1. Introduction
The long-term survival of patients with laryngeal squamous cell carcinoma (LSCC) is excellent when locoregional recurrence is controlled [
1]. However, approximately 2.0% of deaths per annum are attributable to LSCC, with survivors frequently experiencing impaired voice quality [
2,
3]. Therefore, the etiologic risk factors for primary and recurrent LSCC need to be thoroughly studied; potential risk factors include cigarette smoking, alcohol consumption, environmental carcinogens, and gene mutations [
4]. According to previous studies, additional factors include human papillomavirus [
4,
5,
6], contrary to our findings [
7]; and Epstein–Barr virus (EBV) [
8,
9,
10,
11,
12], contrary to various reports [
5,
13,
14].
As the upper aerodigestive tract is in constant contact with the environment, it is easily infected by EBV, making it susceptible to local carcinogenesis [
9]
In nasopharyngeal carcinoma, local infiltration of EBV-infected leukocytes creates a tumor microenvironment that promotes tumor development [
15]. However, the effects of EBV infection on the host’s genetic susceptibility (e.g., expression of
BCL-2 (the Akt signaling pathway) [
16],
MYC (the TGF-β signaling pathway) [
17], and
p16INK4a (the cell cycle G1/S checkpoint signaling pathway) [
7]) and immune response (e.g., expression of
B2M [
18],
CD3 [
19], and
CD161 [
20]) to LSCC have not been reported in detail. Moreover, the relationship between viral infections and LSCC development and prognosis requires further investigation.
In this study, we aim to examine the following hypotheses: (1) EBV infection underlies the risk of primary LSCC, and (2) EBV infection affects the prognosis of LSCC, using a more comprehensive approach. The potential mechanisms of virus-related carcinogenesis will also be discussed.
3. Results
3.1. Clinical Characteristics of Patients
A total of 98 patients were identified, 17 of whom were excluded due to insufficient tissues (
n = 14) and low biomarker quality (
n = 3) (
Figure 1). Therefore, the overall cohort comprised of 42 patients with LSCC (cases) and 39 patients with NMLL (controls); a total of 81 patients (74 (91%) men and 7 (9%) women) with a median age of 58 years (interquartile age: 51–70 years).
Table 1 summarizes the baseline characteristics of the populations in the study. Age ≥ 55 years (unadjusted OR = 8.3; 95% CI: 3.0–22.5;
p < 0.001) and cigarette smoking (unadjusted OR = 4.5; 95% CI: 1.1–17.8;
p = 0.03) were significantly associated with a risk of LSCC.
Most patients had early stage (Stage I–II) LSCC (81%) and had undergone transoral laser microsurgery (67%) or RT (10%) as the definitive treatment.
3.2. EBV-Related Biomarkers in the Larynx and Peripheral Blood
The overall laryngeal EBV infection rate was 37% (
Table 2). The laryngeal EBV DNA positivity rate was significantly higher in case, compared to control, patients (52% vs. 20%; effect size = 0.70; 95% CI 0.24–1.16;
p = 0.01); therefore, patients with laryngeal EBV DNA positivity had a greater risk of developing LSCC, compared to those with EBV DNA negativity (unadjusted OR = 4.3; 95% CI: 1.6–11.4;
p = 0.004).
