
Preclinical and Clinical Status of PSMA-Targeted Alpha Therapy for Metastatic Castration-Resistant Prostate Cancer

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
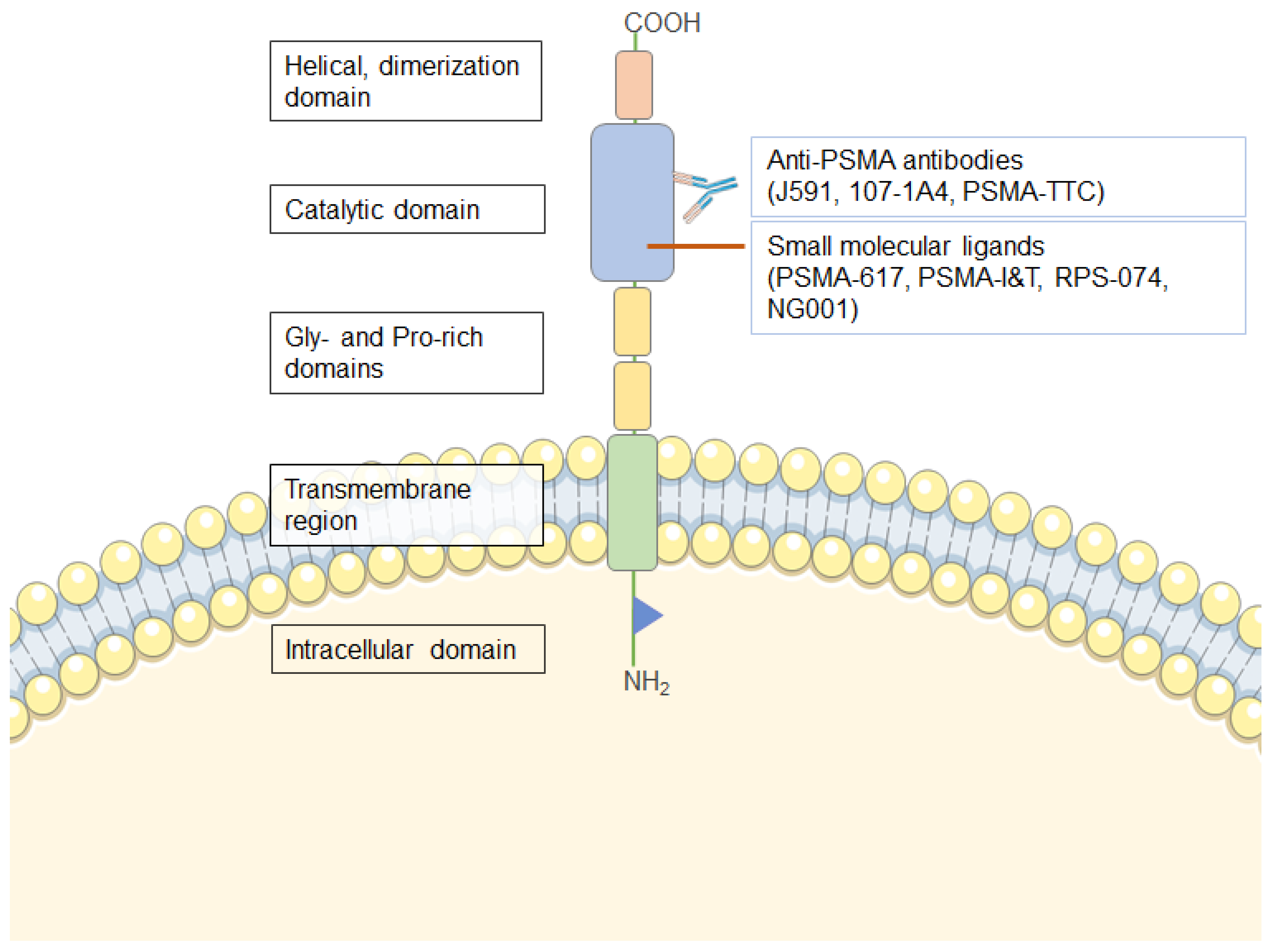
2. Prostate-Specific Membrane Antigen (PSMA)
3. Targeted Radionuclide Therapy of Prostate Cancer
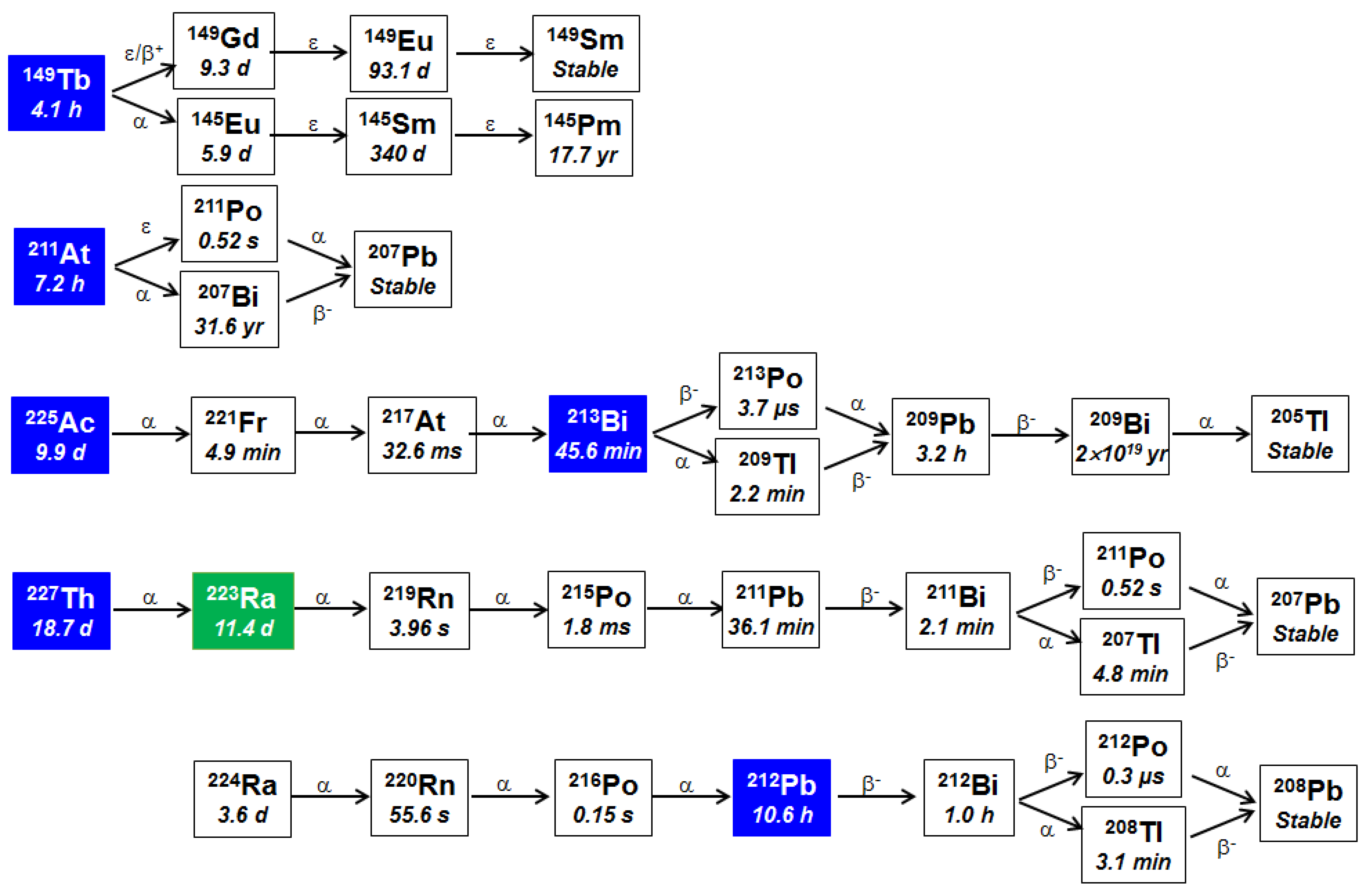
3.1. Radionuclides Used for PSMA-TAT
3.2. PSMA Targeting Agents in TRT
3.3. Radium-223 for PSMA-TAT
3.4. Bismuth-213 for PSMA-TAT
3.5. Astatine-211 for PSMA-TAT
3.6. Actinium-225 for PSMA-TAT
3.7. Thorium-227 for PSMA-TAT
3.8. Terbium-149 for PSMA-TAT
3.9. Lead-212 for PSMA-TAT
3.10. Dual Alpha (224Ra&212Pb) for TAT
3.11. Combination Treatments with PSMA-TAT
4. Limitations of Preclinical Studies Related to Clinical PSMA-TAT
5. Future of PSMA-TAT
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Ingrosso, G.; Detti, B.; Scartoni, D.; Lancia, A.; Giacomelli, I.; Baki, M.; Carta, G.; Livi, L.; Santoni, R. Current therapeutic options in metastatic castration-resistant prostate cancer. Semin. Oncol. 2018, 45, 303–315. [Google Scholar] [CrossRef]
- Labriola, M.K.; Atiq, S.; Hirshman, N.; Bitting, R.L. Management of men with metastatic castration-resistant prostate cancer following potent androgen receptor inhibition: A review of novel investigational therapies. Prostate Cancer Prostat. Dis. 2020. [Google Scholar] [CrossRef]
- Den, R.B.; George, D.; Pieczonka, C.; McNamara, M. Ra-223 Treatment for Bone Metastases in Castrate-Resistant Prostate Cancer: Practical Management Issues for Patient Selection. Am. J. Clin. Oncol. 2019, 42, 399–406. [Google Scholar] [CrossRef] [PubMed]
- Pezaro, C.; Omlin, A.; Lorente, D.; Rodrigues, D.N.; Ferraldeschi, R.; Bianchini, D.; Mukherji, D.; Riisnaes, R.; Altavilla, A.; Crespo, M.; et al. Visceral disease in castration-resistant prostate cancer. Eur. Urol. 2014, 65, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Parker, C.; Nilsson, S.; Heinrich, D.; Helle, S.I.; O’Sullivan, J.M.; Fossa, S.D.; Chodacki, A.; Wiechno, P.; Logue, J.; Seke, M.; et al. Alpha emitter radium-223 and survival in metastatic prostate cancer. N. Engl. J. Med. 2013, 369, 213–223. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mukherji, D.; El Dika, I.; Temraz, S.; Haidar, M.; Shamseddine, A. Evolving treatment approaches for the management of metastatic castration-resistant prostate cancer—Role of radium-223. Ther. Clin. Risk Manag. 2014, 10, 373–380. [Google Scholar] [CrossRef] [Green Version]
- Moussa, M.; Papatsoris, A.; Abou Chakra, M.; Sryropoulou, D.; Dellis, A. Pharmacotherapeutic strategies for castrate-resistant prostate cancer. Expert Opin. Pharmacother. 2020, 1–18. [Google Scholar] [CrossRef]
- Norum, J.; Nieder, C. Treatments for Metastatic Prostate Cancer (mPC): A Review of Costing Evidence. Pharmacoeconomics 2017, 35, 1223–1236. [Google Scholar] [CrossRef]
- Brönimann, S.; Lemberger, U.; Bruchbacher, A.; Shariat, S.F.; Hassler, M.R. Poly(ADP-ribose) polymerase inhibitors in prostate and urothelial cancer. Curr. Opin. Urol. 2020, 30, 519–526. [Google Scholar] [CrossRef]
- Pollard, M.E.; Moskowitz, A.J.; Diefenbach, M.A.; Hall, S.J. Cost-effectiveness analysis of treatments for metastatic castration resistant prostate cancer. Asian J. Urol. 2017, 4, 37–43. [Google Scholar] [CrossRef]
- Agrawal, S. The role of 225Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: Is it the new beginning. Indian J. Urol. IJU J. Urol. Soc. India 2020, 36, 69–70. [Google Scholar] [CrossRef] [PubMed]
- de Bono, J.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. N. Engl. J. Med. 2020, 382, 2091–2102. [Google Scholar] [CrossRef] [PubMed]
- Reyes, E.E.; VanderWeele, D.J.; Isikbay, M.; Duggan, R.; Campanile, A.; Stadler, W.M.; Vander Griend, D.J.; Szmulewitz, R.Z. Quantitative characterization of androgen receptor protein expression and cellular localization in circulating tumor cells from patients with metastatic castration-resistant prostate cancer. J. Transl. Med. 2014, 12, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Arasaratnam, M.; Crumbaker, M.; Bhatnagar, A.; McKay, M.J.; Molloy, M.P.; Gurney, H. Inter- and intra-patient variability in pharmacokinetics of abiraterone acetate in metastatic prostate cancer. Cancer Chemother. Pharmacol. 2019, 84, 139–146. [Google Scholar] [CrossRef] [PubMed]
- Kyriakopoulos, C.E.; Heath, E.I.; Ferrari, A.; Sperger, J.M.; Singh, A.; Perlman, S.B.; Roth, A.R.; Perk, T.G.; Modelska, K.; Porcari, A.; et al. Exploring Spatial-Temporal Changes in (18)F-Sodium Fluoride PET/CT and Circulating Tumor Cells in Metastatic Castration-Resistant Prostate Cancer Treated With Enzalutamide. J. Clin. Oncol. 2020, 38, 3662–3671. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Gray, K.E.; Webb, I.J.; Gray, G.S.; Rolfe, M.; Schenkein, D.P.; Nanus, D.M.; Millowsky, M.I.; Bander, N.H. Antibody-based therapeutics: Focus on prostate cancer. Cancer Metastasis Rev. 2005, 24, 521–537. [Google Scholar] [CrossRef]
- Barve, A.; Jin, W.; Cheng, K. Prostate cancer relevant antigens and enzymes for targeted drug delivery. J. Control. Release Off. J. Control. Release Soc. 2014, 187, 118–132. [Google Scholar] [CrossRef] [Green Version]
- Evans, J.C.; Malhotra, M.; Cryan, J.F.; O’Driscoll, C.M. The therapeutic and diagnostic potential of the prostate specific membrane antigen/glutamate carboxypeptidase II (PSMA/GCPII) in cancer and neurological disease. Br. J. Pharmacol. 2016, 173, 3041–3079. [Google Scholar] [CrossRef] [Green Version]
- Ross, J.S.; Sheehan, C.E.; Fisher, H.A.; Kaufman, R.P., Jr.; Kaur, P.; Gray, K.; Webb, I.; Gray, G.S.; Mosher, R.; Kallakury, B.V. Correlation of primary tumor prostate-specific membrane antigen expression with disease recurrence in prostate cancer. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2003, 9, 6357–6362. [Google Scholar]
- Hupe, M.C.; Philippi, C.; Roth, D.; Kumpers, C.; Ribbat-Idel, J.; Becker, F.; Joerg, V.; Duensing, S.; Lubczyk, V.H.; Kirfel, J.; et al. Expression of Prostate-Specific Membrane Antigen (PSMA) on Biopsies Is an Independent Risk Stratifier of Prostate Cancer Patients at Time of Initial Diagnosis. Front. Oncol. 2018, 8, 623. [Google Scholar] [CrossRef]
- Paschalis, A.; Sheehan, B.; Riisnaes, R.; Rodrigues, D.N.; Gurel, B.; Bertan, C.; Ferreira, A.; Lambros, M.B.K.; Seed, G.; Yuan, W.; et al. Prostate-specific Membrane Antigen Heterogeneity and DNA Repair Defects in Prostate Cancer. Eur. Urol. 2019, 76, 469–478. [Google Scholar] [CrossRef] [Green Version]
- Kasperzyk, J.L.; Finn, S.P.; Flavin, R.; Fiorentino, M.; Lis, R.; Hendrickson, W.K.; Clinton, S.K.; Sesso, H.D.; Giovannucci, E.L.; Stampfer, M.J.; et al. Prostate-specific membrane antigen protein expression in tumor tissue and risk of lethal prostate cancer. Cancer Epidemiol. Prev. Biomark. 2013, 22, 2354–2363. [Google Scholar] [CrossRef] [Green Version]
- Ghosh, A.; Heston, W.D. Tumor target prostate specific membrane antigen (PSMA) and its regulation in prostate cancer. J. Cell. Biochem. 2004, 91, 528–539. [Google Scholar] [CrossRef]
- Troyer, J.K.; Beckett, M.L.; Wright, G.L., Jr. Detection and characterization of the prostate-specific membrane antigen (PSMA) in tissue extracts and body fluids. Int. J. Cancer 1995, 62, 552–558. [Google Scholar]
- Silver, D.A.; Pellicer, I.; Fair, W.R.; Heston, W.D.; Cordon-Cardo, C. Prostate-specific membrane antigen expression in normal and malignant human tissues. Clin. Cancer Res. 1997, 3, 81–85. [Google Scholar]
- Kinoshita, Y.; Kuratsukuri, K.; Landas, S.; Imaida, K.; Rovito, P.M., Jr.; Wang, C.Y.; Haas, G.P. Expression of prostate-specific membrane antigen in normal and malignant human tissues. World J. Surg. 2006, 30, 628–636. [Google Scholar] [CrossRef]
- Jin, W.; Barve, A.; Cheng, K. PSMA-specific ligands in prostate cancer diagnosis and therapy. EMJ Urol. 2016, 4, 62–69. [Google Scholar]
- Cimadamore, A.; Cheng, M.; Santoni, M.; Lopez-Beltran, A.; Battelli, N.; Massari, F.; Galosi, A.B.; Scarpelli, M.; Montironi, R. New Prostate Cancer Targets for Diagnosis, Imaging, and Therapy: Focus on Prostate-Specific Membrane Antigen. Front. Oncol. 2018, 8, 653. [Google Scholar] [CrossRef] [Green Version]
- Vahidfar, N.; Fallahpoor, M.; Farzanehfar, S.; Divband, G.; Ahmadzadehfar, H. Historical review of pharmacological development and dosimetry of PSMA-based theranostics for prostate cancer. J. Radioanal. Nucl. Chem. 2019, 322, 237–248. [Google Scholar] [CrossRef]
