
Personalized Immunotherapy Treatment Strategies for a Dynamical System of Chronic Myelogenous Leukemia



Postgraduate Program in Engineering Sciences, BioMath Research Group, Tecnológico Nacional de México/IT Tijuana, Blvd. Alberto Limón Padilla s/n, Mesa de Otay, Tijuana 22500, Mexico
*
Authors to whom correspondence should be addressed.
Cancers 2021, 13(9), 2030; https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092030
Submission received: 30 March 2021
/
Revised: 20 April 2021
/
Accepted: 21 April 2021
/
Published: 22 April 2021
(This article belongs to the Special Issue Mathematical Models of Cellular Immunotherapies in Cancer)
Abstract
:Simple Summary
As computer performance continues to grow at more affordable costs, mathematical modelling and in silico experimentation begin to play a larger role in understanding cancer evolution. The aim of our work is to formulate a control strategy for the Adaptive Cellular Therapy (ACT) that can fully eradicates the Chronic Myelogenous Leukemia (CML) cells population in a mathematical model describing interactions between naive T cells, effector T cells and CML cancer cells in the circulatory blood system. Mathematical analysis and numerical simulations allow us to conclude that it is possible to design a personalized administration protocol for the ACT in the form of a pulse train with asymmetrical waves and a fixed amplitude to achieve complete CML cancer cells eradication. The amplitude of the impulse on which the treatment is applied is given by an arithmetical combination of the parameters of the system with at least a duty cycle of 45 min/day.
Abstract
This paper is devoted to exploring personalized applications of cellular immunotherapy as a control strategy for the treatment of chronic myelogenous leukemia described by a dynamical system of three first-order ordinary differential equations. The latter was achieved by applying both the Localization of Compact Invariant Sets and Lyapunov’s stability theory. Combination of these two approaches allows us to establish sufficient conditions on the immunotherapy treatment parameter to ensure the complete eradication of the leukemia cancer cells. These conditions are given in terms of the system parameters and by performing several in silico experimentations, we formulated a protocol for the therapy application that completely eradicates the leukemia cancer cells population for different initial tumour concentrations. The formulated protocol does not dangerously increase the effector T cells population. Further, complete eradication is considered when solutions go below a finite critical value below which cancer cells cannot longer persist; i.e., one cancer cell. Numerical simulations are consistent with our analytical results.
1. Introduction
At the cellular level, cancer is defined as the uncontrolled growth of malignant cells that were able to break free from their regulatory mechanisms. For a malignant cell to emerge, several mutations need to be accumulated in the DNA sequence of a previously normal cell. When the latter occurs, clonal expansion begins in the form of multiple cell divisions, these descendants can undergo further mutations, increasing the possibility of a more aggressive tumor progression. Therefore, under the right conditions, cancer cells from a primary tumor could acquire the ability to enter into the circulatory system, travel to a different site, and invade surrounding organs and tissues in a process known as metastasis. Although, the great majority of primary tumors in humans are benign, metastatic or secondary tumors are responsible for most of the cancer-related deaths. Cancer cells may arise from almost any part of the body, hence their great diversity, grouping more than 200 types and each one with their own complexities. These types may be classified by the hierarchy as follows: epithelial, nonepithelial and mixed multilineage. In this work, we focus on a particular type of nonepithelial malignancy: Chronic Myelogenous Leukemia (CML).
Leukemia is a type of non-solid tumour, resulting from the clonal expansion of abnormal hematopoietic cells. That is, it starts in the blood-forming cells affecting both the peripheral blood and the bone marrow. Leukemias are classified based on their cell type: myelogenous or lymphocytic; and chronicity: acute or chronic. The latter depends on whether most of the abnormal cells are immature, with a faster growth rate; or mature, characterized by a slower growth rate. Regardless of the case, the lifespan of leukemia cells is longer than normal cells. Hence, they accumulate in the bone marrow and spill over into the peripheral blood, crowding out their functional counterparts such as healthy white blood cells, red blood cells, and platelets. Leukemia patients may eventually die due to infections, nutritional deficiencies, and multiple organ failure [1,2]. Statistics from the World Health Organization indicate that 474,519 new cases of leukemia and 311,594 deaths, including both sexes in all groups of ages, were registered worldwide in 2020 [3].
In the particular case of CML, this disease occurs mostly in adults, and very rarely in children. CML can be defined as a myeloproliferative neoplasm predominantly composed of proliferating granulocytes that did not mature completely [4]. Therefore, these cells do not have the ability to fight pathogens as well as a normal white blood cell would. Concerning CML prognosis, physicians need to know the patient’s age, general health, phase of CML, number of blasts in the blood or bone marrow, and the size of the spleen, in order to plan the best treatment strategy. That is, the type of therapy, dose, and intervals of application. The following six treatments are the standard for patients with CML: targeted therapy, chemotherapy, immunotherapy, high-dose chemotherapy with stem cell transplant, donor lymphocyte infusion, and surgery [5]. Nonetheless, new types of treatment are being tested in clinical trials [6].
Mathematical modelling through first-order Ordinary Differential Equations (ODEs) has been a powerful tool in understanding cancer evolution for nearly fifty years [7,8,9,10]. As computer performance continues to grow at more affordable costs [11], the so-called in silico experimentation begins to play a larger role in understanding cancer biology. Increased computing power enables researchers to formulate and execute more complex mathematical models that could potentially explore several scenarios of tumor progression in both short- and long-term. Further, one may include in these models the constantly evolving survival mechanisms of cancer cells, the immune system response, and the application of cancer therapies such as chemotherapy, immunotherapy, and cancer vaccines, among others. Cell–cell interaction models suggest that intermittent therapy is more beneficial to delay cancer relapse as compared to the standard continuous therapy [10].
Although not all models have been useful for clinical application, one can find the following works concerning mathematical models of anticancer therapies relating analytical results and in silico experimentations with clinical studies. de Pillis et al. [12,13] constructed a mathematical model of cancer chemoimmunotherapy involving the dynamics of tumor cells, specific and non-specific immune cells, chemotherapy and two types of immunotherapy. The authors were able to identify appropriate values for the parameters according to empirical data concerning two human patients. This system is given by a set of ODEs and it is one of the most complete mathematical models of cancer evolution under combined treatment application. Numerical simulations were performed, following recommended dosages from drug manufacturers and clinical studies in both therapies. Kronik et al. [14] formulated a mathematical model that could be individualized by patient-specific parameters to predict outcomes on prostate cancer patients treated with an allogeneic whole-cell cancer vaccine, a type of immunotherapy. In the period of one year, they were able to accurately estimate prostate-specific antigen levels in twelve vaccine-responsive patients. Further, the model describes the direct vaccine effect in immune stimulation against prostate cancer by a set of linear and nonlinear ODEs. Kim et al. [15] developed two mathematical models that explore interactions between drug-sensitive and resistant melanoma cells to facilitate adaptive therapy dosing. They were able to fit patient-specific parameter values for each model and illustrate tumor burden for eight patients. Numerical simulations predicted that adaptive therapy would have delayed time to progression by 6–25 months compared to continuous therapy. Among many others, these works highlight the potential benefits of applying mathematical modelling in cancer clinical trials by fitting values related to patient-specific tumor parameters in order to better design therapy dosing for each individual case.
In this paper, we aim to study CML evolution and its treatment by means of nonlinear system theory and in silico experimentation, we apply the adaptive cellular therapy (ACT) as a control strategy to a system describing the dynamics between naive T cells, effector T cells and CML cancer cells in the circulatory blood system by means of three ODEs. The mathematical model was constructed by Helen Moore and Natasha Li [16] and, as discussed by the authors, main difficulties in modelling CML evolution is related to the scarcity of experimental data that can be used to estimate parameters values. However, they were able to determine 12 parameters for their system, each one with their corresponding range of values.
ACT is a promising approach in the treatment of CML, it is one of the original forms of cancer immunotherapy that illustrates how T-cells can recognize and eliminate malignant cells. This therapy requires patients to be infused with a large number of autologous or allogeneic T-cells that have undergone ex vivo selection and modification, expecting them to target leukemia antigens with minimal impact on normal tissues [17,18]. Hence, our interest in investigating both the short- and long-term effects of this treatment over CML evolution and immune response on the system proposed by More and Li by means of the Localization of Compact Invariant Sets (LCIS) method [19,20], the stability theory in the sense of Lyapunov, and in silico experimentation.
