
Clinical Relevance of Viable Circulating Tumor Cells in Patients with Metastatic Colorectal Cancer: The COLOSPOT Prospective Study

 , ,
, ,  ,
, 
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
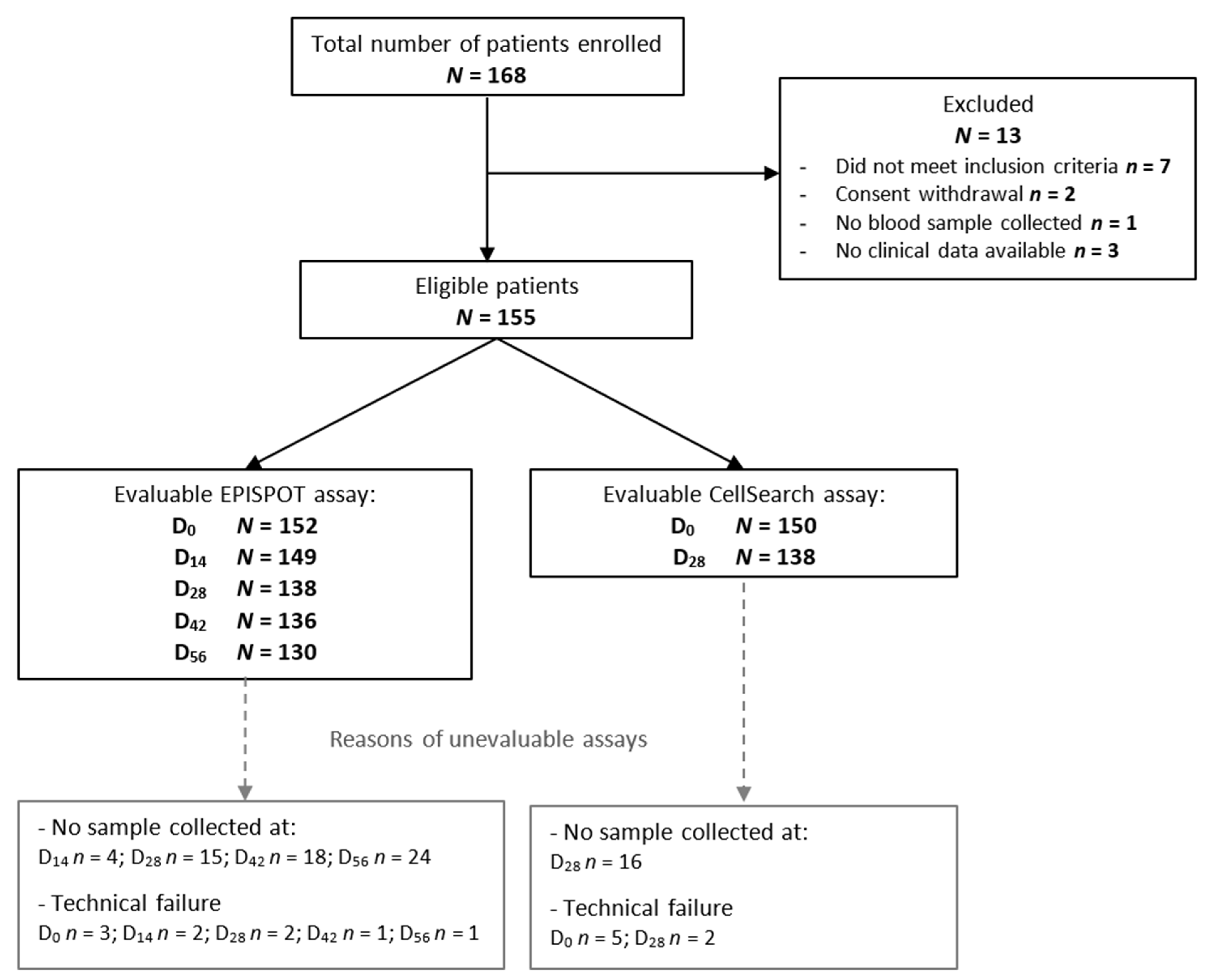
2.1. Study Design
2.2. CTC Isolation and Enumeration
2.3. Statistical Analyses
3. Results
3.1. Clinical and Tumor Characteristics
3.2. CTC Prevalence at Different Time Points and Correlation with Baseline Characteristics
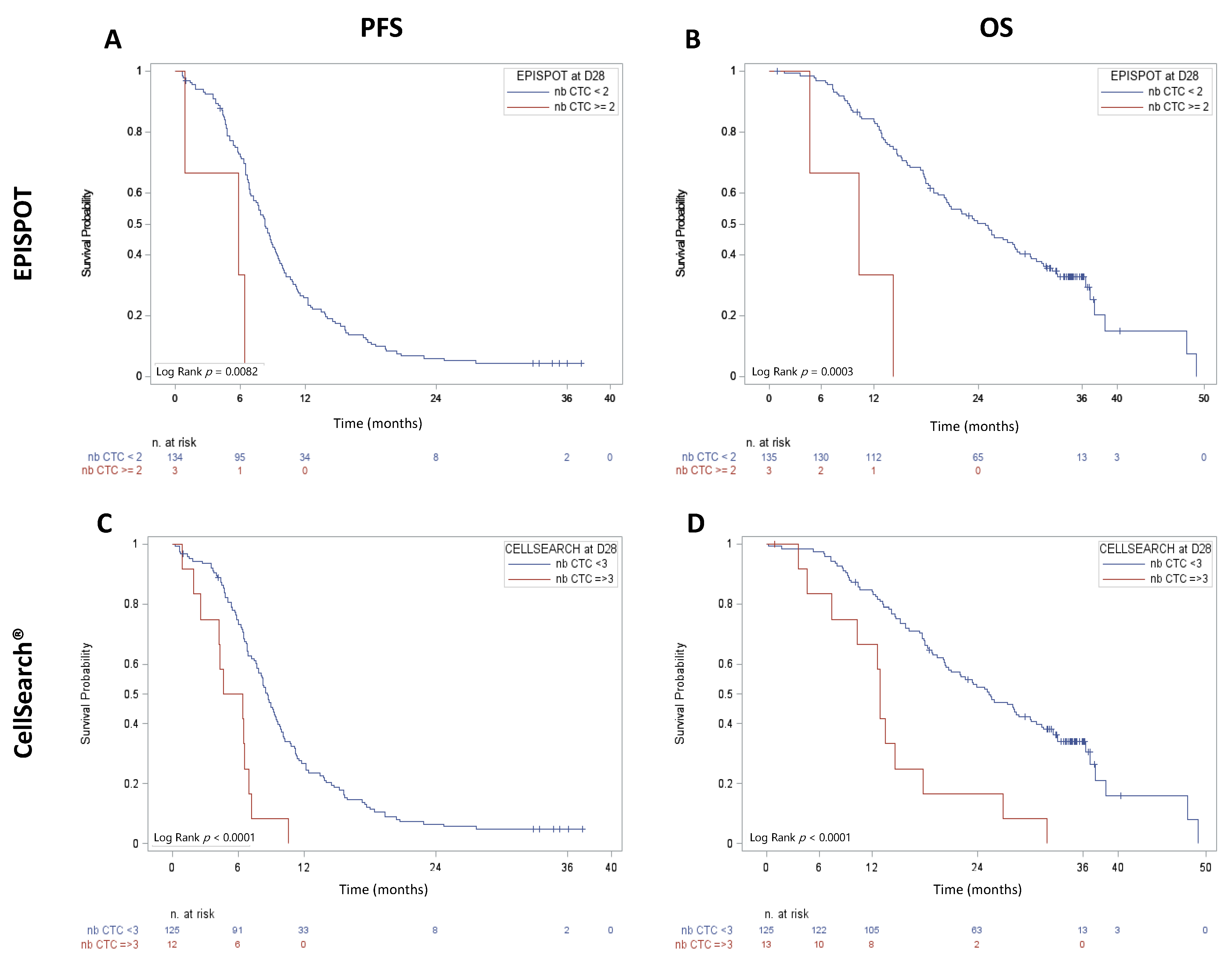
3.3. CTC Presence Correlates with PFS and OS in Patients with Metastatic CRC
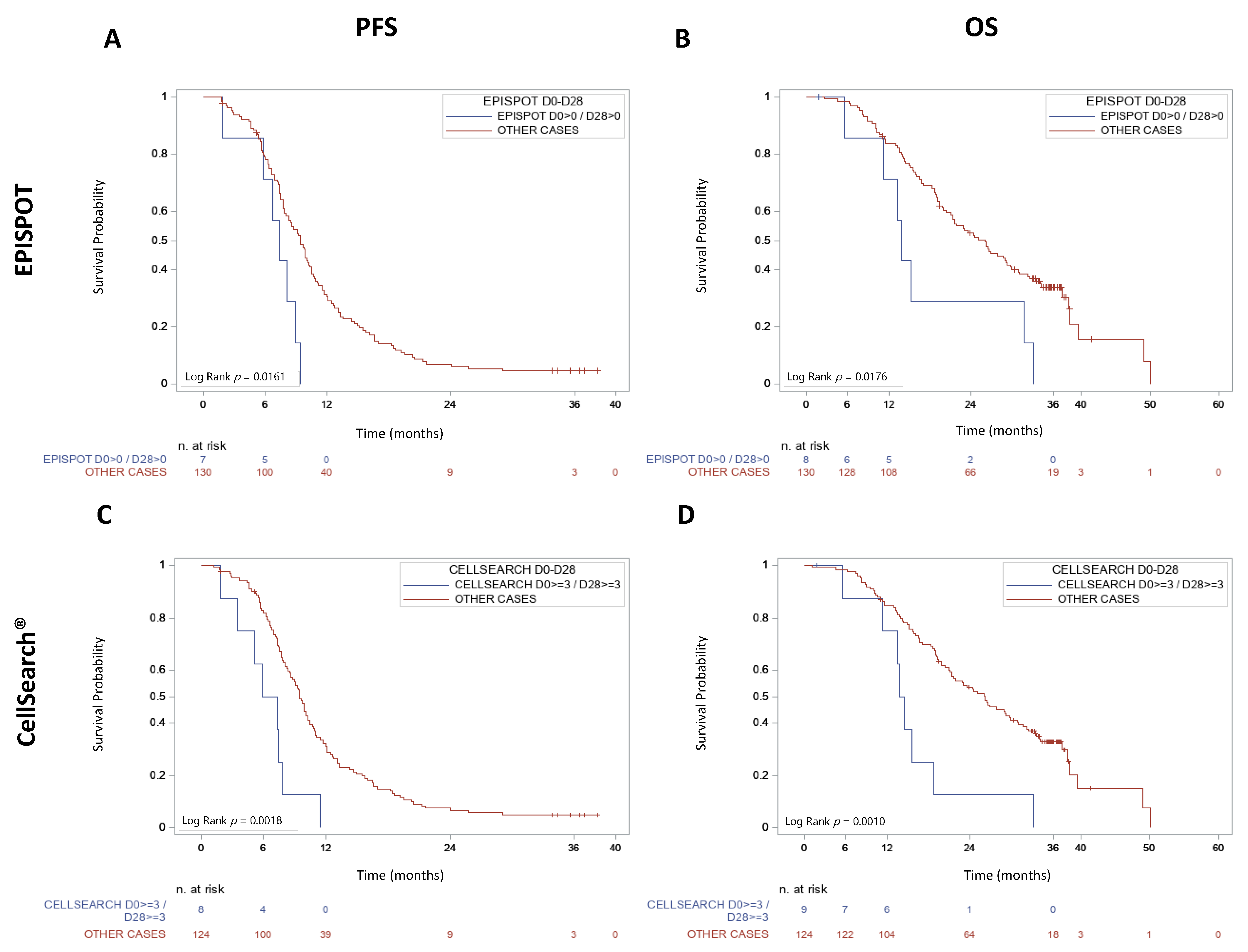
3.4. CTC Kinetics between D0 and D28 Correlates with PFS and OS
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferlay, J.; Colombet, M.; Soerjomataram, I.; Dyba, T.; Randi, G.; Bettio, M.; Gavin, A.; Visser, O.; Bray, F. Cancer incidence and mortality patterns in Europe: Estimates for 40 countries and 25 major cancers in 2018. Eur. J. Cancer 2018, 103, 356–387. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fedewa, S.A.; Ahnen, D.J.; Meester, R.G.S.; Barzi, A.; Jemal, A. Colorectal cancer statistics, 2017. CA Cancer J. Clin. 2017, 67, 177–193. [Google Scholar] [CrossRef]
- Benson, A.B.; Venook, A.P.; Al-Hawary, M.M.; Arain, M.A.; Chen, Y.J.; Ciombor, K.K.; Cohen, S.; Cooper, H.S.; Deming, D.; Farkas, L.; et al. Colon Cancer, Version 2.2021, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2021, 19, 329–359. [Google Scholar] [CrossRef]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; van Krieken, J.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Phelip, J.M.; Tougeron, D.; Léonard, D.; Benhaim, L.; Desolneux, G.; Dupré, A.; Michel, P.; Penna, C.; Tournigand, C.; Louvet, C.; et al. Metastatic colorectal cancer (mCRC): French intergroup clinical practice guidelines for diagnosis, treatments and follow-up (SNFGE, FFCD, GERCOR, UNICANCER, SFCD, SFED, SFRO, SFR). Dig. Liver Dis. 2019, 51, 1357–1363. [Google Scholar] [CrossRef] [PubMed]
