conventional-dose vs high-dose conformal radiation therapy in clinically localized adenocarcinoma of the prostate: A randomized controlled trial. JAMA 2005, 294, 1233–1239. [Google Scholar] [CrossRef] [PubMed]
- Heemsbergen, W.D.; Al-Mamgani, A.; Slot, A.; Dielwart, M.F.; Lebesque, J.V. Long-term results of the Dutch randomized prostate cancer trial: Impact of dose-escalation on local, biochemical, clinical failure, and survival. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2014, 110, 104–109. [Google Scholar] [CrossRef]
- Peeters, S.T.; Heemsbergen, W.D.; Koper, P.C.; van Putten, W.L.; Slot, A.; Dielwart, M.F.; Bonfrer, J.M.; Incrocci, L.; Lebesque, J.V. Dose-response in radiotherapy for localized prostate cancer: Results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J. Clin. Oncol. 2006, 24, 1990–1996. [Google Scholar] [CrossRef] [PubMed]
- Dearnaley, D.P.; Sydes, M.R.; Graham, J.D.; Aird, E.G.; Bottomley, D.; Cowan, R.A.; Huddart, R.A.; Jose, C.C.; Matthews, J.H.; Millar, J.; et al. Escalated-dose versus standard-dose conformal radiotherapy in prostate cancer: First results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2007, 8, 475–487. [Google Scholar] [CrossRef]
- Morris, W.J.; Tyldesley, S.; Rodda, S.; Halperin, R.; Pai, H.; McKenzie, M.; Duncan, G.; Morton, G.; Hamm, J.; Murray, N. Androgen Suppression Combined with Elective Nodal and Dose Escalated Radiation Therapy (the ASCENDE-RT Trial): An Analysis of Survival Endpoints for a Randomized Trial Comparing a Low-Dose-Rate Brachytherapy Boost to a Dose-Escalated External Beam Boost for High- and Intermediate-risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2017, 98, 275–285. [Google Scholar] [CrossRef]
- Spratt, D.E.; Soni, P.D.; McLaughlin, P.W.; Merrick, G.S.; Stock, R.G.; Blasko, J.C.; Zelefsky, M.J. American Brachytherapy Society Task Group Report: Combination of brachytherapy and external beam radiation for high-risk prostate cancer. Brachytherapy 2017, 16, 1–12. [Google Scholar] [CrossRef]
- Hoskin, P.J.; Rojas, A.M.; Ostler, P.J.; Bryant, L.; Lowe, G.J. Randomised trial of external-beam radiotherapy alone or with high-dose-rate brachytherapy for prostate cancer: Mature 12-year results. Radiother. Oncol. 2020, 154, 214–219. [Google Scholar] [CrossRef] [PubMed]
- Benjamin, L.C.; Tree, A.C.; Dearnaley, D.P. The Role of Hypofractionated Radiotherapy in Prostate Cancer. Curr. Oncol. Rep. 2017, 19, 30. [Google Scholar] [CrossRef] [Green Version]
- Brenner, D.J.; Hall, E.J. Fractionation and protraction for radiotherapy of prostate carcinoma. Int. J. Radiat. Oncol. Biol. Phys. 1999, 43, 1095–1101. [Google Scholar] [CrossRef]
- Catton, C.N.; Lukka, H.; Gu, C.S.; Martin, J.M.; Supiot, S.; Chung, P.W.M.; Bauman, G.S.; Bahary, J.P.; Ahmed, S.; Cheung, P.; et al. Randomized Trial of a Hypofractionated Radiation Regimen for the Treatment of Localized Prostate Cancer. J. Clin. Oncol. 2017, 35, 1884–1890. [Google Scholar] [CrossRef]