The remainder of this paper proceeds as follows. In Section 2, we present the mathematical preliminaries concerning the LCIS method and provide references concerning its application on first-order ODEs dynamical systems describing cancer evolution. In Section 3, we describe the CML-Immunotherapy mathematical model, the dynamics of each equation and the description, values, and units of each parameter. In Section 4, we apply the LCIS method to compute the localizing domain of the CML-Immunotherapy system and derived sufficient conditions by means of Lyapunov’s stability theory to ensure CML cancer cells eradication. In Section 5, we perform the in silico experimentation in the form of several numerical simulations to design personalized protocols for the administration of the ACT treatment. We illustrate how this protocol can be implemented for different initial non-solid tumor concentrations and still successfully eradicate the CML cancer cell population. Further, biological implications and interpretation of these results are also discussed. Finally, conclusions are given in Section 6 and an appendix section is provided where the local existence and uniqueness of solutions is discussed.
2. Localization of Compact Invariant Sets Method
The LCIS method was proposed by Krishchenko and Starkov in [19,20] to study the short- and long-time dynamics of nonlinear systems of first-order ODEs by computing the so-called localizing domain. During the past few years, this method has been successfully applied to analyze the global dynamics of cell-cell interaction systems concerning cancer evolution [21,22,23,24,25].
The localizing domain is a bounded region in the state space where all compact invariant sets of a system are located. Equilibrium points, periodic, homoclinic and heteroclinic orbits, limit cycles and chaotic attractors are examples of compact invariant sets. Let us take an autonomous nonlinear ODEs system of the form , where is a differentiable vector function and is the state vector. Let be a differentiable function, denotes the restriction of on a set . The function used in this statement is called localizing and it is assumed that is not the first integral of . denotes the set , where represents the Lie derivative of and is given by: . Now, let us define and . Then, the General Theorem concerning the localization of all compact invariant sets of a dynamical system establishes the following:
Theorem 1.
General Theorem. See Section 2 in [20]. Each compact invariant set Γ of is contained in the localizing domain:
Localizing functions are selected by a heuristic process, this means that one may need to analyze several functions in order to find a proper set that will allow us to fulfill the General Theorem. If one considers the location of all compact invariant sets inside the domain then the set may be formulated. It is evident that if all compact invariant sets are located in the sets and , with , then they are located in the set as well. Furthermore, a refinement of the localizing domain is realized with help of the Iterative Theorem stated as follows:
Theorem 2.
Iterative Theorem. See Section 2 in [20]. Let be a sequence of differentiable functions. Sets
with
contain any compact invariant set of the system and
3. The CML-Immunotherapy Mathematical Model
The mathematical model for CML evolution was formulated by Moore and Li by means of three first-order ODEs that describe the interactions between naive T cells , effector T cells and leukemia cancer cells in the circulatory blood system [16]. In the latter, authors compute equilibrium points and study their local stability by linearization of the system. They also perform a numerical analysis of the relationships between parameters and its influence in the leukemia cancer cells population. The latter allows them to conclude on the biological relevance, validation of the model and how it could be used to solve the optimal drug dosing problem for leukemia patients. Hence, we use their mathematical model to solve the cancer cells eradication problem by considering a cellular immunotherapy treatment application. The CML-Immunotherapy mathematical model is given as follows.
These equations describe the time-evolution of each cell population in the blood compartment and their interactions are discussed below.
The dynamics of naive T cells, both specific and non-specific to CML cancer cells, are described by Equation (1). Naive T cells are considered to enter the blood system at a constant rate with a natural death rate of in the absence of a proper stimulus, e.g., the presence of CML cancer cells. The Michaelis-Menten term represents the differentiation of naive T cells into specific effector cells due to encounters with the CML antigen in the lymph nodes at a constant rate and a half-saturation of . Further, the Michaelis-Menten term considers both activation and energy as contributors to the loss term; naive T cells can become anergic if they encounter the CML antigen without co-stimulators.
The effector T cells specific to CML cancer cells that have differentiated from naive T cells are represented by Equation (2). The first term is due to activation encounters between naive T cells and APC presenting peptides from CML antigen. It is assumed that a total of naive T cell successfully converts into effector T cells specific to CML cancer cells. The second term is a recruitment term of effector T cells due to their encounter with cancer cells, it is assumed that a proportion of effector cells will recruit other immune cells to aid in killing CML cells. The third term represents the natural death of effector T cells with a coefficient of . The fourth term represents the loss of effector T cells at a rate due to activation-induced cell death from leukemia cancer cells. This process is described by the law of mass action as these encounters occur in the blood and there is no saturation effect such as in the lymph nodes. Lastly, is the adaptive T-cell therapy, i.e., this term represents the infused enhanced T-lymphocytes into the patient.
The growth and evolution of CML cancer cells are given by Equation (3). The first term represents tumor growth in the form of a Gompertz law which is considered to be the best fit for leukemic cancers, i.e., non-solid tumors. The CML cancer cells proliferation rate is given by with a maximum carrying capacity of , this limit could be decreased by considering the natural death of these cells which is given by the second term with a constant rate of . The loss of cancer cells due to their encounter with effector T cells is described by the law of mass action with a coefficient of . This last term is directly influenced by the cellular immunotherapy treatment concentration in the blood system.
The description, range of values, and units of each parameter of the CML-Immunotherapy mathematical model (1)–(3) is shown in Table 1 and were retrieved from [16].
Furthermore, the CML-Immunotherapy system (1)–(3) fulfills the positivity property established by De Leenheer and Aeyels, see Section II.A in [26]. The latter implies that given nonnegative initial conditions, all solutions will have nonnegative real values for all . Hence, any semi-trajectory of the system is going to be positively forward invariant in the nonnegative octant and all dynamics of the system are located in the following domain:
and it is important to note that given the constant influx of naive T cells , this population will persist as the natural proliferation rate of these cells is higher than its natural death rate and differentiation rate into T cells , i.e., . Nonetheless, both effector T cells and CML cells populations may be zero; the first one may be zero in the absence of immune stimulation or complete immune suppression, while the other if both the immune response and therapy are successful. Further, local existence and uniqueness of solutions regarding the CML-Immunotherapy system (1)–(3) is discussed in Appendix A.
4. Results
In this section, we will demonstrate how to apply the LCIS method and Lyapunov’s stability theory to derive sufficient conditions on the immunotherapy treatment to ensure the complete eradication of the CML cancer cells population described by system (1)–(3). These conditions are given by inequalities in terms of the system parameters and are going to be applied with in silico experimentations to formulate a therapy administration protocol in a further section.
4.1. Localizing Domain
In order to determine all bounds for a compact localizing domain to the CML-Immunotherapy system we explore four localizing functions. First, let us determine an upper bound for the concentration of naive T cells. Hence, the first localizing function is given by
and its Lie derivative is as follows
hence, set may be written as shown below
now, one can discard the negative term on the right-hand side and estimate the next upper bound for the naive T cells
The lower bound may be computed as well from set when rewriting it as follows
thus, the Michaelis–Menten term on the right-hand side is discarded and the lower bound is estimated
From the latter, the next result concerning the ultimate bounds for the naive T cells population is established in the following set
Now, let us consider the following localizing function to compute an upper bound for the CML cancer cells
hence, the Lie derivative is given by
and set is written as shown below
thus, the following two solutions can be found
from the latter, the lower bound is determined and a preliminary upper bound for any solution is estimated as follows
this upper bound will be improved below by applying the Iterative Theorem when considering both the immune response and the immunotherapy treatment.