- Loupakis, F.; Ruzzo, A.; Cremolini, C.; Vincenzi, B.; Salvatore, L.; Santini, D.; Masi, G.; Stasi, I.; Canestrari, E.; Rulli, E.; et al. KRAS codon 61, 146 and BRAF mutations predict resistance to cetuximab plus irinotecan in KRAS codon 12 and 13 wild-type metastatic colorectal cancer. Br. J. Cancer 2009, 101, 715–721. [Google Scholar] [CrossRef] [Green Version]
- Douillard, J.-Y.; Oliner, K.S.; Siena, S.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N. Engl. J. Med. 2013, 369, 1023–1034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cidon, E.U.; Alonso, P.; Masters, B. Markers of Response to Antiangiogenic Therapies in Colorectal Cancer: Where are We Now and What should be Next? Clin. Med. Insights Oncol. 2016, 10, CMO.S34542. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pantel, K.; Alix-Panabières, C. Circulating tumour cells in cancer patients: Challenges and perspectives. Trends Mol. Med. 2010, 16, 398–406. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.J.; Punt, C.J.A.; Iannotti, N.; Saidman, B.H.; Sabbath, K.D.; Gabrail, N.Y.; Picus, J.; Morse, M.; Mitchell, E.; Miller, M.C.; et al. Relationship of Circulating Tumor Cells to Tumor Response, Progression-Free Survival, and Overall Survival in Patients With Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 3213–3221. [Google Scholar] [CrossRef]
- Tol, J.; Koopman, M.; Miller, M.C.; Tibbe, A.; Cats, A.; Creemers, G.J.M.; Vos, A.H.; Nagtegaal, I.; Terstappen, L.W.M.M.; Punt, C.J.A. Circulating tumour cells early predict progression-free and overall survival in advanced colorectal cancer patients treated with chemotherapy and targeted agents. Ann. Oncol. 