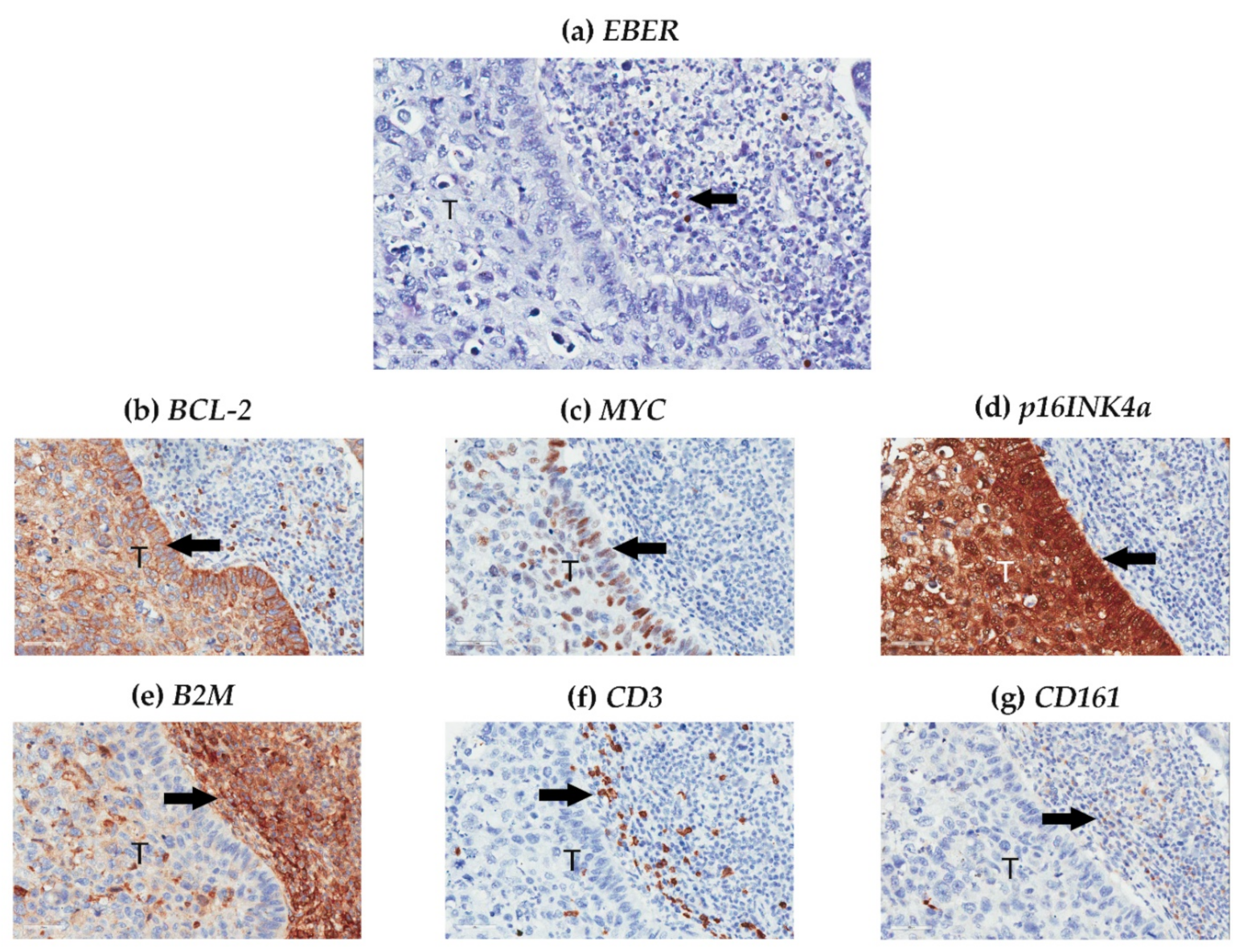
The laryngeal nPI for
EBER was relatively low in both case and control groups, and the staining distribution was equal between the groups (
Table 2). Most
EBER signals were localized to the nuclei of TILs (
Figure 2a); however, laryngeal EBV DNA positivity was not related to laryngeal nPI for
EBER (
r = 0.11,
p = 0.34).
Only 30 patients with LSCC had available peripheral blood EBV test data; among these patients, two (7%) and four (13%) had circulating EBV DNA positivity and serum EBV VCA IgA positivity, respectively. Differences in circulating EBV DNA positivity (7% vs. 6%, p > 0.99) and EBV VCA IgA positivity (7% vs. 19%, p = 0.60) between laryngeal EBV DNA-positive and -negative subgroups were not statistically significant. Therefore, the associations between laryngeal EBV DNA positivity, laryngeal nPI for EBER, plasma EBV DNA positivity, and serum EBV VCA IgA positivity were not statistically significant (all p > 0.05).
