
Molecular Profiling of 22 Primary Atypical Meningiomas Shows the Prognostic Significance of 18q Heterozygous Loss and CDKN2A/B Homozygous Deletion on Recurrence-Free Survival

 ,
,  , , , ,
, , , ,  and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Cases
2.2. Ethical issues
2.3. Clinical Data
2.4. Mutational and Copy Number Variation Status of 409 Cancer Genes
2.5. Tumor Mutational Burden
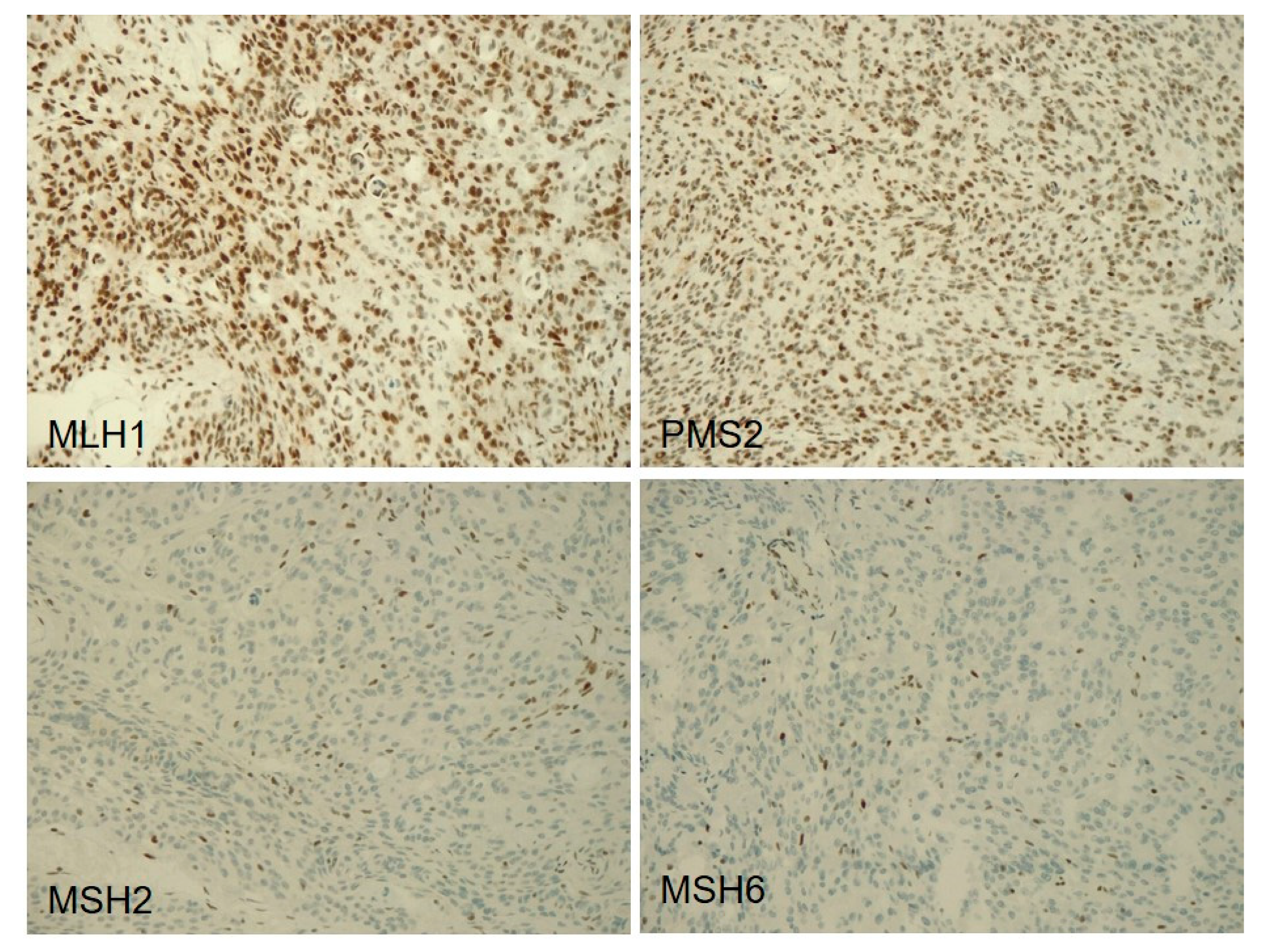
2.6. Immunohistochemistry of DNA Mismatch Repair Proteins
2.7. Microsatellite Instability Analysis
2.8. Statistical Analyses
3. Results
3.1. Cases
3.2. Mutational and Copy Number Variation Status of 409 Cancer Genes
3.3. Chromosomal Alterations
3.4. Tumor Mutational Burden
3.5. Immunohistochemistry of DNA Mismatch Repair Proteins and Microsatellite Instability Analysis
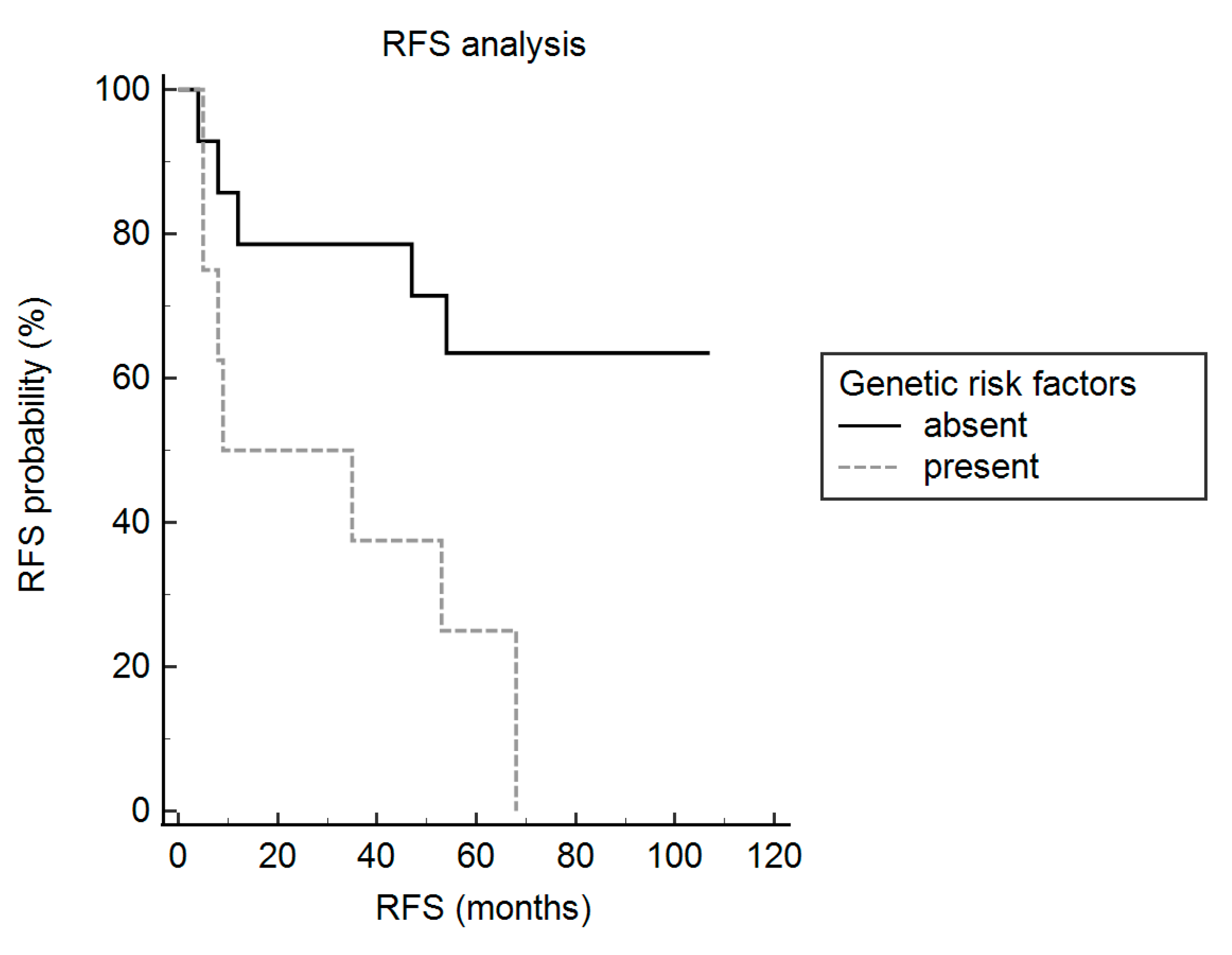
3.6. Recurrence-free Survival Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Louis, D.N.; Ohgaki, H.; Wisteler, O.D.; Cavenee, W.K.; Ellison, D.W.; Figarella-Branger, D.; Perry, A.; Refeinberger, G.; Von Deimling, A. Who Classification Of Tumors Of The Central Nervous System; Iarc: Lyon, France, 2007. [Google Scholar]
- Simpson, D. The Recurrence Of Intracranial Meningiomas After Surgical Treatment. J. Neurol. Neurosurg. Psychiatry 1957, 20, 22–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Przybylowski, C.J.; Hendricks, B.K.; Frisoli, F.A.; Zhao, X.; Cavallo, C.; Borba Moreira, L.; Gandhi, S.; Sanai, N.; Almefty, K.K.; Lawton, M.T.; et al. Prognostic Value Of The Simpson Grading Scale In Modern Meningioma Surgery: Barrow Neurological Institute Experience. J. Neurosurg. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Goldbrunner, R.; Minniti, G.; Preusser, M.; Jenkinson, M.D.; Sallabanda, K.; Houdart, E.; Von Deimling, A.; Stavrinou, P.; Lefranc, F.; Lund-Johansen, M.; et al. Eano Guidelines For The Diagnosis And Treatment Of Meningiomas. Lancet Oncol. 2016, 17, 383–391. [Google Scholar] [CrossRef] [Green Version]
- Hemmati, S.M.; Ghadjar, P.; Grun, A.; Badakhshi, H.; Zschaeck, S.; Senger, C.; Acker, G.; Misch, M.; Budach, V.; Kaul, D. Adjuvant Radiotherapy Improves Progression-Free Survival In Intracranial Atypical Meningioma. Radiat. Oncol. 2019, 14, 160. [Google Scholar] [CrossRef] [Green Version]