- Dearnaley, D.; Syndikus, I.; Mossop, H.; Khoo, V.; Birtle, A.; Bloomfield, D.; Graham, J.; Kirkbride, P.; Logue, J.; Malik, Z.; et al. Conventional versus hypofractionated high-dose intensity-modulated radiotherapy for prostate cancer: 5-year outcomes of the randomised, non-inferiority, phase 3 CHHiP trial. Lancet Oncol. 2016, 17, 1047–1060. [Google Scholar] [CrossRef] [Green Version]
- Incrocci, L.; Wortel, R.C.; Alemayehu, W.G.; Aluwini, S.; Schimmel, E.; Krol, S.; van der Toorn, P.P.; Jager, H.; Heemsbergen, W.; Heijmen, B.; et al. Hypofractionated versus conventionally fractionated radiotherapy for patients with localised prostate cancer (HYPRO): Final efficacy results from a randomised, multicentre, open-label, phase 3 trial. Lancet Oncol. 2016, 17, 1061–1069. [Google Scholar] [CrossRef]
- Lee, W.R.; Dignam, J.J.; Amin, M.B.; Bruner, D.W.; Low, D.; Swanson, G.P.; Shah, A.B.; D’Souza, D.P.; Michalski, J.M.; Dayes, I.S.; et al. Randomized Phase III Noninferiority Study Comparing Two Radiotherapy Fractionation Schedules in Patients With Low-Risk Prostate Cancer. J. Clin. Oncol. 2016, 34, 2325–2332. [Google Scholar] [CrossRef] [PubMed]
- Guckenberger, M.; Baus, W.W.; Blanck, O.; Combs, S.E.; Debus, J.; Engenhart-Cabillic, R.; Gauer, T.; Grosu, A.L.; Schmitt, D.; Tanadini-Lang, S.; et al. Definition and quality requirements for stereotactic radiotherapy: Consensus statement from the DEGRO/DGMP Working Group Stereotactic Radiotherapy and Radiosurgery. Strahlenther. Onkol. 2020, 196, 417–420. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, D.; Blanck, O.; Gauer, T.; Fix, M.K.; Brunner, T.B.; Fleckenstein, J.; Loutfi-Krauss, B.; Manser, P.; Werner, R.; Wilhelm, M.L.; et al. Technological quality requirements for stereotactic radiotherapy: Expert review group consensus from the DGMP Working Group for Physics and Technology in Stereotactic Radiotherapy. Strahlenther. Onkol. 2020, 196, 421–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moraes, F.Y.d.; Siqueira, G.M.S.d.; Abreu, C.E.C.V.; da Silva, J.L.F.; Gadia, R. Hypofractioned radiotherapy in prostate cancer: Is it the next step? Expert Rev. Anticancer Ther. 2014, 14, 1271–1276. [Google Scholar] [CrossRef] [PubMed]
- Brand, D.H.; Tree, A.C.; Ostler, P.; van der Voet, H.; Loblaw, A.; Chu, W.; Ford, D.; Tolan, S.; Jain, S.; Martin, A.; et al. Intensity-modulated fractionated radiotherapy versus stereotactic body radiotherapy for prostate cancer (PACE-B): Acute toxicity findings from an international, randomised, open-label, phase 3, non-inferiority trial. Lancet Oncol. 2019, 20, 1531–1543. [Google Scholar] [CrossRef]
- Widmark, A.; Gunnlaugsson, A.; Beckman, L.; Thellenberg-Karlsson, C.; Hoyer, M.; Lagerlund, M.; Kindblom, J.; Ginman, C.; Johansson, B.; Bjornlinger, K.; et al. Ultra-hypofractionated versus conventionally fractionated radiotherapy for prostate cancer: 5-year outcomes of the HYPO-RT-PC randomised, non-inferiority, phase 3 trial. Lancet 2019, 394, 385–395. [Google Scholar] [CrossRef]