3.3. Histological Factors of the Larynx
In the IHC analysis, expression of
p16INK4A,
BCL-2, and
MYC occurred mainly in intratumoral cells (
Figure 2b–d), whereas
B2M,
CD3, and
CD161 expression occurred mainly in peritumoral (
Figure 2e–g) cells. Expression of
BCL-2,
B2M,
CD3, and
CD161 was higher,
MYC was lower, and
p16INK4a was the same in LSCC, compared with NMLL (
Table 3).
We further dichotomized these biomarkers using receiver operating characteristic curve analyses, with Youden’s J-point as the best trade-off between sensitivity and specificity, to predict LSCC. Expression of BCL-2 ≥ 68.6% (unadjusted OR = 5.5; 95% CI: 2.0–14.9; p = 0.001), B2M ≥ 84.3% (unadjusted OR = 8.6; 95% CI: 3.1–23.9; p < 0.004), CD3 ≥ 6.9% (unadjusted OR = 7.2; 95% CI: 2.6–20.2; p < 0.001), CD161 ≥ 68.8% (unadjusted OR = 3.5; 95% CI: 1.3–9.4; p = 0.01), MYC ≤ 0.44% (unadjusted OR = 2.9; 95% CI 1.2–7.1; p = 0.02), and p16INK4a ≤ 16.8% (unadjusted OR = 6.0; 95% CI 1.6–22.9; p = 0.01) were significant risk factors for LSCC.
3.4. Relationship between EBV-Related Biomarkers and Clinical and Histological Characteristics in the Overall Cohort
In the overall cohort, primary LSCC was significantly associated with age ≥ 55 years, cigarette smoking, EBV DNA positivity,
BCL-2 expression ≥ 68.6%,
B2M expression ≥ 84.3%,
CD3 expression ≥ 6.9%,
CD161 expression ≥ 68.8%,
MYC expression ≤ 0.44%, and
p16INK4a expression ≤ 16.8% (
Table 4).
Additionally, the male sex was significantly associated with cigarette smoking and alcohol consumption. The associations between age ≥ 55 years and MYC expression ≤ 0.44%, B2M expression ≥ 84.3%, and CD3 expression ≥ 6.9% were significant. Furthermore, the relationship between cigarette smoking and alcohol consumption was significant.
EBV DNA positivity was significantly correlated with high BCL-2 expression (≥68.6%), which also significantly correlated with B2M expression ≥ 84.3%, CD3 expression ≥ 6.9%, and CD161 expression ≥ 68.8%. Low p16INK4a expression (≤16.8%) was significantly associated with B2M expression ≥ 84.3% and CD161 expression ≥ 68.8%. B2M expression ≥ 84.3% was significantly associated with CD3 expression ≥ 6.9%, which also significantly associated with CD161 expression ≥ 68.8%.
3.5. Multi-Factor Modeling of Primary LSCC
To improve the precision of the model, we used a “forced simultaneous entry” approach and a “sign-correct” method for multivariate logistic regression analysis [
36]. Variables with a
p < 0.05 in the univariate analysis were entered into the regression analysis. Age ≥ 55 years (OR = 19.3; 95% CI: 3.2–116.0;
p = 0.001), cigarette smoking (OR = 36.4; 95% CI: 2.4–554.2;
p = 0.01), EBV DNA positivity (OR = 39.7; 95% CI: 3.3–478.0;
p = 0.004),
BCL-2 expression ≥ 68.6% (OR = 6.8; 95% CI: 1.2–38.6;
p = 0.03),
B2M expression ≥ 84.3% (OR = 18.1; 95% CI: 2.9–11.6;
p = 0.002), and
CD161 expression ≥ 68.8% (OR = 7.5; 95% CI: 1.1–50.7;
p = 0.04) were significant independent risk factors for primary LSCC.
Using this six-factor model, we accurately predicted which patients with laryngeal lesions had primary LSCC via the optimal cut-off value of 3 (area under the receiver operating characteristic curve: 0.87 [95% CI: 0.79–0.96]; p < 0.001), with a sensitivity, specificity, positive predictive value, and negative predictive value of 98%, 77%, 82%, and 97%, respectively.