- Weber, D.C.; Ares, C.; Villa, S.; Peerdeman, S.M.; Renard, L.; Baumert, B.G.; Lucas, A.; Veninga, T.; Pica, A.; Jefferies, S.; et al. Adjuvant Postoperative High-Dose Radiotherapy For Atypical And Malignant Meningioma: A Phase-Ii Parallel Non-Randomized And Observation Study (Eortc 22042–26042). Radiother. Oncol. 2018, 128, 260–265. [Google Scholar] [CrossRef] [Green Version]
- Fioravanzo, A.; Caffo, M.; Di Bonaventura, R.; Gardiman, M.P.; Ghimenton, C.; Ius, T.; Maffeis, V.; Martini, M.; Nicolato, A.; Pallini, R.; et al. A Risk Score Based On 5 Clinico-Pathological Variables Predicts Recurrence Of Atypical Meningiomas. J. Neuropathol. Exp. Neurol. 2020, 79, 500–507. [Google Scholar] [CrossRef]
- Zang, K.D. Meningioma: A Cytogenetic Model Of A Complex Benign Human Tumor, Including Data On 394 Karyotyped Cases. Cytogenet. Cell Genet. 2001, 93, 207–220. [Google Scholar] [CrossRef]
- Williams, E.A.; Santagata, S.; Wakimoto, H.; Shankar, G.M.; Barker, F.G., 2nd; Sharaf, R.; Reddy, A.; Spear, P.; Alexander, B.M.; Ross, J.S.; et al. Distinct Genomic Subclasses Of High-Grade/Progressive Meningiomas: Nf2-Associated, Nf2-Exclusive, And Nf2-Agnostic. Acta Neuropathol. Commun. 2020, 8, 171. [Google Scholar] [CrossRef] [PubMed]
- Cordova, C.; Kurz, S.C. Advances In Molecular Classification And Therapeutic Opportunities In Meningiomas. Curr. Oncol. Rep. 2020, 22, 84. [Google Scholar] [CrossRef]
- Goutagny, S.; Yang, H.W.; Zucman-Rossi, J.; Chan, J.; Dreyfuss, J.M.; Park, P.J.; Black, P.M.; Giovannini, M.; Carroll, R.S.; Kalamarides, M. Genomic Profiling Reveals Alternative Genetic Pathways Of Meningioma Malignant Progression Dependent On The Underlying Nf2 Status. Clin. Cancer Res. 2010, 16, 4155–4164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mawrin, C.; Perry, A. Pathological Classification And Molecular Genetics Of Meningiomas. J. Neurooncol. 2010, 99, 379–391. [Google Scholar] [CrossRef]
- Youngblood, M.W.; Duran, D.; Montejo, J.D.; Li, C.; Omay, S.B.; Ozduman, K.; Sheth, A.H.; Zhao, A.Y.; Tyrtova, E.; Miyagishima, D.F.; et al. Correlations Between Genomic Subgroup And Clinical Features In A Cohort Of More Than 3000 Meningiomas. J. Neurosurg. 2019, 1–10. [Google Scholar] [CrossRef]