- Zilli, T.; Franzese, C.; Bottero, M.; Giaj-Levra, N.; Forster, R.; Zwahlen, D.; Koutsouvelis, N.; Bertaut, A.; Blanc, J.; Roberto D’agostino, G.; et al. Single fraction urethra-sparing prostate cancer SBRT: Phase I results of the ONE SHOT trial. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2019, 139, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Jackson, W.C.; Silva, J.; Hartman, H.E.; Dess, R.T.; Kishan, A.U.; Beeler, W.H.; Gharzai, L.A.; Jaworski, E.M.; Mehra, R.; Hearn, J.W.D.; et al. Stereotactic Body Radiation Therapy for Localized Prostate Cancer: A Systematic Review and Meta-Analysis of Over 6,000 Patients Treated On Prospective Studies. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 778–789. [Google Scholar] [CrossRef] [Green Version]
- Alayed, Y.; Cheung, P.; Vesprini, D.; Liu, S.; Chu, W.; Chung, H.; Musunuru, H.B.; Davidson, M.; Ravi, A.; Ho, L.; et al. SABR in High-Risk Prostate Cancer: Outcomes From 2 Prospective Clinical Trials With and Without Elective Nodal Irradiation. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 36–41. [Google Scholar] [CrossRef] [Green Version]
- Callan, L.; Bauman, G.; Chen, J.; Lock, M.; Sexton, T.; D’Souza, D.; Rodrigues, G. A Phase I/II Trial of Fairly Brief Androgen Suppression and Stereotactic Radiation Therapy for High-Risk Prostate Cancer (FASTR-2): Preliminary Results and Toxicity Analysis. Adv. Radiat. Oncol. 2019, 4, 668–673. [Google Scholar] [CrossRef] [Green Version]
- Bauman, G.; Ferguson, M.; Lock, M.; Chen, J.; Ahmad, B.; Venkatesan, V.M.; Sexton, T.; D’Souza, D.; Loblaw, A.; Warner, A.; et al. A Phase 1/2 Trial of Brief Androgen Suppression and Stereotactic Radiation Therapy (FASTR) for High-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 856–862. [Google Scholar] [CrossRef]
- King, C.R.; Freeman, D.; Kaplan, I.; Fuller, D.; Bolzicco, G.; Collins, S.; Meier, R.; Wang, J.; Kupelian, P.; Steinberg, M.; et al. Stereotactic body radiotherapy for localized prostate cancer: Pooled analysis from a multi-institutional consortium of prospective phase II trials. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2013, 109, 217–221. [Google Scholar] [CrossRef] [Green Version]
- Bolzicco, G.; Favretto, M.S.; Satariano, N.; Scremin, E.; Tambone, C.; Tasca, A. A single-center study of 100 consecutive patients with localized prostate cancer treated with stereotactic body radiotherapy. BMC Urol. 2013, 13, 49. [Google Scholar] [CrossRef] [Green Version]
- Murthy, V.; Gupta, M.; Mulye, G.; Maulik, S.; Munshi, M.; Krishnatry, R.; Phurailatpam, R.; Mhatre, R.; Prakash, G.; Bakshi, G. Early Results of Extreme Hypofractionation Using Stereotactic Body Radiation Therapy for High-risk, Very High-risk and Node-positive Prostate Cancer. Clin. Oncol. (R. Coll. Radiol.) 2018, 30, 442–447. [Google Scholar] [CrossRef]
- Katz, A.J.; Kang, J. Quality of Life and Toxicity after SBRT for Organ-Confined Prostate Cancer, a 7-Year Study. Front. Oncol. 2014, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, J.; Katz, A.J. Management of high-risk prostate cancer with 5-treatment stereotactic body radiotherapy: Long-term results. J. Clin. Oncol. 2017, 35, 94–94. [Google Scholar] [CrossRef]
- Kang, J.K.; Cho, C.K.; Choi, C.W.; Yoo, S.; Kim, M.S.; Yang, K.; Yoo, H.; Kim, J.H.; Seo, Y.S.; Lee, D.H.; et al. Image-guided stereotactic body radiation therapy for localized prostate cancer. Tumori 2011, 97, 43–48. [Google Scholar] [CrossRef]