3.6. Five Year Prognoses in Patients with LSCC
As of 28 February 2021, the median follow-up time was 68 months (range: 9–94 months). A total of 14 case patients had an LR within the first 5 years after definitive treatment; thus, the five-year LR rate was 34% (95% CI: 16–53%). Two patients had NR (five-year NR rate = 6%; 95% CI: 0–50%) and one had DM (five-year DM rate = 3%; 95% CI: 0–59%); therefore, five-year DFS was 58% (95% CI: 41–71%). Furthermore, two patients had disease-specific deaths (five-year DSS rate = 94%; 95% CI: 75–98%), while another two died of other causes (five-year OS rate = 89%; 95% CI: 72–96%).
Herein, we further focused on investigating the risk factors associated with five-year LR and DFS rates (
Table 5). EBV DNA positivity did not significantly predict five-year LR and DFS rates. However, an
EBER signal ≥ 0.04% significantly predicted both the five-year LR (unadjusted HR = 6.2; 95% CI: 2.0–18.6;
p = 0.001) and DFS (unadjusted HR = 7.1; 95% CI: 2.6–19.5;
p < 0.001) rates using univariate Cox regression models. Furthermore, age ≤ 63 years, TLM, and
CD3 expression ≤ 4.9% also predicted the five-year LR rate, whereas TLM,
BCL-2 expression ≤ 96.0%,
CD3 expression ≤ 4.9%, and
EBER signals ≥ 0.04% predicted five-year DFS rates.
Using multivariate Cox regression models, both EBER signals ≥ 0.04% (adjusted HR: 6.0; 95% CI: 1.9–18.6; p = 0.002) and CD3 expression ≤ 4.9% (adjusted HR = 6.9; 95% CI: 1.9–24.6; p = 0.003) independently predicted five-year LR rates; both risk factors significantly predicted five-year LR rates after adjustment for treatment modality (adjusted HR = 4.7 (95% CI: 1.5–15.0) and 5.4 (95% CI: 1.5–19.4), respectively; p = 0.01, and 0.01, respectively). Similarly, both EBER signals ≥ 0.04% (adjusted HR = 8.6; 95% CI: 2.9–25.3; p < 0.001) and CD3 expression ≤ 4.9% (adjusted HR = 6.6; 95% CI: 1.9–23.6; p = 0.004) independently predicted five-year DFS rates; these risk factors remained significant after adjustment for treatment modality (adjusted HR = 7.7 (95% CI: 2.5–24.0) and 5.4 (95% CI: 1.5–19.3), respectively; p < 0.001 and 0.01, respectively).
3.7. Relationship between EBV-Related Biomarkers and Clinical and Histological Characteristics in Patients with LSCC
In patients with primary LSCC, male sex was significantly associated with cigarette smoking and laryngeal EBV DNA positivity (
Table 6). Furthermore, an age ≤ 63 years was associated with alcohol consumption and
p16INK4a ≤ 81.6%, while cigarette smoking was related to alcohol consumption. As expected, T- and N-stages were associated with LSCC stage. EBV DNA positivity and
EBER signal ≥ 0.04% were not associated with other tissue biomarkers.
BCL-2 expression ≤ 96.0% correlated significantly with
p16INK4a and
CD161 expression ≤ 81.6% and ≤ 69.9%, respectively. In addition,
p16INK4a expression ≤ 81.6% was associated with
CD3 expression ≤ 4.9%.