The third localizing function is intended to study the dynamics of the effector T cells population. The function is given by
and the Lie derivative is computed below
thus, set is presented as follows
hence, if we discard the Michaelis–Menten terms of the right-hand side to estimate a lower bound, then the following result can be determined
where the Iterative Theorem is applied when considering immune suppression from CML cancer cells as indicated below
therefore, the lower bound for the effector T cells population is given by
This previous result allows us to improve the upper bound of the CML cancer cells population. Now, both the immune response and the immunotherapy treatment are going to be considered by applying the Iterative Theorem to set as follows
and by taking the exponential form on both sides of the equation we get the following ultimate lower and upper bounds for the leukemia cancer cells population
Now, to estimate the upper bound for the effector T cells population one can analyze the following localizing function
the Lie derivative is computed as indicated below
and set is written as follows
where
thus, by considering , we get the following
and rewrite the latter by assuming that next condition holds
therefore
and the Iterative Theorem is applied to get the following subset
from the latter, the next constraint is formulated
if (6) is fulfilled, one can conclude the next upper limit for the localizing function as follows
Now, the next upper bound for the effector T cells population can be estimated from
thus, lower and upper bounds for any nondivergent solutions of to the effector T cells population are given in the next set
Results shown in this section allow us to formulate the following statement concerning the ultimate bounds of a compact domain located in the nonnegative octant for the CML-Immunotherapy system (1)–(3).
Theorem 3.
The latter implies that all meaningful dynamics of the system will be forward invariant located within the localizing domain . These dynamics include both tumor-free and tumor-burden equilibria. Hence, sufficient conditions for asymptotic stability of the tumor-free equilibrium point should be derived to properly design an applicable immunotherapy treatment protocol that could potentially control and take the system to a clinically healthy state, i.e., cancer remission or complete tumour eradication.
4.2. Leukemia Cancer Cells Eradication
Now, we will demonstrate how to derive sufficient conditions to ensure the complete leukemia cancer cells eradication in the CML-Immunotherapy system (1)–(3). First, when nonlinear systems theory is combined with systems biology and in silico experimentation, it can be assumed that there is a final critical value below which cancer cells can no longer persist [27,28]. Taking this into account, there is no biological meaning for any numerical value describing fewer than 1 cell in the domain of the variables of the system. Therefore, this threshold is established to discuss and ensure the complete eradication of the CML cancer cells population by means of the immunotherapy treatment application. The latter allows us to propose the following.
Assumption 1.
Threshold for CML Cancer Cells Eradication. For any solution that goes below the threshold value of 1 cell, it is possible to assume complete eradication of the CML cancer cells described by system (1)–(3). Hence,
Furthermore, Moore and Li [16] discuss partial remission when there are fewer than 22,500 CML cancer cells/μL. Results shown in this section are determined by means of Lyapunov’s stability theory (see Theorem 4.2 by Khalil in [29] at Section 4.1) and the Localizing Domain Theorem. Thus, let us exploit the following candidate Lyapunov function
and compute its derivative as follows
It is evident that and in virtue of when considering the Threshold for CML Cancer Cells Eradication, one can formulate the next upper bound to function
from the latter, the next constraint is determined
and solved for the immunotherapy treatment as indicated below
Therefore, we are able to formulate the following statement regarding the leukemia cancer cells eradication by means of the immunotherapy treatment application.
Theorem 4.
The latter implies asymptotic stability for all solutions to the plane . Then, when conditions for the CML Cancer Cells Eradication Theorem are fulfilled, the CML-Immunotherapy system (1)–(3) is simplified as follows
which is an uncoupled linear system with a unique equilibrium point = that is globally asymptotically stable (see Theorem 4.5 by Khalil in [29] at Section 4.3). Additionally, when conditions for the CML Cancer Cells Eradication Theorem are fulfilled, then all solutions of system (1)–(3) with nonnegative initial conditions will go to the tumour-free equilibrium point
and we come to the following result.
5. Discussion and In Silico Experimentation
In this section, we discuss and illustrate our mathematical results concerning the CML cancer cells eradication by an immunotherapy treatment applied as a control strategy. In silico experimentations were performed to formulate an administration protocol that eradicates the CML cancer cells population when considering three different initial non-solid tumour sizes, initial conditions are set as ratios of the maximum carrying capacity, ; a fast-growing tumor rate ; a persistence leukemia cells population with a low death rate ; and an enhanced elimination rate of CML cells by the effector T cells due to the therapy. Table 1 shows the specific value used for each parameter in all numerical simulations.
Now, let us discuss conditions for the Localizing Domain Theorem, i.e., (4)–(6). According to the values of Table 1, these conditions hold, which implies that all compact invariant sets of the CML-Immunotherapy system (1)–(3) are located either inside or at the boundaries of the domain . Hence, all nondivergent solutions are bounded from above and below. Further, it is important to notice that these conditions were derived from function . Therefore, in the case these conditions are not fulfilled, both naive T cells and CML cancer cells will still have their corresponding lower and upper bounds. Additionally, existence of the lower bound for the effector T cells population is not related to conditions (4)–(6), and one can still establish sufficient conditions to ensure the CML cancer cells eradication by means of the immunotherapy treatment application.
Below, by substituting values from Table 1 into condition (7) we get the following
and, one may set the final cellular immunotherapy treatment concentration as
which is sufficient to ensure the CML cancer cells eradication and global stability of the tumour-free equilibrium point (8). The latter is written numerically as follows
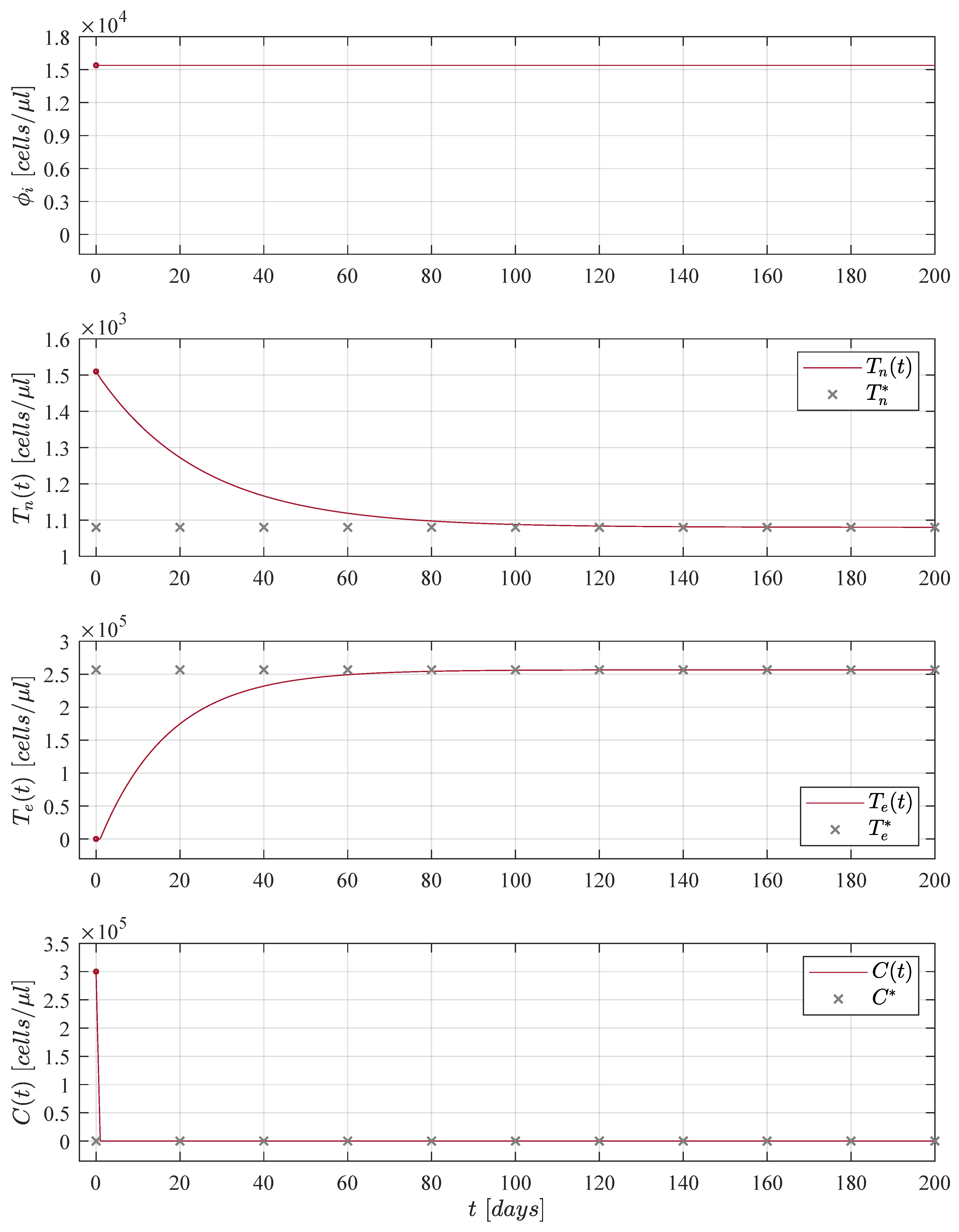
Dynamics of the CML-Immunotherapy system (1)–(3) concerning results discussed above are illustrated in Figure 1. Initial conditions for both naive T cells and effector T cells are set to cells/μL and cells/μL, respectively, as indicated by Moore and Li [16]; these values are applied to the remaining numerical simulations shown in this section. For the leukemia cancer cells concentration we used the maximum carrying capacity as initial condition in order to consider the worst-case scenario of tumour burden.