- Davis, J.; Sharma, S.; Shumway, R.; Perry, D.; Bydder, S.; Simpson, C.K.; D’Ambrosio, D. Stereotactic Body Radiotherapy for Clinically Localized Prostate Cancer: Toxicity and Biochemical Disease-Free Outcomes from a Multi-Institutional Patient Registry. Cureus 2015, 7, e395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ricco, A.; Manahan, G.; Lanciano, R.; Hanlon, A.; Yang, J.; Arrigo, S.; Lamond, J.; Feng, J.; Mooreville, M.; Garber, B.; et al. The Comparison of Stereotactic Body Radiation Therapy and Intensity-Modulated Radiation Therapy for Prostate Cancer by NCCN Risk Groups. Front. Oncol. 2016, 6, 184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Katz, A.; Kang, J. Stereotactic Body Radiation Therapy for Localized Prostate Cancer: Risk Stratification for Intermediate- and High-Risk Patients. Int. J. Radiat. Oncol. Biol. Phys. 2016, 96, E250. [Google Scholar] [CrossRef] [Green Version]
- Musunuru, H.B.; D’Alimonte, L.; Davidson, M.; Ho, L.; Cheung, P.; Vesprini, D.; Liu, S.; Chu, W.; Chung, H.; Ravi, A.; et al. Phase 1-2 Study of Stereotactic Ablative Radiotherapy Including Regional Lymph Node Irradiation in Patients With High-Risk Prostate Cancer (SATURN): Early Toxicity and Quality of Life. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, 1438–1447. [Google Scholar] [CrossRef]
- Koskela, K.; Palmgren, J.E.; Heikkila, J.; Virsunen, H.; Sailas, L.; Auvinen, P.; Seppala, J.; Kataja, V. Hypofractionated stereotactic body radiotherapy for localized prostate cancer—first Nordic clinical experience. Acta Oncol. 2017, 56, 978–983. [Google Scholar] [CrossRef] [Green Version]
- Katz, A.; Kang, J. Stereotactic body radiotherapy with or without external beam radiation as treatment for organ confined high-risk prostate carcinoma: A six year study. Radiat. Oncol. 2014, 9, 1. [Google Scholar] [CrossRef] [Green Version]
- Chen, L.N.; Suy, S.; Uhm, S.; Oermann, E.K.; Ju, A.W.; Chen, V.; Hanscom, H.N.; Laing, S.; Kim, J.S.; Lei, S.; et al. Stereotactic body radiation therapy (SBRT) for clinically localized prostate cancer: The Georgetown University experience. Radiat. Oncol. 2013, 8, 58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oliai, C.; Lanciano, R.; Sprandio, B.; Yang, J.; Lamond, J.; Arrigo, S.; Good, M.; Mooreville, M.; Garber, B.; Brady, L.W. Stereotactic body radiation therapy for the primary treatment of localized prostate cancer. J. Radiat. Oncol. 2013, 2, 63–70. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Musunuru, H.B.; Cheung, P.; Loblaw, A. Evolution of hypofractionated accelerated radiotherapy for prostate cancer—the sunnybrook experience. Front. Oncol. 2014, 4, 313. [Google Scholar] [CrossRef] [Green Version]
- Kishan, A.U.; Fuller, D.B.; Steinberg, M.L.; Ramirez, V.; Ostendorf, E.; Tsai, S.H.; Agazaryan, N.; Ruan, D.; Cao, M.; Kupelian, P.A.; et al. Stereotactic Body Radiotherapy for High-Risk Prostate Cancer: Preliminary Toxicity Results of a Phase 2 Trial. Int. J. Radiat. Oncol. Biol. Phys. 2017, 99, E248. [Google Scholar] [CrossRef]