- Jones, W.; Griffiths, K.; Barata, P.C.; Paller, C.J. PSMA Theranostics: Review of the Current Status of PSMA-Targeted Imaging and Radioligand Therapy. Cancers 2020, 12, 1367. [Google Scholar] [CrossRef]
- Bravaccini, S.; Puccetti, M.; Bocchini, M.; Ravaioli, S.; Celli, M.; Scarpi, E.; De Giorgi, U.; Tumedei, M.M.; Raulli, G.; Cardinale, L.; et al. PSMA expression: A potential ally for the pathologist in prostate cancer diagnosis. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruigrok, E.A.M.; van Weerden, W.M.; Nonnekens, J.; de Jong, M. The Future of PSMA-Targeted Radionuclide Therapy: An Overview of Recent Preclinical Research. Pharmaceutics 2019, 11, 560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rathke, H.; Flechsig, P.; Mier, W.; Bronzel, M.; Mavriopoulou, E.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; Kratochwil, C. Dosimetry Estimate and Initial Clinical Experience with (90)Y-PSMA-617. J. Nucl. Med. 2019, 60, 806–811. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kelly, J.M.; Ponnala, S.; Amor-Coarasa, A.; Zia, N.A.; Nikolopoulou, A.; Williams, C., Jr.; Schlyer, D.J.; DiMagno, S.G.; Donnelly, P.S.; Babich, J.W. Preclinical Evaluation of a High-Affinity Sarcophagine-Containing PSMA Ligand for (64)Cu/(67)Cu-Based Theranostics in Prostate Cancer. Mol. Pharm. 2020, 17, 1954–1962. [Google Scholar] [CrossRef]
- Carlos Dos Santos, J.; Beijer, B.; Bauder-Wüst, U.; Schäfer, M.; Leotta, K.; Eder, M.; Benešová, M.; Kleist, C.; Giesel, F.; Kratochwil, C.; et al. Development of Novel PSMA Ligands for Imaging and Therapy with Copper Isotopes. J. Nucl. Med. 2020, 61, 70–79. [Google Scholar] [CrossRef]
- Yadav, M.P.; Ballal, S.; Bal, C.; Sahoo, R.K.; Damle, N.A.; Tripathi, M.; Seth, A. Efficacy and Safety of 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer Patients. Clin. Nucl. Med. 2020, 45, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Dwivedi, S.N.; Bal, C. Radioligand Therapy With (177)Lu-PSMA for Metastatic Castration-Resistant Prostate Cancer: A Systematic Review and Meta-Analysis. Am. J. Roentgenol. 2019, 213, 275–285. [Google Scholar] [CrossRef]
- von Eyben, F.E.; Roviello, G.; Kiljunen, T.; Uprimny, C.; Virgolini, I.; Kairemo, K.; Joensuu, T. Third-line treatment and (177)Lu-PSMA radioligand therapy of metastatic castration-resistant prostate cancer: A systematic review. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 496–508. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schafers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German Multicenter Study Investigating 177Lu-PSMA-617 Radioligand Therapy in Advanced Prostate Cancer Patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef] [Green Version]
- Chakravarty, R.; Siamof, C.M.; Dash, A.; Cai, W. Targeted alpha-therapy of prostate cancer using radiolabeled PSMA inhibitors: A game changer in nuclear medicine. Am. J. Nucl. Med. Mol. Imaging 2018, 8, 247–267. [Google Scholar]
- Kratochwil, C.; Bruchertseifer, F.; Giesel, F.L.; Weis, M.; Verburg, F.A.; Mottaghy, F.; Kopka, K.; Apostolidis, C.; Haberkorn, U.; Morgenstern, A. 225Ac-PSMA-617 for PSMA-Targeted alpha-Radiation Therapy of Metastatic Castration-Resistant Prostate Cancer. J. Nucl. Med. 2016, 57, 1941–1944. [Google Scholar] [CrossRef] [Green Version]
- Satapathy, S.; Mittal, B.R.; Sood, A. Visceral Metastases as Predictors of Response and Survival Outcomes in Patients of Castration-Resistant Prostate Cancer Treated With 177Lu-Labeled Prostate-Specific Membrane Antigen Radioligand Therapy: A Systematic Review and Meta-analysis. Clin. Nucl. Med. 2020, 45, 935–942. [Google Scholar] [CrossRef]
- Emmett, L.; Willowson, K.; Violet, J.; Shin, J.; Blanksby, A.; Lee, J. Lutetium (177) PSMA radionuclide therapy for men with prostate cancer: A review of the current literature and discussion of practical aspects of therapy. J. Med. Radiat. Sci. 2017, 64, 52–60. [Google Scholar] [CrossRef]
- Bernhardt, P.; Forssell-Aronsson, E.; Jacobsson, L.; Skarnemark, G. Low-energy electron emitters for targeted radiotherapy of small tumours. Acta Oncol. 2001, 40, 602–608. [Google Scholar]
- Hindié, E.; Zanotti-Fregonara, P.; Quinto, M.A.; Morgat, C.; Champion, C. Dose Deposits from 90Y, 177Lu, 111In, and 161Tb in Micrometastases of Various Sizes: Implications for Radiopharmaceutical Therapy. J. Nucl. Med. 2016, 57, 759–764. [Google Scholar] [CrossRef] [Green Version]
- Behr, T.M.; Béhé, M.; Stabin, M.G.; Wehrmann, E.; Apostolidis, C.; Molinet, R.; Strutz, F.; Fayyazi, A.; Wieland, E.; Gratz, S.; et al. High-linear energy transfer (LET) alpha versus low-LET beta emitters in radioimmunotherapy of solid tumors: Therapeutic efficacy and dose-limiting toxicity of 213Bi- versus 90Y-labeled CO17-1A Fab’ fragments in a human colonic cancer model. Cancer Res. 1999, 59, 2635–2643. [Google Scholar]
- Barinka, C.; Sácha, P.; Sklenár, J.; Man, P.; Bezouska, K.; Slusher, B.S.; Konvalinka, J. Identification of the N-glycosylation sites on glutamate carboxypeptidase II necessary for proteolytic activity. Protein Sci. Publ. Protein Soc. 2004, 13, 1627–1635. [Google Scholar] [CrossRef] [Green Version]
- Davis, M.I.; Bennett, M.J.; Thomas, L.M.; Bjorkman, P.J. Crystal structure of prostate-specific membrane antigen, a tumor marker and peptidase. Proc. Natl. Acad. Sci. USA 2005, 102, 5981–5986. [Google Scholar] [CrossRef] [Green Version]
- Sokoloff, R.L.; Norton, K.C.; Gasior, C.L.; Marker, K.M.; Grauer, L.S. A dual-monoclonal sandwich assay for prostate-specific membrane antigen: Levels in tissues, seminal fluid and urine. Prostate 2000, 43, 150–157. [Google Scholar] [CrossRef]
- Yao, V.; Berkman, C.E.; Choi, J.K.; O’Keefe, D.S.; Bacich, D.J. Expression of prostate-specific membrane antigen (PSMA), increases cell folate uptake and proliferation and suggests a novel role for PSMA in the uptake of the non-polyglutamated folate, folic acid. Prostate 2010, 70, 305–316. [Google Scholar] [CrossRef]
- Maurer, T.; Eiber, M.; Schwaiger, M.; Gschwend, J.E. Current use of PSMA-PET in prostate cancer management. Nat. Rev. Urol. 2016, 13, 226–235. [Google Scholar] [CrossRef]
- Wibmer, A.G.; Burger, I.A.; Sala, E.; Hricak, H.; Weber, W.A.; Vargas, H.A. Molecular Imaging of Prostate Cancer. Radiographics 2016, 36, 142–159. [Google Scholar] [CrossRef] [Green Version]
- Rajasekaran, A.K.; Anilkumar, G.; Christiansen, J.J. Is prostate-specific membrane antigen a multifunctional protein? Am. J. Physiol. Cell Physiol. 2005, 288, C975–C981. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Czerwińska, M.; Bilewicz, A.; Kruszewski, M.; Wegierek-Ciuk, A.; Lankoff, A. Targeted Radionuclide Therapy of Prostate Cancer-From Basic Research to Clinical Perspectives. Molecules 2020, 25, 1743. [Google Scholar] [CrossRef] [Green Version]
- Rahbar, K.; Afshar-Oromieh, A.; Jadvar, H.; Ahmadzadehfar, H. PSMA Theranostics: Current Status and Future Directions. Mol. Imaging 2018, 17, 1536012118776068. [Google Scholar] [CrossRef] [Green Version]
- Jadvar, H. Targeted Radionuclide Therapy: An Evolution Toward Precision Cancer Treatment. Am. J. Roentgenol. 2017, 209, 277–288. [Google Scholar] [CrossRef] [Green Version]
- Quast, U. Whole body radiotherapy: A TBI-guideline. J. Med. Phys. 2006, 31, 5–12. [Google Scholar] [CrossRef]
- Seidl, C. Radioimmunotherapy with α-particle-emitting radionuclides. Immunotherapy 2014, 6, 431–458. [Google Scholar] [CrossRef]
- Parker, C.; Lewington, V.; Shore, N.; Kratochwil, C.; Levy, M.; Linden, O.; Noordzij, W.; Park, J.; Saad, F. Targeted Alpha Therapy, an Emerging Class of Cancer Agents: A Review. JAMA Oncol. 2018, 4, 1765–1772. [Google Scholar] [PubMed]
- Navalkissoor, S.; Grossman, A. Targeted Alpha Particle Therapy for Neuroendocrine Tumours: The Next Generation of Peptide Receptor Radionuclide Therapy. Neuroendocrinology 2019, 108, 256–264. [Google Scholar] [CrossRef] [PubMed]
- Tomita, M.; Maeda, M. Mechanisms and biological importance of photon-induced bystander responses: Do they have an impact on low-dose radiation responses. J. Radiat. Res. 2015, 56, 205–219. [Google Scholar] [CrossRef] [Green Version]
- Parker, C.; Heidenreich, A.; Nilsson, S.; Shore, N. Current approaches to incorporation of radium-223 in clinical practice. Prostate Cancer Prostat. Dis. 2018, 21, 37–47. [Google Scholar] [CrossRef]