Results shown in Figure 1 are achieved when immunotherapy treatment is constantly applied, i.e., ∀ as it is shown in the upper panel. The application of the treatment was considered as a constant for the sake of simplicity in the mathematical analysis as has been previously discussed through the years by many authors when modelling the role of immunotherapy in boosting the immune system response to cancer growth, see [9,12,13,30,31,32,33,34,35]. Nonetheless, two issues arise in this case, it is not biologically feasible to constantly applied an immunotherapy treatment to a cancer patient and it is evident that the solution of the effector T cells goes to the value 256,596 cells/μL (a concentration close to that of the the maximum carrying capacity of the CML cancer cells) which could produce adverse events in the patient’s health [36]. Hence, in order to avoid the latter, numerous authors have proposed different treatment strategies to apply therapies such as chemotherapy, radiotherapy and immunotherapy by time intervals or in the form of periodic oscillations, one can see [14,37,38,39,40,41,42,43,44]. Thus, our hypothesis is as follows: Daily applications for a finite period of time of the immunotherapy treatment will decrease the CML cancer cells concentration below a critical threshold under which it is possible to ensure the complete eradication of the disease.
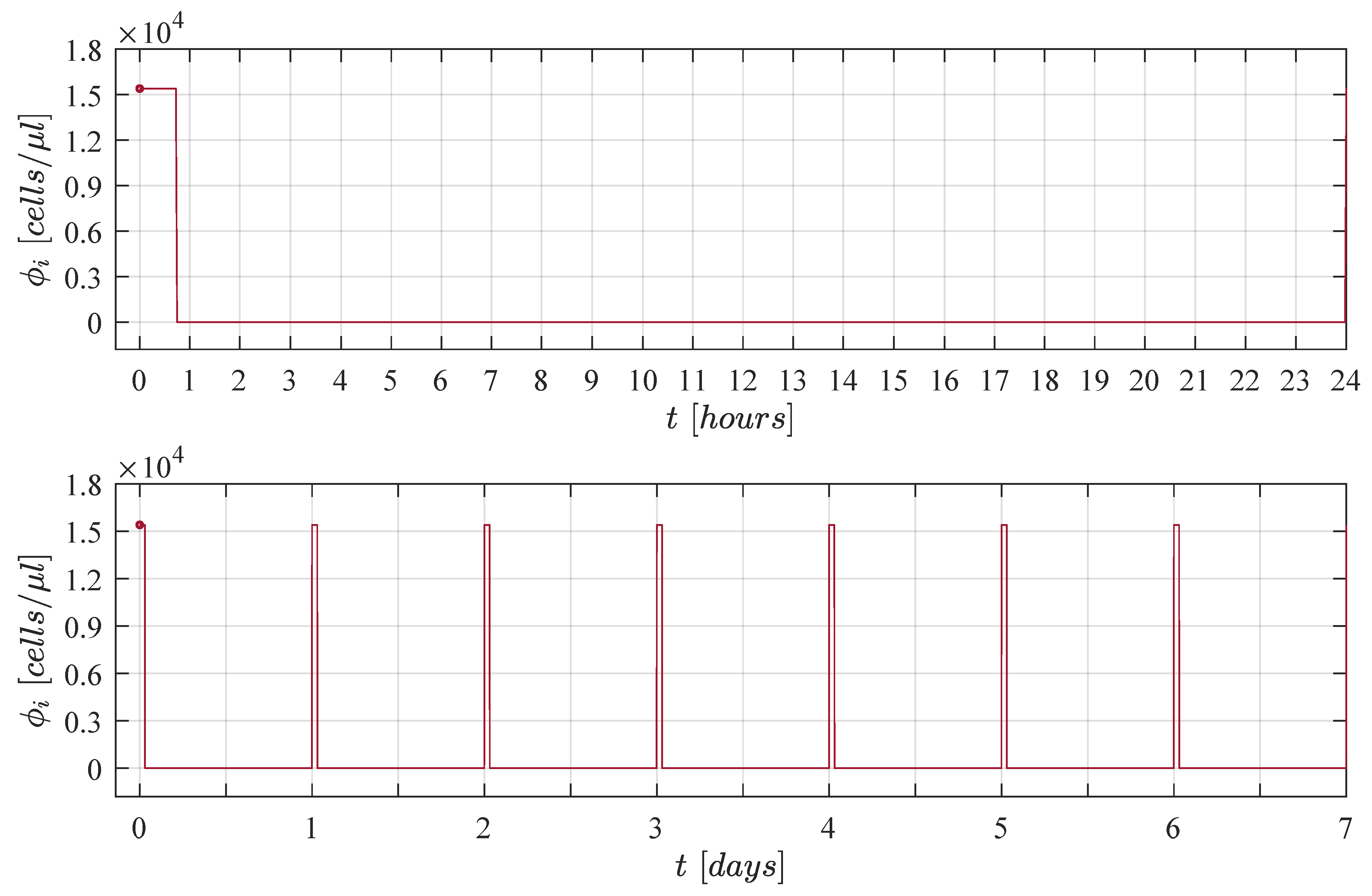
In order to apply the treatment for short intervals of time every day we decided to explore a pulse train with asymmetrical waves and a fixed amplitude of . By performing an in silico experimentation process by means of several numerical simulations where duty cycles were increased by in each iteration we were able to conclude that daily applications of the cellular immunotherapy treatment with at least a duty cycle of /day were needed to achieve complete CML cancer cells eradication when considering the maximum carrying capacity as initial condition . This strategy is illustrated below in Figure 2, one can see the immunotherapy administration protocol in 1 day in the upper panel (time unit is given in hours), and 1 week in the lower panel (time unit is given in days).