- Kotecha, R.; Djemil, T.; Tendulkar, R.D.; Reddy, C.A.; Thousand, R.A.; Vassil, A.; Stovsky, M.; Berglund, R.K.; Klein, E.A.; Stephans, K.L. Dose-Escalated Stereotactic Body Radiation Therapy for Patients with Intermediate- and High-Risk Prostate Cancer: Initial Dosimetry Analysis and Patient Outcomes. Int. J. Radiat. Oncol. Biol. Phys. 2016, 95, 960–964. [Google Scholar] [CrossRef] [PubMed]
- Pontoriero, A.; Iatì, G.; Mondello, S.; Midili, F.; Siragusa, C.; Brogna, A.; Ielo, I.; Anastasi, G.; Magno, C.; Pergolizzi, S.; et al. High-Dose Robotic Stereotactic Body Radiotherapy in the Treatment of Patients With Prostate Cancer: Preliminary Results in 26 Patients. Technol. Cancer Res. Treat. 2016, 15, 179–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janowski, E.; Chen, L.N.; Kim, J.S.; Lei, S.; Suy, S.; Collins, B.; Lynch, J.; Dritschilo, A.; Collins, S. Stereotactic body radiation therapy (SBRT) for prostate cancer in men with large prostates (≥50 cm3). Radiat. Oncol. 2014, 9, 241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.W.; Jang, H.S.; Lee, J.H.; Kim, S.H.; Yoon, S.C. Stereotactic body radiation therapy for prostate cancer patients with old age or medical comorbidity: A 5-year follow-up of an investigational study. Medicine 2014, 93, e290. [Google Scholar] [CrossRef]
- Fan, C.Y.; Chao, H.L.; Huang, W.Y.; Lin, C.S.; Chen, C.M.; Lo, C.H. Stereotactic ablative radiotherapy with CyberKnife in the treatment of locally advanced prostate cancer: Preliminary results. Tumori J. 2015, 101, 684–691. [Google Scholar] [CrossRef] [PubMed]
- Rana, Z.; Hong, R.L.; Abugideiri, M.; McRae, D.; Cernica, G.; Mordkin, R.; Joel, A.B.; Bernstein, G.; Nasr, N.M. Sexual, irritative, and voiding outcomes, following stereotactic body radiation therapy for prostate cancer. Radiat. Oncol. 2015, 10, 182. [Google Scholar] [CrossRef] [Green Version]
- Telkhade, T.; Murthy, V.; Kanala, T.S.; Mathew, J.M.; Phurailatpam, R.; Mokal, S.; Chourasiya, D.; Panigrahi, G.; Krishnatry, R. Safety and Efficacy of Ultra-hypofractionation in Node-positive Prostate Cancer. Clin. Oncol. (R. Coll. Radiol.) 2020. [Google Scholar] [CrossRef] [PubMed]
- Dearnaley, D.; Griffin, C.L.; Lewis, R.; Mayles, P.; Mayles, H.; Naismith, O.F.; Harris, V.; Scrase, C.D.; Staffurth, J.; Syndikus, I.; et al. Toxicity and Patient-Reported Outcomes of a Phase 2 Randomized Trial of Prostate and Pelvic Lymph Node Versus Prostate only Radiotherapy in Advanced Localised Prostate Cancer (PIVOTAL). Int. J. Radiat. Oncol. Biol. Phys. 2019, 103, 605–617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, C.A.; DeSilvio, M.; Roach, M., 3rd; Uhl, V.; Kirsch, R.; Seider, M.; Rotman, M.; Jones, C.; Asbell, S.; Valicenti, R.; et al. An update of the phase III trial comparing whole pelvic to prostate only radiotherapy and neoadjuvant to adjuvant total androgen suppression: Updated analysis of RTOG 94-13, with emphasis on unexpected hormone/radiation interactions. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 646–655. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez-Motta, A.; Roach, M., 3rd. Stereotactic body radiation therapy (SBRT) for high-risk prostate cancer: Where are we now? Pract. Radiat. Oncol. 2018, 8, 185–202. [Google Scholar] [CrossRef]