2010, 21, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; Maestro, M.L.; Gómez-España, A.; Rivera, F.; Valladares, M.; Massuti, B.; Benavides, M.; Gallen, M.; Marcuello, E.; Abad, A.; et al. Circulating Tumor Cell Count Is a Prognostic Factor in Metastatic Colorectal Cancer Patients Receiving First-Line Chemotherapy Plus Bevacizumab: A Spanish Cooperative Group for the Treatment of Digestive Tumors Study. Oncologist 2012, 17, 947–955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riethdorf, S.; Fritsche, H.; Müller, V.; Rau, T.; Schindlbeck, C.; Rack, B.; Janni, W.; Coith, C.; Beck, K.; Jänicke, F.; et al. Detection of Circulating Tumor Cells in Peripheral Blood of Patients with Metastatic Breast Cancer: A Validation Study of the CellSearch System. Clin. Cancer Res. 2007, 13, 920–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikolajczyk, S.D.; Millar, L.S.; Tsinberg, P.; Coutts, S.M.; Zomorrodi, M.; Pham, T.; Bischoff, F.Z.; Pircher, T.J. Detection of EpCAM-Negative and Cytokeratin-Negative Circulating Tumor Cells in Peripheral Blood. J. Oncol. 2011, 2011, 252361. [Google Scholar] [CrossRef] [PubMed]
- Serrano, M.J.; Ortega, F.G.; Cubero, M.J.A.; Nadal, R.; Sánchez, F.G.O.; Salido, M.; Rodríguez, M.; García-Puche, J.L.; Delgado-Rodriguez, M.; Solé, F.; et al. EMT and EGFR in CTCs cytokeratin negative non-metastatic breast cancer. Oncotarget 2014, 5, 7486–7497. [Google Scholar] [CrossRef] [Green Version]
- Soler, A.; Cayrefourcq, L.; Mazel, M.; Alix-Panabières, C. EpCAM-Independent Enrichment and Detection of Viable Circulating Tumor Cells Using the EPISPOT Assay. In Circulating Tumor Cells; Magbanua, M.J.M., Park, J.W., Eds.; Springer: New York, NY, USA, 2017; Volume 1634, pp. 263–276. [Google Scholar] [CrossRef]