- Brastianos, P.K.; Horowitz, P.M.; Santagata, S.; Jones, R.T.; Mckenna, A.; Getz, G.; Ligon, K.L.; Palescandolo, E.; Van Hummelen, P.; Ducar, M.D.; et al. Genomic Sequencing Of Meningiomas Identifies Oncogenic Smo And Akt1 Mutations. Nat. Genet. 2013, 45, 285–289. [Google Scholar] [CrossRef] [PubMed]
- Clark, V.E.; Erson-Omay, E.Z.; Serin, A.; Yin, J.; Cotney, J.; Ozduman, K.; Avsar, T.; Li, J.; Murray, P.B.; Henegariu, O.; et al. Genomic Analysis Of Non-Nf2 Meningiomas Reveals Mutations In Traf7, Klf4, Akt1, And Smo. Science 2013, 339, 1077–1080. [Google Scholar] [CrossRef] [Green Version]
- Bi, W.L.; Greenwald, N.F.; Abedalthagafi, M.; Wala, J.; Gibson, W.J.; Agarwalla, P.K.; Horowitz, P.; Schumacher, S.E.; Esaulova, E.; Mei, Y.; et al. Genomic Landscape Of High-Grade Meningiomas. Npj. Genom. Med. 2017, 2. [Google Scholar] [CrossRef]
- Harmanci, A.S.; Youngblood, M.W.; Clark, V.E.; Coskun, S.; Henegariu, O.; Duran, D.; Erson-Omay, E.Z.; Kaulen, L.D.; Lee, T.I.; Abraham, B.J.; et al. Integrated Genomic Analyses Of De Novo Pathways Underlying Atypical Meningiomas. Nat. Commun. 2018, 9, 16215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domingues, P.H.; Sousa, P.; Otero, A.; Goncalves, J.M.; Ruiz, L.; De Oliveira, C.; Lopes, M.C.; Orfao, A.; Tabernero, M.D. Proposal For A New Risk Stratification Classification For Meningioma Based On Patient Age, Who Tumor Grade, Size, Localization, And Karyotype. Neuro. Oncol. 2014, 16, 735–747. [Google Scholar] [CrossRef] [Green Version]
- Kishida, Y.; Natsume, A.; Kondo, Y.; Takeuchi, I.; An, B.; Okamoto, Y.; Shinjo, K.; Saito, K.; Ando, H.; Ohka, F.; et al. Epigenetic Subclassification Of Meningiomas Based On Genome-Wide Dna Methylation Analyses. Carcinogenesis 2012, 33, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Olar, A.; Wani, K.M.; Wilson, C.D.; Zadeh, G.; Demonte, F.; Jones, D.T.; Pfister, S.M.; Sulman, E.P.; Aldape, K.D. Global Epigenetic Profiling Identifies Methylation Subgroups Associated With Recurrence-Free Survival In Meningioma. Acta Neuropathol. 2017, 133, 431–444. [Google Scholar] [CrossRef] [Green Version]
- Sahm, F.; Schrimpf, D.; Olar, A.; Koelsche, C.; Reuss, D.; Bissel, J.; Kratz, A.; Capper, D.; Schefzyk, S.; Hielscher, T.; et al. Tert Promoter Mutations And Risk Of Recurrence In Meningioma. J. Natl. Cancer Inst. 2016, 108. [Google Scholar] [CrossRef]