- Dixit, A.; Tang, C.; Bydder, S.; Kedda, M.A.; Vosikova, E.; Bharat, C.; Gill, S. First Australian experience of treating localised prostate cancer patients with CyberKnife stereotactic radiotherapy: Early PSA response, acute toxicity and quality of life. J. Med. Radiat. Sci. 2017, 64, 180–187. [Google Scholar] [CrossRef] [Green Version]
- Tree, A.C.; Ostler, P.; Hoskin, P.; Dankulchai, P.; Nariyangadu, P.; Hughes, R.J.; Wells, E.; Taylor, H.; Khoo, V.S.; van As, N.J. Prostate stereotactic body radiotherapy-first UK experience. Clin. Oncol. (R. Coll. Radiol.) 2014, 26, 757–761. [Google Scholar] [CrossRef] [PubMed]
- Katz, A.; Formenti, S.C.; Kang, J. Predicting Biochemical Disease-Free Survival after Prostate Stereotactic Body Radiotherapy: Risk-Stratification and Patterns of Failure. Front. Oncol. 2016, 6, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zilli, T.; Jorcano, S.; Bral, S.; Rubio, C.; Bruynzeel, A.M.E.; Oliveira, A.; Abacioglu, U.; Minn, H.; Symon, Z.; Miralbell, R. Once-a-week or every-other-day urethra-sparing prostate cancer stereotactic body radiotherapy, a randomized phase II trial: 18 months follow-up results. Cancer Med. 2020, 9, 3097–3106. [Google Scholar] [CrossRef]
- Zelefsky, M.J.; Kollmeier, M.; McBride, S.; Varghese, M.; Mychalczak, B.; Gewanter, R.; Garg, M.K.; Happersett, L.; Goldman, D.A.; Pei, I.; et al. Five-Year Outcomes of a Phase 1 Dose-Escalation Study Using Stereotactic Body Radiosurgery for Patients with Low-Risk and Intermediate-Risk Prostate Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2019, 104, 42–49. [Google Scholar] [CrossRef]
- Nicholls, L.; Suh, Y.-E.; Chapman, E.; Henderson, D.; Jones, C.; Morrison, K.; Sohaib, A.; Taylor, H.; Tree, A.; van As, N. Stereotactic Radiotherapy with Focal Boost for Intermediate and High-Risk Prostate Cancer: Initial Results of the Sparc Trial. Clin. Transl. Radiat. Oncol. 2020, 25, 88–93. [Google Scholar] [CrossRef]
- Patel, S.A.; Switchenko, J.M.; Fischer-Valuck, B.; Zhang, C.; Rose, B.S.; Chen, R.C.; Jani, S.B.; Royce, T.J. Stereotactic Body Radiotherapy Versus Conventional/Moderate Fractionated Radiation Therapy with Androgen Deprivation Therapy for Unfavorable Risk Prostate Cancer. Radiat. Oncol. 2020, 15, 217. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, A.V.; Whittington, R.; Malkowicz, S.B.; Schultz, D.; Blank, K.; Broderick, G.A.; Tomaszewski, J.E.; Renshaw, A.A.; Kaplan, I.; Beard, C.J.; et al. Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 1998, 280, 969–974. [Google Scholar] [CrossRef] [PubMed]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. JNCCN 2019, 17, 479–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trial | Year of Publication | Type of Trial | Years Recruited | Radiotherapy (RT) Technique | Risk Classification | Number of High-Risk (HR) Patients | Prescription Dose | Androgen Deprivation Therapy (ADT) Use in HR Patients |