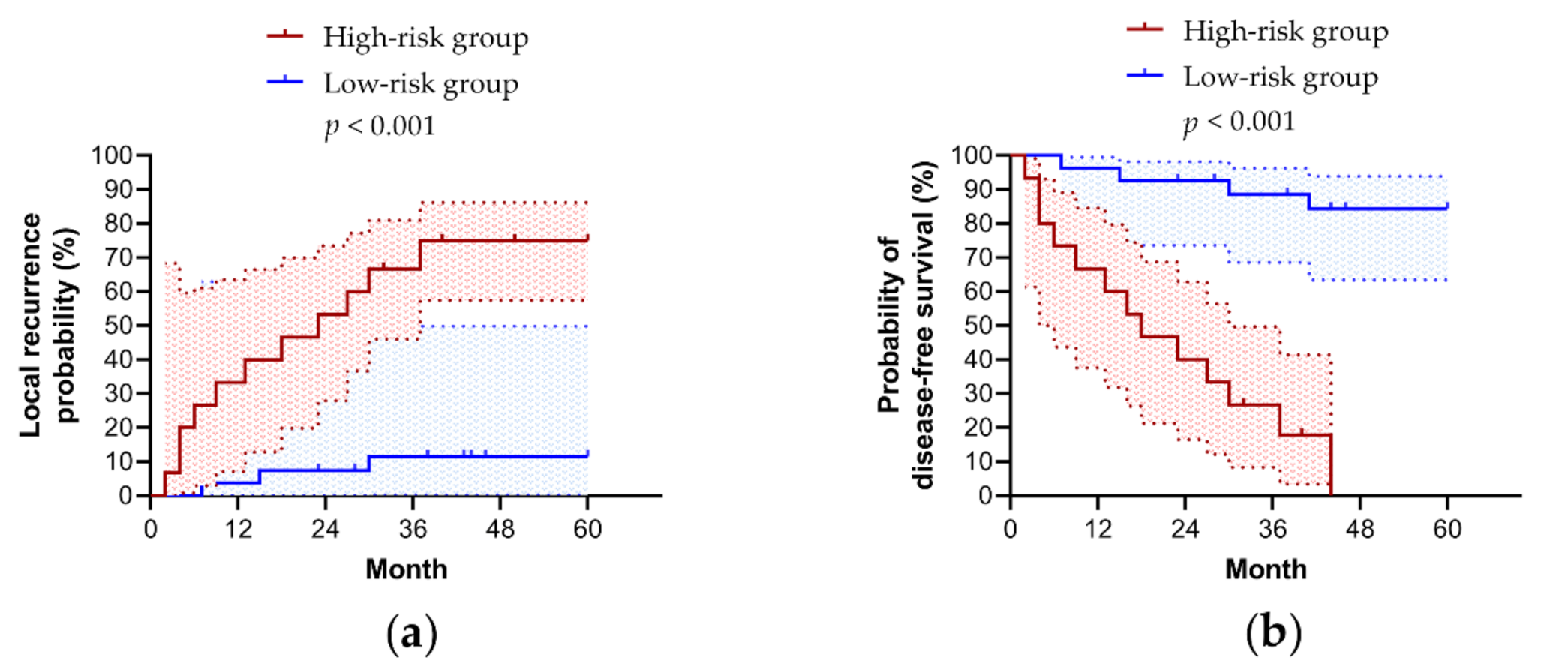
The overall cohort was further dichotomized into a high-risk group (≥1 risk factor) and a low-risk group (<1 risk factor) to predict five-year LR (sensitivity, 79%; specificity, 94%; positive predictive value, 88%; negative predictive value, 90%). This method performed well in predicting five-year DFS (sensitivity, 76%; specificity, 100%; positive predictive value, 100%; negative predictive value, 52%). The five-year LR rate of the high-risk group was significantly higher than that of the low-risk group (75% (95% CI, 57–86%) vs. 11% (95% CI, 0–49%);
p < 0.001) (
Figure 3a). As expected, the five-year DFS rate of the high-risk group was significantly higher than that of the low-risk group (0% vs. 84% (95% CI, 63–84%);
p < 0.001) (
Figure 3b). However, this model predicted the five-year DSS (83% (95% CI, 47–96%) vs. 100%;
p = 0.05) and OS (76% (95% CI, 43–92%) vs. 96% (95% CI, 72–99%);
p = 0.08) rates less efficiently due to relatively low numbers of disease-specific and overall deaths.
4. Discussion
In this study, we found that patients with primary LSCC had a higher prevalence of EBV infection, compared to control patients. In addition to age ≥ 55 years and cigarette smoking [
37], EBV DNA positivity,
BCL-2 expression ≥ 68.6%,
B2M expression ≥ 84.3%, and
CD161 expression ≥ 68.8% were independently associated with LSCC. Using this novel model, we accurately predicted the development of LSCC. Moreover,
EBER signals ≥ 0.04% and
CD3 expression ≤ 4.9% independently predicted five-year LR and DFS rates with or without adjustment for treatment modality. Using this innovative two-factor model, we could also accurately predict the five-year LR and DFS rates of LSCC.