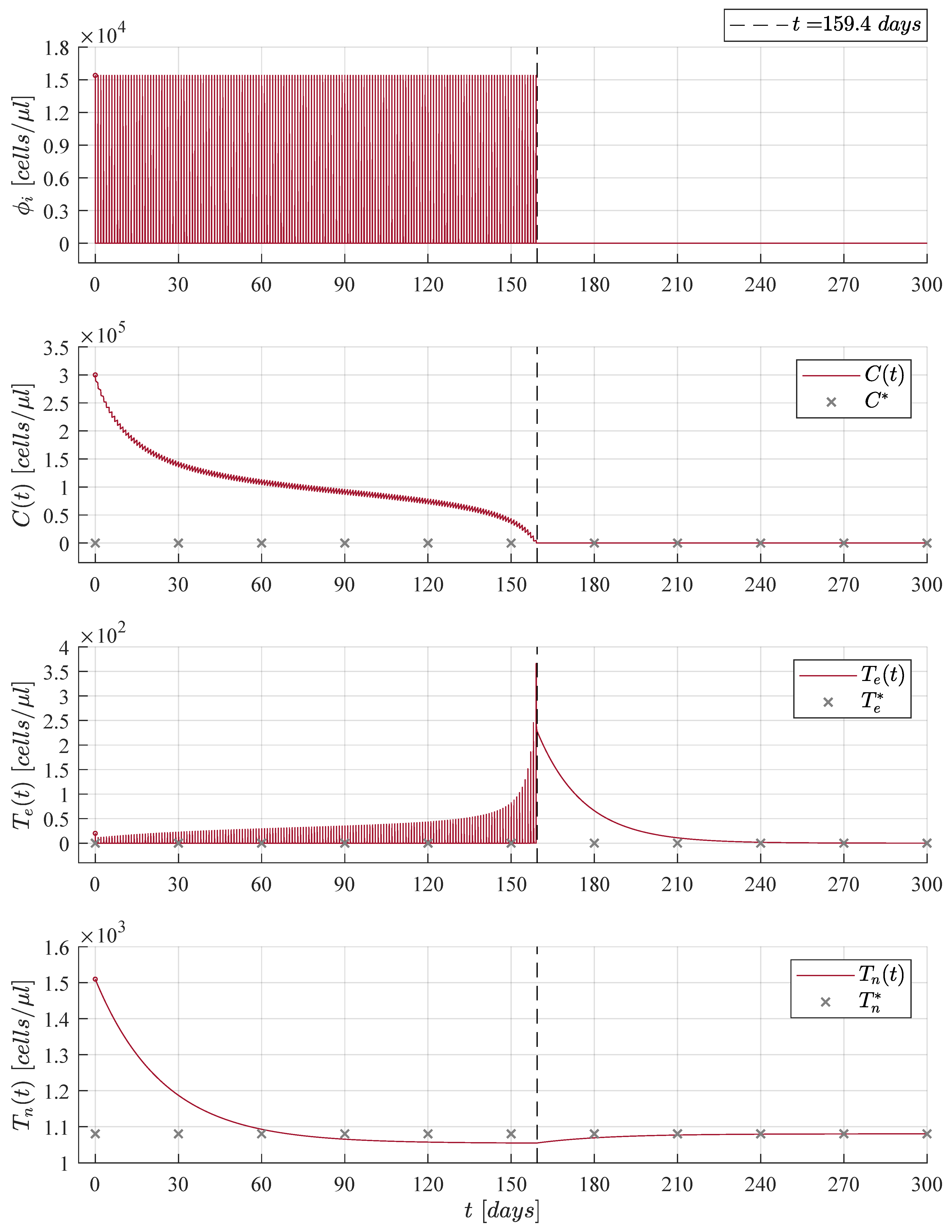
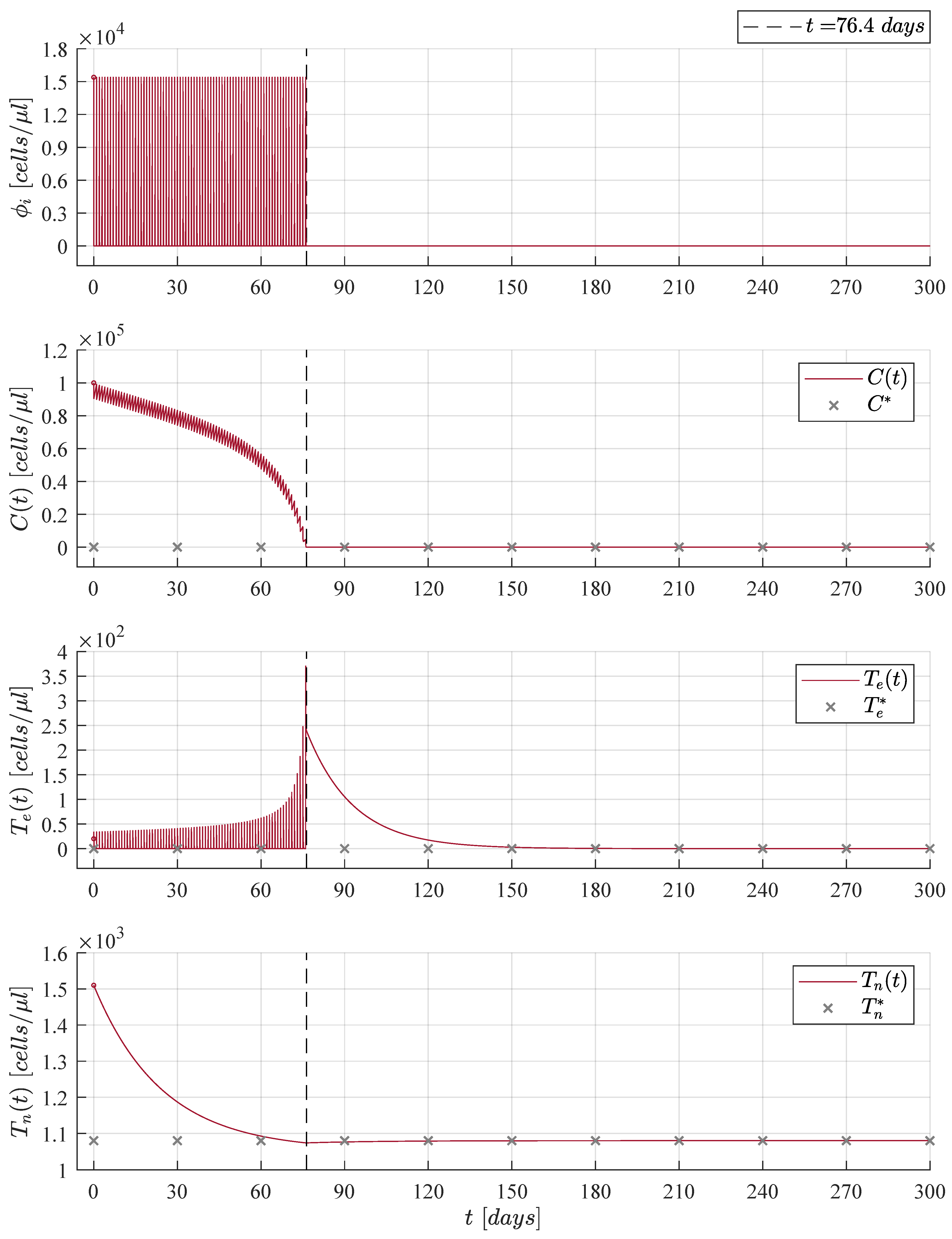
The immunotherapy administration protocol from Figure 2 is applied when considering three different initial tumour concentrations, in Figure 3, in Figure 4, and in Figure 5. Solutions to Equations (1)–(3) as well as the treatment are illustrated in each case. It is evident that as the initial tumour density increases, then the immunotherapy treatment should be applied for a longer period of time.
Numerical simulations were set to stop the immunotherapy application when cancer cells go below the positive finite critical value of one cancer cell, as discussed in Assumption 1. Hence, both the treatment and the CML cancer cells population were set to zero, i.e., and when . After the CML cancer cells eradication, one can see that solutions to both naive T cells and effector T cells go to their respective equilibrium point when . The latter is given by cells/μL and . Further, it is important to notice that the final dynamics of the naive T cells concentration is the average value expected in healthy individuals in steady state [16,45,46,47]. Concerning the maximum concentration of effector T cells, results are as follows: 367 cells/μL in Figure 3, 455 cells/μL in Figure 4, and 371 cells/μL in Figure 5. These values are significantly lower than the 256,596 cells/μL obtained in Figure 1 when the immunotherapy treatment is applied constantly over time.