- Dandapani, S.V.; Wong, J.; Twardowski, P. Review of Radium-223 and Metastatic Castration-Sensitive Prostate Cancer. Cancer Biother. Radiopharm. 2020, 35, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Etchebehere, E.; Brito, A.E.; Rezaee, A.; Langsteger, W.; Beheshti, M. Therapy assessment of bone metastatic disease in the era of (223)radium. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Bruland, Ø.S.; Nilsson, S.; Fisher, D.R.; Larsen, R.H. High-linear energy transfer irradiation targeted to skeletal metastases by the alpha-emitter 223Ra: Adjuvant or alternative to conventional modalities? Clin. Cancer Res. 2006, 12, 6250s–6257s. [Google Scholar] [CrossRef] [Green Version]
- Hoskin, P.; Sartor, O.; O’Sullivan, J.M.; Johannessen, D.C.; Helle, S.I.; Logue, J.; Bottomley, D.; Nilsson, S.; Vogelzang, N.J.; Fang, F.; et al. Efficacy and safety of radium-223 dichloride in patients with castration-resistant prostate cancer and symptomatic bone metastases, with or without previous docetaxel use: A prespecified subgroup analysis from the randomised, double-blind, phase 3 ALSYMPCA trial. Lancet Oncol. 2014, 15, 1397–1406. [Google Scholar]
- De Vincentis, G.; Gerritsen, W.; Gschwend, J.E.; Hacker, M.; Lewington, V.; O’Sullivan, J.M.; Oya, M.; Pacilio, M.; Parker, C.; Shore, N.; et al. Advances in targeted alpha therapy for prostate cancer. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2019, 30, 1728–1739. [Google Scholar] [CrossRef]
- Facchini, G.; Cavaliere, C.; D’Aniello, C.; Iovane, G.; Rossetti, S. Abiraterone acetate treatment in patients with castration-resistant prostate cancer with visceral metastases: A real-world experience. Anti-Cancer Drugs 2019, 30, 179–185. [Google Scholar] [CrossRef]
- Rahbar, K.; Boegemann, M.; Yordanova, A.; Eveslage, M.; Schafers, M.; Essler, M.; Ahmadzadehfar, H. PSMA targeted radioligandtherapy in metastatic castration resistant prostate cancer after chemotherapy, abiraterone and/or enzalutamide. A retrospective analysis of overall survival. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 12–19. [Google Scholar] [CrossRef]
- Ferrier, M.G.; Radchenko, V. An Appendix of Radionuclides Used in Targeted Alpha Therapy. J. Med. Imaging Radiat. Sci. 2019, 50, S58–S65. [Google Scholar] [CrossRef] [Green Version]
- Liberal, F.D.C.G.; O’Sullivan, J.M.; McMahon, S.J.; Prise, K.M. Targeted Alpha Therapy: Current Clinical Applications. Cancer Biother. Radiopharm. 2020, 35, 404–417. [Google Scholar] [CrossRef]
- Garashchenko, B.L.; Korsakova, V.A.; Yakovlev, R.Y. Radiopharmaceuticals Based on Alpha Emitters: Preparation, Properties, and Application. Phys. Nucl. 2018, 81, 1515–1525. [Google Scholar] [CrossRef]
- Poty, S.; Francesconi, L.C.; McDevitt, M.R.; Morris, M.J.; Lewis, J.S. Alpha-Emitters for Radiotherapy: From Basic Radiochemistry to Clinical Studies-Part 1. J. Nucl. Med. 2018, 59, 878–884. [Google Scholar] [CrossRef] [Green Version]
- National Nuclear Data Center, Brookhaven National Laboratory, Upton, NY. Available online: https://www.nndc.bnl.gov/ (accessed on 4 September 2020).
- Covell, D.G.; Barbet, J.; Holton, O.D.; Black, C.D.; Parker, R.J.; Weinstein, J.N. Pharmacokinetics of monoclonal immunoglobulin G1, F(ab’)2, and Fab’ in mice. Cancer Res. 1986, 46, 3969–3978. [Google Scholar]
- Tabrizi, M.A.; Tseng, C.M.; Roskos, L.K. Elimination mechanisms of therapeutic monoclonal antibodies. Drug Discov. Today 2006, 11, 81–88. [Google Scholar] [CrossRef]
- Ovacik, M.; Lin, K. Tutorial on Monoclonal Antibody Pharmacokinetics and Its Considerations in Early Development. Clin. Transl. Sci. 2018, 11, 540–552. [Google Scholar] [CrossRef]
- Miyahira, A.K.; Pienta, K.J.; Morris, M.J.; Bander, N.H.; Baum, R.P.; Fendler, W.P.; Goeckeler, W.; Gorin, M.A.; Hennekes, H.; Pomper, M.G.; et al. Meeting report from the Prostate Cancer Foundation PSMA-directed radionuclide scientific working group. Prostate 2018, 78, 775–789. [Google Scholar] [CrossRef]
- Holmes, E.H. PSMA specific antibodies and their diagnostic and therapeutic use. Expert Opin. Investig. Drugs 2001, 10, 511–519. [Google Scholar] [CrossRef]
- Ballangrud, A.M.; Yang, W.H.; Charlton, D.E.; McDevitt, M.R.; Hamacher, K.A.; Panageas, K.S.; Ma, D.; Bander, N.H.; Scheinberg, D.A.; Sgouros, G. Response of LNCaP spheroids after treatment with an alpha-particle emitter (213Bi)-labeled anti-prostate-specific membrane antigen antibody (J591). Cancer Res. 2001, 61, 2008–2014. [Google Scholar]
- Vaidyanathan, G.; Mease, R.; Affleck, D.; Chen, Y.; Welsh, P.; Hens, M.; Pomper, M.; Zalutsky, M. An astatine-211 labeled PSMA inhibitor for targeted alpha-particle radiotherapy of prostate carcinoma. J. Nucl. Med. 2009, 50, 40. [Google Scholar]
- Bandekar, A.; Zhu, C.; Jindal, R.; Bruchertseifer, F.; Morgenstern, A.; Sofou, S. Anti-prostate-specific membrane antigen liposomes loaded with 225Ac for potential targeted antivascular α-particle therapy of cancer. J. Nucl. Med. 2014, 55, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Czerwińska, M.; Fracasso, G.; Pruszyński, M.; Bilewicz, A.; Kruszewski, M.; Majkowska-Pilip, A.; Lankoff, A. Design and Evaluation of (223)Ra-Labeled and Anti-PSMA Targeted NaA Nanozeolites for Prostate Cancer Therapy-Part I. Materials 2020, 13, 3875. [Google Scholar] [CrossRef]
- Umbricht, C.A.; Koster, U.; Bernhardt, P.; Gracheva, N.; Johnston, K.; Schibli, R.; van der Meulen, N.P.; Muller, C. Alpha-PET for Prostate Cancer: Preclinical investigation using (149)Tb-PSMA-617. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Wilbur, D.S.; Hamlin, D.; Nguyen, H.; Nakamae, H.; Chyan, M.K.; Vessella, R.L.; Sandmaier, B. Preliminary studies using At-211-labeled anti-PSMA MAb for treatment of metastatic prostate cancer in a mouse model. J. Nucl. Med. 2009, 50, 39. [Google Scholar]
- Wilbur, D.S.; Chyan, M.K.; Hamlin, D.K.; Nguyen, H.; Vessella, R.L. Reagents for astatination of biomolecules. 5. Evaluation of hydrazone linkers in (211)At- and (125)I-labeled closo-decaborate(2-) conjugates of Fab’ as a means of decreasing kidney retention. Bioconjug. Chem. 2011, 22, 1089–1102. [Google Scholar] [CrossRef] [Green Version]
- Kiess, A.P.; Minn, I.; Vaidyanathan, G.; Hobbs, R.F.; Josefsson, A.; Shen, C.; Brummet, M.; Chen, Y.; Choi, J.; Koumarianou, E.; et al. (2S)-2-(3-(1-Carboxy-5-(4-211At-Astatobenzamido)Pentyl)Ureido)-Pentanedioic Acid for PSMA-Targeted alpha-Particle Radiopharmaceutical Therapy. J. Nucl. Med. 2016, 57, 1569–1575. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.M.; Amor-Coarasa, A.; Nikolopoulou, A.; Wüstemann, T.; Barelli, P.; Kim, D.; Williams, C., Jr.; Zheng, X.; Bi, C.; Hu, B.; et al. Dual-Target Binding Ligands with Modulated Pharmacokinetics for Endoradiotherapy of Prostate Cancer. J. Nucl. Med. 2017, 58, 1442–1449. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Chyan, M.K.; Hamlin, D.K.; Nguyen, H.; Vessella, R.; Wilbur, D.S. Evaluation of radioiodinated protein conjugates and their potential metabolites containing lysine-urea-glutamate (LuG), PEG and closo-decaborate(2-) as models for targeting astatine-211 to metastatic prostate cancer. Nucl. Med. Biol. 2020, 92, 217–227. [Google Scholar] [CrossRef]
- Dos Santos, J.C.; Schafer, M.; Bauder-Wust, U.; Lehnert, W.; Leotta, K.; Morgenstern, A.; Kopka, K.; Haberkorn, U.; Mier, W.; Kratochwil, C. Development and dosimetry of (203)Pb/(212)Pb-labelled PSMA ligands: Bringing “the lead“ into PSMA-targeted alpha therapy? Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1081–1091. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, S.R.; Minn, I.L.; Kumar, V.; Josefsson, A.; Lisok, A.; Brummet, M.; Chen, J.; Kiess, A.; Baidoo, K.; Brayton, C.; et al. Preclinical evaluation of 203/212Pb-labeled low-molecular-weight compounds for targeted radiopharmaceutical therapy of prostate cancer. J. Nucl. Med. 2020, 61, 80–88. [Google Scholar] [CrossRef]
- Larsen, R.H. Lead and Thorium Compounds. U.S. Patent 10377778B2, 13 August 2019. [Google Scholar]
- Stenberg, V.Y.; Juzeniene, A.; Chen, Q.; Yang, X.; Bruland, O.S.; Larsen, R.H. Preparation of the alpha-emitting PSMA targeted radioligand [(212) Pb]Pb-NG001 for prostate cancer. J. Label. Compd. Radiopharm. 2020, 63, 129–143. [Google Scholar] [CrossRef] [Green Version]
- Stenberg, V.Y.; Juzeniene, A.; Bruland, Ø.S.; Larsen, R.H. In situ Generated 212Pb-PSMA Ligand in a 224Ra-Solution for Dual Targeting of Prostate Cancer Sclerotic Stroma and PSMA-positive Cells. Curr. Radiopharm. 2020, 13, 130–141. [Google Scholar] [CrossRef]