- Aizer, A.A.; Abedalthagafi, M.; Bi, W.L.; Horvath, M.C.; Arvold, N.D.; Al-Mefty, O.; Lee, E.Q.; Nayak, L.; Rinne, M.L.; Norden, A.D.; et al. A Prognostic Cytogenetic Scoring System To Guide The Adjuvant Management Of Patients With Atypical Meningioma. Neuro. Oncol. 2016, 18, 269–274. [Google Scholar] [CrossRef] [Green Version]
- Simbolo, M.; Gottardi, M.; Corbo, V.; Fassan, M.; Mafficini, A.; Malpeli, G.; Lawlor, R.T.; Scarpa, A. Dna Qualification Workflow For Next Generation Sequencing Of Histopathological Samples. PLoS ONE 2013, 8, 62692. [Google Scholar] [CrossRef] [Green Version]
- Cingolani, P.; Patel, V.M.; Coon, M.; Nguyen, T.; Land, S.J.; Ruden, D.M.; Lu, X. Using Drosophila Melanogaster As A Model For Genotoxic Chemical Mutational Studies With A New Program, Snpsift. Front Genet. 2012, 3, 35. [Google Scholar] [CrossRef] [Green Version]
- Mclaren, W.; Pritchard, B.; Rios, D.; Chen, Y.; Flicek, P.; Cunningham, F. Deriving The Consequences Of Genomic Variants With The Ensembl Api And Snp Effect Predictor. Bioinformatics 2010, 26, 2069–2070. [Google Scholar] [CrossRef]
- Robinson, J.T.; Thorvaldsdottir, H.; Winckler, W.; Guttman, M.; Lander, E.S.; Getz, G.; Mesirov, J.P. Integrative Genomics Viewer. Nat. Biotechnol. 2011, 29, 24–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boeva, V.; Popova, T.; Lienard, M.; Toffoli, S.; Kamal, M.; Le Tourneau, C.; Gentien, D.; Servant, N.; Gestraud, P.; Rio Frio, T.; et al. Multi-Factor Data Normalization Enables The Detection Of Copy Number Aberrations In Amplicon Sequencing Data. Bioinformatics 2014, 30, 3443–3450. [Google Scholar] [CrossRef] [Green Version]
- Abedalthagafi, M.; Bi, W.L.; Aizer, A.A.; Merrill, P.H.; Brewster, R.; Agarwalla, P.K.; Listewnik, M.L.; Dias-Santagata, D.; Thorner, A.R.; Van Hummelen, P.; et al. Oncogenic Pi3k Mutations Are As Common As Akt1 And Smo Mutations In Meningioma. Neuro. Oncol. 2016, 18, 649–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, S.Q.; Cai, C.; Murphy, R.K.; Dewees, T.; Dacey, R.G.; Grubb, R.L.; Rich, K.M.; Zipfel, G.J.; Dowling, J.L.; Leuthardt, E.C.; et al. Management Of Atypical Cranial Meningiomas, Part 2: Predictors Of Progression And The Role Of Adjuvant Radiation After Subtotal Resection. Neurosurgery 2014, 75, 356–363; Discussion 363. [Google Scholar] [CrossRef] [Green Version]