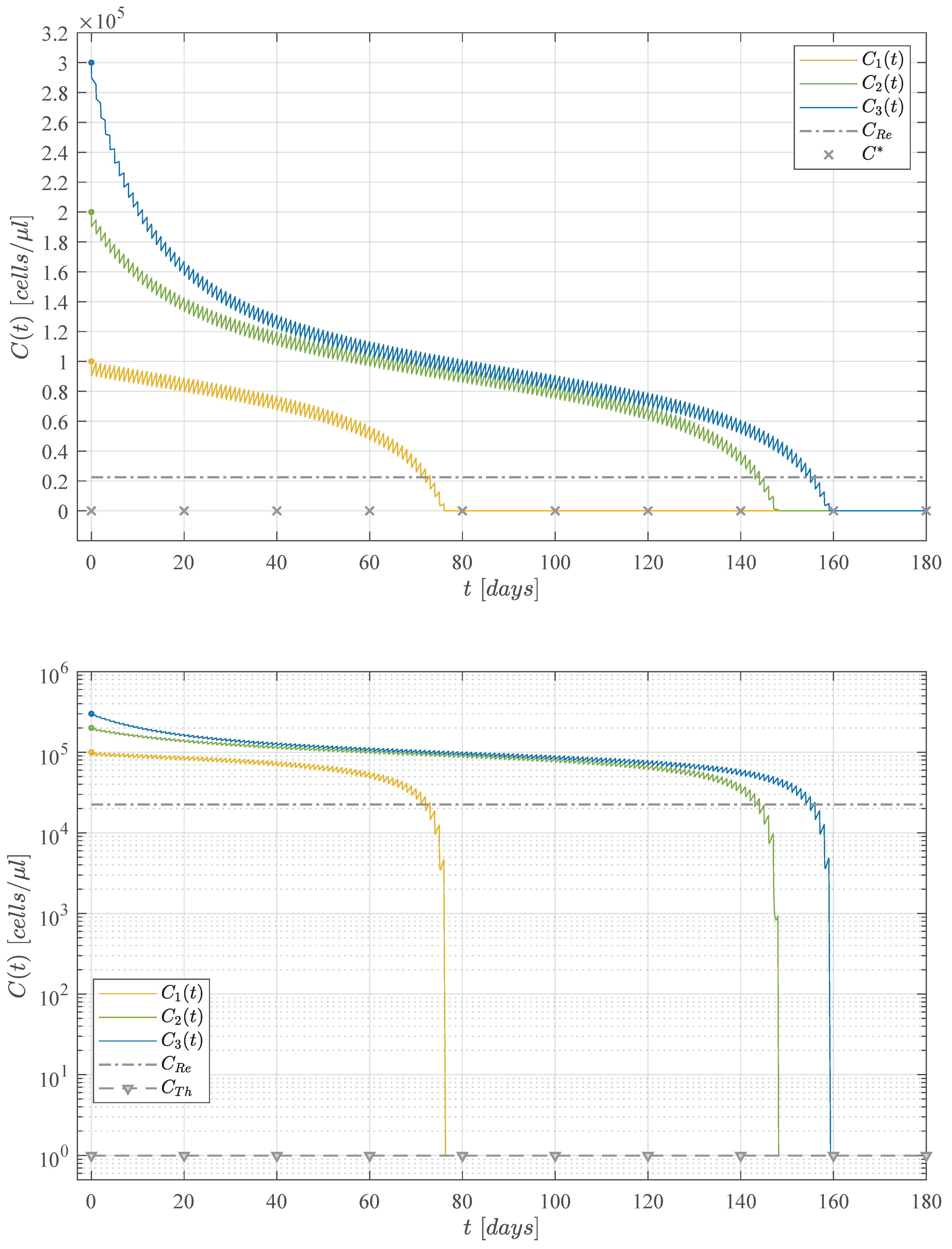
Now, results concerning the CML cancer cells populations for each initial concentration are summarized in Figure 6. These dynamics are illustrated in both linear and logarithmic scales in the upper and lower panels, respectively. In the upper panel one can see the threshold for tumour remission ( 22,500 cells/μL) and the tumour-free plane . Whilst, in the lower panel, both thresholds for tumor remission and tumor eradication cell/μL) are shown. Times when CML cancer cells go below the tumour eradication threshold are as follows: days for (initial concentration ); days for (initial concentration ); and days for (initial concentration ). These results are also indicated in Figure 3, Figure 4 and Figure 5.
When condition (7) is fulfilled, then the CML cancer cells population will decrease as it is stated by the CML Cancer Cells Eradication Theorem. Therefore, it is necessary to note that immediately after stopping treatment in each iteration, then the leukemia cancer cells begin to grow again, which implies that is imperative for the patient to continue with the daily applications of the treatment until the cancer cells concentration goes below the established threshold of one cancer cell.
We expect our work will benefit a leukemia patient in the sense that the methodology described in this paper could be applied to solve the optimal ACT dosing problem for each particular case in any scenario that may potentially be described by the CML-Immunotherapy system (1)–(3). The mathematical analysis indicates that only a subset of parameters influence the amount of treatment concentration that should ultimately be applied to the patient in order to fulfill condition (7) to achieve CML Cancer Cells Eradication from Theorem 4 and, it should be noted that this expression is written as a simple algebraic combination of this subset of parameters. With this condition, an administration protocol that can be individualized for each patient was designed and, as Moore and Li concluded in their research [16], this kind of control strategy may increase the time-period in which a cancer patient remains healthy. Additionally, the cost of the treatment could be constrained to the severity of the disease in each patient, as immunotherapy is often very expensive [48]. We aim to further extend our work to design a control strategy for the application of combined cancer therapies such as chemoimmunotherapy and, if possible, discussed how these strategies could be useful in avoiding cancer cell resistance to the prolonged administration of these treatments.
6. Conclusions
Cancer dynamics result in a complex set of events all happening at the same time in the tumor site. These events may trigger cancer cells to evolve with diverse mechanisms that allow them to escape immune response and invade other tissues and organs in the human body. Adaptive cellular immunotherapy is a type of treatment that can help the immune system to better respond against cancer growth. However, open questions still remain, e.g., What is the right dose of the treatment to be applied? and How often should the treatment be applied? Mathematical modelling and nonlinear systems theory combined with in silico experimentation may help us to provide scientifically formulated answers to these important questions related to cancer evolution.
Moore and Li [16] provided some insights concerning local stability of the two main equilibrium points of their system, i.e., the healthy state and one with tumor burden. They determined, under certain conditions on the parameters, that both could be locally asymptotically stable. Further, their numerical analysis regarding relationships between parameters and the dynamics of solutions indicate that both the growth rate and natural death rate of CML cancer cells are the most important parameters to control tumour growth. Nonetheless, conditions for local stability may not always be fulfilled, at least not without a proper treatment that can influence the values of the parameters. However, these values are expected to be different for each individual case. Authors conclude their work by providing recommendations on how the model may be applied to include immune system-boosting treatments and to solve the optimal drug dosing problem. Hence, in this paper, we incorporate the adaptive cellular therapy treatment and demonstrate how to apply the LCIS method and Lyapunov’s stability theory to derive sufficient conditions to ensure the complete eradication of the CML cancer cells population, i.e., global asymptotic stability conditions. Further, extensive in silico experimentations allowed us to formulate a control strategy for the administration of the immunotherapy treatment in diverse scenarios.
Numerical simulations allow us to understand and explore diverse scenarios which are illustrated in Figure 3, Figure 4 and Figure 5. We formulate these cases in terms of the initial tumor concentration, initial conditions are set as ratios of . This parameter describes the maximum carrying capacity of the CML cancer cells in the circulatory blood system, as it is shown in Table 1. Hence, we decided to explore the dynamics between cancer growth, the immune response and the effect of the cellular immunotherapy treatment for three initial tumour concentration given as follows: , , and . Results concerning the final dynamics of the leukemia cancer cells in each case are summarized in Figure 6. Further, one can see two important numerical values concerning cancer cells, the first is given by the threshold for tumor remission on CML cells/μL), and the second by the threshold for complete tumor eradication cell/μL). The latter is discussed in Assumption 1 as we consider that there is no biological meaning for any numerical value describing fewer than one cancer cell. Further, this assumption allows us to establish conditions to ensure both CML cancer cells eradication and global stability of the tumor-free equilibrium point.
Mathematical and in silico results shown in this paper allow us to conclude that it possible to formulate a control strategy for the cellular immunotherapy administration that can fully eradicate the CML cancer cells population described by system (1)–(3). Numerical simulations illustrate that the total iterations of the treatment application are directly related to the initial tumor concentration in order to decrease it below the final critical value of one cancer cell. The amplitude of the impulse on which the treatment is applied is given by an arithmetical combination of the parameters of the system, as it is written in condition (7), i.e., . In Table 1 one can see the range of values for parameters of the CML-Immunotherapy mathematical model. Hence, the latter implies that therapy doses could be personalized for an individual patient as parameters may have different values for each particular case.
Author Contributions
Conceptualization and design, P.A.V.; methodology, P.A.V. and C.P.; formal analysis and software, P.A.V. and L.N.C.; paper writing—original draft preparation, P.A.V.; paper writing—reviewing and editing, L.N.C. and C.P.; project administration, P.A.V. and C.P.; supervision, P.A.V., L.N.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data is contained within the article.
Acknowledgments
This research is fulfilled within the TecNM project number 9951.21-P ‘Computational modelling and in silico experimentation applied to the analysis and control of biological systems’ (Modelizado computacional y experimentos in silico aplicados al análisis y control de sistemas biológicos).