- Ramirez, J.-M.; Fehm, T.; Orsini, M.; Cayrefourcq, L.; Maudelonde, T.; Pantel, K.; Alix-Panabières, C. Prognostic Relevance of Viable Circulating Tumor Cells Detected by EPISPOT in Metastatic Breast Cancer Patients. Clin. Chem. 2014, 60, 214–221. [Google Scholar] [CrossRef] [Green Version]
- DeNeve, E.; Riethdorf, S.; Ramos, J.; Nocca, D.; Coffy, A.; Daurès, J.-P.; Maudelonde, T.; Fabre, J.-M.; Pantel, K.; Alix-Panabières, C. Capture of Viable Circulating Tumor Cells in the Liver of Colorectal Cancer Patients. Clin. Chem. 2013, 59, 1384–1392. [Google Scholar] [CrossRef] [Green Version]
- Cristofanilli, M.; Budd, G.T.; Ellis, M.J.; Stopeck, A.; Matera, J.; Miller, M.C.; Reuben, J.M.; Doyle, G.V.; Allard, W.J.; Terstappen, L.W.; et al. Circulating Tumor Cells, Disease Progression, and Survival in Metastatic Breast Cancer. N. Engl. J. Med. 2004, 351, 781–791. [Google Scholar] [CrossRef] [Green Version]
- De Bono, J.S.; Scher, H.I.; Montgomery, R.B.; Parker, C.; Miller, M.C.; Tissing, H.; Doyle, G.V.; Terstappen, L.W.; Pienta, K.; Raghavan, D. Circulating Tumor Cells Predict Survival Benefit from Treatment in Metastatic Castration-Resistant Prostate Cancer. Clin. Cancer Res. 2008, 14, 6302–6309. [Google Scholar] [CrossRef] [Green Version]
- Bidard, F.-C.; Peeters, D.J.; Fehm, T.; Nolé, F.; Gisbert-Criado, R.; Mavroudis, D.; Grisanti, S.; Generali, D.; Garcia-Saenz, J.A.; Stebbing, J.; et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: A pooled analysis of individual patient data. Lancet Oncol. 2014, 15, 406–414. [Google Scholar] [CrossRef]
- Bidard, F.-C.; Jacot, W.; Kiavue, N.; Dureau, S.; Kadi, A.; Brain, E.; Bachelot, T.; Bourgeois, H.; Gonçalves, A.; Ladoire, S.; et al. Efficacy of Circulating Tumor Cell Count–Driven vs Clinician-Driven First-line Therapy Choice in Hormone Receptor–Positive, ERBB2-Negative Metastatic Breast Cancer. JAMA Oncol. 