- Mcnulty, S.N.; Schwetye, K.; Goldstein, M.; Carter, J.; Schmidt, R.E.; Ansstas, G.; Tsien, C.I.; Kim, A.H.; Dahiya, S. Analysis Of Point Mutations And Copy Number Variation In Grade Ii And Iii Meningioma. Exp. Mol. Pathol. 2018, 105, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Yuzawa, S.; Nishihara, H.; Yamaguchi, S.; Mohri, H.; Wang, L.; Kimura, T.; Tsuda, M.; Tanino, M.; Kobayashi, H.; Terasaka, S.; et al. Clinical Impact Of Targeted Amplicon Sequencing For Meningioma As A Practical Clinical-Sequencing System. Mod. Pathol. 2016, 29, 708–716. [Google Scholar] [CrossRef]
- Elisei, R.; Tacito, A.; Ramone, T.; Ciampi, R.; Bottici, V.; Cappagli, V.; Viola, D.; Matrone, A.; Lorusso, L.; Valerio, L.; et al. Twenty-Five Years Experience On Ret Genetic Screening On Hereditary Mtc: An Update On The Prevalence Of Germline Ret Mutations. Genes (Basel) 2019, 10, 698. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.P.; Ma, J.M.; Du, Z.F.; Ying, R.B.; Fei, J.; Jin, H.Y.; Han, J.S.; Wang, J.Q.; Chen, X.L.; Chen, C.Y.; et al. Ret Germline Mutations Identified By Exome Sequencing In A Chinese Multiple Endocrine Neoplasia Type 2a/Familial Medullary Thyroid Carcinoma Family. PLoS ONE 2011, 6, 20353. [Google Scholar] [CrossRef]
- Tamanaha, R.; Camacho, C.P.; Ikejiri, E.S.; Maciel, R.M.; Cerutti, J.M. Y791f Ret Mutation And Early Onset Of Medullary Thyroid Carcinoma In A Brazilian Kindred: Evaluation Of Phenotype-Modifying Effect Of Germline Variants. Clin. Endocrinol. (Oxf) 2007, 67, 806–808. [Google Scholar] [CrossRef] [PubMed]
- Dunn, I.F.; Du, Z.; Touat, M.; Sisti, M.B.; Wen, P.Y.; Umeton, R.; Dubuc, A.M.; Ducar, M.; Canoll, P.D.; Severson, E.; et al. Mismatch Repair Deficiency In High-Grade Meningioma: A Rare But Recurrent Event Associated With Dramatic Immune Activation And Clinical Response To Pd-1 Blockade. Jco. Precis. Oncol. 2018, 2018, 15–30. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.B.; Light, N.; Fabrizio, D.; Zatzman, M.; Fuligni, F.; De Borja, R.; Davidson, S.; Edwards, M.; Elvin, J.A.; Hodel, K.P.; et al. Comprehensive Analysis Of Hypermutation In Human Cancer. Cell 2017, 171, 1042–1056 E1010. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Le, D.T.; Durham, J.N.; Smith, K.N.; Wang, H.; Bartlett, B.R.; Aulakh, L.K.; Lu, S.; Kemberling, H.; Wilt, C.; Luber, B.S.; et al. Mismatch Repair Deficiency Predicts Response Of Solid Tumors To Pd-1 Blockade. Science 2017, 357, 409–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barresi, V.; Simbolo, M.; Mafficini, A.; Piredda, M.L.; Caffo, M.; Cardali, S.M.; Germano, A.; Cingarlini, S.; Ghimenton, C.; Scarpa, A. Ultra-Mutation In Idh Wild-Type Glioblastomas Of Patients Younger Than 55 Years Is Associated With Defective Mismatch Repair, Microsatellite Instability, And Giant Cell Enrichment. Cancers (Basel) 2019, 11, 1279. [Google Scholar] [CrossRef] [Green Version]
- Luchini, C.; Bibeau, F.; Ligtenberg, M.J.L.; Singh, N.; Nottegar, A.; Bosse, T.; Miller, R.; Riaz, N.; Douillard, J.Y.; Andre, F.; et al. Esmo Recommendations On Microsatellite Instability Testing For Immunotherapy In Cancer, And Its Relationship With Pd-1/Pd-L1 Expression And Tumour Mutational Burden: A Systematic Review-Based Approach. Ann. Oncol. 2019, 30, 1232–1243. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, G.; Barresi, V.; Indraccolo, S.; Simbolo, M.; Fassan, M.; Mandruzzato, S.; Simonelli, M.; Caccese, M.; Pizzi, M.; Fassina, A.; et al. Pembrolizumab Activity In Recurrent High-Grade Gliomas With Partial Or Complete Loss Of Mismatch Repair Protein Expression: A Monocentric, Observational And Prospective Pilot Study. Cancers (Basel) 2020, 12, 2283. [Google Scholar] [CrossRef]
- Ma, J.; Hong, Y.; Chen, W.; Li, D.; Tian, K.; Wang, K.; Yang, Y.; Zhang, Y.; Chen, Y.; Song, L.; et al. High Copy-Number Variation Burdens In Cranial Meningiomas From Patients With Diverse Clinical Phenotypes Characterized By Hot Genomic Structure Changes. Front. Oncol. 2020, 10, 1382. [Google Scholar] [CrossRef]
- Yang, H.W.; Kim, T.M.; Song, S.S.; Shrinath, N.; Park, R.; Kalamarides, M.; Park, P.J.; Black, P.M.; Carroll, R.S.; Johnson, M.D. Alternative Splicing Of Chek2 And Codeletion With Nf2 Promote Chromosomal Instability In Meningioma. Neoplasia. 2012, 14, 20–28. [Google Scholar] [CrossRef] [Green Version]
- Guyot, A.; Duchesne, M.; Robert, S.; Lia, A.S.; Derouault, P.; Scaon, E.; Lemnos, L.; Salle, H.; Durand, K.; Labrousse, F. Analysis Of Cdkn2a Gene Alterations In Recurrent And Non-Recurrent Meningioma. J. Neurooncol. 2019, 145, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Sahm, F.; Schrimpf, D.; Stichel, D.; Jones, D.T.W.; Hielscher, T.; Schefzyk, S.; Okonechnikov, K.; Koelsche, C.; Reuss, D.E.; Capper, D.; et al. Dna Methylation-Based Classification And Grading System For Meningioma: A Multicentre, Retrospective Analysis. Lancet. Oncol. 2017, 18, 682–694. [Google Scholar] [CrossRef] [Green Version]