|---|---|---|---|---|---|---|---|---|
| Kang JK et al. [34] | 2011 | Retrospective | 2002–2007 | CyberKnife (CK) | D’Amico | 29 | 4 × 8–9 Gy | 100% (≥24 months, 2 months neoadjuvant) |
| Oliai C et al. [42] | 2012 | Retrospective | 2007–2010 | CK | D’Amico | 12 | 5 × 7–7.5 Gy | 31% (<6–24 months) |
| King CR et al. [29] | 2013 | Phase II (pooled data) | 2003–2011 | CK | D’Amico | 121 | 5 × 7.25 Gy (median) | 38% 4 months (median) |
| Bolzicco G et al. [30] | 2013 | Prospective database | 2006–2012 | CK | National Comprehensive Cancer Network (NCCN) | 17 | 5 × 7 Gy | N/A |
| Chen LN et al. [41] | 2013 | Prospective database | 2008–2010 | CK | D’Amico | 8 | 5 × 7–7.25 Gy | 11% (3 weeks–36 months) |
| Tree AC et al. [56] | 2014 | Prospective database | 2010–2013 | CK | NCCN | 6 | 5 × 7.25 Gy | N/A |
| Lee SW et al. [48] | 2014 | Retrospective | 2006–2012 | CK | NCCN | 13 | 5 × 7.2 Gy | N/A |
| Janowski E et al. [47] | 2014 | Prospective database | 2008–2011 | CK | D’Amico | 9 | 5 × 7–7.25 Gy | 33.3% |
| Davis J et al. [35] | 2015 | Retrospective | 2006–2015 | CK Linear accelerator (Linac) | NCCN | 33 | 5 × 7.25 Gy (87%) | 45.5% |
| Rana Z et al. [50] | 2015 | Retrospective | 2008–2014 | CK | D’Amico | 8 | 5 × 7.25 Gy (median) | N/A |
| FASTR Baumann G et al. [28] | 2015 | Phase I/II | 2011–2017 | Linac | NCCN | 16 | 5 × 8 Gy (prostate) and 5 × 5 Gy (pelvic elective nodal irradiation (ENI)) | 100% (12 months) |
| Fan CY et al. [49] | 2015 | Retrospective | 2010–2013 | CK | NCCN | 16 | 5 × 7.5 Gy | 81% (6–24 months, neoadjuvant) |
| Dixit A et al. [55] | 2016 | Prospective database | 2014–2015 | CK | D’Amico | 6 | 5 × 7.25 Gy | 50% (3–6 months) |
| Kotecha R et al. [45] | 2016 | Prospective database | 2011–2014 | Linac | NCCN | 13 | 5 × 7.25/10 Gy (simultaneous-integrated boost (SIB)) | No |
| Ricco A et al. [36] | 2016 | Retrospective | 2007–2012 | CK | NCCN | 32 | 5 × 7–7.25 Gy | N/A |
| Katz A et al. [57] | 2016 | Prospective database | 2006–2010 | CK | NCCN | 38 | 5 × 7–7.25 Gy | 55.3% (6 months, neoadjuvant) |
| Koskela K et al. [39] | 2017 | Retrospective | 2012–2015 | CK | D’Amico | 111 | 5 × 7–7.25 Gy | 88.3% (48% for ≥2 years) |
| Murthy V et al. [31] | 2018 | Prospective database | 2014–2017 | Tomotherapy Linac | NCCN | 68 | 5 × 7–7.45 Gy (prostate) and 5 × 5 Gy (cN1) | 100% (≥2 years) |
| SATURN Alayed Y et al. [26] Musunuru HB et al. [38] | 2018/2019 | Phase I/II | 2013–2014 | Linac | NCCN | 30 | 5 × 8 Gy (prostate) and 5 × 5 Gy (pelvic ENI) | 100% (12–18 months) |
| HYPO-RT-PC Widmark A et al. [23] | 2019 | Phase III | 2005–2015 | Linac | NCCN | 62 | 7 × 6.1 Gy | No |
| FASTR-2 Callan L et al. [27] | 2019 | Phase I/II | 2015–2017 | Linac | NCCN | 28 | 5 × 7 Gy | 100% (18 months, 2 months neoadjuvant) |
| pHART8 Alayed Y et al. [26] | 2019 | Phase I/II | 2011–2013 | Linac | NCCN | 30 | 5 × 6/8 Gy (SIB) | 100% (12–18 months) |
| Zilli T et al. [58] | 2020 | Phase II | 2012–2015 | Linac | NCCN | 29 | 5 × 7.25 Gy | 100% (6 months, 2 months neoadjuvant) |
| Parameters | FASTR [28] | SATURN [38] | Murthy et al. 2018 [31] | |
|---|---|---|---|---|