- McDevitt, M.R.; Barendswaard, E.; Ma, D.; Lai, L.; Curcio, M.J.; Sgouros, G.; Ballangrud, A.M.; Yang, W.H.; Finn, R.D.; Pellegrini, V.; et al. An alpha-particle emitting antibody ([213Bi]J591) for radioimmunotherapy of prostate cancer. Cancer Res. 2000, 60, 6095–6100. [Google Scholar]
- Li, Y.; Tian, Z.; Rizvi, S.M.; Bander, N.H.; Allen, B.J. In vitro and preclinical targeted alpha therapy of human prostate cancer with Bi-213 labeled J591 antibody against the prostate specific membrane antigen. Prostate Cancer Prostat. Dis. 2002, 5, 36–46. [Google Scholar] [CrossRef]
- Nonnekens, J.; Chatalic, K.L.; Molkenboer-Kuenen, J.D.; Beerens, C.E.; Bruchertseifer, F.; Morgenstern, A.; Veldhoven-Zweistra, J.; Schottelius, M.; Wester, H.J.; van Gent, D.C.; et al. (213)Bi-Labeled Prostate-Specific Membrane Antigen-Targeting Agents Induce DNA Double-Strand Breaks in Prostate Cancer Xenografts. Cancer Biother. Radiopharm. 2017, 32, 67–73. [Google Scholar] [CrossRef]
- Meyer, C.; Stuparu, A.; Wei, L.; Capri, J.; Le, T.; Radu, C.; Czernin, J.; Dahlbom, M.; Slavik, R. Therapeutic Efficacy and Dosimetry of Targeted Alpha Therapy using 225Ac-PSMA-617 in a Murine Model of Prostate Cancer. J. Med. Imaging Radiat. Sci. 2019, 50, S93–S94. [Google Scholar] [CrossRef]
- Stuparu, A.D.; Meyer, C.A.L.; Evans-Axelsson, S.L.; Lückerath, K.; Wei, L.H.; Kim, W.; Poddar, S.; Mona, C.E.; Dahlbom, M.; Girgis, M.D.; et al. Targeted alpha therapy in a systemic mouse model of prostate cancer—A feasibility study. Theranostics 2020, 10, 2612–2620. [Google Scholar] [CrossRef]
- Current, K.; Meyer, C.; Magyar, C.E.; Mona, C.E.; Almajano, J.; Slavik, R.; Stuparu, A.D.; Cheng, C.; Dawson, D.W.; Radu, C.G.; et al. Investigating PSMA-targeted radioligand therapy efficacy as a function of cellular PSMA levels and intra-tumoral PSMA heterogeneity. Clin. Cancer Res. 2020, 26, 2946–2955. [Google Scholar] [CrossRef]
- Czernin, J.; Current, K.; Mona, C.E.; Nyiranshuti, L.; Hikmat, F.; Radu, C.G.; Lueckerath, K. Immune-Checkpoint Blockade Enhances (225)Ac-PSMA617 Efficacy in a Mouse Model of Prostate Cancer. J. Nucl. Med. 2020, 62, 228–231. [Google Scholar] [CrossRef]
- Kelly, J.M.; Amor-Coarasa, A.; Ponnala, S.; Nikolopoulou, A.; Williams, C., Jr.; Thiele, N.A.; Schlyer, D.; Wilson, J.J.; DiMagno, S.G.; Babich, J.W. A Single Dose of (225)Ac-RPS-074 Induces a Complete Tumor Response in an LNCaP Xenograft Model. J. Nucl. Med. 2019, 60, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hammer, S.; Hagemann, U.B.; Zitzmann-Kolbe, S.; Larsen, A.; Ellingsen, C.; Geraudie, S.; Grant, D.; Indrevoll, B.; Smeets, R.; von Ahsen, O.; et al. Preclinical Efficacy of a PSMA-Targeted Thorium-227 Conjugate (PSMA-TTC), a Targeted Alpha Therapy for Prostate Cancer. Clin. Cancer Res. 2020, 26, 1985–1996. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sathekge, M.; Knoesen, O.; Meckel, M.; Modiselle, M.; Vorster, M.; Marx, S. (213)Bi-PSMA-617 targeted alpha-radionuclide therapy in metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 1099–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Bronzel, M.; Apostolidis, C.; Weichert, W.; Haberkorn, U.; Giesel, F.L.; Morgenstern, A. Targeted alpha-Therapy of Metastatic Castration-Resistant Prostate Cancer with (225)Ac-PSMA-617: Dosimetry Estimate and Empiric Dose Finding. J. Nucl. Med. 2017, 58, 1624–1631. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Bruchertseifer, F.; Rathke, H.; Hohenfellner, M.; Giesel, F.L.; Haberkorn, U.; Morgenstern, A. Targeted alpha-Therapy of Metastatic Castration-Resistant Prostate Cancer with (225)Ac-PSMA-617: Swimmer-Plot Analysis Suggests Efficacy Regarding Duration of Tumor Control. J. Nucl. Med. 2018, 59, 795–802. [Google Scholar] [CrossRef] [Green Version]
- Sathekge, M.M.; Bruchertseifer, F.; Lawal, I.O.; Vorster, M.; Knoesen, O.; Lengana, T.; Boshomane, T.G.; Mokoala, K.K.; Morgenstern, A. Treatment of brain metastases of castration-resistant prostate cancer with (225)Ac-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 1756–1757. [Google Scholar] [CrossRef] [PubMed]
- Sathekge, M.; Bruchertseifer, F.; Knoesen, O.; Reyneke, F.; Lawal, I.; Lengana, T.; Davis, C.; Mahapane, J.; Corbett, C.; Vorster, M.; et al. (225)Ac-PSMA-617 in chemotherapy-naive patients with advanced prostate cancer: A pilot study. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 129–138. [Google Scholar] [CrossRef] [Green Version]
- de Medeiros, R.B.; Grigolon, M.V.; Araújo, T.P.; Srougi, M. Metastatic castration-resistant prostate cancer (mCRPC) treated with 225Ac-PSMA-617. Case report. Braz. J. Oncol. 2019, 15, 1–9. [Google Scholar] [CrossRef]
- Sathekge, M.; Bruchertseifer, F.; Vorster, M.; Lawal, I.O.; Knoesen, O.; Mahapane, J.; Davis, C.; Reyneke, F.; Maes, A.; Kratochwil, C.; et al. Predictors of Overall and Disease-Free Survival in Metastatic Castration-Resistant Prostate Cancer Patients Receiving (225)Ac-PSMA-617 Radioligand Therapy. J. Nucl. Med. 2020, 61, 62–69. [Google Scholar] [CrossRef]
- Feuerecker, B.; Tauber, R.; Knorr, K.; Heck, M.; Beheshti, A.; Seidl, C.; Bruchertseifer, F.; Pickhard, A.; Gafita, A.; Kratochwil, C.; et al. Activity and Adverse Events of Actinium-225-PSMA-617 in Advanced Metastatic Castration-resistant Prostate Cancer After Failure of Lutetium-177-PSMA. Eur. Urol. 2020. [Google Scholar] [CrossRef]
- Yadav, M.P.; Ballal, S.; Sahoo, R.K.; Tripathi, M.; Seth, A.; Bal, C. Efficacy and safety of (225)Ac-PSMA-617 targeted alpha therapy in metastatic castration-resistant Prostate Cancer patients. Theranostics 2020, 10, 9364–9377. [Google Scholar] [CrossRef]
- Pelletier, K.; Côté, G.; Fallah-Rad, N.; John, R.; Kitchlu, A. Chronic kidney disease after 225Ac-PSMA617 therapy in patients with metastatic prostate cancer. Kidney Int. Rep. 2021, in press. [Google Scholar]
- van der Doelen, M.J.; Mehra, N.; van Oort, I.M.; Looijen-Salamon, M.G.; Janssen, M.J.R.; Custers, J.A.E.; Slootbeek, P.H.J.; Kroeze, L.I.; Bruchertseifer, F.; Morgenstern, A.; et al. Clinical outcomes and molecular profiling of advanced metastatic castration-resistant prostate cancer patients treated with (225)Ac-PSMA-617 targeted alpha-radiation therapy. Urol. Oncol. 2020. [Google Scholar] [CrossRef]
- Ilhan, H.; Gosewisch, A.; Böning, G.; Völter, F.; Zacherl, M.; Unterrainer, M.; Bartenstein, P.; Todica, A.; Gildehaus, F.J. Response to (225)Ac-PSMA-I&T after failure of long-term (177)Lu-PSMA RLT in mCRPC. Eur. J. Nucl. Med. Mol. Imaging 2020, 1–2. [Google Scholar] [CrossRef]
- Zacherl, M.J.; Gildehaus, F.J.; Mittlmeier, L.; Boening, G.; Gosewisch, A.; Wenter, V.; Schmidt-Hegemann, N.S.; Belka, C.; Kretschmer, A.; Casuscelli, J.; et al. First clinical results for PSMA targeted alpha therapy using (225)Ac-PSMA-I&T in advanced mCRPC patients. J. Nucl. Med. 2020, jnumed-120. [Google Scholar] [CrossRef]
- Ackerman, N.L.; de la Fuente Rosales, L.; Falzone, N.; Vallis, K.A.; Bernal, M.A. Targeted alpha therapy with (212)Pb or (225)Ac: Change in RBE from daughter migration. Phys. Med. 2018, 51, 91–98. [Google Scholar] [CrossRef]
- Jaggi, J.S.; Seshan, S.V.; McDevitt, M.R.; LaPerle, K.; Sgouros, G.; Scheinberg, D.A. Renal tubulointerstitial changes after internal irradiation with alpha-particle-emitting actinium daughters. J. Am. Soc. Nephrol. 2005, 16, 2677–2689. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Kruijff, R.M.; Wolterbeek, H.T.; Denkova, A.G. A Critical Review of Alpha Radionuclide Therapy-How to Deal with Recoiling Daughters? Pharmaceuticals 2015, 8, 321–336. [Google Scholar] [CrossRef]
- Kozempel, J.; Mokhodoeva, O.; Vlk, M. Progress in Targeted Alpha-Particle Therapy. What We Learned about Recoils Release from In Vivo Generators. Molecules 2018, 23, 581. [Google Scholar] [CrossRef] [Green Version]
- Castillo Seoane, D.; de Saint-Hubert, M.; Crabbe, M.; Struelens, L.; Koole, M. Targeted alpha therapy: A critical review of translational dosimetry research with emphasis on actinium-225. Q. J. Nucl. Med. Mol. Imaging Off. Publ. Ital. Assoc. Nucl. Med. Int. Assoc. Radiopharmacol. 2020, 64, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Wester, H.J.; Schottelius, M. PSMA-Targeted Radiopharmaceuticals for Imaging and Therapy. Semin. Nucl. Med. 2019, 49, 302–312. [Google Scholar] [CrossRef]