Chronic viral infection is a risk factor for many cancers, such as hepatitis B virus/hepatocellular carcinoma, human papillomavirus/cervical cancer, and EBV/NPC. Quantifying EBV-related biomarker levels in tumor specimens could improve our understanding of the etiology of some laryngeal cancers, and assist in patient selection for treatment and follow-up protocols [
38]. However, quantification in FFPE tissue is difficult due to ambiguous uncertainties and the absence of reliable detection methods. Determining the interactions between EBV-related biomarkers and host factors is also challenging. For translation purposes, we developed and validated risk and prognostic models based on EBV-related biomarkers in this case-control study of Taiwanese patients with primary LSCC.
Similar to other studies [
8,
9,
11], we found that EBV infection was significantly more frequent in patients with primary LSCC than in those with NMLL. However, we found that most
EBERs were detected in the TILs of LSCC. The absence of latent EBV infection in the tumor tissue of LSCC suggests that its multistep nature of development may include “hit-and-run” carcinogenesis in the laryngeal epithelium. Notably, EBV DNA positivity was positively correlated with
BCL-2 expression, an anti-apoptotic protein in tumor cells.
Wp, a viral promoter located within
BamHI W repeats of the EBV genome, activates the gene encoding the viral
BCL-2 homolog
BHRF1, thereby increasing apoptosis resistance [
39]. Moreover, oncogenic EBV latent membrane protein 1 directly upregulates
BCL-2 in NPC [
40], potentially also contributing to LSCC [
11].
Furthermore, we found that
BCL-2 overexpression in LSCC was common (80%).
BCL-2 interacts with
Hsp90β, and may be involved in the anti-apoptotic progression of LSCC [
41].
BCL-2 overexpression appears to be associated with a complete response to induction chemotherapy [
16] and worse prognoses due to tumoral radioresistance [
42]. Although
BCL-2 overexpression might not contribute to the prognostic significance of LSCC development [
43], we found that both EBV DNA positivity and
BCL-2 overexpression in the larynx were independently associated with a risk of LSCC. Our results also indicate that
BCL-2 expression is not related to tumor aggressiveness and prognosis after a single surgical treatment [
42].
Regarding therapeutic prognoses, we found that
EBER signals ≥ 0.04% and
CD3 expression ≤ 4.9% were important prognostic factors for five-year LR and DFS in patients with LSCC. In our literature review, only a few patients with LSCC had positive
EBER signals in the larynx [
39,
44]. Although positive
EBER signals in LSCC tissues are considered poorer predictors of head and neck squamous cell carcinoma (HNSCC) [
39], a small LSCC sample size (two and six cases of positive and negative EBER signals, respectively) is difficult to draw conclusions from. Therefore, this study was the first to identify a high laryngeal
EBER signal as a poorer prognostic factor in LSCC. Since most
EBER signals presented the peritumor microenvironment in our patients, we presumed that
EBERs could induce the initial transformation of epithelial cells [
45], and trigger cancer-related inflammation via the RIG-I pathway to promote tumor development and growth [
46]; rather than downregulate B2M expression to evade T cell-mediated cytotoxic immune responses [
47], as according to previous NPC studies. Moreover, EBV-infected TILs of residual laryngeal tissue following curative treatment may increase the five-year LR risk via
BHRF1-mediated apoptosis resistance [
48]. Accordingly, mechanistic studies are warranted to confirm that EBV involves the
EBER-mediated process of LSCC recurrence.
Circulating EBV DNA is a robust biomarker for EBV-associated NPC [
49] and lymphoma [
50]. EBV VCA IgA positivity indicates previous repeated EBV infections or frequent reactivation of latent EBV in B cells [
51]. Patients with LSCC might have a higher positive rate of EBV VCA IgA than healthy controls [
52]. Therefore, both circulating EBV DNA and VCA IgA could be potential biomarkers for EBV-positive LSCC. In this study, neither circulating EBV DNA positivity nor serum EBV VCA IgA positivity was associated with laryngeal EBV DNA positivity and EBER nPI. Furthermore, the low positive rates of these peripheral blood biomarkers may limit their application in patients with LSCC.