2021, 7, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Cremolini, C.; Loupakis, F.; Antoniotti, C.; Lupi, C.; Sensi, E.; Lonardi, S.; Mezi, S.; Tomasello, G.; Ronzoni, M.; Zaniboni, A.; et al. FOLFOXIRI plus bevacizumab versus FOLFIRI plus bevacizumab as first-line treatment of patients with metastatic colorectal cancer: Updated overall sur-vival and molecular subgroup analyses of the open-label, phase 3 TRIBE study. Lancet Oncol. 2015, 16, 1306–1315. [Google Scholar] [CrossRef]
- E Silva, V.S.; Chinen, L.; Abdallah, E.A.; Damascena, A.; Paludo, J.; Chojniak, R.; Dettino, A.; Mello, C.A.L.; Alves, V.S.; Fanelli, M.F. Early detection of poor outcome in patients with metastatic colorectal cancer: Tumor kinetics evaluated by circulating tumor cells. OncoTargets Ther. 2016, 9, 7503–7513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, C.; Chen, F.; Wang, S.; Xiong, B. Circulating Tumor Cells in Gastrointestinal Cancers: Current Status and Future Perspectives. Front. Oncol. 2019, 9, 1427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuske, A.; Gorges, T.M.; Tennstedt, P.; Tiebel, A.-K.; Pompe, R.S.; Preißer, F.; Prues, S.; Mazel, M.; Markou, A.; Lianidou, E.; et al. Improved detection of circulating tumor cells in non-metastatic high-risk prostate cancer patients. Sci. Rep. 2016, 6, 39736. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cayrefourcq, L.; De Roeck, A.; Garcia, C.; Stoebner, P.-E.; Fichel, F.; Garima, F.; Perriard, F.; Daures, J.-P.; Meunier, L.; Alix-Panabières, C. S100-EPISPOT: A New Tool to Detect Viable Circulating Melanoma Cells. Cells 2019, 8, 755. [Google Scholar] [CrossRef] [Green Version]
- Garrel, R.; Mazel, M.; Perriard, F.; Vinches, M.; Cayrefourcq, L.; Guigay, J.; Digue, L.; Aubry, K.; Alfonsi, M.; Delord, J.-P.; et al. Circulating Tumor Cells as a Prognostic Factor in Recurrent or Metastatic Head and Neck Squamous Cell Carcinoma: The CIRCUTEC Prospective Study. Clin. Chem. 2019, 65, 1267–1275. [Google Scholar] [CrossRef]