- Pastorino, S.; Riondato, M.; Uccelli, L.; Giovacchini, G.; Giovannini, E.; Duce, V.; Ciarmiello, A. Toward the Discovery and Development of PSMA Targeted Inhibitors for Nuclear Medicine Applications. Curr. Radiopharm. 2020, 13, 63–79. [Google Scholar] [CrossRef] [PubMed]
- Lutje, S.; Heskamp, S.; Cornelissen, A.S.; Poeppel, T.D.; van den Broek, S.A.; Rosenbaum-Krumme, S.; Bockisch, A.; Gotthardt, M.; Rijpkema, M.; Boerman, O.C. PSMA Ligands for Radionuclide Imaging and Therapy of Prostate Cancer: Clinical Status. Theranostics 2015, 5, 1388–1401. [Google Scholar] [CrossRef] [Green Version]
- Lutje, S.; Slavik, R.; Fendler, W.; Herrmann, K.; Eiber, M. PSMA ligands in prostate cancer—Probe optimization and theranostic applications. Methods 2017, 130, 42–50. [Google Scholar] [CrossRef]
- Wustemann, T.; Bauder-Wust, U.; Schafer, M.; Eder, M.; Benesova, M.; Leotta, K.; Kratochwil, C.; Haberkorn, U.; Kopka, K.; Mier, W. Design of Internalizing PSMA-specific Glu-ureido-based Radiotherapeuticals. Theranostics 2016, 6, 1085–1095. [Google Scholar] [CrossRef] [Green Version]
- Eiber, M.; Fendler, W.P.; Rowe, S.P.; Calais, J.; Hofman, M.S.; Maurer, T.; Schwarzenboeck, S.M.; Kratowchil, C.; Herrmann, K.; Giesel, F.L. Prostate-Specific Membrane Antigen Ligands for Imaging and Therapy. J. Nucl. Med. 2017, 58, 67s–76s. [Google Scholar] [CrossRef] [Green Version]
- Tykvart, J.; Schimer, J.; Bařinková, J.; Pachl, P.; Poštová-Slavětínská, L.; Majer, P.; Konvalinka, J.; Šácha, P. Rational design of urea-based glutamate carboxypeptidase II (GCPII) inhibitors as versatile tools for specific drug targeting and delivery. Bioorg. Med. Chem. 2014, 22, 4099–4108. [Google Scholar] [CrossRef] [PubMed]
- Benesova, M.; Schafer, M.; Bauder-Wust, U.; Afshar-Oromieh, A.; Kratochwil, C.; Mier, W.; Haberkorn, U.; Kopka, K.; Eder, M. Preclinical Evaluation of a Tailor-Made DOTA-Conjugated PSMA Inhibitor with Optimized Linker Moiety for Imaging and Endoradiotherapy of Prostate Cancer. J. Nucl. Med. 2015, 56, 914–920. [Google Scholar] [CrossRef] [Green Version]
- Benesova, M.; Bauder-Wust, U.; Schafer, M.; Klika, K.D.; Mier, W.; Haberkorn, U.; Kopka, K.; Eder, M. Linker Modification Strategies To Control the Prostate-Specific Membrane Antigen (PSMA)-Targeting and Pharmacokinetic Properties of DOTA-Conjugated PSMA Inhibitors. J. Med. Chem. 2016, 59, 1761–1775. [Google Scholar] [CrossRef] [PubMed]
- Benesova, M.; Umbricht, C.A.; Schibli, R.; Muller, C. Albumin-Binding PSMA Ligands: Optimization of the Tissue Distribution Profile. Mol. Pharm. 2018, 15, 934–946. [Google Scholar] [CrossRef]
- Schmidt, A.; Wirtz, M.; Farber, S.F.; Osl, T.; Beck, R.; Schottelius, M.; Schwaiger, M.; Wester, H.J. Effect of Carbohydration on the Theranostic Tracer PSMA I&T. ACS Omega 2018, 3, 8278–8287. [Google Scholar]
- Barrett, J.A.; Coleman, R.E.; Goldsmith, S.J.; Vallabhajosula, S.; Petry, N.A.; Cho, S.; Armor, T.; Stubbs, J.B.; Maresca, K.P.; Stabin, M.G.; et al. First-in-man evaluation of 2 high-affinity PSMA-avid small molecules for imaging prostate cancer. J. Nucl. Med. 2013, 54, 380–387. [Google Scholar] [CrossRef] [Green Version]
- Weineisen, M.; Schottelius, M.; Simecek, J.; Eiber, M.; Schwaiger, M.; Wester, H. Development and first in human evaluation of PSMA I&T—A ligand for diagnostic imaging and endoradiotherapy of prostate cancer. J. Nucl. Med. 2014, 55, 1083. [Google Scholar]
- Eder, M.; Neels, O.; Müller, M.; Bauder-Wüst, U.; Remde, Y.; Schäfer, M.; Hennrich, U.; Eisenhut, M.; Afshar-Oromieh, A.; Haberkorn, U.; et al. Novel Preclinical and Radiopharmaceutical Aspects of [68Ga]Ga-PSMA-HBED-CC: A New PET Tracer for Imaging of Prostate Cancer. Pharmaceuticals 2014, 7, 779–796. [Google Scholar] [CrossRef]
- Carlucci, G.; Ippisch, R.; Slavik, R.; Mishoe, A.; Blecha, J.; Zhu, S. (68)Ga-PSMA-11 NDA Approval: A Novel and Successful Academic Partnership. J. Nucl. Med. 2021, 62, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Chatalic, K.L.; Heskamp, S.; Konijnenberg, M.; Molkenboer-Kuenen, J.D.; Franssen, G.M.; Clahsen-van Groningen, M.C.; Schottelius, M.; Wester, H.J.; van Weerden, W.M.; Boerman, O.C.; et al. Towards Personalized Treatment of Prostate Cancer: PSMA I&T, a Promising Prostate-Specific Membrane Antigen-Targeted Theranostic Agent. Theranostics 2016, 6, 849–861. [Google Scholar]
- Jilg, C.A.; Reichel, K.; Stoykow, C.; Rischke, H.C.; Bartholomä, M.; Drendel, V.; von Büren, M.; Schultze-Seemann, W.; Meyer, P.T.; Mix, M. Results from extended lymphadenectomies with [(111)In]PSMA-617 for intraoperative detection of PSMA-PET/CT-positive nodal metastatic prostate cancer. EJNMMI Res. 2020, 10, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Rauscher, I.; Maurer, T.; Souvatzoglou, M.; Beer, A.J.; Vag, T.; Wirtz, M.; Weirich, G.; Wester, H.J.; Gschwend, J.E.; Schwaiger, M.; et al. Intrapatient Comparison of 111In-PSMA I&T SPECT/CT and Hybrid 68Ga-HBED-CC PSMA PET in Patients With Early Recurrent Prostate Cancer. Clin. Nucl. Med. 2016, 41, e397–e402. [Google Scholar]
- Eppard, E.; de la Fuente, A.; Benesova, M.; Khawar, A.; Bundschuh, R.A.; Gartner, F.C.; Kreppel, B.; Kopka, K.; Essler, M.; Rosch, F. Clinical Translation and First In-Human Use of [(44)Sc]Sc-PSMA-617 for PET Imaging of Metastasized Castrate-Resistant Prostate Cancer. Theranostics 2017, 7, 4359–4369. [Google Scholar] [CrossRef]
- Umbricht, C.A.; Benesova, M.; Schmid, R.M.; Turler, A.; Schibli, R.; van der Meulen, N.P.; Muller, C. (44)Sc-PSMA-617 for radiotheragnostics in tandem with (177)Lu-PSMA-617-preclinical investigations in comparison with (68)Ga-PSMA-11 and (68)Ga-PSMA-617. EJNMMI Res. 2017, 7, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Khawar, A.; Eppard, E.; Sinnes, J.P.; Roesch, F.; Ahmadzadehfar, H.; Kürpig, S.; Meisenheimer, M.; Gaertner, F.C.; Essler, M.; Bundschuh, R.A. [44Sc]Sc-PSMA-617 Biodistribution and Dosimetry in Patients With Metastatic Castration-Resistant Prostate Carcinoma. Clin. Nucl. Med. 2018, 43, 323–330. [Google Scholar] [CrossRef]
- Kopka, K.; Benešová, M.; Bařinka, C.; Haberkorn, U.; Babich, J. Glu-Ureido-Based Inhibitors of Prostate-Specific Membrane Antigen: Lessons Learned During the Development of a Novel Class of Low-Molecular-Weight Theranostic Radiotracers. J. Nucl. Med. 2017, 58, 17s–26s. [Google Scholar] [CrossRef] [Green Version]
- Kelly, J.M.; Amor-Coarasa, A.; Ponnala, S.; Nikolopoulou, A.; Williams, C., Jr.; DiMagno, S.G.; Babich, J.W. Albumin-Binding PSMA Ligands: Implications for Expanding the Therapeutic Window. J. Nucl. Med. 2019, 60, 656–663. [Google Scholar] [CrossRef] [Green Version]
- Ling, X.; Latoche, J.D.; Choy, C.J.; Kurland, B.F.; Laymon, C.M.; Wu, Y.; Salamacha, N.; Shen, D.; Geruntho, J.J.; Rigatti, L.H.; et al. Preclinical Dosimetry, Imaging, and Targeted Radionuclide Therapy Studies of Lu-177-Labeled Albumin-Binding, PSMA-Targeted CTT1403. Mol. Imaging Biol. 2019, 22, 274–284. [Google Scholar] [CrossRef]
- Wang, Z.; Tian, R.; Niu, G.; Ma, Y.; Lang, L.; Szajek, L.P.; Kiesewetter, D.O.; Jacobson, O.; Chen, X. Single Low-Dose Injection of Evans Blue Modified PSMA-617 Radioligand Therapy Eliminates Prostate-Specific Membrane Antigen Positive Tumors. Bioconjug. Chem. 2018, 29, 3213–3221. [Google Scholar] [CrossRef] [PubMed]
- Kuo, H.T.; Merkens, H.; Zhang, Z.; Uribe, C.F.; Lau, J.; Zhang, C.; Colpo, N.; Lin, K.S.; Benard, F. Enhancing Treatment Efficacy of (177)Lu-PSMA-617 with the Conjugation of an Albumin-Binding Motif: Preclinical Dosimetry and Endoradiotherapy Studies. Mol. Pharm. 2018, 15, 5183–5191. [Google Scholar] [CrossRef]
- Umbricht, C.A.; Benesova, M.; Hasler, R.; Schibli, R.; van der Meulen, N.P.; Muller, C. Design and Preclinical Evaluation of an Albumin-Binding PSMA Ligand for (64)Cu-Based PET Imaging. Mol. Pharm. 2018, 15, 5556–5564. [Google Scholar] [CrossRef]
- Umbricht, C.A.; Benesova, M.; Schibli, R.; Muller, C. Preclinical Development of Novel PSMA-Targeting Radioligands: Modulation of Albumin-Binding Properties To Improve Prostate Cancer Therapy. Mol. Pharm. 2018, 15, 2297–2306. [Google Scholar] [CrossRef] [PubMed]
- Zang, J.; Fan, X.; Wang, H.; Liu, Q.; Wang, J.; Li, H.; Li, F.; Jacobson, O.; Niu, G.; Zhu, Z.; et al. First-in-human study of (177)Lu-EB-PSMA-617 in patients with metastatic castration-resistant prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Siow, A.; Kowalczyk, R.; Brimble, M.A.; Harris, P.W.R. Evolution of Peptide-Based Prostate-Specific Membrane Antigen (PSMA) Inhibitors: An Approach to Novel Prostate Cancer Therapeutics. Curr. Med. Chem. 2020. [Google Scholar] [CrossRef]