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CML | Chronic Myelogenous Leukemia |
| ODEs | Ordinary Differential Equations |
| LCIS | Localization of Compact Invariant Sets |
Appendix A. Existence and Uniqueness
In this section we discuss the local existence and uniqueness concerning solutions to the CML-Immunotherapy system (1)–(3). First, for the sake of simplicity, let us define the following
with and . Now, the Jacobian matrix of (1)–(3) is computed as indicated below
and it is evident that both and are continuous and exist on the domain with and . It is important to note that the value should not be considered as initial condition due to the indetermination of the logarithmic term. Further, does not represent a biologically meaningful initial scenario concerning any type of cancer evolution.
Now, the latter implies that is locally Lipschitz in x on where see Lemma 3.2 by Khalil in [29] at Section 3.1. Further, by conditions of the Localizing Domain Theorem each element of J is bounded. Therefore, we conclude the following.
Theorem A1.
Local existence and uniqueness. There is a Lipschitz constant such that on Then, satisfies the Lipschitz condition
and there exists some such that the CML-Immunotherapy system (1)–(3), given as with , has a unique solution over .
References
- Weinberg, R.A. The Biology of Cancer, 3rd ed.; Garland Science: New York, NY, USA, 2013. [Google Scholar]
- Ruddon, R.W. Cancer Biology, 4th ed.; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Cancer Today. 2020. Available online: https://gco.iarc.fr/today/online-analysis-table (accessed on 12 March 2021).
- Eden, R.E.; Coviello, J.M. Chronic myelogenous leukemia. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- National Cancer Institute. Chronic Myelogenous Leukemia. 2020. Available online: https://www.cancer.gov/types/leukemia/patient/cml-treatment-pdq (accessed on 12 March 2021).
- National Cancer Institute. Clinical Trials. 2021. Available online: https://www.cancer.gov/about-cancer/treatment/clinical-trials/search/r?loc=0&rl=1&t=C3173 (accessed on 12 March 2021).
- Swan, G.W. Role of optimal control theory in cancer chemotherapy. Math. Biosci. 1990, 101, 237–284. [Google Scholar] [CrossRef]
- Swierniak, A.; Kimmel, M.; Smieja, J. Mathematical modeling as a tool for planning anticancer therapy. Eur. J. Pharmacol. 2009, 625, 108–121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Talkington, A.; Dantoin, C.; Durrett, R. Ordinary differential equation models for adoptive immunotherapy. Bull. Math. Biol. 2018, 80, 1059–1083. [Google Scholar] [CrossRef] [PubMed]
- Phan, T.; Crook, S.M.; Bryce, A.H.; Maley, C.C.; Kostelich, E.J.; Kuang, Y. Mathematical modeling of prostate cancer and clinical application. Appl. Sci. 2020, 10, 2721. [Google Scholar] [CrossRef] [Green Version]
- Colquitt, R.B.; Colquhoun, D.A.; Thiele, R.H. In silico modelling of physiologic systems. Best Pract. Res. Clin. Anaesthesiol. 2011, 25, 499–510. [Google Scholar] [CrossRef]
- De Pillis, L.G.; Gu, W.; Radunskaya, A.E. Mixed immunotherapy and chemotherapy of tumors: Modeling, applications and biological interpretations. J. Theor. Biol. 2006, 238, 841–862. [Google Scholar] [CrossRef]
- De Pillis, L.; Renee Fister, K.; Gu, W.; Collins, C.; Daub, M.; Gross, D.; Moore, J.; Preskill, B. Mathematical model creation for cancer chemo-immunotherapy. Comput. Math. Methods Med. 2009, 10, 165–184. [Google Scholar] [CrossRef] [Green Version]
- Kronik, N.; Kogan, Y.; Elishmereni, M.; Halevi-Tobias, K.; Vuk-Pavlović, S.; Agur, Z. Predicting outcomes of prostate cancer immunotherapy by personalized mathematical models. PLoS ONE 2010, 5, e15482. [Google Scholar] [CrossRef] [Green Version]
- Kim, E.; Brown, J.S.; Eroglu, Z.; Anderson, A.R. Adaptive Therapy for Metastatic Melanoma: Predictions from Patient Calibrated Mathematical Models. Cancers 2021, 13, 823. [Google Scholar] [CrossRef] [PubMed]
- Moore, H.; Li, N.K. A mathematical model for chronic myelogenous leukemia (CML) and T cell interaction. J. Theor. Biol. 2004, 227, 513–523. [Google Scholar] [CrossRef] [PubMed]
- Schürch, C.; Riether, C.; Amrein, M.A.; Ochsenbein, A.F. Cytotoxic T cells induce proliferation of chronic myeloid leukemia stem cells by secreting interferon-γ. J. Exp. Med. 2013, 210, 605–621. [Google Scholar] [CrossRef]
- Garber, H.R.; Mirza, A.; Mittendorf, E.A.; Alatrash, G. Adoptive T-cell therapy for Leukemia. Mol. Cell Ther. 2014, 2, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Krishchenko, A.P. Localization of invariant compact sets of dynamical systems. Differ. Equ. 2005, 41, 1669–1676. [Google Scholar] [CrossRef]
- Krishchenko, A.P.; Starkov, K.E. Localization of compact invariant sets of the Lorenz system. Phys. Lett. A 2006, 353, 383–388. [Google Scholar] [CrossRef]
- Starkov, K.E.; Coria, L.N. Global dynamics of the Kirschner–Panetta model for the tumor immunotherapy. Nonlinear Anal. Real World Appl. 2013, 14, 1425–1433. [Google Scholar] [CrossRef]
- Valle, P.A.; Starkov, K.E.; Coria, L.N. Global stability and tumor clearance conditions for a cancer chemotherapy system. Commun. Nonlinear Sci. Numer. Simul. 2016, 40, 206–215. [Google Scholar] [CrossRef]
- Krishchenko, A.P.; Starkov, K.E. The four-dimensional Kirschner-Panetta type cancer model: How to obtain tumor eradication? Math. Biosci. Eng. 2018, 15, 1243. [Google Scholar] [CrossRef] [Green Version]
- Valle, P.A.; Coria, L.N.; Salazar, Y. Tumor Clearance Analysis on a Cancer Chemo-Immunotherapy Mathematical Model. Bull. Math. Biol. 2019, 81, 4144–4173. [Google Scholar] [CrossRef] [PubMed]
- Starkov, K.E.; Kanatnikov, A.N.; Andres, G. Ultimate tumor dynamics and eradication using oncolytic virotherapy. Commun. Nonlinear Sci. Numer. Simul. 2021, 92, 105469. [Google Scholar] [CrossRef]
- De Leenheer, P.; Aeyels, D. Stability properties of equilibria of classes of cooperative systems. IEEE Trans. Autom. Contr. 2001, 46, 1996–2001. [Google Scholar] [CrossRef] [Green Version]
- Korobeinikov, A.; Starkov, K.E.; Valle, P.A. Modeling cancer evolution: Evolutionary escape under immune system control. J. Phys. Conf. Ser. 2017, 811, 012004. [Google Scholar] [CrossRef]
- Jenner, A.L.; Kim, P.S.; Frascoli, F. Oncolytic virotherapy for tumours following a Gompertz growth law. J. Theor. Biol. 2019, 480, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Khalil, H.K. Nonlinear Systems, 3rd ed.; Prentice-Hall: Hoboken, NJ, USA, 2002. [Google Scholar]
- Kuznetsov, V.A.; Makalkin, I.A.; Taylor, M.A.; Perelson, A.S. Nonlinear dynamics of immunogenic tumors: Parameter estimation and global bifurcation analysis. Bull. Math. Biol. 1994, 56, 295–321. [Google Scholar] [CrossRef]
- Kirschner, D.; Panetta, J.C. Modeling immunotherapy of the tumor–immune interaction. J. Math. Biol. 1998, 37, 235–252. [Google Scholar] [CrossRef] [Green Version]
- Kronik, N.; Kogan, Y.; Vainstein, V.; Agur, Z. Improving alloreactive CTL immunotherapy for malignant gliomas using a simulation model of their interactive dynamics. Cancer Immunol. Immunother. 2008, 57, 425–439. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, S.; Khajanchi, S.; Chaudhuri, S. A mathematical model to elucidate brain tumor abrogation by immunotherapy with T11 target structure. PLoS ONE 2015, 10, e0123611. [Google Scholar] [CrossRef] [Green Version]
- Valle, P.A.; Coria, L.N.; Carballo, K.D. Chemoimmunotherapy for the treatment of prostate cancer: Insights from mathematical modelling. Appl. Math. Model. 2021, 90, 682–702. [Google Scholar] [CrossRef]
- Mehdizadeh, R.; Shariatpanahi, S.P.; Goliaei, B.; Peyvandi, S.; Rüegg, C. Dormant Tumor Cell Vaccination: A Mathematical Model of Immunological Dormancy in Triple-Negative Breast Cancer. Cancers 2021, 13, 245. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Immunotherapy Side Effects. 2019. Available online: https://www.cancer.gov/about-cancer/treatment/types/immunotherapy/side-effects (accessed on 12 March 2021).