- Krebs, M.; Renehan, A.; Backen, A.; Gollins, S.; Chau, I.; Hasan, J.; Valle, J.W.; Morris, K.; Beech, J.; Ashcroft, L.; et al. Circulating Tumor Cell Enumeration in a Phase II Trial of a Four-Drug Regimen in Advanced Colorectal Cancer. Clin. Color. Cancer 2015, 14, 115–122.e2. [Google Scholar] [CrossRef] [PubMed]
- Sastre, J.; de la Orden, V.; Martínez, A.; Bando, I.; Balbín, M.; Bellosillo, B.; Palanca, S.; Gomez, M.I.P.; Mediero, B.; Llovet, P.; et al. Association Between Baseline Circulating Tumor Cells, Molecular Tumor Profiling, and Clinical Characteristics in a Large Cohort of Chemo-naïve Metastatic Colorectal Cancer Patients Prospectively Collected. Clin. Color. Cancer 2020, 19, e110–e116. [Google Scholar] [CrossRef]
- Kaifi, J.T.; Kunkel, M.; Dicker, D.T.; Joude, J.; E Allen, J.; Das, A.; Zhu, J.; Yang, Z.; E Sarwani, N.; Li, G.; et al. Circulating tumor cell levels are elevated in colorectal cancer patients with high tumor burden in the liver. Cancer Biol. Ther. 2015, 16, 690–698. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Parameters | EPISPOT (n = 152) | CellSearch® (n = 150) | ||||
|---|---|---|---|---|---|---|
| ≥1 | <1 | p-Value (Fisher) | ≥3 | <3 | p-Value (Fisher) | |
| Age | ||||||
| <70 years | 21 (66%) | 77 (64%) | 1 | 42 (71%) | 55 (61%) | 0.22 |
| ≥70 years | 11 (34%) | 43 (36%) | 17 (29%) | 36 (39%) | ||
| Sex | ||||||
| Men | 23 (72%) | 73 (61% | 0.31 | 35 (59%) | 58 (64%) | 0.61 |
| Women | 9 (28%) | 47 (39%) | 24 (41%) | 33 (36%) | ||
| Baseline ECOG PS score | ||||||
| 0 | 15 (47%) | 67 (57%) | 0.32 | 22 (39%) | 59 (66%) | 0.0021 |
| 1–2 | 17 (53%) | 50 (43%) | 35 (61%) | 31 (34%) | ||
| CRC localization | ||||||
| Right | 11 (37%) | 39 (32%) | 0.67 | 21 (37%) | 29 (32%) | 0.59 |
| Left | 19 (63%) | 81 (68%) | 36 (63%) | 62 (68%) | ||
| Metastases | ||||||