- Nováková, Z.; Foss, C.A.; Copeland, B.T.; Morath, V.; Baranová, P.; Havlínová, B.; Skerra, A.; Pomper, M.G.; Barinka, C. Novel Monoclonal Antibodies Recognizing Human Prostate-Specific Membrane Antigen (PSMA) as Research and Theranostic Tools. Prostate 2017, 77, 749–764. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Vallabhajosula, S.; Jhanwar, Y.; Ballman, K.V.; Hackett, A.; Emmerich, L.; Babich, J.; Sartor, O.; Harshman, L.C.; Beltran, H.; et al. Phase I dose-escalation study of 225Ac-J591 for progressive metastatic castration resistant prostate cancer (mCRPC). J. Clin. Oncol. 2017, 36, TPS399. [Google Scholar] [CrossRef]
- Liu, H.; Moy, P.; Kim, S.; Xia, Y.; Rajasekaran, A.; Navarro, V.; Knudsen, B.; Bander, N.H. Monoclonal antibodies to the extracellular domain of prostate-specific membrane antigen also react with tumor vascular endothelium. Cancer Res. 1997, 57, 3629–3634. [Google Scholar] [PubMed]
- Brown, L.G.; Wegner, S.K.; Wang, H.; Buhler, K.R.; Arfman, E.W.; Lange, P.H.; Vessella, R.L. A novel monoclonal antibody 107-1A4 with high prostate specificity: Generation, characterization of antigen expression, and targeting of human prostate cancer xenografts. Prostate Cancer Prostat. Dis. 1998, 1, 208–215. [Google Scholar] [CrossRef] [Green Version]
- Kraeber-Bodéré, F.; Rousseau, C.; Bodet-Milin, C.; Mathieu, C.; Guérard, F.; Frampas, E.; Carlier, T.; Chouin, N.; Haddad, F.; Chatal, J.F.; et al. Tumor immunotargeting using innovative radionuclides. Int. J. Mol. Sci. 2015, 16, 3932–3954. [Google Scholar] [CrossRef]
- Sartor, O.; Sharma, D. Radium and other alpha emitters in prostate cancer. Transl. Androl. Urol. 2018, 7, 436–444. [Google Scholar] [CrossRef]
- Dauer, L.T.; Williamson, M.J.; Humm, J.; O’Donoghue, J.; Ghani, R.; Awadallah, R.; Carrasquillo, J.; Pandit-Taskar, N.; Aksnes, A.K.; Biggin, C.; et al. Radiation safety considerations for the use of 223RaCl₂ DE in men with castration-resistant prostate cancer. Health Phys. 2014, 106, 494–504. [Google Scholar] [CrossRef] [Green Version]
- Henriksen, G.; Hoff, P.; Larsen, R.H. Evaluation of potential chelating agents for radium. Appl. Radiat. Isot. 2002, 56, 667–671. [Google Scholar] [CrossRef]
- Gott, M.; Yang, P.; Kortz, U.; Stephan, H.; Pietzsch, H.J.; Mamat, C. A (224)Ra-labeled polyoxopalladate as a putative radiopharmaceutical. Chem. Commun. 2019, 55, 7631–7634. [Google Scholar] [CrossRef]
- Mokhodoeva, O.; Vlk, M.; Málková, E.; Kukleva, E.; Mičolová, P.; Štamberg, K.; Šlouf, M.; Dzhenloda, R.; Kozempel, J. Study of 223Ra uptake mechanism by Fe3O4 nanoparticles: Towards new prospective theranostic SPIONs. J. Nanopart. Res. 2016, 10, 1–12. [Google Scholar] [CrossRef]
- Suchánková, P.; Kukleva, E.; Štamberg, K.; Nykl, P.; Vlk, M.; Kozempel, J. Study of 223Ra uptake mechanism on hydroxyapatite and titanium dioxide nanoparticles as a function of pH. RSC Adv. 2020, 10, 3659–3666. [Google Scholar] [CrossRef] [Green Version]
- Reissig, F.; Zarschler, K.; Hübner, R.; Pietzsch, H.J.; Kopka, K.; Mamat, C. Sub-10 nm Radiolabeled Barium Sulfate Nanoparticles as Carriers for Theranostic Applications and Targeted Alpha Therapy. ChemistryOpen 2020, 9, 797–805. [Google Scholar] [CrossRef]
- Piotrowska, A.; Leszczuk, E.; Bruchertseifer, F.; Morgenstern, A.; Bilewicz, A. Functionalized NaA nanozeolites labeled with (224,225)Ra for targeted alpha therapy. J. Nanopart. Res. 2013, 15, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suchánková, P.; Kukleva, E.; Štamberg, K.; Nykl, P.; Sakmár, M.; Vlk, M.; Kozempel, J. Determination, Modeling and Evaluation of Kinetics of (223)Ra Sorption on Hydroxyapatite and Titanium Dioxide Nanoparticles. Materials 2020, 13, 1915. [Google Scholar] [CrossRef] [Green Version]
- Khodadadi Yazdi, M.; Zarrintaj, P.; Hosseiniamoli, H.; Mashhadzadeh, A.H.; Saeb, M.R.; Ramsey, J.D.; Ganjali, M.R.; Mozafari, M. Zeolites for theranostic applications. J. Mater. Chem. B 2020, 8, 5992–6012. [Google Scholar] [CrossRef]
- Kratochwil, C.; Schmidt, K.; Afshar-Oromieh, A.; Bruchertseifer, F.; Rathke, H.; Morgenstern, A.; Haberkorn, U.; Giesel, F.L. Targeted alpha therapy of mCRPC: Dosimetry estimate of (213)Bismuth-PSMA-617. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Lindegren, S.; Albertsson, P.; Bäck, T.; Jensen, H.; Palm, S.; Aneheim, E. Realizing Clinical Trials with Astatine-211: The Chemistry Infrastructure. Cancer Biother. Radiopharm. 2020, 35, 425–436. [Google Scholar] [CrossRef] [Green Version]
- Makvandi, M.; Dupis, E.; Engle, J.W.; Nortier, F.M.; Fassbender, M.E.; Simon, S.; Birnbaum, E.R.; Atcher, R.W.; John, K.D.; Rixe, O.; et al. Alpha-Emitters and Targeted Alpha Therapy in Oncology: From Basic Science to Clinical Investigations. Target. Oncol. 2018, 13, 189–203. [Google Scholar] [CrossRef]
- Puttemans, J.; Lahoutte, T.; D’Huyvetter, M.; Devoogdt, N. Beyond the Barrier: Targeted Radionuclide Therapy in Brain Tumors and Metastases. Pharmaceutics 2019, 11, 376. [Google Scholar] [CrossRef] [Green Version]
- Langbein, T.; Chausse, G.; Baum, R.P. Salivary Gland Toxicity of PSMA Radioligand Therapy: Relevance and Preventive Strategies. J. Nucl. Med. 2018, 59, 1172–1173. [Google Scholar] [CrossRef] [Green Version]
- Khreish, F.; Ebert, N.; Ries, M.; Maus, S.; Rosar, F.; Bohnenberger, H.; Stemler, T.; Saar, M.; Bartholomä, M.; Ezziddin, S. (225)Ac-PSMA-617/(177)Lu-PSMA-617 tandem therapy of metastatic castration-resistant prostate cancer: Pilot experience. Eur. J. Nucl. Med. Mol. Imaging 2020, 47, 721–728. [Google Scholar] [CrossRef]
- Rathke, H.; Kratochwil, C.; Hohenberger, R.; Giesel, F.L.; Bruchertseifer, F.; Flechsig, P.; Morgenstern, A.; Hein, M.; Plinkert, P.; Haberkorn, U.; et al. Initial clinical experience performing sialendoscopy for salivary gland protection in patients undergoing (225)Ac-PSMA-617 RLT. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Baum, R.P.; Langbein, T.; Singh, A.; Shahinfar, M.; Schuchardt, C.; Volk, G.F.; Kulkarni, H. Injection of Botulinum Toxin for Preventing Salivary Gland Toxicity after PSMA Radioligand Therapy: An Empirical Proof of a Promising Concept. Nucl. Med. Mol. Imaging 2018, 52, 80–81. [Google Scholar] [CrossRef] [PubMed]
- Gallyamov, M.; Meyrick, D.; Barley, J.; Lenzo, N. Renal outcomes of radioligand therapy: Experience of 177lutetium—prostate-specific membrane antigen ligand therapy in metastatic castrate-resistant prostate cancer. Clin. Kidney J. 2019, 13, 1049–1055. [Google Scholar] [CrossRef] [Green Version]
- Ristau, B.T.; O’Keefe, D.S.; Bacich, D.J. The prostate-specific membrane antigen: Lessons and current clinical implications from 20 years of research. Urol. Oncol. 2014, 32, 272–279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Melville, G.; Allen, B.J. Cyclotron and linac production of Ac-225. Appl. Radiat. Isot. 2009, 67, 549–555. [Google Scholar] [CrossRef]
- Robertson, A.K.H.; Ramogida, C.F.; Schaffer, P.; Radchenko, V. Development of (225)Ac Radiopharmaceuticals: TRIUMF Perspectives and Experiences. Curr. Radiopharm. 2018, 11, 156–172. [Google Scholar] [CrossRef]
- Frantellizzi, V.; Cosma, L.; Brunotti, G.; Pani, A.; Spanu, A.; Nuvoli, S.; De Cristofaro, F.; Civitelli, L.; De Vincentis, G. Targeted Alpha Therapy with Thorium-227. Cancer Biother. Radiopharm. 2020, 35, 437–445. [Google Scholar] [CrossRef]
- Müller, C.; Vermeulen, C.; Köster, U.; Johnston, K.; Türler, A.; Schibli, R.; van der Meulen, N.P. Alpha-PET with terbium-149: Evidence and perspectives for radiotheragnostics. EJNMMI Radiopharm. Chem. 2017, 1, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Müller, C.; Domnanich, K.A.; Umbricht, C.A.; van der Meulen, N.P. Scandium and terbium radionuclides for radiotheranostics: Current state of development towards clinical application. Br. J. Radiol. 2018, 91, 20180074. [Google Scholar] [CrossRef]
- Beyer, G.J.; Miederer, M.; Vranjes-Durić, S.; Comor, J.J.; Künzi, G.; Hartley, O.; Senekowitsch-Schmidtke, R.; Soloviev, D.; Buchegger, F. Targeted alpha therapy in vivo: Direct evidence for single cancer cell kill using 149Tb-rituximab. Eur. J. Nucl. Med. Mol. Imaging 2004, 31, 547–554. [Google Scholar] [CrossRef]
- Westrom, S.; Generalov, R.; Bonsdorff, T.B.; Larsen, R.H. Preparation of (212)Pb-labeled monoclonal antibody using a novel (224)Ra-based generator solution. Nucl. Med. Biol. 2017, 51, 1–9. [Google Scholar] [CrossRef]