- Kirschner, D.; Webb, G.F. A model for treatment strategy in the chemotherapy of AIDS. Bull. Math. Biol. 1996, 58, 367–390. [Google Scholar] [CrossRef]
- De Pillis, L.G.; Radunskaya, A. The dynamics of an optimally controlled tumor model: A case study. Math. Comput. Model. 2003, 37, 1221–1244. [Google Scholar] [CrossRef]
- D’Onofrio, A. A general framework for modeling tumor-immune system competition and immunotherapy: Mathematical analysis and biomedical inferences. Physica D 2005, 208, 220–235. [Google Scholar] [CrossRef] [Green Version]
- De Pillis, L.G.; Gu, W.; Fister, K.R.; Head, T.A.; Maples, K.; Murugan, A.; Neal, T.; Yoshida, K. Chemotherapy for tumors: An analysis of the dynamics and a study of quadratic and linear optimal controls. Math. Biosci. 2007, 209, 292–315. [Google Scholar] [CrossRef] [PubMed]
- Ledzewicz, U.; Amini, B.; Schättler, H. Dynamics and control of a mathematical model for metronomic chemotherapy. Math. Biosci. Eng. 2015, 12, 1257–1275. [Google Scholar] [CrossRef] [PubMed]
- Letellier, C.; Sasmal, S.K.; Draghi, C.; Denis, F.; Ghosh, D. A chemotherapy combined with an anti-angiogenic drug applied to a cancer model including angiogenesis. Chaos Soliton Fract. 2017, 99, 297–311. [Google Scholar] [CrossRef]
- Isaac Oke, S.; Matadi, M.B.; Xulu, S.S. Optimal Control Analysis of a Mathematical Model for Breast Cancer. Math. Comput. Appl. 2018, 23, 21. [Google Scholar] [CrossRef] [Green Version]
- Belfo, J.P.; Lemos, J.M. Optimal Impulsive Control for Cancer Therapy; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Mohri, H.; Perelson, A.S.; Tung, K.; Ribeiro, R.M.; Ramratnam, B.; Markowitz, M.; Kost, R.; Weinberger, L.; Cesar, D.; Hellerstein, M.K.; et al. Increased turnover of T lymphocytes in HIV-1 infection and its reduction by antiretroviral therapy. J. Exp. Med. 2001, 194, 1277–1288. [Google Scholar] [CrossRef] [Green Version]
- Hull, M.W.; Harris, M.; Montaner, J.S. Principles of Management of HIV in the Industrialized World. In Infectious Diseases; Elsevier: Amsterdam, The Netherlands, 2017; pp. 912–917. [Google Scholar] [CrossRef]
- Cruz, S.A.; Valle, P.A.; Sotelo, A.; Plata, C.; Coria, L.N. HIV Mathematical Model considering Antiretroviral Administration. Rev. Mex. Ing. Biomédica 2017, 38, 563–573. [Google Scholar] [CrossRef] [Green Version]
- Geynisman, D.M.; Chien, C.R.; Smieliauskas, F.; Shen, C.; Shih, Y.C.T. Economic evaluation of therapeutic cancer vaccines and immunotherapy: A systematic review. Hum. Vaccines Immunother. 2014, 10, 3415–3424. [Google Scholar] [CrossRef] [Green Version]
Figure 1.
When the cellular immunotherapy treatment parameter fulfills condition (7), i.e., , all solutions for the CML-Immunotherapy system (1)–(3) go to the tumour-free equilibrium point (8) given by . For this particular case, we set the initial tumour density as cells/μL, as we consider the concentration of leukemia cancer cells at the maximum carrying capacity. Different initial conditions will yield the same result: CML cancer cells eradication and asymptotic stability of the tumour-free equilibrium point.
Figure 1.
When the cellular immunotherapy treatment parameter fulfills condition (7), i.e., , all solutions for the CML-Immunotherapy system (1)–(3) go to the tumour-free equilibrium point (8) given by . For this particular case, we set the initial tumour density as cells/μL, as we consider the concentration of leukemia cancer cells at the maximum carrying capacity. Different initial conditions will yield the same result: CML cancer cells eradication and asymptotic stability of the tumour-free equilibrium point.

Figure 2.
Administration protocol for the immunotherapy treatment. Characteristics are as follows: amplitude of 15,396 cells/μL and a duty cycle of /day. Complete CML cancer cells eradication was achieved by means of this strategy for three considered initial non-solid tumour sizes given by , , and .
Figure 2.
Administration protocol for the immunotherapy treatment. Characteristics are as follows: amplitude of 15,396 cells/μL and a duty cycle of /day. Complete CML cancer cells eradication was achieved by means of this strategy for three considered initial non-solid tumour sizes given by , , and .

Figure 3.
Case 1: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.
Figure 3.
Case 1: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.

Figure 4.
Case 2: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.
Figure 4.
Case 2: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.

Figure 5.
Case 3: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.
Figure 5.
Case 3: The initial tumour size for the CML cancer cells is set as cells/μL. The cellular immunotherapy had to be applied days to achieve complete leukemia cancer cells eradication.

Figure 6.
Dynamics of solutions of the CML cancer cells population when considering three initial tumour sizes: with cells/μL, with cells/μL, and with cells/μL. Regardless of the initial tumour concentration, complete leukemia cells eradication is achieved in all cases. The immunotherapy administration protocol from Figure 2 is applied to each case, i.e., daily applications of the treatment with a duty cycle of /day and a fixed amplitude of 15,396 cells/μL.
Figure 6.
Dynamics of solutions of the CML cancer cells population when considering three initial tumour sizes: with cells/μL, with cells/μL, and with cells/μL. Regardless of the initial tumour concentration, complete leukemia cells eradication is achieved in all cases. The immunotherapy administration protocol from Figure 2 is applied to each case, i.e., daily applications of the treatment with a duty cycle of /day and a fixed amplitude of 15,396 cells/μL.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Parameter information for the CML-immunotherapy dynamical system.
| Parameter | Description | Value | Range | Units |
|---|---|---|---|---|
| Natural proliferation of naive T cells | cells/(μL × day) | |||
| Natural death rate of naive T cells | day | |||
| Differentiation rate of naive T cells into effector | day | |||
| T cells due to their interaction with CML cells | ||||
| Half saturation term of T cells recruitment | 100 | cells/μL | ||
| Proliferation rate of effector T cells | ||||
| Recruitment rate of effector T cells by CML cells | day | |||
| Natural death rate of effector T cells | day | |||
| Inactivation rate of effector T cells by CML cells | μL/(cells × day) | |||
| Adaptive T-cell therapy | to be estimated | cells/(μL × day) | ||
| Growth rate of CML cells | day | |||
| Maximum carrying capacity of the CML cells | cells/μL | |||
| Natural death rate of the CML cells | day | |||
| Elimination of CML cells by effector T cells | μL/(cells × day) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Valle, P.A.; Coria, L.N.; Plata, C. Personalized Immunotherapy Treatment Strategies for a Dynamical System of Chronic Myelogenous Leukemia. Cancers 2021, 13, 2030. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092030
AMA Style
Valle PA, Coria LN, Plata C. Personalized Immunotherapy Treatment Strategies for a Dynamical System of Chronic Myelogenous Leukemia. Cancers. 2021; 13(9):2030. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092030
Chicago/Turabian StyleValle, Paul A., Luis N. Coria, and Corina Plata. 2021. "Personalized Immunotherapy Treatment Strategies for a Dynamical System of Chronic Myelogenous Leukemia" Cancers 13, no. 9: 2030. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13092030
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.