- Patel, A.J.; Wan, Y.W.; Al-Ouran, R.; Revelli, J.P.; Cardenas, M.F.; Oneissi, M.; Xi, L.; Jalali, A.; Magnotti, J.F.; Muzny, D.M.; et al. Molecular Profiling Predicts Meningioma Recurrence And Reveals Loss Of Dream Complex Repression In Aggressive Tumors. Proc. Natl. Acad. Sci. USA 2019, 116, 21715–21726. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Case | Sex | Age | Site | Histological Group | Sheeting | Necrosis | TMB (muts/Mb) | Simpson Grade | Recurrence | DFS (months) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1M | F | 68 | SB | Brain Invasion | no | Absent | 12.68 | 1 | no | 54 |
| 2M | M | 88 | C | Brain Invasion | no | Absent | 12.21 | 1 | no | 107 |
| 3M | F | 83 | C | Brain Invasion | no | Present | 8.7 | 1 | yes | 9 |
| 4M | F | 70 | S | Brain Invasion | no | Absent | 11.62 | 1 | no | 78 |
| 5M | M | 69 | S | Brain Invasion | no | Absent | 2.19 | 1 | yes | 53 |
| 6M | F | 67 | C | Brain Invasion | no | Present | 10.42 | 1 | yes | 68 |
| 7M | F | 71 | SB | Brain Invasion | no | Present | 12.19 | 2 | yes | 54 |
| 8M | F | 51 | C | Brain Invasion | no | Present | 6.56 | 1 | yes | 47 |
| 9M | F | 36 | C | High mitotic index | no | Present | 9.32 | 1 | no | 62 |
| 10M | F | 50 | C | High mitotic index | yes | Present | 6.61 | 1 | no | 61 |
| 11M | M | 68 | C | High mitotic index | yes | Present | 10.25 | 3 | yes | 35 |
| 12M | F | 44 | C | High mitotic index | yes | Absent | 11.89 | 1 | no | 47 |
| 13M | M | 56 | C | High mitotic index | no | Present | 10.55 | 2 | yes | 68 |
| 14M | M | 63 | S | High mitotic index | yes | Present | 9.76 | 3 | yes | 4 |
| 15M | M | 60 | C | High mitotic index | no | Absent | 8.05 | 1 | yes | 8 |
| 16M | M | 57 | C | High mitotic index | yes | Present | 11.47 | 1 | yes | 8 |
| 17M | F | 54 | S | Only minor criteria | no | Absent | 8.87 | 3 | no | 89 |
| 18M | F | 79 | S | Only minor criteria | yes | Present | 5.84 | 3 | no | 84 |
| 19M | M | 76 | C | Only minor criteria | no | Present | 5.58 | 1 | no | 72 |