- Larsen, R.H. Radiopharmaceutical Solutions with Advantageous Properties. U.S. Patent 9433690B1, 6 September 2016. [Google Scholar]
- Chappell, L.L.; Dadachova, E.; Milenic, D.E.; Garmestani, K.; Wu, C.; Brechbiel, M.W. Synthesis, characterization, and evaluation of a novel bifunctional chelating agent for the lead isotopes 203Pb and 212Pb. Nucl. Med. Biol. 2000, 27, 93–100. [Google Scholar] [CrossRef]
- Yong, K.; Brechbiel, M. Application of (212)Pb for Targeted alpha-particle Therapy (TAT): Pre-clinical and Mechanistic Understanding through to Clinical Translation. AIMS Med. Sci. 2015, 2, 228–245. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.J.B.; Andersson, J.D.; Wuest, F. Targeted Alpha Therapy: Progress in Radionuclide Production, Radiochemistry, and Applications. Pharmaceutics 2020, 13, 49. [Google Scholar] [CrossRef]
- Gholami, Y.H.; Willowson, K.P.; Forwood, N.J.; Harvie, R.; Hardcastle, N.; Bromley, R.; Ryu, H.; Yuen, S.; Howell, V.M.; Kuncic, Z.; et al. Comparison of radiobiological parameters for (90)Y radionuclide therapy (RNT) and external beam radiotherapy (EBRT) in vitro. EJNMMI Phys. 2018, 5, 1–19. [Google Scholar] [CrossRef]
- Mirzadeh, S.; Kumar, K.; Gansow, O.A. The chemical fate of 212Bi-DOTA formed by b-decay of 212Pb(DOTA)2. Radiochim. Acta 1993, 60, 1–10. [Google Scholar]
- Maaland, A.F.; Saidi, A.; Torgue, J.; Heyerdahl, H.; Stallons, T.A.R.; Kolstad, A.; Dahle, J. Targeted alpha therapy for chronic lymphocytic leukaemia and non-Hodgkin’s lymphoma with the anti-CD37 radioimmunoconjugate 212Pb-NNV003. PLoS ONE 2020, 15, e0230526. [Google Scholar] [CrossRef] [Green Version]
- Kratochwil, C.; Giesel, F.L.; Heussel, C.P.; Kazdal, D.; Endris, V.; Nientiedt, C.; Bruchertseifer, F.; Kippenberger, M.; Rathke, H.; Leichsenring, J.; et al. Patients Resistant Against PSMA-Targeting α-Radiation Therapy Often Harbor Mutations in DNA Damage-Repair-Associated Genes. J. Nucl. Med. 2020, 61, 683–688. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.G.; O’Neill, E.; Habjan, C.; Cornelissen, B. Combination Strategies to Improve Targeted Radionuclide Therapy. J. Nucl. Med. 2020, 61, 1544–1552. [Google Scholar] [CrossRef]
- Kulkarni, H.; Zhang, J.; Langbein, T.; Schuchardt, C.; Singh, A.; Mueller, D.; Baum, R. Radioligand therapy using combination of Ac-225 and Lu-177 labelled PSMA ligands for progressive end-stage metastatic prostate cancer: Effective trade-off between response and toxicity. J. Nucl. Med. 2019, 60, 464. [Google Scholar]
- Roy, J.; Warner, B.; Basuli, F.; Williams, M.; Wong, K.J.; Ton, A.; Chiorini, J.; Choyke, P.; Lin, F.; Jagoda, E. Identifying an appropriate animal model to examine preservation of salivary function with PSMA targeted radiotherapies. J. Nucl. Med. 2018, 59, 1255. [Google Scholar]
- Simons, B.W.; Turtle, N.F.; Ulmert, D.H.; Abou, D.S.; Thorek, D.L.J. PSMA expression in the Hi-Myc model; extended utility of a representative model of prostate adenocarcinoma for biological insight and as a drug discovery tool. Prostate 2019, 79, 678–685. [Google Scholar] [CrossRef] [Green Version]
- Roy, J.; Warner, B.M.; Basuli, F.; Zhang, X.; Wong, K.; Pranzatelli, T.; Ton, A.T.; Chiorini, J.A.; Choyke, P.L.; Lin, F.I.; et al. Comparison of Prostate-Specific Membrane Antigen Expression Levels in Human Salivary Glands to Non-Human Primates and Rodents. Cancer Biother. Radiopharm. 2020, 35, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Rupp, N.J.; Umbricht, C.A.; Pizzuto, D.A.; Lenggenhager, D.; Töpfer, A.; Müller, J.; Muehlematter, U.J.; Ferraro, D.A.; Messerli, M.; Morand, G.B.; et al. First Clinicopathologic Evidence of a Non-PSMA-Related Uptake Mechanism for (68)Ga-PSMA-11 in Salivary Glands. J. Nucl. Med. 2019, 60, 1270–1276. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ma, D.; Olson, W.C.; Heston, W.D. In vitro and in vivo responses of advanced prostate tumors to PSMA ADC, an auristatin-conjugated antibody to prostate-specific membrane antigen. Mol. Cancer Ther. 2011, 10, 1728–1739. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.; Zammarchi, F.; Williams, D.G.; Havenith, C.E.G.; Monks, N.R.; Tyrer, P.; D’Hooge, F.; Fleming, R.; Vashisht, K.; Dimasi, N.; et al. Antitumor Activity of MEDI3726 (ADCT-401), a Pyrrolobenzodiazepine Antibody-Drug Conjugate Targeting PSMA, in Preclinical Models of Prostate Cancer. Mol. Cancer Ther. 2018, 17, 2176–2186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fendler, W.P.; Stuparu, A.D.; Evans-Axelsson, S.; Luckerath, K.; Wei, L.; Kim, W.; Poddar, S.; Said, J.; Radu, C.G.; Eiber, M.; et al. Establishing (177)Lu-PSMA-617 Radioligand Therapy in a Syngeneic Model of Murine Prostate Cancer. J. Nucl. Med. 2017, 58, 1786–1792. [Google Scholar] [CrossRef] [Green Version]
- Lin, M.; Ta, R.T.; Kairemo, K.; Le, D.B.; Ravizzini, G.C. Prostate-Specific Membrane Antigen-Targeted Radiopharmaceuticals in Diagnosis and Therapy of Prostate Cancer: Current Status and Future Perspectives. Cancer Biother. Radiopharm. 2020. [Google Scholar] [CrossRef]
- Weineisen, M.; Schottelius, M.; Simecek, J.; Baum, R.P.; Yildiz, A.; Beykan, S.; Kulkarni, H.R.; Lassmann, M.; Klette, I.; Eiber, M.; et al. 68Ga- and 177Lu-Labeled PSMA I&T: Optimization of a PSMA-Targeted Theranostic Concept and First Proof-of-Concept Human Studies. J. Nucl. Med. 2015, 56, 1169–1176. [Google Scholar] [PubMed] [Green Version]
- Banerjee, S.R.; Kumar, V.; Lisok, A.; Chen, J.; Minn, I.; Brummet, M.; Boinapally, S.; Cole, M.; Ngen, E.; Wharram, B.; et al. (177)Lu-labeled low-molecular-weight agents for PSMA-targeted radiopharmaceutical therapy. Eur. J. Nucl. Med. Mol. Imaging 2019, 46, 2545–2557. [Google Scholar] [CrossRef] [PubMed]
- Ruigrok, E.A.M.; van Vliet, N.; Dalm, S.U.; de Blois, E.; van Gent, D.C.; Haeck, J.; de Ridder, C.; Stuurman, D.; Konijnenberg, M.W.; van Weerden, W.M.; et al. Extensive preclinical evaluation of lutetium-177-labeled PSMA-specific tracers for prostate cancer radionuclide therapy. Eur. J. Nucl. Med. Mol. Imaging 2020, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Kulkarni, H.R.; Singh, A.; Schuchardt, C.; Niepsch, K.; Sayeg, M.; Leshch, Y.; Wester, H.J.; Baum, R.P. PSMA-Based Radioligand Therapy for Metastatic Castration-Resistant Prostate Cancer: The Bad Berka Experience Since 2013. J. Nucl. Med. 2016, 57, 97s–104s. [Google Scholar] [CrossRef] [Green Version]
- Hagemann, U.B.; Wickstroem, K.; Hammer, S.; Bjerke, R.M.; Zitzmann-Kolbe, S.; Ryan, O.B.; Karlsson, J.; Scholz, A.; Hennekes, H.; Mumberg, D.; et al. Advances in Precision Oncology: Targeted Thorium-227 Conjugates As a New Modality in Targeted Alpha Therapy. Cancer Biother. Radiopharm. 2020, 35, 497–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gosewisch, A.; Schleske, M.; Gildehaus, F.J.; Berg, I.; Kaiser, L.; Brosch, J.; Bartenstein, P.; Todica, A.; Ilhan, H.; Böning, G. Image-based dosimetry for (225)Ac-PSMA-I&T therapy using quantitative SPECT. Eur. J. Nucl. Med. Mol. Imaging 2020, 1–2. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Properties | Targeted Radionuclide Therapy | External Radiation Therapy | |
|---|---|---|---|
| α Emitters | β− Emitters | χ- and γ-rays | |
| Type | Helium nucleus | Electron | Photon |
| Mass (AMU) | 4 (heavy) | 0.0005 (light) | 0 (massless) |
| Speed of light | 6% (slow) | 98% (fast) | 100% (fast) |
| Initial energy | 4–9 MeV | 0.05–2.3 MeV | 0.035–3 MeV |
| Range in tissue | 0.04–0.1 mm | 0.05–12 mm | centimetres |
| LET | 50–230 keV/µm | 0.1–1.0 keV/µm | 0.2 keV/µm |
| DNA damage | Irrepairable (DSB) | Repairable (SSB) | Repairable (SSB) |
| Ionizing ability | Very high | Medium | Low |
| Number of DNA hits to kill cells | 1–5 | 100–2000 | >>1000 |
| Irradiation field | Whole-body | Whole-body | Region |
| Dose distribution | Very heterogeneous | Heterogeneous | Homogenous |
| Dose rate | <1 Gy/h | <1 Gy/h | 60–120 Gy/h, in 2 Gy fractions |
| Effect of oxygen on cell killing | Weak | Moderate | Strong |
| Bystander effect | Yes | Yes | Yes |
| Crossfire radiation | Yes | Yes | Yes |
| Radio- Nuclide | Half- Life | Main Production Method | Radio- Nuclide Availability | Emitted Particles | Total α Energy Emitted per Decay (MeV) | Range in Tissue (µm) | LET (keV/µm) | Emissions for Imaging |
|---|---|---|---|---|---|---|---|---|
| 149Tb | 4.1 h | Accelerator | Moderate | 1α, 1ε/2ε, 1β+/2β+ | 0.7 * | 25 | 140 | 165 and 730 keV |