| Primary clinical target volume (CTV) | Prostate + 1 cm seminal vesicles (SV) | Prostate | Prostate + entire SV | |
| Primary CTV to planning target volume (PTV) | 5 mm | 3 mm | 5 mm (3 mm posteriorly) | |
| Dose to prostate | 40 Gy to PTV | 40 Gy to CTV 33.25 Gy to PTV | 35 Gy–37.5 Gy to PTV | |
| Pelvic lymph node irradiation | 25 Gy to PTV | 25 Gy to CTV 23.75 Gy to PTV | 25 Gy to PTV | |
| Fractionation | Once weekly | Once weekly | Thrice weekly | |
| Image guidance | Cone beam computed tomography (CBCT) | CBCT + fiducials | CBCT | |
| Bladder dose constraints | V35 < 30% V29 < 50% | V35 < 5% V32 < 10% | V35 < 3% V17.5 < 20% | |
| Rectum dose constraints | V35 < 20% V27 < 50% | V35 < 5% V32 < 10% | V35 < 3% V31.5 < 8% V28 < 15% V17.5 < 40% | |
| Small bowel dose constraints | V25 < 190 cc V27.5 < 2 cc | V25 < 20 cc V30 < 2 cc | V28 < 80 cc | |
| Median Follow-up | 6 months | 24 months | 18 months | |
| Grade 2+ acute gastrointestinal (GI) toxicity | 0.0% | 3.3% | 4.0% | |
| Grade 2+ acute genitourinary (GU) toxicity | 25% | 46.7% | 12.0% | |
| Grade 2+ late GI toxicity | 50.1% | 32.0% | 4.0% | |
| Grade 2+ late GU toxicity | 37.5% | 60.0% | 7.0% | |
| Studies | ~1 year | ~2 years | ~3 years | ~4 years | 5 years | 7 years |
|---|---|---|---|---|---|---|
| Kang JK et al., 2011 [34] | - | - | 91% | - | - | - |
| King CR et al., 2013 [29] | - | - | - | - | 81% | - |
| Bolzicco G et al., 2013 [30] | - | - | 94% | - | - | - |
| Tree AC et al., 2014 [56] | 100% | - | - | - | - | - |
| Davis J et al., 2015 [35] | - | 82% | - | - | - | - |
| Rana Z et al., 2015 [50] | - | - | 100% | - | - | - |
| Fan CY et al., 2015 [49] | - | - | 56% | - | - | - |
| Ricco A et al., 2016 [36] | - | - | - | 88% | - | - |
| Kotecha R et al., 2016 [45] | - | 85% | - | - | - | - |
| Katz A et al., 2016 [57] | - | - | - | - | - | 71% |
| Koskela K et al., 2017 [39] | - | 93% | - | - | - | - |
| Murthy V et al., 2018 [31] | - | 94% | - | - | - | - |
| SATURN (2018/2019) [38] | - | 100% | - | - | - | - |
| FASTR-2 (2019) [27] | 100% | - | - | - | - | - |
| pHART 8 (2019) [26] | - | 97% | - | - | 85% | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Foerster, R.; Zwahlen, D.R.; Buchali, A.; Tang, H.; Schroeder, C.; Windisch, P.; Vu, E.; Akbaba, S.; Bostel, T.; Sprave, T.; et al. Stereotactic Body Radiotherapy for High-Risk Prostate Cancer: A Systematic Review. Cancers 2021, 13, 759. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040759
Foerster R, Zwahlen DR, Buchali A, Tang H, Schroeder C, Windisch P, Vu E, Akbaba S, Bostel T, Sprave T, et al. Stereotactic Body Radiotherapy for High-Risk Prostate Cancer: A Systematic Review. Cancers. 2021; 13(4):759. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040759
Chicago/Turabian StyleFoerster, Robert, Daniel Rudolf Zwahlen, Andre Buchali, Hongjian Tang, Christina Schroeder, Paul Windisch, Erwin Vu, Sati Akbaba, Tilman Bostel, Tanja Sprave, and et al. 2021. "Stereotactic Body Radiotherapy for High-Risk Prostate Cancer: A Systematic Review" Cancers 13, no. 4: 759. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040759