| Synchronous | 23 (74%) | 77 (65%) | 0.40 | 48 (83%) | 50 (57%) | 0.0012 |
| Metachronous | 8 (26%) | 41 (35%) | 10 (17%) | 38 (43%) | ||
| Nb of organs with metastases | ||||||
| 1 | 14 (45%) | 47 (39%) | 0.55 | 21 (36%) | 39 (43%) | 0.49 |
| >1 | 17 (55%) | 73 (61%) | 37 (64%) | 51 (57%) | ||
| Liver metastases | ||||||
| Yes | 26 (84%) | 97 (81%) | 0.80 | 54 (93%) | 66 (73%) | 0.0025 |
| No | 5 (16%) | 23 (19%) | 4 (7%) | 24 (27%) | ||
| RAS status | ||||||
| Wild type | 10 (38%) | 30 (31%) | 0.49 | 13 (29%) | 26 (34%) | 0.69 |
| Mutant | 16 (62%) | 66 (69%) | 32 (71%) | 50 (66%) | ||
| B-RAF status | ||||||
| Wild type | 28 (97%) | 92 (92%) | 0.68 | 46(92%) | 74(95%) | 0.71 |
| Mutant | 1 (3%) | 8 (8%) | 4(8%) | 4(5%) | ||
| CEA value | ||||||
| Normal | 8 (25%) | 36 (31%) | 0.66 | 7 (12%) | 37 (42%) | 0.0001 |
| >normal | 24 (75%) | 81 (69%) | 51 (88%) | 52 (58%) | ||
| Parameters | PFS | OS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age: ≥70 vs. <70 years | 1.04 | 0.74–1.46 | 0.84 | 1.08 | 0.72–1.62 | 0.71 |
| Sex: W vs. M | 0.84 | 0.6–1.19 | 0.32 | 1.28 | 0.86–1.89 | 0.22 |
| ECOG PS: 1–2 vs. 0 | 1.46 | 1.05–2.05 | 0.0259 | 2.66 | 1.77–3.99 | <0.0001 |
| Right vs. left colon | 1.07 | 0.75–1.51 | 0.72 | 1.54 | 1.03–2.31 | 0.04 |
| Synchronous vs. metachronous mets | 0.78 | 0.55–1.11 | 0.17 | 1.24 | 0.81–1.88 | 0.32 |
| N of organs with mets: >1 vs. 1 | 1.21 | 0.86–1.69 | 0.27 | 1.34 | 0.9–2 | 0.15 |
| Liver mets vs. no-liver mets | 0.9 | 0.59–1.37 | 0.62 | 1.53 | 0.87–2.69 | 0.14 |
| CEA: >nal vs. nal | 1.04 | 0.71–1.5 | 0.85 | 1.46 | 0.92–2.32 | 0.11 |
| RAS: MT vs. WT | 0.76 | 0.51–1.12 | 0.16 | 0.71 | 0.45–1.12 | 0.14 |
| B-RAF: MT vs. WT | 3.27 | 1.61–6.64 | 0.001 | 7.39 | 3.36–16.25 | <0.0001 |
| D0-D28 CTC kinetics (EPISPOT): Positive at both time points (≥1) vs. other cases | 2.52 | 1.15–5.52 | 0.0204 | 2.48 | 1.14–5.37 | 0.0219 |