| 211At | 7.2 h | Cyclotron | Moderate | 1α, 1ε | 6.9 | 55–80 | 71–230 | 77–92 keV |
| 212Pb/ 212Bi | 10.6 h | 224Ra generator | Very high | 1α, 2β− | 7.9 | 40–100 | 61–230 | 238 keV |
| 213Bi | 45.6 min | 225Ac generator | Moderate | 2α, 2β− | 8.5 | 40–100 | 65–230 | 440 and 1566 keV |
| 223Ra | 11.4 days | 227Th generator | High | 4α, 2β− | 26.8 | 46–70 | 71–230 | 84, 95, 144, 154 and 270 keV |
| 225Ac | 9.9 days | 229Th generator; cyclotron, accelerator, etc. in the future | Moderate | 4α, 2β− | 27.9 | 47–85 | 61–230 | 218 and 440 keV |
| 227Th | 18.7 days | 227Ac generator | High | 5α, 2β− | 32.8 | 50–70 | 71–230 | 84, 95, 236 and 270 keV |
| Characteristics | Small Molecules | Antibody Fragments | Antibodies |
|---|---|---|---|
| Molecular weight | <1.5 kDa | 15–110 kDa | 150 kDa |
| Structure | Peptidomimetic chain | One to four polypeptide chains | Complex; four polypeptide chains |
| Manufacture | Easy | Difficult | Difficult |
| Stability | Stable | Instable | Instable |
| In vivo half-life | Few hours | 0.5–30 h | 2–7 days |
| Pharmacokinetics | Rapid clearance from blood, rapid tissue penetration | Rapid to intermediate clearance from blood, rapid to intermediate tissue penetration | Circulates long in blood, slow tissue penetration, longer tumor retention |
| Excretion | Renal clearance | Renal clearance of Ab fragments <70 kDa | Hepatobiliary clearance and Fc-receptor- mediated recycling |
| Target binding to the extracellular domain | Enzymatic pocket of the catalytic domain | Apical region of the extracellular domain | Apical region of the extracellular domain |
| Immunogenicity | Seldom | Low | Expected |
| Examples | PSMA-617, PSMA-I&T, NG001 | IAB2M, scFvD2B, JVZ-008, PSMA6 and 30 | J591, 107-1A4, PSMA-TTC |
| Radio- Nuclide | PSMA Targeting Agent | Activity | Main Observations | References |
|---|---|---|---|---|
| Preclinical studies in vitro | ||||
| 213Bi | J591 (mAb) | 0–1.8 MBq/mL | Antitumor activity, growth delay of LNCaP-LN3 spheroids | Ballangrud et al., 2001 [81] |
| 211At | ABCPUP | NA | Binds to PC3 PIP cells | Vaidyanathan et al., 2009 [82] |
| 227Ac | 0–370 kBq/mL | Antitumor activity (LNCaP, Mat-Lu cells) | Bandekar et al., 2014 [83] | |
| 223Ra | NA-silane-PEG-D2B (mAb) | 0–20 kBq/mL | Antitumor activity, LD50 ≈ 2.5kBq/mL (C4-2 cells) | Czerwińska et al., 2020 [84] |
| Preclinical studies in vivo | ||||
| 149Tb | PSMA-617 | 2 × 3 MBq | 37%ID/g (tumor targeting at 1 h, subcutaneous, PC3 PIP cells); antitumor activity, TI ≈ 1.8 | Umbricht et al., 2019 [85] |
| 211At | 107-1A4 (mAb) | 370 kBq | PSA decline (intratibial, C4-2B cells) | Wilbur et al., 2009 [86] |
| 107-1A4 Fab’ | 740 kBq | 25%ID/g (tumor targeting at 1 h, subcutaneous, LNCaP cells) | Wilbur et al., 2011 [87] | |
| PSMA 6 | 740 kBq | 14%ID/g (tumor targeting at 1 h, subcutaneous, PC3 PIP cells); antitumor activity, TI ≈ 2.1; delayed nephropathy dose limiting; dehalogenation in vivo | Kiess et al., 2016 [88] | |
| 131I as a surrogate for 211At | RPS-027 | NA | Dual targeting to PSMA and albumin; 9%ID/g (tumor targeting at 1 h, subcutaneous, LNCaP cells) | Kelly et al., 2017 [89] |
| 16b | NA | 15%ID/g (tumor targeting at 1 h, subcutaneous, C4-2B cells) | Li et al., 2020 [90] | |
| 212Pb/ 212Bi | CA009, CA012 | NA | 25%ID/g (tumor targeting at 1 h (203Pb) subcutaneous, C4-2 cells) | Dos Santos et al., 2019 [91] |
| L2 | 1.5 and 3.7 MBq | 22%ID/g (tumor targeting at 1 h (203Pb), subcutaneous, PC3 PIP cells); antitumor activity, TI ≈ 1.9 and TI ≈ 3 | Banerjee et al., 2020 [92] | |
| NG001 | 320 kBq | 22%ID/g (tumor targeting at 1 h, subcutaneous, C4-2 cells); antitumor activity, TI * ≈ 2.3 | Larsen, 2019 [93]; Stenberg et al., 2020 [94,95] | |
| 213Bi | J591 (mAb) | 3.3 MBq | Antitumor activity, TI ≈ 1.8 (subcutaneous, LNCaP cells) | McDevitt et al., 2000 [96] |
| 3.7 MBq | Antitumor activity, inhibition of tumor growth in mice (subcutaneous, LN3 cells) | Li et al., 2002 [97] | ||
| PSMA I&T | 5.4–6.6 MBq | 5.8%ID/g (tumor targeting at 1 h, subcutaneous, LNCaP cells) | Nonnekens et al., 2017 [98] | |
| JVZ-008 (nanobody) | 4.5–5.4 MBq | 2.7%ID/g (tumor targeting at 1 h, subcutaneous, LNCaP cells) | ||
| 225Ac | PSMA-617 | 40 kBq | Antitumor activity (subcutaneous, C4-2 cells); weight loss at 100 kBq | Meyer et al., 2019 [99] |
| 40 kBq | Antitumor activity (intravenous, C4-2 cells), TI ≈ 3.9 | Stuparu et al., 2020 [100] | ||
| 40 kBq | Antitumor activity, (subcutaneous, RM1-PSMA+++ cells) | Current et al., 2020 [101] | ||
| 30 kBq | Antitumor activity (subcutaneous, RM1-PGLS cells), TI ≈ 1.2 | Czernin et al., 2020 [102] | ||
| RPS-074 | 148 kBq | 6%ID/g (tumor targeting at 4 h, subcutaneous, LNCaP cells); antitumor activity, complete response in 86% | Kelly et al., 2019 [103] | |
| 227Th | PSMA-TTC (mAb) | 100–500 kBq/kg | 20%ID/g and 37%ID/g (tumor targeting after 3 and 7 days, respectively, subcutaneous, MDA-PCa-2b cells); antitumor activity | Hammer et al., 2020 [104] |
| PSMA- TAT | n | Activity per Cycle | PSA Decline After TAT (Patients) | Median PFS/OS (Months) | Toxicity | References | |
|---|---|---|---|---|---|---|---|
| ≤0% | ≥50% | ||||||
| 213Bi- PSMA- 617 | 1 | 296 MBq | 100% (1/1) | NA | NA | Sathekge et al., 2017 [105] | |
| 225Ac- PSMA- 617 | 2 | 100 kBq/kg | 100% (2/2) | NA | Xerostomia | Kratochwil et al., 2016 [42] | |
| 14 | 50–200 kBq/kg | 22% (2/9) | 44% (4/9) | NA/8.5 | Xerostomia | Kratochwil et al., 2017 [106] | |
| 40 | 100 kBq/kg | 13% (5/40) | 63% (24/38) | NA/>12 | Xerostomia | Kratochwil et al., 2018 [107] | |
| 1 | 8 MBq | 100% (1/1) | NA | NA | Sathekge et al., 2019 [108] | ||
| 17 | 8–4 MBq | 6% (1/17) | 88% (15/17) | NA | Xerostomia | Sathekge et al., 2019 [109] | |
| 1 | 8–6 MBq | 100% (1/1) | NA | Xerostomia xero- phthalmia | De Medeiros et al., 2019 [110] | ||
| 73 | 8–4 MBq | 18% (13/73) | 70% (51/73) | 15.2/18.0 | NA | Sathekge et al., 2020 [111] | |
| 26 | 8–4 MBq | 11% (3/26) | 65% (17/26) | 3.5/7.7 | Xerostomia, anemia, leucopenia, thrombopenia | Feuerecker et al., 2020 [112] | |
| 28 | 100 kBq/kg | 18% (5/28) | 39% (11/28) | 12/17 | Transient fatigue, xerostomia | Yadav et al., 2020 [113] | |
| 2 | NA | NA | NA | NA | Chronic kidney disease | Pelletier et al., 2021[114] | |
| 13 | 8–6 MBq | 15% (2/13) | 69% (9/13) | NA/8.5 | Xerostomia | Van der Doelen et al., 2020 [115] | |
| 225Ac- PSMA I&T | 1 | 8 MBq | 100% (1/1) | NA | Xerostomia | Ilhan et al., 2020 [116] | |
| 14 | 7.8 MBq | 21% (3/14) | 50% (7/14) | NA | Xerostomia | Zacherl etal, 2020 [117] | |
| Trial ID | Phase | TAT | Number of Patients | Period | Sponsor |
|---|---|---|---|---|---|
| NCT03276572 | 1 | 225Ac-J591 | 42 | 2017–2021 | Weill Medical College of Cornell University |
| NCT04506567 | 1/2 | 225Ac-J591 | 105 | 2020–2025 | Weill Medical College of Cornell University |
| NCT04225910 | 1 | 225Ac-PSMA | 20 | 2019–2021 | Xinhua Hospital, Shanghai Jiao Tong University School of Medicine |
| NCT04597411 | 1 | 225Ac-PSMA-617 | 30 | 2021–2022 | Novartis Pharmaceuticals |
| NCT03724747 | 1 | BAY 2315497 (227Th-mAb) | 157 | 2018–2023 | Bayer |
| Cell Line | Number of PSMA Per Cell | References |
|---|---|---|
| DU145 | Negative | [199,200] |
| PC3 | Negative | [199,200] |
| 22Rv1 | 15,000 | [101] |
| RM1-h-PSMA | 19,000 | [201] |
| LS174T-PSMA | 43,000 | [138] |
| PSMA++ RM1 | 49,000 | [101] |
| RM1-PGLS | 56,000 | [201] |
| MDA PCa2b | 118,000 | [200] |
| LNCaP | 126,000–250,000 | [96,138,199] |
| C4-2 | 102,000–255,000 | [101,199,201] |
| PC3 PIP | 552,000 | [101] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juzeniene, A.; Stenberg, V.Y.; Bruland, Ø.S.; Larsen, R.H. Preclinical and Clinical Status of PSMA-Targeted Alpha Therapy for Metastatic Castration-Resistant Prostate Cancer. Cancers 2021, 13, 779. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040779
Juzeniene A, Stenberg VY, Bruland ØS, Larsen RH. Preclinical and Clinical Status of PSMA-Targeted Alpha Therapy for Metastatic Castration-Resistant Prostate Cancer. Cancers. 2021; 13(4):779. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040779
Chicago/Turabian StyleJuzeniene, Asta, Vilde Yuli Stenberg, Øyvind Sverre Bruland, and Roy Hartvig Larsen. 2021. "Preclinical and Clinical Status of PSMA-Targeted Alpha Therapy for Metastatic Castration-Resistant Prostate Cancer" Cancers 13, no. 4: 779. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040779