| 20M | F | 71 | S | Only minor criteria | yes | Present | 7.36 | 2 | yes | 12 |
| 21M | M | 77 | S | Only minor criteria | no | Present | 4.15 | 2 | yes | 5 |
| 22M | M | 73 | S | Only minor criteria | no | Present | 7.3 | 2 | yes | 5 |
| Parameter | HR (95% CI) | p |
|---|---|---|
| Clinical-pathological risk score | ||
| low | 1 | |
| high | 3.5 (1.1–11.1) | 0.03 |
| Spontaneous necrosis | ||
| absent | 1 | |
| present | 2.7 (0.8–8.5) | 0.087 |
| 18q deletion | ||
| no | 1 | |
| yes | 2.6 (0.7–7.6) | 0.03 |
| 1p deletion | ||
| no | 1 | |
| yes | 3 (0.8–11.1) | 0.111 |
| 10q deletion | ||
| no | 1 | |
| yes | 0.6 (0.1–3.7) | 0.642 |
| 14q deletion | ||
| no | 1 | |
| yes | 1.9 (0.4–3.7) | 0.346 |
| 22q deletion | ||
| no | 1 | |
| yes | 1.4 (0–4–4.8) | 0.551 |
| NF2 mutation | ||
| no | 1 | |
| yes | 0.7 (0.2–2.3) | 0.617 |
| Genetic risk score | ||
| no | 1 | |
| yes | 5.3 (1.5–18.2) | 0.008 |
| CNL | ||
| low | 1 | |
| high | 2.3 (0.7–7.2) | 0.145 |
| TMB | ||
| low | 1 | |
| high | 0.6 (0.2–1.9) | 0.423 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barresi, V.; Simbolo, M.; Fioravanzo, A.; Piredda, M.L.; Caffo, M.; Ghimenton, C.; Pinna, G.; Longhi, M.; Nicolato, A.; Scarpa, A. Molecular Profiling of 22 Primary Atypical Meningiomas Shows the Prognostic Significance of 18q Heterozygous Loss and CDKN2A/B Homozygous Deletion on Recurrence-Free Survival. Cancers 2021, 13, 903. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040903
Barresi V, Simbolo M, Fioravanzo A, Piredda ML, Caffo M, Ghimenton C, Pinna G, Longhi M, Nicolato A, Scarpa A. Molecular Profiling of 22 Primary Atypical Meningiomas Shows the Prognostic Significance of 18q Heterozygous Loss and CDKN2A/B Homozygous Deletion on Recurrence-Free Survival. Cancers. 2021; 13(4):903. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040903
Chicago/Turabian StyleBarresi, Valeria, Michele Simbolo, Adele Fioravanzo, Maria Liliana Piredda, Maria Caffo, Claudio Ghimenton, Giampietro Pinna, Michele Longhi, Antonio Nicolato, and Aldo Scarpa. 2021. "Molecular Profiling of 22 Primary Atypical Meningiomas Shows the Prognostic Significance of 18q Heterozygous Loss and CDKN2A/B Homozygous Deletion on Recurrence-Free Survival" Cancers 13, no. 4: 903. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13040903