Laryngeal cancer usually develops over many years, and approximately 80% of patients with LSCC are 60 years or older at first discovery [
53]. In this study, an age ≥ 55 years was associated with
B2M expression ≥ 84.3%, and both were independent risk factors for LSCC development. Recently,
B2M was validated as a key reference gene in laryngeal and hypopharyngeal cancers, highlighting its suitability for investigating target gene expression [
54]. Interestingly, its expression in patients with EBV-positive cancer was significantly higher than that in patients with EBV-negative cancer [
55]. The
B2M protein forms the light chain of the class I major histocompatibility complex, and is important for antigen recognition by cytotoxic T cells [
56]. Overexpression of
B2M is found in solid tumors and blood-borne malignancies, and is associated with advanced disease and poor prognosis [
57]. Although
B2M expression was not associated with LSCC stage and prognosis, it was an independent risk factor for LSCC development.
Furthermore, cigarette smoking is strongly associated with an increased risk of LSCC in a dose-response and time-response manner [
58]. Although significant smoking trend reductions have led to the declined global burden of LSCC in developed countries, smoking continues to trend upward in low socioeconomic countries, potentially inducing an increased burden of LSCC in the future [
59]. Notably, smoking prevention programs conducted in health care settings and interventions, including enhancement of interpersonal communication and support strategies, can be effective in preventing smoking behavior for three months to four years in children and adolescents [
60]. However, the latest meta-analysis indicated that findings which suggest that reduction-to-quit is more effective than no treatments were inconclusive and of low certainty [
61]. Nevertheless, the risk of developing LSCC can be reduced by smoking cessation for ≥ 15 years [
58].
CD161 is expressed on natural killer (NK) cells and subpopulations of T lymphocytes, such as invariant natural killer T cells (iNKT), CD4
+CD161
+ T cells, and CD8
+CD161
+ T cells [
62]. These cells may play significant roles in tumor development [
63], and may regulate the immune response in the tumor microenvironment [
64]. However, the effect of
CD161 expression on tumor development remains unclear. Patients with LSCC had a significantly lower percentage of circulating iNKT cells, compared to healthy controls [
65], whereas circulating CD4
+CD161
+ T cells, representing a memory T cell population, significantly increased in cancer patients [
66]. Notably, CD8
+CD161
+ T cell-specific EBV infections might express high levels of anti-apoptotic molecules to survive hostile inflammatory conditions, also involving the pathogenesis of tumor tissues [
67]. Furthermore, we found that
CD161 overexpression in LSCC was not uncommon, and correlated with
BCL-2 overexpression and low
p16INK4a expression. However, both
CD161 and
BCL-2 overexpression were independent risk factors for LSCC development.
In patients with LSCC, low
CD3 expression was associated with a poor prognosis. Similarly, a high infiltration of CD3
+ T lymphocytes was associated with a significantly better prognosis in patients with HNSCC [
68]. In patients with HNSCC, low
CD3 mRNA levels have been found to be worse predictors of 8-year DFS [
69]. Therefore, dysfunction of the immune response in removing the oncogenic EBV infection may increase the risk of cancer progression. Although we did not find a significant association between
CD3 expression and EBV infection in the larynx, patients with LSCC and EBV infection may have a lower proportion of late activated T lymphocytes in the peripheral blood compared to patients without EBV infection [
70]. Therefore, investigating peripheral blood T lymphocytes may help us to comprehensively understand the possible mechanisms of LR and relapse in EBV-related LSCC.
Our study had some limitations. First, when considering high EBV DNA positivity, false positivity is a real risk; PCR, which was used for EBV DNA detection, is extremely sensitive, and the EBER signal was minimal. However, we applied strict anti-contamination measures in the laboratory to reduce the risk of contamination [
27]. Second, in some patients, insufficient tissue and low-quality biomarkers limited the sample size; despite the use of TMAs to reduce the lesion volume required for comprehensive comparisons. Nevertheless, larger sample sizes may provide only modest benefits in complex statistical analyses.


 ,
, 




{kind=link}
{kind=link}
{kind=link}