| D0-D28 CTC kinetics (CellSearch®): Positive at both time points (≥3) vs. other cases | 3.02 | 1.45–6.3 | 0.0031 | 3.22 | 1.54–6.74 | 0.0019 |
| Parameters | PFS | OS | ||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| ECOG PS: 1–2 vs. 0 | 2.48 | 1.51–4.07 | 0.0003 | |||
| B-RAF: MT vs. WT | 3.046 | 1.43–6.5 | 0.0043 | 5.34 | 2.23–12.79 | 0.0002 |
| D0–D28 CTC kinetics (EPISPOT): Positive at both time points (≥1) vs. other cases | 2.445 | 1.04–5.78 | 0.0414 | |||
| D0–D28 CTC kinetics (CellSearch®): Positive at both time points (≥3) vs. other cases | 2.461 | 1.06–5.74 | 0.037 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mazard, T.; Cayrefourcq, L.; Perriard, F.; Senellart, H.; Linot, B.; de la Fouchardière, C.; Terrebonne, E.; François, E.; Obled, S.; Guimbaud, R.; et al. Clinical Relevance of Viable Circulating Tumor Cells in Patients with Metastatic Colorectal Cancer: The COLOSPOT Prospective Study. Cancers 2021, 13, 2966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13122966
Mazard T, Cayrefourcq L, Perriard F, Senellart H, Linot B, de la Fouchardière C, Terrebonne E, François E, Obled S, Guimbaud R, et al. Clinical Relevance of Viable Circulating Tumor Cells in Patients with Metastatic Colorectal Cancer: The COLOSPOT Prospective Study. Cancers. 2021; 13(12):2966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13122966
Chicago/Turabian StyleMazard, Thibault, Laure Cayrefourcq, Françoise Perriard, Hélène Senellart, Benjamin Linot, Christelle de la Fouchardière, Eric Terrebonne, Eric François, Stéphane Obled, Rosine Guimbaud, and et al. 2021. "Clinical Relevance of Viable Circulating Tumor Cells in Patients with Metastatic Colorectal Cancer: The COLOSPOT Prospective Study" Cancers 13, no. 12: 2966. https://0-doi-org.brum.beds.ac.uk/10.3390/cancers13122966